

Abstract
Background:
Medical and health advances have led to relative increases in human longevity and elderly population. Common diseases in elders can be prevented using healthy lifestyle. Identifying current status of the elderly is necessary to design educational intervention programs to improve their health and quality of life. Therefore, this study aimed at assessing the lifestyle of the elderly in Islamshar (suburban of Tehran).
Materials and Methods:
A descriptive – analytical study conducted among 480 elderly people over 60 years old referred to Islamshahr Health Center of Tehran University of Medical Sciences for a period of 12 months in 2012–2013. Data were collected through at two-part questionnaire including sociodemographic and health-related characteristics and healthy lifestyle instrument. Healthy lifestyle of the elderly was assessed using a 46 items self-report standard instrument with five subscales reflecting domains including exercise, nutrition, prevention, stress management, and social relationship. Finally, the data obtained were analyzed using the SPSS 18 software using an independent t-test, analysis of variance and ordinal logistic regression test at a significant level of P < 0.05.
Results:
Mean score of total healthy lifestyle was 148.56 ± 11.5. Men and women scored 151.95 ± 11.15 and 145 ± 10.32, respectively (P < 0.001). 76.2% of participants had moderately healthy lifestyle, and 23.8% had desirable healthy lifestyle. Marital status and gender were important factors in elderly healthy lifestyle.
Discussion:
The status of a healthy lifestyle among the elderly in Islamshar was relatively moderate. However, more studies are needed for further information to confirm study results. Study results were posed the necessity of tailoring specific interventional programs to achieve desirable healthy lifestyle.
Keywords: Elderly, healthy lifestyle, Islamshahr
INTRODUCTION
The ageing process is, of course, a biological fact which has its own dynamic, largely further than human control.[1] Elderly population is the fastest growing population in the world.[2] Efforts to maintain elderly people active have been done by investigating all possible factors that may affect their lives.[3,4] The elderly are increasing in Iran, too. Based on the 2006 census, 7 million people are over 60 years in Iran.[5] On the other hand, aging is accompanied with diminishing physical and mental capacities in daily life and incidence of chronic disease and comorbidities.[3] Investigating lifestyle patterns among older adults is particularly important, since the impact of behavioral risk factors increases with age and many chronic diseases will present during late adulthood.[6] Because of the cumulative effect of adverse factors throughout life, it is particularly important for older persons to adopt diet and lifestyle practices that minimize their risk of death from morbidity and maximize their prospects for healthful aging.[7]
Dietary patterns and other modifiable lifestyle factors are associated with mortality from all causes, coronary heart disease, cardiovascular diseases, and cancer.[8,9]
Regardless of predisposing factors, diet and lifestyle influence morbidity and mortality during the course of life.[10] Several papers have reported that longevity or healthy outcomes are associated with a healthy lifestyle, such as not smoking, drinking alcohol in moderation, exercising regularly or consuming a Mediterranean-type diet.[11,12,13] Many studies have suggested that attention to lifestyle of elder can help them get used to their lives and maintain their life satisfaction.[13,14] Brandt suggested that subordination of four modifiable healthy lifestyle factors (healthy diet, nonsmoking, normal weight, and regular physical activity) can significantly reduce premature mortality.[15] Chakravarty et al. found the elderly with fewer behavioral risk factors (overweight, smoking, inactivity) during middle age have lower disability and improved survival.[16]
Ford et al. reported, among older women, current health, and health related behaviors are stronger forecasters than social factors of comparatively early mortality. Accepting a healthier lifestyle, by doing more exercise and not smoking, is advantageous even in old age.[17]
However, elder psychological obstacle, lack of knowledge as an interpersonal and structural obstacle have all made it difficult for them to take part in healthy lifestyles. Consequently, besides the promotion of adhering healthy lifestyle by elder to stay healthy, more attention should also be paid to their internal and external difficulties in addition to improvement of the situation through facilities and arrangement of activities.[2,3]
According to above issues, lack of healthy life style, is a reason to increase mortality and seniors with a healthier lifestyle, can experience healthy ageing and improve their quality of life. Therefore, assess the elderly life style in order to prevent disease and improve their quality of life is very important.
In order to decrease barriers in adopting healthy lifestyle in the elderly, it needs to identify the exact difficulties to determine factors influencing them. According to limited studies in Iran, we tried to conduct a study in suburban dwellers of Tehran city as capital of Iran. Our older suburban dwellers are also likely to face various chronic physical and mental health problems based on some health indicators. Limited access to health care might help explain the overall poorer health of suburban residents who need more health-care services, but often have the fewest options and availability. This study aimed at assessing determinants of a healthy lifestyle and its related factors among elderly people living in Islamshar, South of Tehran.
MATERIALS AND METHODS
A descriptive – analytical study was conducted on 480 elderly people over 60 years old referred to Islamshahr Health Center of Tehran University of Medical Sciences (TUMS) for a period of 12 months in 2012–2013. Eligibility of participants was confirmed by welling to provide verbal informed consent to become involved the study, having at least 60 years old and living in Islamshahr at least 1-year. In order to ethical consideration, formal consent was obtained from TUMS research Ethical Clearance Committee and all participants were informed about aims of the study, and they were declared their verbal informed consent. A sample size with a confidence interval of 0.95, power of 0.8 and considering 20% sample size reduction, determined 480 elderly. Random clustering sampling method was applied based on the number of under coverage population that is, the more populous health centers, and the more selected subjects. Data collected through at two-part questionnaire including sociodemographic such as age, gender, level of education and living with spouse or family; and health-related characteristics, e.g. body mass index (BMI), history, type and frequency of chronic disease; and standard healthy lifestyle instrument. Healthy lifestyle of elders were assessed by a 46 items self-report standard instrument with five subscales reflecting domains including exercise (5 items), nutrition (14 items), prevention (15 items), stress management (5 items) and social relationship (7 items). Many questions contain 5 point Likert scale (never, rarely, sometimes, often, and always), yielding a score from 1 to 5, 1 for high risk behavior and 5 for the best healthy behavior. About questions 20–23 with triplet scale (low, medium, high) to coordinate the definition of these quantities, a page containing information about description of each food portions and recommended amount of daily nutrient intake was appendix. There weren’t any score, in questions 34, 44, 45 and 46 for cases who were living without a spouse. The minimum and maximum scores of instrument were from 42 to 211. This instrument categorized healthy lifestyle in three levels including desirable (156–211), moderate (99–155) and undesirable (42–98). Internal reliability of the original instrument was estimated adequate agreement (α =0.76).[18] Interviewers were aware of objectives of the study, collected information. The collected data were analyzed by descriptive statistics (tables, mean, median…) and analytic statistics using the SPSS 18 software (SPSS Inc: Chicago.). Independent t-test, analysis of variance (ANOVA), Chi-square test and ordinal logistic regression test were used to compare mean scores at a significant level of P < 0.05. The Chi-square test was used to determine the relation between type of lifestyle with and demographic information. We used independent t-test to determine the relationship between the mean score of lifestyle and demographic characteristics and in more than we groups we used ANOVA test. The logistic regression model was used to determine effective factors in elder lifestyle.
RESULTS
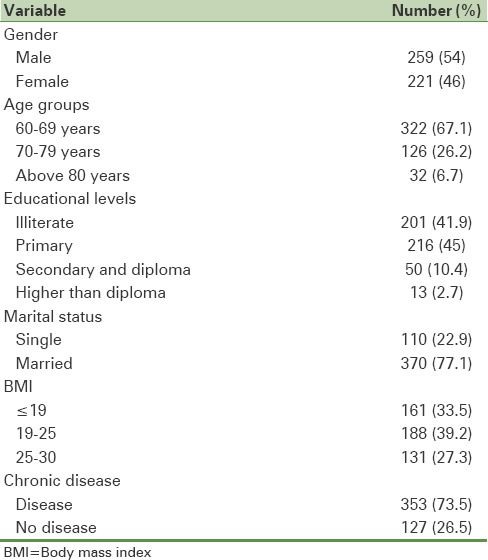
Overall, 480 people participated in the study, sociodemographic information and the elderly health related characteristics are revealed in [Table 1].
Table 1.
Demographic variables and the elderly health related characteristics
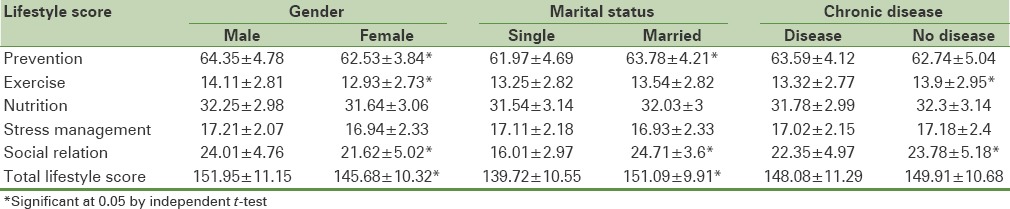
Mean score of a healthy lifestyle was 148.56 ± 11.15; the lowest was 102 and the highest 190. After division of lifestyle score to three levels (desirable, moderate and undesirable); 366 (76.3%) participants had moderate healthy lifestyle and 114 (23.8%) of them had desirable healthy lifestyle. None of the elderly had undesirable lifestyle.
Investigating the relationship between mean score of healthy lifestyle with age, gender, educational level, marital status, chronic diseases, and BMI revealed a significant association between lifestyle, age, gender and marital status (P < 0.05)
Distribution of mean score of a healthy lifestyle is presented based on demographic variables in [Table 2].
Table 2.
Distribution of mean score of healthy lifestyle based on demographic variables
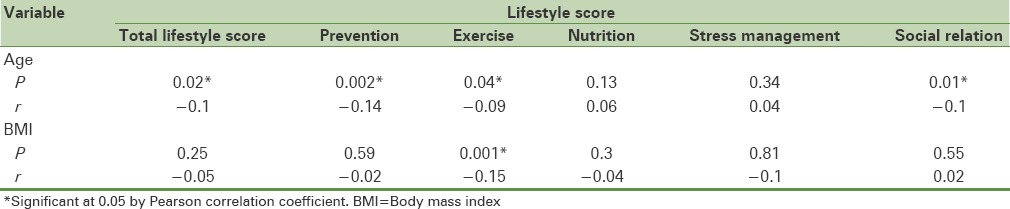
Correlation between lifestyle domains and age indicated the total score of a healthy lifestyle and its domains (prevention, exercise, and social relationship) were negatively correlated with age. When age increased, the mean score of the domains decreased. Furthermore, correlation between the different domains of lifestyle and BMI revealed negatively correlated between exercise domain and BMI [Table 3].
Table 3.
Correlation between age and BMI with lifestyle domains
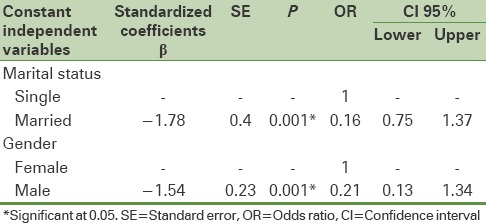
In order to assess relationship between lifestyle and demographic factors logistic regression analysis was utilized. Study results were revealed, there were significant association between lifestyle, gender and marital (P < 0.001). Logistics regression indicated that these two variables were the strongest predictors of desirable lifestyle. The odds ratio (OR) for achieving desired healthy lifestyle in married elderly were, 0.16 versus those without spouses. Furthermore, OR for achieving the desired lifestyle of males are 0.21 versus females [Table 4].
Table 4.
Logistic regression model for determining effective factors in healthy lifestyle
DISCUSSION
Study results revealed a relationship between age and the lifestyle. With increasing age, the average score in exercise domain decreases. By reason of decrease the elderly ability to activity with increasing age, this finding is reasonable. Babak et al. found similar results.[19] Seo and Hah demonstrated age as a related variable of promoting healthy lifestyle behavior.[20]
The study also indicated an inverse relationship between BMI and exercise domain. This is acceptable owing to the lack of interest in exercise for obese people. In Kisvetrová and Valášková study, obesity was observed as a risk factor with deficient physical activity by 36.60%, but the relationship between the BMI values in the elderly and their participation in physical activity was not confirmed.[21] Hodge et al. reported that moderate exercise and physical activity, was associated with the experience of successful aging and a healthy lifestyle, ideal weight can lead to appropriate changes in old age.[22]
In the present study, there was no significant association between educational level and lifestyle domains apart from exercise, but Babak et al. represented with increasing level of education, score of lifestyle and all domains increased.[19] Roskam and Kunst informed lower education levels have been shown to predict overweight.[23] This difference between our study and others may be as a result of very low educational level in current study. Perhaps because less educated groups are less receptive to health education messages and do not perceive their lifestyles as a health risk.
Relationship between mean score of healthy lifestyle and chronic disease revealed statistically significant difference between exercise, relationship domains and chronic diseases among healthy elderly and patients. Although, multiple regression analysis was demonstrated prevention domain as a predictor variable, these results are due to the inability of most elderly patients is defensible. Babak et al. reported elderly had lower scores in all domains except nutrition.[19] The results may be acceptable owing to patients feeling more positive and hopeful in dealing with their disease through improvements in nutritional status. Campbell et al. found quality of life is related to nutritional status in predialysis patients. Providing individualized nutritional counseling improves many components of quality of life, compared with standard nutrition care.[24]
Score of healthy lifestyle significantly was higher in men than women. Men in the prevention, exercise and social relations domains were obtained significantly higher scores. As well as in the nutrition and stress management domains scores were higher in men, but it was not significant. It may be argued that men are paying more attention to their lifestyle, perhaps it may be result of more social freedom and cultural causes in society, men have more social and physical activities. These results partly are consistent the results of Babak et al., however, in her study women had earned higher scores than men in the prevention domain.[19] Södergren et al. reported important gender differences in lifestyle behaviors and their association with health outcomes.[25,26]
The elderly who were living without a spouse, total healthy lifestyle and social relations domain scores were less than others who were living with their spouse. However in the first group the exercise domain score was higher. Seo and Hah reported, living with a spouse, including variables that are associated with health promoting lifestyle behaviors.[20] Manzori et al. stated living with spouse had a protective role against moderate depression.[27] Södergren et al. found women who were married more likely to belong to healthier group, compared to single women.[26]
The present study has a number of limitations that should be noted. First, most participants were illiteracy and it's an obstacle for using data sources by elderly. Second, the use of self-reported data may lead to measurement errors including under and over reporting of lifestyle behaviors. Finally, data were obtained from the province, so, results of this study might not be generalizable to other groups of older adults.
CONCLUSION
These findings suggest that a variation in health behaviors exist between men and women. Also, marital status had great impact in achieving the desired lifestyle between elderly. Hence, it seems in our society, family and social support are essential role in achieving healthier lifestyle between the elderly. Finally, this study suggests that adherence modifiable healthy lifestyle factors can substantially help senior for productive life.
Furthermore, most the elderly had moderate score of lifestyle, should try that affecting factors in lifestyle and its domains be as an important educational priority for elderly.
Financial support and sponsorship
Tehran University of Medical Sciences supported this survey as an original research. This study was granted by Tehran University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to thank research chancellor of (TUMS) for finding and the elderly who participated in the study.
REFERENCES
- 1.Gorman M. Development and the rights of older people. In: Randel J, editor. The Ageing and Development Report: Poverty, Independence and the World's Older People. London: Earthscan Publications Ltd; 1999. pp. 3–21. [Google Scholar]
- 2.World Health Organization. Active ageing: A policy framework. 2002. [Last cited on 2014 Feb 05]. Available from: http://www.who.int/ageing/publications/active/en/
- 3.Donaldson J, Watson R. Loneliness in elderly people: An important area for nursing research. J Adv Nurs. 1996;24:952–9. doi: 10.1111/j.1365-2648.1996.tb02931.x. [DOI] [PubMed] [Google Scholar]
- 4.Fillit HM, Rockwood K, Woodhouse K. 7th ed. Philadelphia, PA: Saunders Elsevier; 2010. Brocklehurst's Textbook of Geriatric Medicine and Gerontology; pp. 82–90. [Google Scholar]
- 5.Amar.org.ir. Statistical Center of Iran. [Last accessed on 2014 May 05]. Available from: http://www.amar.org.ir/Portals/2/fileExcell/13.pdf .
- 6.World Health Organization. 2008.2013 Action plan for the global strategy for the prevention and control of non-communicable diseases. [Last cited on 2014 Mar 10]. Available from: http://www.who.int/nmh/publications/9789241597418/en .
- 7.World Health Organization. Keep Fit for Life: Meeting the Nutritional Needs of Older Persons. [Last cited on 2014 Mar 12]. Available from: http://www.whqlibdoc.who.int/publications/9241562102.pdf .
- 8.Bijnen FC, Caspersen CJ, Mosterd WL. Physical inactivity as a risk factor for coronary heart disease: A WHO and International Society and Federation of Cardiology position statement. Bull World Health Organ. 1994;72:1–4. [PMC free article] [PubMed] [Google Scholar]
- 9.Huijbregts P, Feskens E, Räsänen L, Fidanza F, Nissinen A, Menotti A, et al. Dietary pattern and 20 year mortality in elderly men in Finland, Italy, and The Netherlands: Longitudinal cohort study. BMJ. 1997;315:13–7. doi: 10.1136/bmj.315.7099.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Knoops KT, de Groot LC, Kromhout D, Perrin AE, Moreiras-Varela O, Menotti A, et al. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA. 2004;292:1433–9. doi: 10.1001/jama.292.12.1433. [DOI] [PubMed] [Google Scholar]
- 11.Spencer CA, Jamrozik K, Norman PE, Lawrence-Brown M. A simple lifestyle score predicts survival in healthy elderly men. Prev Med. 2005;40:712–7. doi: 10.1016/j.ypmed.2004.09.012. [DOI] [PubMed] [Google Scholar]
- 12.Willcox DC, Scapagnini G, Willcox BJ. Healthy aging diets other than the Mediterranean: A focus on the Okinawan diet. Mech Ageing Dev. 2014;136:148–62. doi: 10.1016/j.mad.2014.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Davies N. Promoting healthy ageing: The importance of lifestyle. Nurs Stand. 2011;25:43–9. doi: 10.7748/ns2011.01.25.19.43.c8270. [DOI] [PubMed] [Google Scholar]
- 14.Hammar M, Ostgren CJ. Healthy aging and age-adjusted nutrition and physical fitness. Best Pract Res Clin Obstet Gynaecol. 2013;27:741–52. doi: 10.1016/j.bpobgyn.2013.01.004. [DOI] [PubMed] [Google Scholar]
- 15.Van den Brandt PA. The impact of a Mediterranean diet and healthy lifestyle on premature mortality in men and women. Am J Clin Nutr. 2011;94:913–20. doi: 10.3945/ajcn.110.008250. [DOI] [PubMed] [Google Scholar]
- 16.Chakravarty EF, Hubert HB, Krishnan E, Bruce BB, Lingala VB, Fries JF. Lifestyle risk factors predict disability and death in healthy aging adults. Am J Med. 2012;125:190–7. doi: 10.1016/j.amjmed.2011.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ford J, Spallek M, Dobson A. Self-rated health and a healthy lifestyle are the most important predictors of survival in elderly women. Age Ageing. 2008;37:194–200. doi: 10.1093/ageing/afm171. [DOI] [PubMed] [Google Scholar]
- 18.Eshaghi SR, Farajzadegan Z, Babak A. Healthy lifestyle assessment questionnaire in elderly: Translation, reliability and validity. Payesh. 2010;9:91–9. [Google Scholar]
- 19.Babak A, Davari S, Aghdak P, Pirhaji O. Assessment of healthy lifestyle among elderly in Isfahan. J Isfahan Med Sch. 2011;29:1074–64. [Google Scholar]
- 20.Seo HM, Hah YS. A study of factors influencing on health promoting lifestyle in the elderly – Application of Pender's health promotion model. Taehan Kanho Hakhoe Chi. 2004;34:1288–97. doi: 10.4040/jkan.2004.34.7.1288. [DOI] [PubMed] [Google Scholar]
- 21.Kisvetrová H, Valášková P. Regular physical activity amongst Czech and Slovak older adults - A pilot study. Kontakt. 2014;16:209–14. [Google Scholar]
- 22.Hodge AM, English DR, Giles GG, Flicker L. Social connectedness and predictors of successful ageing. Maturitas. 2013;75:361–6. doi: 10.1016/j.maturitas.2013.05.002. [DOI] [PubMed] [Google Scholar]
- 23.Roskam AJ, Kunst AE. The predictive value of different socio-economic indicators for overweight in nine European countries. Public Health Nutr. 2008;11:1256–66. doi: 10.1017/S1368980008002747. [DOI] [PubMed] [Google Scholar]
- 24.Campbell KL, Ash S, Bauer JD. The impact of nutrition intervention on quality of life in pre-dialysis chronic kidney disease patients. Clin Nutr. 2008;27:537–44. doi: 10.1016/j.clnu.2008.05.002. [DOI] [PubMed] [Google Scholar]
- 25.Södergren M, McNaughton SA, Salmon J, Ball K, Crawford DA. Associations between fruit and vegetable intake, leisure-time physical activity, sitting time and self-rated health among older adults: Cross-sectional data from the WELL study. BMC Public Health. 2012;12:551. doi: 10.1186/1471-2458-12-551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Södergren M, Wang WC, Salmon J, Ball K, Crawford D, McNaughton SA. Predicting healthy lifestyle patterns among retirement age older adults in the WELL study: A latent class analysis of sex differences. Maturitas. 2014;77:41–6. doi: 10.1016/j.maturitas.2013.09.010. [DOI] [PubMed] [Google Scholar]
- 27.Manzori L, Babak A, Marathi M. Depression and its related factors in elderly Isfahan. Iran Aging J. 2009;5:27–33. [Google Scholar]