

Abstract
Background:
Noncommunicable diseases such as Hypertension are among the important factors of mortality and morbidity of the elderly people. The family-centered empowerment model (FCEM) has not been performed for elderly people with hypertension.
Settings and Design:
This clinical trial study was carried out on 62 elderly people with hypertension under the coverage of the Lenjan Health Network in 2013. After performing the sampling by using the cluster-randomized method, the samples were divided randomly into the experimental and control groups.
Methods:
For the experimental group, the (FCEM) was implemented based on the four steps. For the control group, it was only implemented the usual care and one training session. Research tools included questionnaires of demographic data, empowerment assessment and a blood pressure-measuring device. The post-test was performed 1 week later. The blood pressure was recorded, and it was followed 1.5 month later again.
Statistical Tests:
Statistical tests for data analysis included χ2-test, independent t-test, Mann–Whitney, analysis of variance, and SPSS 20.
Results:
1 week later and 1.5 month after the intervention, the mean blood pressure was significant in both groups (P < 0.001). also, the difference in the mean score of empowerment dimensions was significant in the experimental group 1 week later and 1.5 month after the intervention (P < 0.001).
Conclusion:
Implementation of the FCEM for elderly people with hypertension has been possible from a practical point of view, and it has been associated with controlling and improving the blood pressure.
Keywords: Aging, empowerment dimensions, family-centered empowerment model, hypertension
INTRODUCTION
Aging phenomenon is one of the major demographic, social, economical, and medical issues that is formed today in the industrialized world and is being developed gradually in the Third World too. Demographers are considered the beginning of the aging period at ages from 60 to 65 years. Studies showed that the world population is currently aging.[1] According to the United Nations’ report in 1950, there were approximately 200 million elderly people worldwide, 350 million people in 1975, 687 million and 923000 people in 2006, and it is estimated that the figure exceeds 1 billion and 100 million people in 2025.[2] This is the same as other countries, and the ratio of the elderly population is rising every year in Iran because of the reduction of child mortality, declining of birth rate, and increased longevity.[3] According to the latest census of population and housing in Iran in 2006, the population of the people older than 60 years has been 7.2% of the total population. It is expected that by the year of 2021, the elderly population will reach to 10 million people or in other words, about 10% of the country population.[4] However, the problem has not shown itself as acute because of the youth population. But there is no doubt about it that in the near future, the health care system of the country will strongly face with it. The elderly people due to plenty of health difficulties are the major consumers of health-treatment services.[2] Noncommunicable diseases (NCDs) clearly have been one of the main problems in this age group, and these diseases have been one of the major causes of mortality in elderly people.[5] Currently, in Iran, NCDs with 60% mortality during the next 10 years will be responsible for 17% of mortality in the country.[4] Among these diseases, high blood pressure or hypertension is one of the treatable and major causes of morbidity and mortality in elderly people. In addition, hypertension is a correctable risk factor for cardiovascular diseases (CVDs)[5] with a slow start. This disease may not be diagnosed until the occurrence of a cerebrovascular or brain injury accident or a cardiovascular examination without clue. High blood pressure often is identified in the elderly people during a screening. Its major complication is the ultimate failure in vital organs such as heart, brain, kidney and vessels.[6] The blood pressure target in everyone is <90/140 and for people with diabetes should be ≤80/130.[6,7,8] Elderly people often have a systolic blood pressure or systolic–diastolic blood pressure and rarely, diastolic blood pressure.[7,8] The findings of the study of Framingham have shown that the increase in systolic and diastolic blood pressures in people at the age of 65 years and older had increased cardiovascular complications.[5] By performing timely diagnosis, targeted treatments, and proper management of this complication in the elderly population, it is possible to affect on different aspects of life of elderly people.[9] The ultimate goal in the management of hypertension is to reduce the risk of complications or eliminating the modifiable risk factors.[6] Various studies have shown that to control hypertension, it was used different approaches, including the continuous care model[10] and medical care on the patients.[11] Ghavami and colleagues[10], in a trial-clinical study entitled, “The effect of continuous care model in diabetic and hypertension patients”, showed that applying the continuous care model in the control of diastolic blood pressure was significantly effective in the experimental group. They suggested that the model may be used for continuous monitoring of blood pressure.[10] Furthermore, the results of the quasi-experimental prospective study of Pereira and Sergio in Brazil entitled, “The impact of pharmaceutical care interventions on blood pressure of outpatients’ elderly people with hypertension” indicated that pharmaceutical care interventions of nurses had a positive impact on health outcomes and blood pressure control in elderly patients with hypertension.[11] As we know, in our country, 92% of the elderly people are held by the family, and the family is regarded as the best source of support in the elderly people.[12] A family role is essential to improve the health level in the processes of prevention and treatment of diseases.[13] Thus, while caring a patient, his/her family needs to know the correct understanding of disease. The duty of a nurse, in addition to patient care, is to help the family to increase hope and trust. Such an approach would cause the promotion of family health and welfare.[14] Various studies emphasized on the role of other family members in the care of patients. Accordingly, Ezzati et al.[15], in a quasi-experimental study entitled “The effect of group discussion on high school boys to control high blood pressure of their parents”, demonstrated that group discussion was effective. They suggested that training through group discussion could be used as an effective educational strategy in the field of adolescents’ participation in improving their own health and their families too.[15] Training of elderly people is also very important, because elderly people believe that they are very old to worry about nutrition, exercise, health screening, and immunization.[16] Nowadays, in addition to the above strategies, pedagogical practices and assistance to individuals and families to obtain an active role in health care, it is emphasized on empowerment.[14] Empowerment is defined as the discovery process and the development of personal capacity to take the responsibility for life due to have adequate knowledge and resources to obtain and implement reasoned decisions and enough experiences in order to evaluate the effectiveness of decisions. Many scholars believe that empowerment is a dynamic, positive, interactive, and social process. It is a process that is formed in relation to others to respond better to treatment, prevention of complications, reducing health care costs, and creating a positive view toward the disease.[17] Family empowerment is meant to help the family, in order to be able to change.[14] In various studies, different models of health promotion and empowerment approaches have been used. However, few studies have pointed to the valuable role of the family to prevent controlling and treatment of diseases. The family-centered empowerment model is a native model with the centrality of the family. This model has not been used, so far for the elderly people with hypertension. The family-centered empowerment model has been designed with an emphasis on effectiveness of the individual and other family members’ role in three motivational, psychological (self-esteem, self-control, and self-efficacy) and characteristics of the problem (knowledge, attitude, and perceived threat). The principal goal of the family-centered empowerment model is empowering the patient family system for health promotion.[18] Some studies have been carried out with this approach on quality of life of elderly people,[19] children with thalassemia,[11] lifestyle of patients with myocardial infarction,[17] chronic diseases including multiple sclerosis[12] and asthma[20] to examine the influence of the empowerment model on the quality of life and health promotion of the subjects. Mentioned studies have shown that the empowerment model has been applicable from a practical point of view and has been associated with improvement and modification of quality of life, disease, and treatment. The implementation of this model has been resulted the increasing of awareness, understanding, and skill acquisition, and it has helped individuals and their families for efficient care to improve the illness condition. Community health nurse as the members of interdisciplinary teams play an important role for prevention and management of chronic diseases. They are the first and the most steadfast point of contact with patients, and in most cases, they have the best position to collect data about the patient's family. In addition, they have the needed skills in evaluating the ongoing care, training, and family support.[21] The researcher as a nurse has had several years of work experience in the health and medical sector and has witnessed the repeated visits of elderly people with critical hypertension to emergency wards and repeated hospitalizations in health centers, despite the provided training. Regarding the effectiveness of the family-centered empowerment model on patient care improving, in the conducted studies, lack of using this model for the patients with hypertension, and in particular, the vulnerable elderly people, severe complications of this disease in the absence of control have been occurred in addition to the high costs of treatment. Therefore, this study was conducted to determine the effect of the family-centered empowerment model on blood pressure, and the empowering dimension of the elderly people with hypertension to offer solutions, health care programs, empowering them to control and keep their blood pressure in interacting with the family and health systems to take a step, although short, in line for promoting the health among the elderly people.
MATERIALS AND METHODS
This trial-clinical study was conducted with two groups and three stages with pre- and post-test on 62 elderly people over 60 years in the Lenjan County of Isfahan in 2013. As per the Pukak formula and the results of the pilot study (Massoudi 2009, Teimouri 2011 and Vahedian Azimi 2009), the number of required samples was 25 elderly people for the experimental group and 25 elderly people for the control group including a 20% loss, and finally, it was estimated 31 subjects for each group.
Where Z1: 95% confidence factor = 1.96, Z2: 80% test power factor = 0.84, S is an estimate of the standard deviation of each of the variables of blood pressure and empowerment in both the experimental and control groups, d is the least mean difference of each of the variables between the experimental and control groups to show the significant difference (=0.8S).
Inclusion criteria for the elderly people were consisted of age of 60 years and older, having hypertension with the approval of the physician of the healthcare centers in their health records, having health records in the center, willingness of a patient to participate in the research, completing the questionnaire of assessing the empowerment dimensions, acquiring the score on a scale of moderate to poor, lack of known mental disorders, lack of Alzheimer's disease for affecting the ability to learn, ability to complete the questionnaire, learning ability, minimum literacy for reading and writing, and ability for understanding. Exclusion criteria for the elderly people were included lack of desire to continue cooperation in the empowerment program, unwillingness to complete research tools, and lack of participating in the meetings for more than one session. Inclusion criteria for the active member of the family were included to be a constant participated member in the study such as spouse, child, and grandchildren who live with the elderly people in a family, having the ability for decision-making, willingness to participate in the study (with the understanding of the importance of health of elderly people), completing the questionnaire of assessing the dimensions of empowerment, and acquiring the score on a scale of moderate to poor. The exclusion criteria for an active member were included unwillingness to participate and continued cooperation in the research at each stage and unwillingness to complete research tools. Gathering data tools were included the checking list of demographic characteristics, empowerment assessment questionnaire, and a sphygmomanometer device. The researcher made questionnaire was designed by the researcher with the guidance of professors to assess the empowerment dimensions of elderly people with hypertension and elderly family members based on similar studies[17] with eight dimensions included: Detection dimension of control (A) with 3 questions, assessment dimension of perceived severity (B) with 13 questions, dimensions of perceived susceptibility (C) with 16 questions, feelings of self-efficacy dimension (D) with 10 questions, dimension of self-efficacy of the patient to self-report (E) with 12 questions, dimension of the researcher observation from patient's self-efficacy (F) with 5 questions, dimensions of self-esteem (G) with 12 questions and dimension of patient's self-control (I) with 7 questions, and 78 closed questions with the scale of “yes”, with a score of 1, and “no” and “I do not know”, with a score of 0. The rating was from 0 to 100 points. The questionnaire was used before the intervention to identify the lack of ability of elderly people for inclusion criteria. The final analysis was based on the mean. For trust and validity of the scientific tools, it was used to read books, new articles, different studies and experiences, and opinions of 10 members of the nursing faculty. Its reliability was confirmed by the test/retest (r = 0.735) and Cronbach's a coefficient of 0.753. A blood pressure gauge was calibrated before the intervention, 1 week after the intervention, and 1.5 months after the intervention, and its reliability was confirmed by the measurement of blood pressures of 20 elderly people within 3 min from each other and calculating the correlation coefficient of systolic blood pressure (r = 0.949) and correlation coefficient of diastolic blood pressure (r = 0.772). The researcher at the stage of before intervention was referred to the Lenjan Health Network. After receiving the referral letter and written permission from the Vice Chancellor for Research of the faculty of nursing and midwifery of Isfahan, and then by using the cluster method among the four regions of Lenjan County, four centers were selected (one center per region). The list of all elderly people with high blood pressure was extracted (items with the approval of the physician of the studied center). In order to ensure the lack of elderly people empowerment, the questionnaire was completed for them by the interview with the researcher. After analyzing the results, 62 elderly people by using the table of random numbers were assigned into two experimental and control groups to implement the intervention program of empowerment in accordance with the needs of the studied elderly people. Upon completion of the sampling, the desired elderly people were invited to health centers of their own, and it was expressed the importance of issue for them and how to do research. Later, an informed consent form was completed, and the blood pressure was taken based on the criteria of the seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure (jnc7). The individual was placed at first for 5 min in a relaxed position and fully at rest by avoiding stimulants such as tea, coffee, cigarettes, and adrenergic stimulants such as nose drops, and while sitting and the arm was placed at the level of heart, then systolic and diastolic blood pressures were controlled with a mercury sphygmomanometer (model of Richter) from both right and left arms for two times with the interval, and the mean blood pressure was recorded from the arm with the higher blood pressure. The first phase of korotkoff sound was regarded as systolic blood pressure and the korotkoff fifth phase sound, and disconnection of sound was considered as diastolic pressure. The mean of measurements were recorded as the blood pressures of the elderly people in the month before training.[7] The second step was included the empowerment intervention only for the experimental group. The family-centered empowerment model was performed according to the model steps in the following order:
First step: Perceived threat: The first step in the family-centered empowerment model was increasing the perceived threat (perceived intensity and susceptibility) of elderly people through group discussions to increase knowledge, attitude, and awareness. For this purpose, the elderly people at their respective centers were placed in the groups of seven to eight persons for holding three sessions of 45 min (Allah Yari 2006, Vahedian Azimi 2009, and Teimouri 2011). The titles of sessions were included the discussions: 1, physiology, nature, and symptoms; 2, risk factors and classification of diseases; 3, side effects, acute relapses, and prognosis; 4, pharmacological and nonpharmacological treatment; and 5, lifestyle. The meetings were carried out with the participation of the elderly people and telling their experiences with the role of guiding, supportive, and educational role of the researcher. At the end of each session, the articles were summarized, and the questions were answered. Then, they were identified for date, time, and objectives of the next meeting. At the beginning of the next session, three questions out of the previous session discussions were discussed for the assessment of the trainings and to employ them (evaluation process).
Second step: Self-efficacy: To promote the self-efficacy level, group discussion and practical views were used in groups of seven to eight persons at their own related centers for four sessions of 45 min by using the required skills including skills for lifestyle changes (nutrition, sporting activities, smoking, and stress coping skills), skill of how to work with the blood pressure gauge, and the skill of drug adjustment plan for elderly people. After explaining the skills practically, elderly people actively participated in educational activities, and they told their experiences to the others. In the discussion group sessions, elderly people were actually faced their problems. They discussed under the supervision of the researcher by specifying objective examples of their situation and performed actions to improve the problems. Thus, by participating in group discussions, they had an opportunity to be empowered to apply those skills practically and repeatedly. Therefore, without the presence of the nurse, they are able to do it themselves. Encouragement receiving from nurses was increased self-efficacy and self-control in the studied samples.
Third step: Self-confidence: At this step, elderly people were asked to participate in training of the member of their families in connection with related issues to hypertension and encouraging them to help themselves. By this way, the discussed items in previous meetings based on educational participation (by training cards or pamphlet) should be transferred to the active member of their family. On the cards, three open questions were asked from the family member about the disease of the elderly people. In addition, the educational pamphlet should be given to the families by elderly people, and they were asked to tell their families that after reading the instructions of pamphlet and what they have learned from the sayings of the elderly people, they should write their related questions on a sheet of paper and deliver it to the researcher in the next meeting. Later, to measure the learning and empowerment of family member from the material provided by the elderly people, three sessions of 45 min were held in the respective centers with the presence of the researchers, elderly people, and the active member of their family. The researcher received feedbacks from the taught subjects to the family member by the elderly people through the card or pamphlet. Transfer of training materials from elderly people to their family was strengthening better learning for the implementation of the above program and increased sense of self-efficacy and responsibility in elderly people. Thus, an opportunity was provided for choices and decisions. Therefore, with the active participation of the elderly people, the sense of self-esteem was increased in them.
Fourth step: Evaluation: This step was included an evaluation process and the final evaluation as follows:
Evaluation process: During holding empowerment intervention sessions in the form of question and answer sessions and group discussion, questions and uncertainties were raised. Elderly people and their active family member had active participation in the questions and answers and group discussion. The meeting continued to resolve ambiguities. After performing the next steps of the model, the researcher to ensure the empowerment of elderly people and the active member of their family, 1 week after the intervention performed the post-test (interviewed with the elderly people and active member of the family, completed the assessment questionnaire of the dimensions of family-centered empowerment with one 45-min session and controlled blood pressure of the elderly people). Then, the elderly people and active family member were allowed to apply the family-centered empowerment model.
Final evaluation (after the intervention): Finally, one and a half month after the intervention, another 45-min session was held and with completing the assessment questionnaire, empowerment dimensions and controlling blood pressure of the elderly people (final evaluation) were followed.
After finishing the third step, considering ethical issues in the control group, elderly people in the control group and active member of the family were invited to their respective health centers to teach all subjects. For the experimental group in one training session, the pamphlet was provided and then, one and a half month later, the post-test questionnaires were completed and followed-up.
RESULTS
Demographic variables related to the elderly people and the active member the family are given in Tables 1 and 2.
Table 1.
Determination and comparison of demographic variables of elderly people and the active member of the family
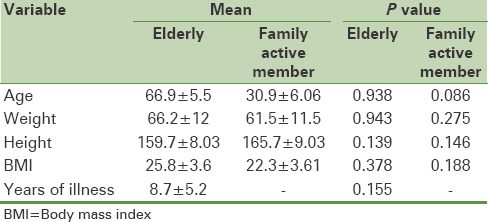
Table 2.
Determination and comparison of frequency distribution of demographic variables of elderly people and an active member of the family
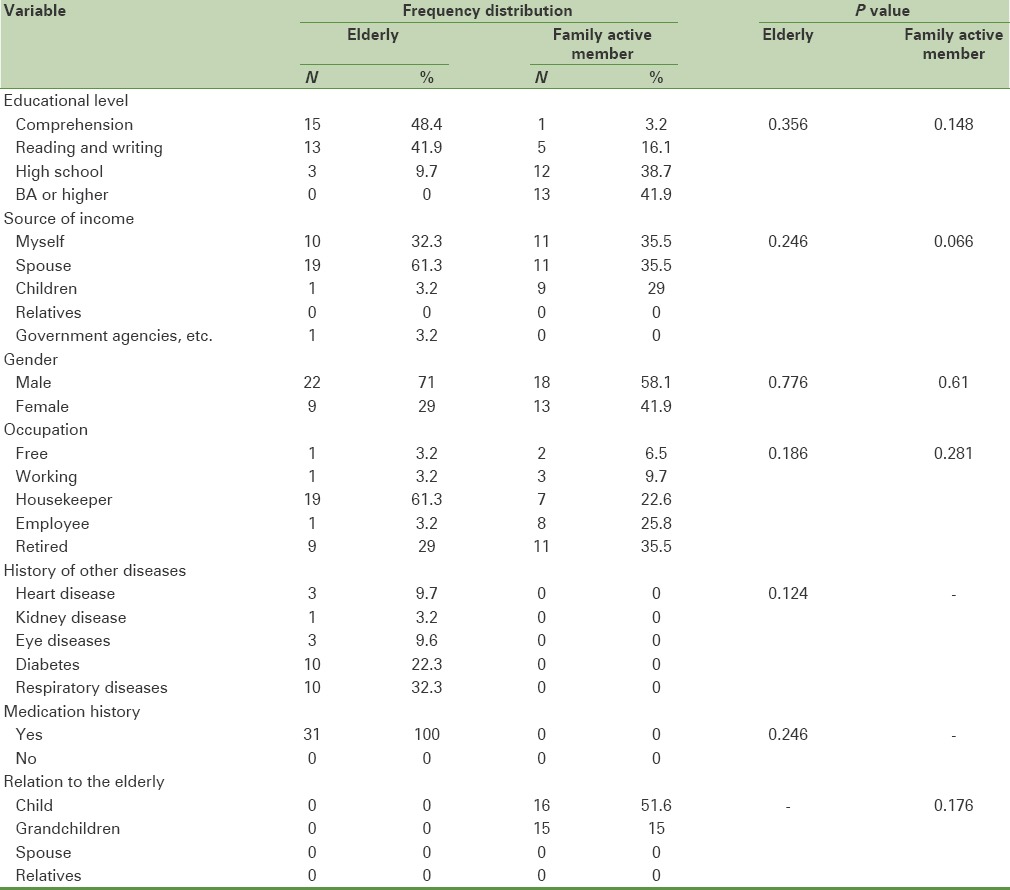
The results of this study showed that in the groups of elderly people and the active member of the family, there was no significant difference in demographic variables between the experimental and control groups. The two groups were matched in this regard. In the explanation, it should be noted that considering assigning randomized samples in both the experimental and control groups, such an outcome was expected. In fact, their lack of significance confirmed the randomized assignment of subjects in both groups.
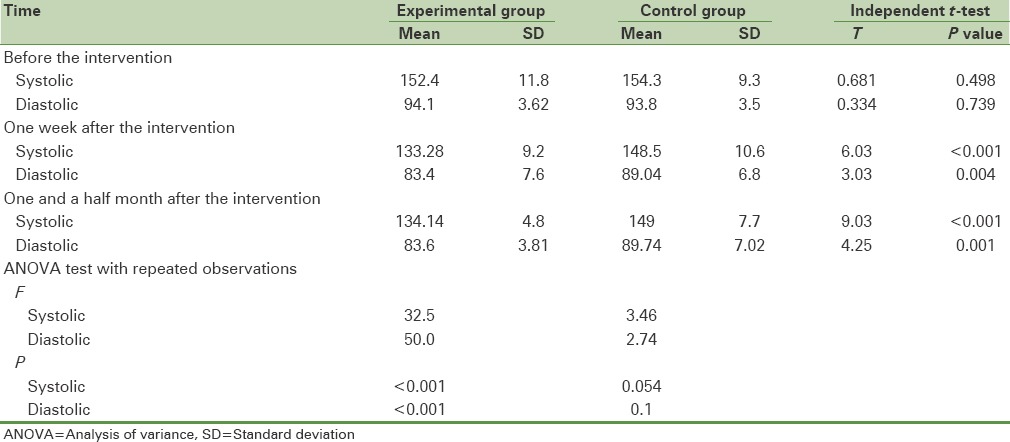
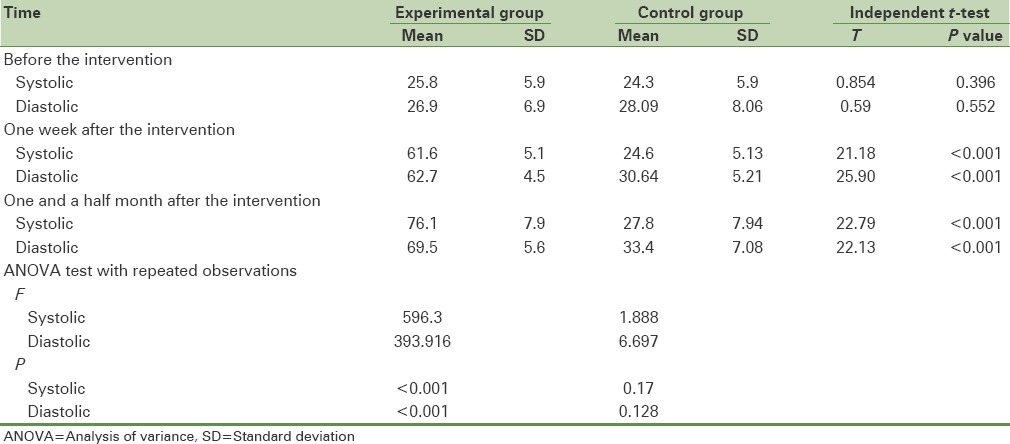
The mean systolic and diastolic blood pressures in the elderly group in both experimental and control groups are given in Table 3. In both experimental and control groups, there was no significant difference between the mean systolic and diastolic blood pressures before the intervention. However, 1 week later and 1.5 after the intervention, the difference in the experimental group was dramatically significant compared with the control group.
Table 3.
The mean blood pressure in the elderly people in the experimental and control groups at different times
The mean score of empowerment dimensions in the elderly people and the active member of the family in both the experimental and control groups are given in Table 4. There was no significant difference before the intervention in both experimental and control groups. However, 1 week after the intervention and 1.5 month after the intervention, this difference was dramatically significant in the experimental group. However, there was no difference in the control group.
Table 4.
The mean of total score of elderly people empowerment assessment dimensions and the active member of the family in both experimental and control groups at different times
DISCUSSION
In this study, it was investigated the impact of implementation of the family-centered empowerment model on blood pressure and dimensions of empowerment in 62 elderly people with hypertension under the coverage of Health and Treatment Network of Lenjan. The results of this study showed that the there was a significant difference between the mean difference before intervention, in 1-week interval after intervention, and 1.5 month after the intervention in systolic blood pressure and the mean of diastolic blood pressure of the elderly people between the experimental and control groups. In fact, it indicated the impact of intervention of family-centered empowerment on the improvement of blood pressure in elderly people. This was consistent with the results of Vanaprapan and colleagues study in 2011. They showed in their study that the intervention of empowerment process in 4 days has been effective in promoting health to control the blood pressure and the results before the intervention and after the intervention were significantly different (P < 0.001).[22] Abudagga and colleagues conducted a review study in 2010 entitled “the effects of blood pressure monitoring on hypertension results”. They stated that home blood pressure monitoring and self-management of hypertension in individuals in 51–76 years old people have facilitated the achievement of controlled blood pressure and it can promote medication self-management, confidence, and awareness of the patients. This study results also confirmed the results of Abudagga study.[23] In confirming the findings of this study, Cigar and colleagues in 2009 conducted a clinical trial entitled, “Evaluation of the impact of education on the blood pressure in elderly people aged 65 years and older”. They have stated that in the participated group at the training workshop based on empowerment and patient self-management, there was a significant decrease of 8 mmHg in the systolic blood pressure compared with the control group participants at the workshop based on the reliability-centered model, and there was a reduction of 3 mmHg in the systolic blood pressure. Therefore, researchers have acknowledged that training based on the empowerment model and self-management has been more effective than the reliability-centered educational model.[24] In [Table 3], the differences of the mean score of empowerment dimensions assessment in both experimental and control groups, before, 1 week later, and 1.5 month after the intervention are shown. The results showed that between the experimental and control groups, there was also a significant difference in the experimental group compared with the control group (P < 0.001). In the mean score of empowerment dimensions assessment of the active member of the family, there was a significant difference between the experimental and control groups in the 1-week intervals after intervention and 1.5 month after the intervention (P < 0.001). In fact, this case indicated that intervention impact on empowerment and the ability of family member. This intervention by promoting the level of awareness, and attitude, attracting family participation, using the existing skills within the family under the supervision and assistance of community health nurse and through transferring knowledge and skills of elderly people to family members have been increased self-esteem, feelings of worthiness, and finally, self-efficacy and self-control of disease in the elderly people. In confirming some of the results of this study, Carr in 2011 in a study entitled, “Empowerment: A framework for development of supporting grandmothers caring of their grandchildren” recommended empowerment based on the need of grandmothers. The obtained results of empowering education demonstrated the development of grandmothers’ skills, increasing self-care, self-efficacy, life self-control, problem-solving ability, and their support for themselves and their descendants. However, about the difference between this model and the present model, it should be noted that the study of Carr proposed that designing a collaborative curriculum for both groups of grandmothers and their descendants was among the disadvantages of this model and empowerment program, which only focused on grandmothers.[25] Vanessa Hodges in a research entitled ‘Framework of family-centered practices’ has performed an intervention to compare the model of family-centered activities and system-centered model. She has stated that the model of family-centered activities has focused on the entire family unit with the aim of strengthening, empowerment, supporting, and problem solving. For this purpose, it has been used traditional and non-traditional strategies such as consultation, learning new skill, supporting and connection to official and unofficial sources. Decision-makers were included the personnel and their families, while in the system-centered model, it was often given to people and in some cases to the family with the aim of solving the problem referred to the family. Due to this reason, it was frequently used traditional and selected strategies such as consultation and development of skills with personnel decision making, while the family-centered empowerment model has been focused on the patients and their family members as a whole. Its purpose has been the development of perceived threat, self-control, self-efficacy, and promoting self-esteem along with supporting and solving the referred problem to the family. For this purpose, it was used all possible strategies as an empowerment intervention such as consultation, learning new skills, supporting and connection to official and unofficial sources with the decision-making of the patient, every member of the family, and medical team personnel.[26] The results of this study were consistent with the study of Tang in 2010. He has shown in a cohort study entitled, “Self-management support: An empowering-centered intervention” that a 6-month self-management support based on empowering-centered intervention on 77 adult subjects has been caused the promotion of health, self-management, empowerment, feeling of support, self-efficacy, and self-esteem.[27] Resenick and colleagues conducted a 12-week empowerment intervention program on the elderly people in 2008. They showed that the self-efficacy and the hope in them have been increased significantly, and finally, they have been empowered.[28] Massoudi study (2010) showed that implementation of the family-centered empowerment model on the elderly people resulted better quality of life and by applying of this model can facilitate the path for healthy aging on the elderly people.[19] Santo and his colleagues in 2008 in a study stated that empowerment was triggered increasing of public authority and community groups in interpersonal relationships. The primary goal of empowerment is to help individuals and communities for further tasks of independence, self-confidence, feelings of power, and control. In empowerment, it has been emphasized on the strategy of health promotion for the elderly people.[29] The results of this study were consistent with these results. Family-centered care is one of the methods of effective care in chronic diseases. By using the valuable experiences of the elderly people and their family and improving their capabilities in facing with chronic diseases and especially hypertension, it will be possible to pass a basic step in order to promote the health of elderly people. Implementing an empowerment program can lead to preventive behaviors to promote health. Finally, based on the findings of this study, implementation of the family-centered empowerment model has been effective on the blood pressure and the empowerment dimensions of elderly people with hypertension. Therefore, nurses can have an important role to keep blood pressure in elderly people with the centrality of the family by using family-centered empowerment intervention and due to the different dimensions of empowerment, family-centered empowerment model, which was discussed in this article. Thus, it can be pointed out to the reasons of effectiveness of this intervention including strengthening the spirit of independence, accountability, self-control, identifying opportunities, motivation, improving skills, and being self-efficient. However, due to self-esteem for the promotion of health status and following up the hypertension disease in the elderly people with the central role of the family and according to the description of this disease, symptoms, being serious and incurable, offering practical solutions and the creation of empowered belief have been the benefits of using this model. According to the results of this study, the importance of the family-centered empowerment model in aging would be a priority. Due to this fact that aging is a stage of people life, it puts them at the risk of encountering with chronic diseases including hypertension. Due to the nature of aging and increased prevalence of hypertension in the elderly people, which several studies have proved it; therefore, it is recommended to apply this model as an alternative to promote health in hypertension disease in the elderly people and in the healthcare centers. Furthermore, by using and implementation of the family-centered empowerment model, it is possible to increase various dimensions of empowerment and in particular, self-efficacy and self-esteem in the elderly people and their autonomy to keep up and improve blood pressure for having the successful aging process. This type of health care can be helpful due to the nature of aging in affecting the elderly people, their family, and health care personnel. Therefore, it is recommended to design and implementation of such effective, safe and inexpensive programs for elderly people. Due to the development of nursing roles in different areas of health, treatment, education, and research and according to the results of this study, besides the expressed roles by the researcher as a community health nurse, that the elderly people were able to achieve empowerment with the centrality on family, the researcher hopes that the obtained results from this study will be used in various fields. The findings can also be used in a broader level by other categories of health care system, technicians, health professionals, nurses, and particularly the community health nurses as advocates and health care leaders should provide effective services for patients by engaging in training, creating family participation in health activities, and involving in research studies and health care policies. Community health nurses as members of interdisciplinary teams play an important role to prevent and management of chronic diseases such as hypertension, diabetes, and cancer. Therefore, by applying this model in all areas of health, they can help the family, clients, and health systems. Studies have proven that using the family-centered empowerment model in the chronic disease care has been effective, simple, cheap, affordable, and feasible from a practical point of view with a favorable reception by the elderly people and other clients. Therefore, it is possible to use the findings of this study in the empowerment intervention and training of clients. Completion of each research is associated with the start of new questions about the topic of study and other topics. The existing questions in this study would indicate the need for conducting new surveys to lead to further research studies.
Suggestions for future research
Evaluation the impact of the family-centered empowerment model on other chronic diseases in the elderly people.
Comparison of the effects of other models of empowerment on blood pressure of elderly people with hypertension.
CONCLUSION
Based on the shown results, empowerment of elderly people with high blood pressure is prompted the preservation and improvement of blood pressure of elderly people, and it indirectly involves the family member as well. Health care providers and especially nurses should pay attention that useful and effective care of the elderly people should be performed within the family framework to promote self-esteem, self-efficacy, and empowerment of the elderly people and finally, preservation and improving their blood pressure and reducing costs incurred by the health care system and family. Different models and approaches have been provided in the world for empowerment, and several studies have also used some of them for patients with hypertension. However, the family-centered empowerment model is a localized native model and its surveillance protocol with the approval of the Deputy of Health Department specifically designed for elderly people with hypertension. Therefore, it is recommended to implement this model in other chronic diseases of aging for having more effective steps in order to improve the health of elderly people faced with chronic diseases. This study was the first research to apply the family-centered empowerment model in the elderly people with hypertension. The findings of a study must be evaluated along with its limitations. Therefore, it is suggested that the limitations of this study will be resolved in subsequent studies. In fact, the limited duration of the study will require approximately 1–3 months for following-up. However, it was limited to a student research. Other limitations of the study were having two groups of elderly people and active members of the families and each of them separately in two experimental and control groups, multiple centers under study, working with elderly people that from their own point of views, it was too late to investigate health condition. Certainly, performing the intervention with a more time limitation and having an expert research group in aging could be more effective for obtaining the best results. It should be noted that in this study, some variables affecting the blood pressure were outside the control of the researcher such as lifestyle, nutrition, exercising time, stress, and the possibility of finding information by the control group from the information given to the experimental group.
Financial support and sponsorship
Isfahan University of Medical Sciences.
Conflicts of Interest
There are no conflicts of interest.
Acknowledgments
To the authors appreciate the Vice Chancellor for Research, faculty members of Nursing and Midwifery faculty of Isfahan, Lenjan Health Network officials, and all the beloved people who cooperated in conducting this study. The also acknowledge the dear elderly people and their families for their sincere cooperation and the obtained results.
REFERENCES
- 1.Nanbakhsh F, Mohaddesi H, Amirai A, Haji Shafiha M, Broomand F, Bahadori F, et al. The Effect of Health Education on Elderly Weomen Life Quality. Payavard. 2011;5:47–57. [Google Scholar]
- 2.Rejeh N, Heravi Karimooi M, Montazeri A, Foroughan M. psychometric properties of the iranian version of the facts on aging quiz (FAQI) Payesh. 2012;11:245–2513. [Google Scholar]
- 3.Habibi A, Nemadi-Vosoughi M, Habibi S, Mohammadi M. Ardabil, Iran: Journal Of Health; 2012. Quality of life and prevalence of chronic illnesses among elderly people: A cross-sectional survey; pp. 58–66. [Google Scholar]
- 4.Noncommunicable diseases. [Last accessed on 2012 Apr 7]. Available from: http://www.webda.behdasht.gov.ir/index.aspx?siteid=326andpageid=32628 and newsview=60111andpro=nobak .
- 5.Chinnakali P, Mohan B, Upadhyay RP, Singh AK, Srivastava R, Yadav K. Hypertension in the elderly: Prevalence and health seeking behavior. N Am J Med Sci. 2012;4:558–62. doi: 10.4103/1947-2714.103314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ebersol P, Hess P, Touhy TA, Jett K, Schmidt Luggen A. 7th ed. Florida: Mosby/Elsevier- Medical; Toward healthy aging: Human needs and nursing response; pp. 228–9. [Google Scholar]
- 7.JNC7 Express. The seventh report of the joint national committee. 2003 [Google Scholar]
- 8.Kaplan NM. 9th edn. Philadelphia, United States: Lippincott Williams and Wilking; 2006. Clinical hypertension; p. 11. [Google Scholar]
- 9.Kamali M, Arjmand Hesabi M, Ahangari M. The study of quality of life in the elderly with hypertension who are member of tehran senile culture house clubs. Salmand. 2008;3:26–32. [Google Scholar]
- 10.Ghavami H, Ahmadi F, Entezami H, Meamarian R. The effect of continuous care model on diabetic patients’ blood pressure. Iran J Med Edu. 2006;6:87–94. [Google Scholar]
- 11.De Lyra DP, Junior, Sergio Marcellini P, Rosemir Pela I. Effect of pharmaceutical care intervention on blood pressure of elderly outpatients with hypertension. Braz J Pharm Sci. 2008;44:3. [Google Scholar]
- 12.Heydari S, Salahshourian-Fard A, Rafiee F. Correlation of perceived social support from different supportive sources and the size of social network with quality of life in Cancer Patients. Iran J Nurs. 2009;22:71–82. [Google Scholar]
- 13.Allahyari I, Alhani F, Kazemnezhad A, Izadyar M. The effect of family empowerment model-based on the quality of life of school-age children with thalassemia. Iran J Pediatr. 2006;16:455–61. [Google Scholar]
- 14.Masoudi R, Alhani F, Moghadassi J. The effect of family-centered empowerment model on skill, attitude, and knowledge of multiple sclerosis caregivers. J Birjand Univ Med Sci. 2010;17:87–97. [Google Scholar]
- 15.Ezzati E, Anoosheh M, Mohammadi E. A study of the effects of group discussion with male high school students on their parents’ hypertension control. J Res Health. 2011;1:64–72. [Google Scholar]
- 16.Hejazi SH, Sahbaiee F, Fesharaki M, Abdollahi A. The effect of education about health-promoting behaviors on the knowledge of the elderly in the geriatric nursing residences in Tehran. J Birjand Univ Med Sci. 2012;19:114–21. [Google Scholar]
- 17.Azimi A, Alhani F, Ahmadi F. Effect of family-oriented empowerment model on the life style of myocardial infarction patients. Iran J Crit Care Nurs. 2010;2:127–32. [Google Scholar]
- 18.Alhani F. Tehran: Tarbiyat Modarres University; 2003. Design and evaluation of the family-oriented prevention of iron deficiency anemia. [Google Scholar]
- 19.Masoudi R, Soleimani MR, Qorbani M, Hasheminia AM, Pour Dehkordi AH, Bahrami N. The effect of family-centered empowerment model on the quality of life of in elderly people. J Qazvin Univ Med Sci. 2010;14:57–64. [Google Scholar]
- 20.Teymori F, Alhani F, Kazemnejad A. The effect of family-centered empowerment model on the quality of life of school-age asthma children. Iranian J Nurs Res. 2011;6:52–63. [Google Scholar]
- 21.Lee L W. Chronic Disease and Nursing. [Last accessed on 2005 Oct]. Available from: http://www.2.Cna Aiic.Ca/CNA/Documents/Pdf/Publications .
- 22.Wannaprapan B, Pansila W, Tansakul C, Shelp F. Tertiary prevention of Hypertention throught empowerment health behaviore of ambulatory patients at selected primary care units of nakhonratchasima province, Thailand. Pak J Soc Sci. 2012;9:63–8. [Google Scholar]
- 23.Abudagga A, Resnick HE, Alwan M. United States: Mary Ann Liebert, Inc; 2010. Impact of Blood pressure telemonitoring on hypertension outcomes: Telemedicine and E-Health. Vol. 16, No. 7; pp. 830–8. [DOI] [PubMed] [Google Scholar]
- 24.Figar S, Galarza C, Petrlik E, Hornstein L, Rodríguez Loria G, Waisman G, et al. Effect of education on blood pressure control in elderly persons: A randomized controlled trial. [Last accessed on 2009 Jun 28];Am J Hypertens. 2006 19:737–43. doi: 10.1016/j.amjhyper.2005.10.005. Available from: http://www.Sciencedirect.Com/Science/Article/Pii/S089570610501201x . [DOI] [PubMed] [Google Scholar]
- 25.Carr GF. Empowerment: A Framework to develop advocacy in African American Grandmothers providing care for their grandchildren. ISRN Nurs 2011. 2011:531717. doi: 10.5402/2011/531717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hodges V. Family-centered practice: The basics. [Last accessed on 2009 Oct 07]. Available from: http://www.ssw.unc.edu/mch/default.asp .
- 27.Tang TS, Funnell MM, Brown MB, Kurlander JE. Self-Management Support in “Real-World” Settings: An Empowerment-Based Intervention. Patient Educ Couns. 2010;79:178–84. doi: 10.1016/j.pec.2009.09.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Resenick B, Luisi D, Vogel A. Testing the Senior Exercise Self-efficacy Project (SESEP) for use with urban dwelling minority older adults. Public Health Nurs. 2008;25:221–34. doi: 10.1111/j.1525-1446.2008.00699.x. [DOI] [PubMed] [Google Scholar]
- 29.Santo SS, Barlem EL, Tarouco Da Silva B. Health promotion for the Elderly: Gerontogeriatric nursing commitment. Acta Paul Enferm. 2008;21:649–53. [Google Scholar]