

Abstract
AIM: To investigate the association between adherence to health recommendations and detection of advanced colorectal neoplasia (ACN) in colorectal cancer (CRC) screening.
METHODS: A total of 14832 women and men were invited to CRC screening, 6959 in the fecal immunochemical test arm and 7873 in the flexible sigmoidoscopy arm. These were also sent a self-reported lifestyle questionnaire to be completed prior to their first CRC screening. A lifestyle score was created to reflect current adherence to healthy behaviors in regard to smoking, body mass index, physical activity, alcohol consumption and food consumption, and ranged from zero (poorest) to six (best). Odds ratios (ORs) and 95%CIs were calculated using multivariable logistic regression to evaluate the association between the single lifestyle variables and the lifestyle score and the probability of detecting ACN.
RESULTS: In all 6315 women and men completed the lifestyle questionnaire, 3323 (53%) in the FIT arm and 2992 (47%) in the FS arm. This was 89% of those who participated in screening. ACN was diagnosed in 311 (5%) participants of which 25 (8%) were diagnosed with CRC. For individuals with a lifestyle score of two, three, four, and five-six, the ORs (95%CI) for the probability of ACN detection were 0.82 (0.45-1.16), 0.43 (0.28-0.73), 0.41 (0.23-0.64), and 0.41 (0.22-0.73), respectively compared to individuals with a lifestyle score of zero-one. Of the single lifestyle factors, adherence to non-smoking and moderate alcohol intake were associated with a decreased probability of ACN detection compared to being a smoker or having a high alcohol intake 0.53 (0.42-0.68) and 0.63 (0.43-0.93) respectively.
CONCLUSION: Adopted healthy behaviors were inversely associated with the probability of ACN detection. Lifestyle assessment might be useful for risk stratification in CRC screening.
Keywords: Screening, Colorectal neoplasia, Lifestyle, Prevention, Health recommendations
Core tip: Colorectal cancer (CRC) is a highly prevalent disease, developing from adenomas. In primary prevention of CRC, following public health recommendations such as non-smoking, normal body weight, physical activity, limited alcohol consumption and healthy diet is important. In the present study, we showed that adherence to multiple health recommendations was associated with decreased risk of detecting advanced colorectal neoplasia (ACN) in CRC screening. Regarding single health recommendations, non-smoking and moderate alcohol consumption were the most important lifestyle factors associated with low risk of ACN. Lifestyle assessment in CRC screening may therefore be used as a tool in risk stratification of participants.
INTRODUCTION
Worldwide and in Norway, colorectal cancer (CRC) is the second and third most common cancer type in women and men, respectively[1]. In Norway, approximately 4000 new cases of CRC are diagnosed each year[2]. CRC usually develops from an adenoma within 10-15 years on average, but very few adenomas (less than 10%) may progress to CRC within a lifetime[3,4]. Still, early detection and removal of adenomas by screening may prevent CRC. Screening for CRC by either fecal immunochemical test (FIT), flexible sigmoidoscopy (FS) or guaiac-based fecal occult blood test (gFOBT) has been shown to reduce CRC mortality (FIT, FS and gFOBT) and CRC incidence (FS only)[5-10]. Also, favorable lifestyle factors such as abstention from smoking, normal body mass, physical activity, limited alcohol consumption, and healthy dieting have been associated with a reduced risk of colorectal adenomas and CRC[11,20]. Only a few studies have investigated the association between the number of healthy lifestyle factors and the risk of advanced colorectal neoplasia (ACN) in an average-risk population[21,22]. When planning a national CRC screening program, it is important to identify and estimate the predictive value of lifestyle characteristics associated with detection of ACN. Stratifying of participants according to their risk profile will aid open possibilities for personalized CRC screening.
The aim of the present study was to investigate the association between the number of adherence of healthy lifestyle behaviors (based on Norwegian and international health recommendations) at the time of invitation to screening, and the probability of detecting ACN. Further, we aimed to investigate whether it was possible to predict screen-detected ACN based on single modifiable lifestyle factors. The present study is a lifestyle sub-study within the Bowel Cancer Screening in Norway (BCSN) - a randomized pilot study on a national program.
MATERIALS AND METHODS
Study population
The BCSN compares two screening modalities; five biennial rounds of FIT for occult blood in stools and a single FS[23,24]. A total of 140000 women and men aged 50-74 at the time of randomization from two geographically defined areas in South-East Norway are randomly assigned (1:1 ratio) to one of the two screening modalities. Invitations are scheduled from 2012 to 2018.
From November 2012 to September 2013, a total of 14832 individuals (6959 in the FIT arm and 7873 in the FS arm) were additional invited to a separate lifestyle sub study (Figure 1). These were sent a two-page lifestyle questionnaire (LSQ) along with the invitation to the CRC screening. The LSQ was to be completed prior to the first CRC screening on paper or online prior to the availability of the screening results.
Figure 1.

Flow chart of the participation in the screening and responders to the lifestyle questionnaire in the lifestyle sub-study of the bowel cancer screening in norway-a pilot study. FIT: Fecal Immunochemical Test, FS: Flexible Sigmoidoscopy; LSQ: Lifestyle questionnaire.
Examination procedures (outcome)
Participants assigned to FIT were mailed a self-administered kit with which they obtained a stool sample and returned by mail to the laboratory. A test result of ≥ 75 μg hemoglobin/L buffer was considered a positive FIT. In the present study, FIT results were based on the first round out of five. FS was defined as positive if one of the following was detected or suspected: (1) any polyp ≥ 10 mm in diameter; (2) any adenoma with villous histology or high-grade dysplasia; (3) ≥ 3 adenomas; or (4) cancer. Participants with a positive screening result were referred to a follow-up colonoscopy. Based on the findings from the FIT, FS and follow-up colonoscopy, the participants were categorized into the following categories: (1) no adenomas (negative findings, non-neoplastic findings, other polyps); (2) low-risk adenomas (one or two adenomas with low-grade dysplasia of size < 10 mm in diameter); (3) high-risk adenomas (≥ 3 small adenomas or any adenoma of size ≥ 10 mm in diameter or adenomas with villous/tubulovillous/severe dysplasia); and (4) CRC [25]. ACN was defined as high-risk adenomas or CRC and served as the outcome. Individuals with low-risk adenomas or no adenomas were not considered to have ACN.
Exposure information - the LSQ
The LSQ consisted of questions copied from previous national surveys[26,27] and previously used in the Norwegian Colorectal Cancer Prevention study (NORCCAP)[28,29]. In the LSQ, participants were asked about their ethnicity, marital status and years of formal education (Table 1). Participants were also asked to report smoking habits, weight, height, physical activity, and their consumption of alcohol and selected dietary items during the previous year. Reply options for smoking status were: “yes, daily”, “yes, occasionally”, “former”, and “never smoked”. Former smokers were further asked to state the number of years since smoking cessation. Three questions were asked regarding physical activity: “Have you during the last three years had any chronic disease that limits your physical activity?” (yes/no), and “How many times per week are you physically active for 30 min (1) with light or moderate intensity; and (2) with high intensity?”. The reply options ranged from “never” to “more than seven times per week”. Alcohol consumption was determined by two questions: (1) “How often have you consumed alcohol during the last year?”, with reply options that ranged from “never” to “four-seven times per week”; and (2) “When consuming alcohol, how many glasses do you usually drink?”. Consumption of fruit, berries and vegetables was determined by three separate questions regarding (1) fruit and berries; (2) raw vegetables; and (3) boiled vegetables. The consumption of red and processed meat was ascertained by three questions, where participants indicated their consumption at dinner of (1) steak, chops or similar; (2) hamburgers and dishes with minced meat; and (3) sausages. Consumption of fish was determined by one question on fatty fish. Bread consumption was ascertained by questions regarding the number of slices of bread with (1) a non-whole meal; (2) a partly whole meal; and (3) a whole meal. For the dietary items except bread, six frequency alternatives that ranged from “never/rarely” to “more than three servings per day” were given. For bread consumption, more than seven slices per day was the maximum.
Table 1.
Characteristics of participant’s n (%)
| Variable | Total (n = 6315)1 % column | Advanced colorectal neoplasia (n = 311) % row |
| Screening arm | ||
| Fecal immunochemical test | 3323 (53) | 85 (3) |
| Flexible sigmoidoscopy | 2992 (47) | 226 (8) |
| Age | ||
| mean (SD) | 62.0 (7.0) | 64.2 (6.9) |
| Sex | ||
| Female | 3255 (52) | 118 (4) |
| Male | 3060 (48) | 193 (6) |
| Occupation | ||
| Employed | 3186 (50) | 115 (4) |
| Unemployed | 2944 (47) | 189 (6) |
| Missing | 185 (3) | 7 (4) |
| Education length | ||
| Primary school | 1008 (16) | 58 (6) |
| High school | 2388 (38) | 132 (5) |
| University/college studies of min. 2 yr | 2636 (42) | 104 (4) |
| Missing | 283 (4) | 17 (6) |
| Ethnicity | ||
| Norwegian | 5887 (93) | 295 (5) |
| Not norwegian | 361 (6) | 12 (3) |
| Missing | 67 (1) | 4 (6) |
| Marital status | ||
| Single, widowed, divorced | 1195 (19) | 62 (5) |
| Married, living together | 5032 (80) | 247 (5) |
| Missing | 88 (1) | 2 (2) |
| Chronic disease2 | ||
| Yes | 1593 (26) | 86 (5) |
| No | 4507 (74) | 212 (5) |
| Missing | 215 (3) | 13 (6) |
| Whole meal bread slices per day | ||
| < 1.5 | 1293 (20) | 88 (7) |
| 1.5 | 1895 (30) | 83 (4) |
| 3.5 | 2175 (34) | 101 (5) |
| > 3.5 | 928 (15) | 38 (4) |
| Missing | 24 (0) | 1 (4) |
The number of replies may not sum to the total due to incomplete replies on the lifestyle questionnaire;
Chronic disease was asked as: have you doing the last 3 years had some chronic disease that limited your physical activity (e.g., problem with the hip or cardiovascular diseases) Demographic characteristics and whole meal bread consumption for participants in the lifestyle sub-study of the Bowel Cancer Screening in Norway - a pilot study.
Lifestyle variables
Individuals with certain smoking habits were divided into two groups: (1) smokers comprised current smokers, occasional smokers and those with smoking cessation ≤ 10 years ago; and (2) non-smokers who had never smoked or had stopped smoking > 10 years ago[30]. Body mass index (BMI, kg/m2) was calculated from self-reported weight (kg) and height (cm). The two questions on physical activity (light/moderate and high intensity) were summed to the total number of times per week for 30 min or more. Alcohol consumption (glasses per week) was calculated by multiplying the answers to the two questions. The consumption of fruit and berries, raw vegetables and boiled vegetables was summed to a total fruit and vegetables consumed (F&V, servings per day). Consumption of total red and processed meat for dinner (R&P meat, servings per week) was calculated by summing the answers to the three questions on meat.
Categorization of variables
A lifestyle score was generated to reflect the number of favorable lifestyle factors fulfilled. The score was based on the following factors: smoking habits, BMI, physical activity, and consumption of alcohol, F&V, R&P meat, and fatty fish. These factors were chosen for their modifiable character and for being central in Norwegian and international health recommendations. Each of the single lifestyle factors was dichotomized to reflect adherence to health recommendations[31-33]. Each participant was assigned one point for each fulfilled lifestyle criterion, except F&V and fish for which both had to be fulfilled to earn one point (Table 2). The total number of points in the lifestyle score ranged from zero (poorest) to six (best) (Table 3).
Table 2.
Risk of advanced colorectal neoplasia by single lifestyle factors n (%)
| Variable | Total (n = 6315) % column1 | Advanced colorectal neoplasia (n = 311) % row | Lifestyle point2 | OR, (95%CI)3 |
| Smoking4 | ||||
| Smoker | 1988 (31) | 140 (7) | 0 | 1.00 (Ref) |
| Non-smoker | 4311 (68) | 171 (4) | 1 | 0.53 (0.42-0.68) |
| Missing | 16 (0) | 0 (0) | ||
| Body Mass Index5 | ||||
| ≥ 25.0 | 3658 (59) | 205 (6) | 0 | 1.00 (Ref) |
| < 25.0 | 2542 (41) | 97 (4) | 1 | 0.78 (0.60-1.01) |
| Missing | 115 (2) | 9 (8) | ||
| Physical activity 30 min, times per week | ||||
| < 7 | 4480 (71) | 238 (5) | 0 | 1.00 (Ref) |
| ≥ 7 | 1504 (24) | 58 (4) | 1 | 0.81 (0.60-1.09) |
| Missing | 331 (5) | 15 (5) | ||
| Alcohol, glasses per week | ||||
| ≤ 14 for male, ≤ 7 for female) | 5525 (88) | 264 (5) | 1 | 0.63 (0.43-0.93) |
| Above | 514 (8) | 34 (7) | 0 | 1.00 (Ref) |
| Missing | 276 (4) | 13 (5) | ||
| Fruits and vegetables, servings per day | ||||
| < 3 | 4621 (73) | 244 (5) | 0 | 1.00 (Ref) |
| ≥ 3 | 1446 (23) | 52 (4) | 0.5 | 0.93 (0.67-1.27) |
| Missing | 248 (4) | 15 (6) | ||
| Red and processed meat, servings per week | ||||
| > 4 | 2059 (32) | 108 (5) | 0 | 1.00 (Ref) |
| ≤ 4 | 4093 (65) | 196 (5) | 1 | 0.98 (0.76-1.26) |
| Missing | 163 (3) | 7 (4) | ||
| Fatty fish, servings per week | ||||
| < 1 | 1257 (20) | 78 (6) | 0 | 1.00 (Ref) |
| ≥ 1 | 5023 (79) | 232 (5) | 0.5 | 0.79 (0.60-1.05) |
| Missing | 35 (1) | 1 (3) | ||
| C-statistics | 0.72 (0.69-0.75) |
The number of replies may not sum to the total due to incomplete replies on the lifestyle questionnaire;
One point for each lifestyle adherence, except only 1 point if adherence to both: fatty fish and fruits and vegetables;
Models are adjusted for: age (continuously), screening arm (flexible sigmoidoscopy, fecal immunochemical), gender (women, men), center (Moss, Bærum), education (primary school, high school, university/college studies of minimum 2 yr) and whole meal bread. Lifestyle factors (Body Mass Index, smoking, alcohol, physical activity, fruits and vegetables, red and processed meat and fatty fish) were mutually adjusted for each other;
18% current smoker, 14% ≤ 10 yr stopped, 28% > 10 yr stopped, 40% never smokers;
43% had a Body Mass Index of 25.0-30.0; 16% had a Body Mass Index of > 30.0. Lifestyle characteristics, point for the lifestyle score, odds ratio (OR) and 95%CI between the single lifestyle factors and the risk of advanced colorectal neoplasia by multivariable logistic regression for participants in the lifestyle sub-study of the Bowel Cancer Screening in Norway - a pilot study.
Table 3.
Risk of advanced colorectal neoplasia by the lifestyle score n (%)
| Total (n = 6315) % column1 | Advanced colorectal neoplasia (n = 311), n | Absolute risk estimates per 10004 | OR, (95%CI)2 | P trend5 | |
| Lifestyle score3 | < 0.001 | ||||
| 0-1 | 371 (6) | 32 | 86.3 | 1.00 (Ref) | |
| 2 | 1248 (20) | 92 | 73.7 | 0.82 (0.45-1.16) | |
| 3 | 1749 (27) | 71 | 40.6 | 0.43 (0.28-0.73) | |
| 4 | 1312 (21) | 46 | 35.1 | 0.41 (0.23-0.64) | |
| 5-6 | 684 (11) | 21 | 30.7 | 0.41 (0.22-0.73) | |
| Mising | 951 (15) | 49 | |||
| C-statistics | 0.71 (0.68-0.74) |
The number of replies may not sum to the total due to incomplete replies on the lifestyle questionnaire;
The model was adjusted for age (continuously), screenings arm (fecal immunochemical test, flexible sigmoidoscopy), gender (women, men), center (Moss, Bærum), education (primary school, high school, university/college studies of minimum 2 years) and whole meal bread;
One point for each lifestyle adherence, except only 1 point if adherence to both: fatty fish and fruits and vegetables;
Absolute risk calculated: with in each score: (n ACN/Total n)*1000;
P trend was calculated using the lifestyle score as continuous. Lifestyle score characteristics, odds ratio (OR) and 95%CI for the risk of advanced colorectal neoplasia by multivariable logistic regression for participants in the lifestyle sub-study of the Bowel Cancer Screening in Norway - a pilot study.
The Norwegian health recommendation for F&V is a minimum of five servings per day[31]. However, only 4.5% of the participants in the present study reported this value. According to a national survey, 25% of the Norwegian population fulfill the recommendation for F&V[34]. As 25% of the participants in our study had a total consumption of three or more servings per day, we used this cut off value to mark favorable F&V consumption in our analyses.
Statistical analysis
The odds ratio (OR) and 95%CIs were calculated using multivariable logistic regression models to evaluate the association between single lifestyle factors and the lifestyle score with the risk of ACN. Single lifestyle factors were analyzed as dichotomous variables using values that did not reach the lifestyle score point as the reference category. To gain enough participants for the reference group, the scores of zero or one were pooled (zero-one) in the lifestyle score analyses. Statistical models that examined the association between single lifestyle factors and the risk of ACN were mutually adjusted for the remaining single lifestyle factors. Moreover, all multivariable models were adjusted for gender, age at invitation (continuous), years of formal education (primary school, high school, university/college studies of minimum 2 years), screening modality (FIT or FS), screening center (Moss or Bærum Hospital) and whole meal bread consumption (< 1.5, 1.5, 3.5, or > 3.5 slices per day). These factors were selected based on a priori knowledge of the association of these factors with CRC[12,14,35] and colorectal adenomas[15-19,36]. In spite of the convincing evidence of an inverse association with the risk of CRC, we included whole meal bread consumption as a covariate and not in the lifestyle score. This was based on the uncertainty of bread consumption alone to mark dietary fiber/wholegrain intake.
Omitted values for the lifestyle factors in question were treated as fixed/dummy values. If a participant had a missing value in a lifestyle factor used to create the lifestyle score, this factor was considered missing in the lifestyle score for that participant.
Multivariable restricted cubic spline logistic regression models with three knots were used to analyze the functional form, and P trend, of the relationship between single lifestyle factors as continuous (BMI, physical activity, alcohol consumption, F&V and R&P meat) and the probability of ACN[37].
C-statistics were calculated to examine how well the multivariable logistic regression models discriminated between participants who were and were not diagnosed with ACN, estimating C. C is an estimate for the sensitivity and specificity of the statistical model[38].
In the sensitivity analysis, we tested the effect of the lifestyle score on the risk of ACN by including fewer than six lifestyle factors. A change in the order of the included factors was also tested. We then stratified the analyses for gender, smoking and screening modality. Likelihood ratio tests were also performed to test for effect modification.
Absolute risk was calculated for each lifestyle score category as well.
Analyses were performed using STATA™ software, version 13.1 (Stata Corp, College Station, Texas, United States) and R software (The R Foundation for Statistical Computing Platform 2014, Free Software Foundation, Boston, MA, United States). The statistical methods of this study were reviewed by statistician Edoardo Botteri from Department bowel cancer screening, Cancer Registry of Norway.
Ethics
The Regional Research Ethics Committee of South-East Norway and the Norwegian Data Inspectorate approved the study protocol (approval No. 2011/1272). The participants gave their consent to participate in the lifestyle study by completing and returning the mailed questionnaire.
RESULTS
In all, 6315 participants were included in the present study; 53% (n = 3323) were in the FIT arm and 47% (n = 2992) were in the FS arm (Figure 1). The participation rate for both the screening examination and successful completion of the LSQ was 43% (48% in the FIT arm and 38% in the FS arm). ACN was diagnosed in 311 (4.9%) participants of which 25 (8%) were diagnosed with CRC.
A higher proportion of participants who were diagnosed with ACN were unemployed, smokers, and had a BMI ≥ 25 kg/m2 compared with participants without ACN (Tables 1 and 2).
Age at invitation, male gender and randomization to FS screening compared with FIT screening were associated with an increased risk of ACN (results not shown). The adjusted OR for the risk of ACN was 0.53 (95%CI: 0.42-0.68) for non-smokers compared with smokers. The adjusted OR for the risk of ACN was 0.63 (95%CI: 0.43-0.93) in individuals with moderate alcohol consumption compared with those with a consumption above the moderate level. No significant associations were observed between BMI, the single dietary factors or physical activity and the risk of ACN (Table 2).
Figure 2 shows the functional form of the relationship between single continuous lifestyle factors (except smoking and consumption of fatty fish) and the probability of ACN. Based on the multivariable restricted cubic spline logistic regression, continuous BMI (p-trend) was associated with an increased probability of ACN (Figure 2).
Figure 2.
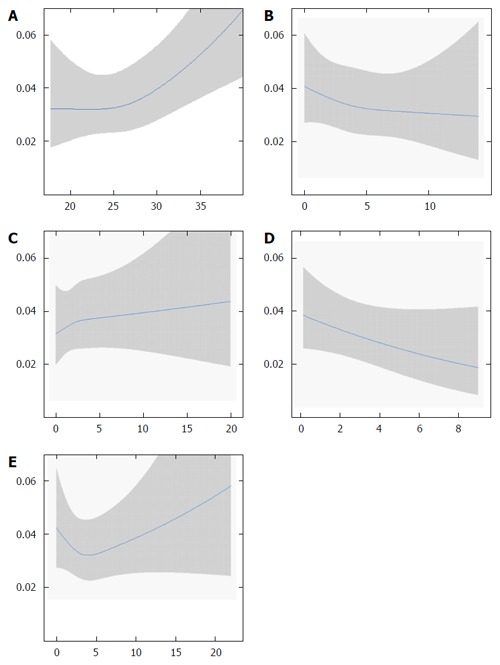
Relationship between advanced colorectal neoplasia and Body Mass Indexa (A) physical activity(B) alcohol consumption(C) fruit and vegetable consumption (D); and (E) red and processed meat consumption. The relationship is modeled by cubic splines logistic (continuous line) with 3 knots. The model is based on 95%CI, which are reported by the grey areas. All models are adjusted for: age (continuously), screening arm (flexible sigmoidoscopy, fecal immunochemical), gender (women, men), center (Moss, Bærum), education (primary school, high school, university/college studies of minimum 2 year) whole meal bread, fatty fish and smoking (smoker, non-smoker). The lifestyle factors (BMI, physical activity, alcohol consumption, fruit and vegetables and red and processed meat) were mutually adjusted for each other. A: BMI 16.5-40 (> 40 does not appear in the figure); B: Physical activity 0-14 times for 30 min per week; C: Alcohol consumption 0-30 glasses per week; D: Total fruit and vegetable consumption 0-9 servings per day; E: Red and processed meat consumption 0-15 servings per week. aP < 0.001, increase/decrease in the regression coefficient significantly different from 0.
The lifestyle score was inversely associated with the risk of ACN, P trend < 0.001. The absolute number of individuals with ACN decreased from 86.3 to 30.7 per 1000 by increase of the lifestyle score from zero-one to four or five-six. The adjusted OR for ACN was 0.41 (95%CI: 0.22-0.73) for participants with a lifestyle score of five-six compared with those with a score of zero-one (Table 3).
Sensitivity analyses, which included fewer than six lifestyle factors and tested the order of the lifestyle factors that were included in the score showed that non-smoking was the most important factor in the reduction of the OR for ACN. Lowest risk for ACN was associated with adherences to the four lifestyle factors; non-smoking, normal BMI, adequate physical activity and moderate alcohol consumption, compared to adherence to none or only one of these behaviors (OR = 0.31, 95%CI: 0.17-0.59). The addition of points for a healthy diet did not reduce the risk of ACN further. Results did not change when stratifying for gender (results not shown). When stratifying for smoking status, the risk of ACN was reduced for non-smokers having a moderate alcohol consumption, compared to non-smokers with a consumption above moderate 0.76 (95%CI: 0.33-0.99). For smokers the risk of ACN was reduced for those with a high F&V intake 0.45 (95%CI: 0.23-0.88) compared to those with a low F&V intake. Results for the remaining variables were not changed when stratifying for smoking status. When the results were stratified according to screening modality, we observed a significant inverse association between the lifestyle score and ACN only in the FS arm. Results from the FIT arm showed a similar trend but did not reach statistical significance. There was no indication of effect modification by the screening arm in the association between the lifestyle score or the single lifestyle factors, and ACN risk (P values for interaction ranged from 0.178 to 0.984).
The results from the C-statistics indicate that the models used were acceptable in the discrimination between participants with and without ACN, as the C values were between 0.70-0.80[39]: C-statistics = 0.72 (95%CI: 0.69-0.75) for ACN and single lifestyle factors, C-statistics = 0.71 (95%CI: 0.68-0.74) for ACN and the lifestyle score (Table 2 and 3).
DISCUSSION
In the present study, we observed a low risk of ACN in CRC screening participants who fulfilled several healthy lifestyle factors reflecting adherence to public health recommendations. The present study suggests that favorable health behavior, particularly non-smoking and moderate alcohol consumption predicts a low risk of CRC in a general population. These results highlight the potential of lifestyle assessment as a tool in risk stratification of participants in CRC screening.
Studies that investigate the association between lifestyle factors and the risk of ACN in a CRC screening setting are unusual. In the FS-based NORCCAP study, similar associations were observed between smoking, physical activity, and consumption of F&V, R&P meat and fatty fish and the risk of ACN[29], but no information on alcohol was collected. A Chinese CRC screening study[40] and an American case-control study[21] investigated the association between ACN and a lifestyle score. Our results are in agreement with results from these two studies, although some differences were seen in the factors that were considered for the lifestyle scores. The Chinese study included both non-modifiable factors (e.g., family history of CRC, diabetes, age and gender) along with the modifiable risk factors smoking and BMI in their scoring system[40]. The American study included calcium intake and the use of non-steroidal anti-inflammatory drugs in the lifestyle score[21].
Three European studies and one American cross-sectional study on colonoscopy screening concluded that through a set of participant characteristics, it might be possible to identify a high-risk population for adenomas and to target that population for CRC-screening[41-44]. These studies included both modifiable and non-modifiable risk factors such as family history of CRC, previous detection of polyps, diabetes and FIT results. Based on the C-statistics that were obtained in these previous European[41-43], Chinese[40] and American[44,45] studies, our model that included only modifiable risk factors for CRC was equally able to discriminate between the participants diagnosed and not diagnosed with ACN. This suggests that modifiable lifestyle assessment in CRC screening could be used as a tool in risk stratification of participants and to identify high-risk participants in CRC-screening. Two large prospective cohort studies, one in the European Prospective Investigation into Cancer and Nutrition and a Danish study, showed that lifestyle scores based on modifiable factors similar to those in the present study predict the risk of future CRC[11,13]. The present study with the cross-sectional design is not comparable with those studies. However, we observed similar associations between current lifestyle and ACN to those in the large cohort studies, although current lifestyle at the time of screening might not represent the lifestyle at the time of onset of adenoma development.
The present study has several strengths. The population registry based randomization limits the risk of selection bias. Compared to other European population-based trials in CRC screening[41,46], compliance to complete the LSQ among screening participants (89%) was high. This may have reduced the risk of selection bias, suggesting that the results are representative for CRC screening participants. Information bias was unlikely due to the study design that entailed the completion of the LSQ before the screening results were available. The limitations of the present study include that we had no information on potential confounders such as energy intake, use of non-steroidal anti-inflammatory drugs and hormone therapy in women, or family history of CRC[14,47,48]. However, because BMI and physical activity were included in the statistical models, the risk of confounding by energy intake should be limited.
The specific questions in the LSQ have been used in other validated questionnaires[26,27], however, the brevity of the LSQ, which was designed to require less than 10 min for completion, may have sacrificed details on dietary consumption. The overall participation rate of 43% might question the present study’s representativeness of the general Norwegian population. Prevalence of smoking (18%, including occasional smokers) in the present study compared to the 15%-20% daily smokers in the Norwegian population of similar age[49] suggests representative lifestyle characteristics in the study population. We acknowledge that FIT and FS as screening modalities might have caused some false negative screening results (misclassification) because one round of FIT has limited sensitivity to discover ACN, and FS only involves the distal segments of the colon[50,51]. Any misclassification might have attenuated the association between the lifestyle factors and the risk of ACN. This added to the brevity of the LSQ might also be a reason why no significant linear association was observed for the single lifestyle factors. Furthermore, the lack of significant associations between the single lifestyle factors, the lifestyle score, and ACN in the stratified FIT arm might be explained by misclassification because it was based on only the first of five FIT rounds.
Alternative lifestyle scores based on quartiles of the single lifestyle factors could have been considered. However, quartiles are not as easy interpretable for the general population as the present lifestyle score which reflects adherence to public health guidelines.
In summary, the simplicity of the lifestyle score, which was created to reflect healthy lifestyle behaviors in the present study, makes it an easy tool to implement in CRC screening. This score provides straightforward information on the probability of detecting ACN in a general population. Furthermore, the lifestyle score could be considered used as a risk stratification tool when predicting the risk of detecting ACN in CRC screening. We showed that the probability of detecting ACN was 59% lower in screening participants having a score of minimum four compared to a score of zero-one. Based on this population-based screening study, the single lifestyle factor with the lowest probability of detecting ACN was non-smoking. However, moderate alcohol consumption was also effective for non-smokers and F&V for smokers. When the results from the present study are generalized, one should consider that the study was based only on Norwegians.
In conclusion, the present study suggests that the probability of detecting ACN in CRC screening is low in participants who adhere to multiple favorable lifestyle behaviors. Lifestyle assessment may be useful for risk stratification in CRC screening.
ACKNOWLEDGMENTS
The authors thanks the participants for participating in the study.
COMMENTS
Background
Single lifestyle factors are associated with the risk of colorectal adenomas and cancer. In the planning of a colorectal cancer (CRC) screening programs, it is important to estimate the predictive value of lifestyle factors for detection of advanced colorectal neoplasia (ACN).
Research frontiers
The aim of this study was to investigate whether detection of ACN was associated with the number of modifiable healthy lifestyle factors in CRC screening participants.
Innovations and breakthroughs
The present study shows that the number of adopted healthy lifestyle behaviors reflecting public health recommendations predicts the outcome in a CRC screening examination. Screening participants adhering to at least four healthy behaviors have 59% lower risk of ACN detected at screening, when compared to participants adhering to none or only one healthy behavior.
Applications
Adhering to several health recommendations is effective in the prevention of CRC. Assessment of lifestyle factors at CRC screening may be useful as a tool in risk stratification of participants.
Peer-review
CRC is one of the most common cancer types in both women and men. This is an important study, investigating whether detection of ACN was associated with the number of modifiable healthy lifestyle factors in CRC screening participants. The study shows a lower risk of ACN with increased number of healthy lifestyle factors. The results were interesting and the article is of great interest for the readers of the journal.
Footnotes
Institutional review board statement: The Regional Research Ethics Committee of South-East Norway and the Norwegian Data Inspectorate approved the study protocol (approval No. 2011/1272). Clinical Trials.gov: NCT01538550.
Informed consent statement: The participants gave their consent to participate in the lifestyle study by completing and returning the mailed questionnaire.
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Data sharing statement: Statistical code and dataset available from the corresponding author at (t.d.lange@medisin.uio.no) No additional data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Peer-review started: April 9, 2016
First decision: May 12, 2016
Article in press: June 13, 2016
P- Reviewer: Kajzrlikova IM, Hoffman A, Shi BM S- Editor: Qi Y L- Editor: A E- Editor: Wang CH
References
- 1.Globocan. Colorectal Cancer Estimated Incidence, Mortality and Prevalence Worldwide in 2012. IARC, 2012. Available from: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx.
- 2.Cancer Registry of Norway. Cancer in Norway 2013 - Cancer incidence, mortality, survival and prevalence in Norway. Norway: Oslo; 2015. [Google Scholar]
- 3.Muto T, Bussey HJ, Morson BC. The evolution of cancer of the colon and rectum. Cancer. 1975;36:2251–2270. doi: 10.1002/cncr.2820360944. [DOI] [PubMed] [Google Scholar]
- 4.Brenner H, Kloor M, Pox CP. Colorectal cancer. Lancet. 2014;383:1490–1502. doi: 10.1016/S0140-6736(13)61649-9. [DOI] [PubMed] [Google Scholar]
- 5.Holme Ø, Løberg M, Kalager M, Bretthauer M, Hernán MA, Aas E, Eide TJ, Skovlund E, Schneede J, Tveit KM, Hoff G. Effect of flexible sigmoidoscopy screening on colorectal cancer incidence and mortality: a randomized clinical trial. JAMA. 2014;312:606–615. doi: 10.1001/jama.2014.8266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Segnan N, Armaroli P, Bonelli L, Risio M, Sciallero S, Zappa M, Andreoni B, Arrigoni A, Bisanti L, Casella C, et al. Once-only sigmoidoscopy in colorectal cancer screening: follow-up findings of the Italian Randomized Controlled Trial--SCORE. J Natl Cancer Inst. 2011;103:1310–1322. doi: 10.1093/jnci/djr284. [DOI] [PubMed] [Google Scholar]
- 7.Atkin WS, Edwards R, Kralj-Hans I, Wooldrage K, Hart AR, Northover JM, Parkin DM, Wardle J, Duffy SW, Cuzick J, et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet. 2010;375:1624–1633. doi: 10.1016/S0140-6736(10)60551-X. [DOI] [PubMed] [Google Scholar]
- 8.Schoen RE, Pinsky PF, Weissfeld JL, Yokochi LA, Church T, Laiyemo AO, Bresalier R, Andriole GL, Buys SS, Crawford ED, et al. Colorectal-cancer incidence and mortality with screening flexible sigmoidoscopy. N Engl J Med. 2012;366:2345–2357. doi: 10.1056/NEJMoa1114635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Scholefield JH, Moss SM, Mangham CM, Whynes DK, Hardcastle JD. Nottingham trial of faecal occult blood testing for colorectal cancer: a 20-year follow-up. Gut. 2012;61:1036–1040. doi: 10.1136/gutjnl-2011-300774. [DOI] [PubMed] [Google Scholar]
- 10.Chiu HM, Chen SL, Yen AM, Chiu SY, Fann JC, Lee YC, Pan SL, Wu MS, Liao CS, Chen HH, et al. Effectiveness of fecal immunochemical testing in reducing colorectal cancer mortality from the One Million Taiwanese Screening Program. Cancer. 2015;121:3221–3229. doi: 10.1002/cncr.29462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kirkegaard H, Johnsen NF, Christensen J, Frederiksen K, Overvad K, Tjønneland A. Association of adherence to lifestyle recommendations and risk of colorectal cancer: a prospective Danish cohort study. BMJ. 2010;341:c5504. doi: 10.1136/bmj.c5504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Norat T, Aune D, Chan D, Romaguera D. Fruits and vegetables: updating the epidemiologic evidence for the WCRF/AICR lifestyle recommendations for cancer prevention. Cancer Treat Res. 2014;159:35–50. doi: 10.1007/978-3-642-38007-5_3. [DOI] [PubMed] [Google Scholar]
- 13.Aleksandrova K, Pischon T, Jenab M, Bueno-de-Mesquita HB, Fedirko V, Norat T, Romaguera D, Knüppel S, Boutron-Ruault MC, Dossus L, et al. Combined impact of healthy lifestyle factors on colorectal cancer: a large European cohort study. BMC Med. 2014;12:168. doi: 10.1186/s12916-014-0168-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.World cancer research fund and american institute for cancer research. Continuous Update Project Report. Food, Nutrition, Physical Actevity, and the Prevention of Colorectal Cancer. London, UK: Imperial College London; 2011. [Google Scholar]
- 15.Zhu JZ, Wang YM, Zhou QY, Zhu KF, Yu CH, Li YM. Systematic review with meta-analysis: alcohol consumption and the risk of colorectal adenoma. Aliment Pharmacol Ther. 2014;40:325–337. doi: 10.1111/apt.12841. [DOI] [PubMed] [Google Scholar]
- 16.Wolin KY, Yan Y, Colditz GA. Physical activity and risk of colon adenoma: a meta-analysis. Br J Cancer. 2011;104:882–885. doi: 10.1038/sj.bjc.6606045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hong S, Cai Q, Chen D, Zhu W, Huang W, Li Z. Abdominal obesity and the risk of colorectal adenoma: a meta-analysis of observational studies. Eur J Cancer Prev. 2012;21:523–531. doi: 10.1097/CEJ.0b013e328351c775. [DOI] [PubMed] [Google Scholar]
- 18.Ben Q, Sun Y, Chai R, Qian A, Xu B, Yuan Y. Dietary fiber intake reduces risk for colorectal adenoma: a meta-analysis. Gastroenterology. 2014;146:689–699.e6. doi: 10.1053/j.gastro.2013.11.003. [DOI] [PubMed] [Google Scholar]
- 19.Aune D, Chan DS, Vieira AR, Navarro Rosenblatt DA, Vieira R, Greenwood DC, Kampman E, Norat T. Red and processed meat intake and risk of colorectal adenomas: a systematic review and meta-analysis of epidemiological studies. Cancer Causes Control. 2013;24:611–627. doi: 10.1007/s10552-012-0139-z. [DOI] [PubMed] [Google Scholar]
- 20.Botteri E, Iodice S, Raimondi S, Maisonneuve P, Lowenfels AB. Cigarette smoking and adenomatous polyps: a meta-analysis. Gastroenterology. 2008;134:388–395. doi: 10.1053/j.gastro.2007.11.007. [DOI] [PubMed] [Google Scholar]
- 21.Fu Z, Shrubsole MJ, Smalley WE, Wu H, Chen Z, Shyr Y, Ness RM, Zheng W. Lifestyle factors and their combined impact on the risk of colorectal polyps. Am J Epidemiol. 2012;176:766–776. doi: 10.1093/aje/kws157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ma GK, Ladabaum U. Personalizing colorectal cancer screening: a systematic review of models to predict risk of colorectal neoplasia. Clin Gastroenterol Hepatol. 2014;12:1624–1634.e1. doi: 10.1016/j.cgh.2014.01.042. [DOI] [PubMed] [Google Scholar]
- 23.Bretthauer M, Hoff G. Comparative effectiveness research in cancer screening programmes. BMJ. 2012;344:e2864. doi: 10.1136/bmj.e2864. [DOI] [PubMed] [Google Scholar]
- 24.Cancer Registry of Norway. Bowel Cancer Screening in Norway - a pilot study 2012. Cited 2015-5-8. Avaailable from: URL: http://www.kreftregisteret.no/en/Cancer-prevention/Screening-for-colorectal-cancer/ [Google Scholar]
- 25.Lieberman DA, Rex DK, Winawer SJ, Giardiello FM, Johnson DA, Levin TR. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143:844–857. doi: 10.1053/j.gastro.2012.06.001. [DOI] [PubMed] [Google Scholar]
- 26.Johansson L, Solvoll K, Bjørneboe GE, Drevon CA. Under- and overreporting of energy intake related to weight status and lifestyle in a nationwide sample. Am J Clin Nutr. 1998;68:266–274. doi: 10.1093/ajcn/68.2.266. [DOI] [PubMed] [Google Scholar]
- 27.Søgaard Aj, Selmer R. The Oslo Study I and II. Norwegian Institute of Public Health, 2005 cited 2015-02-24. Available from: http://www.fhi.no/dav/736B5D55E9.rtf.
- 28.Berstad P, Løberg M, Larsen IK, Kalager M, Holme Ø, Botteri E, Bretthauer M, Hoff G. Long-term lifestyle changes after colorectal cancer screening: randomised controlled trial. Gut. 2015;64:1268–1276. doi: 10.1136/gutjnl-2014-307376. [DOI] [PubMed] [Google Scholar]
- 29.Larsen IK, Grotmol T, Almendingen K, Hoff G. Lifestyle as a predictor for colonic neoplasia in asymptomatic individuals. BMC Gastroenterol. 2006;6:5. doi: 10.1186/1471-230X-6-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.World Healh Organization. Fact sheet about health benefits of smoking cessation. Available from: http://www.who.int/tobacco/quitting/en_tfi_quitting_fact_sheet.pdf.
- 31.The Norwegian Directory of Health. Kostråd for å fremme folkehelsen og forebygge kroniske sykdommer. Available from: https://helsedirektoratet.no/Lists/Publikasjoner/Attachments/400/Kostrad-for-a-fremme-folkehelsen-og-forebygge-kroniske-sykdommer-metodologi-og-vitenskapelig-kunnskapsgrunnlag-IS-1881.pdf.
- 32.Wold Health Organization. Diet, nutrition and the prevention of chronic diseases. Available from: http://www.who.int/dietphysicalactivity/publications/trs916/download/en/ [PubMed]
- 33.Nordic Council of Ministers. Nordic Nutrition Recommendations, 5th edition, Nordic Council of Ministers, Copehagen, Denmark. Available from: https://www.norden.org/en/theme/nordic-nutrition-recommendation/nordic-nutrition-recommendations-2012.
- 34.Totland T, Melnæs B, Lundberg-Hallén N, Helland-Kigen K, Lund-Blix N, Myhre J, Johansen A, Løken E, Andersen L. Norkost 3 En landsomfattende kostholdsundersøkelse blant menn og kvinner i Norge i alderen 18-70 år, 2010-2011. Universitetet i Oslo, Mattilsynet and Helsedirektoratet 2012: 70. Available from: https://helsedirektoratet.no/Lists/Publikasjoner/Attachments/301/Norkost-3-en-landsomfattende-kostholdsundersokelse-blant-menn-og-kvinner-i-norge-i-alderen-18-70-ar-2010-11-IS-2000.pdf.
- 35.Aune D, Chan DS, Lau R, Vieira R, Greenwood DC, Kampman E, Norat T. Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose-response meta-analysis of prospective studies. BMJ. 2011;343:d6617. doi: 10.1136/bmj.d6617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Austin GL, Adair LS, Galanko JA, Martin CF, Satia JA, Sandler RS. A diet high in fruits and low in meats reduces the risk of colorectal adenomas. J Nutr. 2007;137:999–1004. doi: 10.1093/jn/137.4.999. [DOI] [PubMed] [Google Scholar]
- 37.Durrleman S, Simon R. Flexible regression models with cubic splines. Stat Med. 1989;8:551–561. doi: 10.1002/sim.4780080504. [DOI] [PubMed] [Google Scholar]
- 38.LaValley MP. Logistic regression. Circulation. 2008;117:2395–2399. doi: 10.1161/CIRCULATIONAHA.106.682658. [DOI] [PubMed] [Google Scholar]
- 39.Hosmer DW, Lemeshow S. Introduction to the logistic regression model. Second Edition. Applied Logistic Regression; 2000. pp. 160–164. [Google Scholar]
- 40.Wong MC, Lam TY, Tsoi KK, Hirai HW, Chan VC, Ching JY, Chan FK, Sung JJ. A validated tool to predict colorectal neoplasia and inform screening choice for asymptomatic subjects. Gut. 2014;63:1130–1136. doi: 10.1136/gutjnl-2013-305639. [DOI] [PubMed] [Google Scholar]
- 41.Stegeman I, de Wijkerslooth TR, Stoop EM, van Leerdam ME, Dekker E, van Ballegooijen M, Kuipers EJ, Fockens P, Kraaijenhagen RA, Bossuyt PM. Combining risk factors with faecal immunochemical test outcome for selecting CRC screenees for colonoscopy. Gut. 2014;63:466–471. doi: 10.1136/gutjnl-2013-305013. [DOI] [PubMed] [Google Scholar]
- 42.Tao S, Hoffmeister M, Brenner H. Development and validation of a scoring system to identify individuals at high risk for advanced colorectal neoplasms who should undergo colonoscopy screening. Clin Gastroenterol Hepatol. 2014;12:478–485. doi: 10.1016/j.cgh.2013.08.042. [DOI] [PubMed] [Google Scholar]
- 43.Kaminski MF, Polkowski M, Kraszewska E, Rupinski M, Butruk E, Regula J. A score to estimate the likelihood of detecting advanced colorectal neoplasia at colonoscopy. Gut. 2014;63:1112–1119. doi: 10.1136/gutjnl-2013-304965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Imperiale TF, Monahan PO, Stump TE, Glowinski EA, Ransohoff DF. Derivation and Validation of a Scoring System to Stratify Risk for Advanced Colorectal Neoplasia in Asymptomatic Adults: A Cross-sectional Study. Ann Intern Med. 2015;163:339–346. doi: 10.7326/M14-1720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Cao Y, Rosner BA, Ma J, Tamimi RM, Chan AT, Fuchs CS, Wu K, Giovannucci EL. Assessing individual risk for high-risk colorectal adenoma at first-time screening colonoscopy. Int J Cancer. 2015;137:1719–1728. doi: 10.1002/ijc.29533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Pox CP, Altenhofen L, Brenner H, Theilmeier A, Von Stillfried D, Schmiegel W. Efficacy of a nationwide screening colonoscopy program for colorectal cancer. Gastroenterology. 2012;142:1460–1467.e2. doi: 10.1053/j.gastro.2012.03.022. [DOI] [PubMed] [Google Scholar]
- 47.Chan AT, Arber N, Burn J, Chia WK, Elwood P, Hull MA, Logan RF, Rothwell PM, Schrör K, Baron JA. Aspirin in the chemoprevention of colorectal neoplasia: an overview. Cancer Prev Res (Phila) 2012;5:164–178. doi: 10.1158/1940-6207.CAPR-11-0391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Barzi A, Lenz AM, Labonte MJ, Lenz HJ. Molecular pathways: Estrogen pathway in colorectal cancer. Clin Cancer Res. 2013;19:5842–5848. doi: 10.1158/1078-0432.CCR-13-0325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Statitics Norway. Smoking habits, 2014. Smoking continues to decrease. Available from: https://www.ssb.no/en/helse/statistikker/royk/aar/2015-02-03.
- 50.Hassan C, Giorgi Rossi P, Camilloni L, Rex DK, Jimenez-Cendales B, Ferroni E, Borgia P, Zullo A, Guasticchi G. Meta-analysis: adherence to colorectal cancer screening and the detection rate for advanced neoplasia, according to the type of screening test. Aliment Pharmacol Ther. 2012;36:929–940. doi: 10.1111/apt.12071. [DOI] [PubMed] [Google Scholar]
- 51.Segnan N, Senore C, Andreoni B, Azzoni A, Bisanti L, Cardelli A, Castiglione G, Crosta C, Ederle A, Fantin A, et al. Comparing attendance and detection rate of colonoscopy with sigmoidoscopy and FIT for colorectal cancer screening. Gastroenterology. 2007;132:2304–2312. doi: 10.1053/j.gastro.2007.03.030. [DOI] [PubMed] [Google Scholar]