

Abstract
We are reporting a case of extensor pollicis longus tendon rupture which did not require tendon transfer owing to the ability of the intact extensor pollicis brevis (EPB) to fully hyperextend the thumb interphalangeal joint. The thumb metacarpophalangeal joint was also able to be fully actively extended by the EPB. Previous anatomical studies have demonstrated that the insertional anatomy of the EPB tendon is highly variable and sometimes inserts onto the extensor hood and distal phalanx, which is likely the mechanism by which our patient was able to fully extend the thumb interphalangeal joint. Despite the potential for the EPB to extend the IP joint of the thumb, virtually all previously reported cases of extensor pollicis longus (EPL) tendon rupture had deficits of thumb IP extension requiring tendon transfer. This case highlights the potential ability of the EPB tendon to completely substitute for the function of the EPL tendon in providing thumb IP joint extension.
Keywords: Extensor pollicis brevis, Extensor pollicis longus, Tendon rupture, Extensor pollicis longus tendon rupture
Core tip: The extensor pollicis brevis may be able to substitute for extensor pollicis longus (EPL) function in some patients when EPL has ruptured.
INTRODUCTION
Extensor pollicis longus (EPL) tendon rupture may occur spontaneously or following distal radius fracture, surgical fixation, or repetitive use[1,2]. Virtually all reported cases of EPL tendon rupture have been treated by tendon transfer or tendon grafting in order to restore thumb interphalangeal joint extension. The extensor pollicis brevis (EPB) tendon is classically described as inserting upon the base of the thumb proximal phalanx providing thumb metacarpophalangeal joint extension. Several anatomic studies, however, have demonstrated the EPB insertional anatomy to be highly variable with potential insertions on the extensor hood as well as the distal phalanx (Table 1)[3-8]. One study demonstrated that 21% of EPB tendons, when pulled on at the wrist level, would cause thumb IP joint extension in cadavers[7]. It is therefore interesting that, to the best of our knowledge, there have been no reports of EPL rupture in which thumb MP and IP joint extension remains normal. We report a case of EPL tendon rupture in which normal thumb MP and IP motion was preserved most likely owing to the EPB inserting on the extensor hood and/or the distal phalanx.
Table 1.
Previous anatomic studies of extensor pollicis brevis insertional anatomy
| Ref. | Type of study | # of hands | EPB insertion site |
| Stein[3] | Cadaver study | 42 cadavers, 84 wrists dissected | No comment on insertional anatomy |
| Dawson et al[4] | Cadaver Study | 16 hands of eight cadavers | 56% inserted partly to the base of the first phalanx and partly to the extensor hood 25% inserted entirely on the base of the thumb proximal phalanx 19% inserted entirely onto the extensor hood 5% were absent - the Abductor pollicis longus tendon instead inserted partly to the extensor hood and partly to proximal phalanx Four out of the eight cadavers showed asymmetry of the EPB between right and left hands |
| Brunelliet al[5] | Cadaver study | 52 hands | 19% inserted onto proximal phalanx with most also having attachments to extensor hood 69% inserted into the extensor hood 8% inserted into the base of the distal phalanx 4% were absent |
| Kulshreshtha et al[6] | Cadaver study | 44 hands 23 cadavers | 25% inserted onto proximal phalanx 25% of tendons insert partly to the base of the proximal phalanx and partly to the extensor hood 2% of tendons inserted entirely into extensor hood 27% of tendons inserted partly to the base of the proximal phalanx and partly to the extensor hood, and from there, continuing further to the base of the distal phalanx with EPL 20% of tendons inserted into the extensor hood and, from there, continued further to the base of the distal phalanx with EPL The EPB was present in all hands, but anatomy of the EPB is variable on the left and right sides of 14 of the 21 paired hands |
| Alemohammad et al[7] | Clinical study and Cadaver study | 90 cadaver wrists, and 143 patients undergoing Dequervain’s release surgery | In the cadaver group - in 21% pulling on the EPB tendon produced thumb IP joint extension 79% inserted onto proximal phalanx 17% inserted onto distal phalanx 4% inserted onto extensor hood |
| Shigematsu et al[8] | Cadaver study | 72 cadaver specimens, 144 hands | 29% inserted entirely onto the extensor hood 22% inserted onto the base of the proximal phalanx 19% inserted partly onto the base of the proximal phalanx and partly into the extensor hood 9.0% inserted onto the base of the proximal phalanx and into the extensor hood, and then on the base of the distal phalanx, along with EPL 9.0% inserted onto the extensor hood, and then onto the base of the distal phalanx, along with the EPL 2% were completely absent with no accessory tendon 6% were absent but an accessory tendon inserted at the MP joint 4% had 2 EPB tendons - with variable insertions |
EPB: Extensor pollicis brevis; EPL: Extensor pollicis longus.
CASE REPORT
A 64-year-old right handed man had sustained a right wrist scaphoid fracture in 1969 which went on to develop a scaphoid nonunion advanced collapsed deformity (SNAC wrist) with arthritic changes and a large bone spur from the dorsal scaphoid. Nevertheless, he had no wrist pain and the right wrist never bothere him enough to warrant treatment. Six weeks prior to presentation, he was reaching for something and felt a pop in his right wrist. His physician referred him for hand surgery evaluation. On physical examination his right wrist extended to 30 degrees and flexed to 30 degrees compared to 45 degrees and 70 degrees respectively on the left wrist. His right wrist had bony enlargement dorsally on the radial side, but was non-tender and there was no pain with motion. His EPL tendon was noted to be completely ruptured. However, his EPB tendon could visibly fully extend both the thumb MP and IP joints (Figures 1, 1 and 3). His active thumb motion was 0-60 degrees at the MP joint and 15 degrees of hyperextension to 50 degrees of flexion at the IP joint. The only difference between the right and left thumbs was that when his hands were put flat on the table, he was unable to fully lift the right thumb up off the table compared to the left side (Figure 4 and Video core tip 1). X-rays of his right wrist revealed a SNAC wrist with a large bony osteophyte protruding dorsally from the scaphoid. The impression was that the EPL tendon had ruptured over the dorsal spike from the scaphoid as this was directly underlying the normal course of the EPL tendon and there was concern that his wrist extensors might also rupture over the bony spike. Therefore, a magnetic resonance imaging of the right wrist was obtained which revealed that the extensor carpi radialis longus (ECRL) tendon was 50% eroded over the dorsal spike of the scaphoid nonunion and that the EPL tendon had completely ruptured. After discussion with the patient, it was decided to perform a surgical procedure to debride the bone spike from the scaphoid nonunion that could potentially lead to rupture of his wrist extensor tendons, having already ruptured the EPL tendon. Since he had no pain in the wrist nor deficits of thumb IP joint extension we did not plan to perform any procedure to address the arthritis or the EPL rupture. At the time of surgery, which was performed under a regional anesthetic, the EPL tendon was seen to be completely ruptured with the proximal end retracted and the ECRL tendon was 50% eroded. The sharp spikes from the scaphoid nonunion were debrided and the capsule was closed over the scaphoid as a soft tissue interposition between the bone and the wrist extensor tendons. Post-operatively, he was immobilized for 10 d at which time the sutures were removed and he resumed normal activities without pain. At 3 mo follow up he had no complaints of pain and was using his hand and wrist normally.
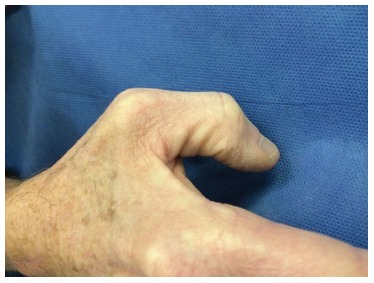
Figure 1.

Patient demonstrating full thumb MP and IP extension using only extensor pollicis brevis tendon.
Figure 3.
Patient demonstrating thumb MP and IP flexion.
Figure 4.

Extensor pollicis brevis tendon extending thumb (Video core tip 1).
Figure 2.

Examiner’s finger pointing to extensor pollicis brevis tendon which is extending thumb at MP and IP joints.
DISCUSSION
To the best of our knowledge, virtually all previously reported cases of EPL tendon rupture have been associated with deficits of thumb interphalangeal joint extension. Anatomical dissections have shown the EPB tendon insertion to be highly variable with insertions on the thumb proximal phalanx as well as the extensor hood and the distal phalanx (Table 1). It is, therefore, reasonable to assume that a minority of EPL tendon ruptures may be clinically overlooked owing to the ability of the EPB tendon to fully extend the thumb interphalangeal joint. These cases may never come to the attention of physicians since, while the patients may experience a pop and temporary discomfort, their thumbs may continue to work fairly normally. The cases presenting to orthopedic and hand surgeons, therefore, may represent patients in whom the EPB tendon is unable to fully compensate for the function of the EPL tendon. This case report highlights the anatomical ability of the EPB tendon to fully substitute for the EPL tendon with respect to thumb interphalangeal joint extension. EPL tendon rupture may therefore be more common than is currently appreciated since cases such as these may never present for treatment.
COMMENTS
Case characteristics
A 64-year-old man with rupture of the extensor pollicis longus (EPL) tendon presenting with preserved ability to full extend his thumb at the interphalangeal and metacarpophalangeal joints.
Clinical diagnosis
The EPL tendon was noted to be ruptured both visibly, on examination, on magnetic resonance imaging (MRI) and at the time of surgical exploration, and yet the extensor pollicis brevis (EPB) tendon was able to fully extend the thumb at the IP and MP joints.
Differential diagnosis
The EPB tendon was clearly seen extending the thumb, likely due to its insertion on the extensor hood and/or distal phalanx.
Imaging diagnosis
MRI showed EPL tendon rupture.
Treatment
The prominent bony outgrowth that had caused the EPL rupture was surgically excised so it did not further erode the wrist extensor tendons.
Related reports
Virtually all previously reported series of EPL tendon rupture had deficits of IP thumb joint extension requiring surgery with tendon transfer or grafting. This case report highlights that tendon transfer may not always be required for EPL tendon rupture.
Term explanation
The EPB tendon and the EPL tendon both extend the thumb.
Experiences and lessons
There may be many patients with EPL tendon rupture who do not require tendon transfer due to the ability of the EPB to extend the thumb IP joint.
Peer-review
This is a concise and well written report which is of surgical interest. The video is a useful adjunct.
Footnotes
Institutional review board statement: Attached-no formal IRB approval needed for case report.
Informed consent statement: The patient involved in this study gave his verbal consent to inclusion in this case report.
Conflict-of-interest statement: The authors have no conflict of interests.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Peer-review started: February 1, 2016
First decision: April 15, 2016
Article in press: May 9, 2016
P- Reviewer: Musumeci G, Wharton R S- Editor: Ji FF L- Editor: A E- Editor: Wu HL
References
- 1.Kim CH. Spontaneous rupture of the extensor pollicis longus tendon. Arch Plast Surg. 2012;39:680–682. doi: 10.5999/aps.2012.39.6.680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hu CH, Fufa D, Hsu CC, Lin YT, Lin CH. Revisiting spontaneous rupture of the extensor pollicis longus tendon: eight cases without identifiable predisposing factor. Hand (N Y) 2015;10:726–731. doi: 10.1007/s11552-015-9746-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Stein AH. Variations of the tendons of insertion of the abductor pollicis longus and the extensor pollicis brevis. Anat Rec. 1951;110:49–55. doi: 10.1002/ar.1091100106. [DOI] [PubMed] [Google Scholar]
- 4.Dawson S, Barton N. Anatomical variations of the extensor pollicis brevis. J Hand Surg Br. 1986;11:378–381. doi: 10.1016/0266-7681(86)90161-0. [DOI] [PubMed] [Google Scholar]
- 5.Brunelli GA, Brunelli GR. Anatomy of the extensor pollicis brevis muscle. J Hand Surg Br. 1992;17:267–269. doi: 10.1016/0266-7681(92)90112-f. [DOI] [PubMed] [Google Scholar]
- 6.Kulshreshtha R, Patel S, Arya AP, Hall S, Compson JP. Variations of the extensor pollicis brevis tendon and its insertion: a study of 44 cadaveric hands. J Hand Surg Eur Vol. 2007;32:550–553. doi: 10.1016/J.JHSE.2007.04.013. [DOI] [PubMed] [Google Scholar]
- 7.Alemohammad AM, Yazaki N, Morris RP, Buford WL, Viegas SF. Thumb interphalangeal joint extension by the extensor pollicis brevis: association with a subcompartment and de Quervain’s disease. J Hand Surg Am. 2009;34:719–723. doi: 10.1016/j.jhsa.2008.12.015. [DOI] [PubMed] [Google Scholar]
- 8.Shigematsu S, Shimizu H, Beppu M, Hirata K. Anatomy of the extensor pollicis brevis associated with an extension mechanism of the thumb metacarpophalangeal joint. Hand Surg. 2014;19:171–179. doi: 10.1142/S0218810414500166. [DOI] [PubMed] [Google Scholar]