

Abstract
Background and Objectives:
Addicts account for approximately 68.15% of AIDS cases in Iran and injection drug users are considered as a major factor in the spread of AIDS in Iran. The purpose of this study was to determine the effect of an educational intervention on the perceived self-efficacy, benefits, and barriers concerning AIDS preventive behaviors among drug addicts in Khorramabad, Iran.
Methods:
This is a quasi-experimental study carried out in 2013 on 88 addicts kept in rehabilitations center in Khorramabad. The data collection instruments included a questionnaire on self-efficacy, perceived benefits, perceived barriers, knowledge and preventive behaviors regarding HIV. Data were analyzed by paired t-test, independent t-test, Chi-square and analysis of covariance.
Results:
Paired t-test showed that the mean scores for perceived benefits and barriers, knowledge and preventive behaviors significantly increased in the intervention group after the intervention than before the intervention. But the increase in self-efficacy score was not statistically significant.
Conclusions:
The results of this study showed that training and education based on the health belief model led to an increase in knowledge, self-efficacy, perceived benefits, performance and reduction in perceived barriers in addicts. It is recommended that future studies should include strategies for enhancing self-efficacy and perceived benefits as well as strategies for reducing barriers to the adoption of preventive behaviors.
Keywords: AIDS, Drug Abusers, perceived barriers, perceived benefits, perceived self-efficacy
INTRODUCTION
The HIV virus is one of the most lethal viruses discovered in the modern age and due to its high mortality rates and excessive caring costs, it is considered as a serious health and financial burden among all societies.[1,2] HIV has turned into an epidemic disease that threatens the global community.[3] Drug users (injecting drug users [IDUs]) represent the highest risk group for acquiring HIV and in some Eastern European and Asian countries almost all reported HIV cases are related to drug addicts. Studies and statistics show that the age of using drugs in these countries has reduced and that drug abuse is rapidly on the rise.[4,5] Besides, most addicts are not aware that they are infected with HIV.[6]
According to estimates 3.4% of the world population or 4.7% of the world population aged 15 and older are drug addicts. In Iran, between 1.7% and 2.8% of the population aged 15 and older and 7.5% and 8% of the country's adult population are addicted to opium.[7] According to a report by the World Health Organization (WHO), the numbers of countries that report HIV infection in drug addicts are on the rising and this problem is particularly severe in developing countries.[8]
According to the Ministry of Health and Medical Education to 92/7/1 in sum 27,041 persons with AIDS/HIV has been detected in the country. About 89.3% of men and 10.7% of women have been infected. 45.9% of patients at 25–34 have been that highest proportion among the age groups into account. The total of infection cases so far have been records in the country, sequencing intravenous drug abuse (68.15%), sexual intercourse (12.66%), blood and blood products (0.9%), mother to child (1.22%), (17.05%) is unknown.[9]
The majority of HIV infection cases in Iran are IDUs. Injection drug use-related HIV transmission accounts for 5–10% of HIV cases in the world, 36% in the US and more than 60% of infection cases in Iran.[7,9] Studies have showed that IDU's are able to change their behaviors in a manner to protect themselves and others from HIV infection, and this point is very important for researchers that study in this field.[8] According to the WHO the only effective way to combat AIDS is health education and vulnerable groups should be prioritized.[10] HIV infection are highest among drug users and the problem of addiction combined with issues such as poverty, illiteracy, unemployment, and homelessness contributes to the risk of HIV infection.[10] The emerging HIV epidemic in Iran is serious and doubtlessly the rise of this epidemic will have a vast negative impact on the economic, social, and political situation in the country. Thus, efforts to contain this epidemic in Iran are a national obligation and urgent intervention strategies in the risk groups specifically injecting drug users is key to solving this problem.[11]
Unawareness of or disregard for correct health behaviors is inevitable in any society. Individuals and societies require learning correct health behaviors through education in order to recognize and adopt a good lifestyle, maintain their health and prevent diseases.[12] The only way to combat this disease in the absence of treatment and effective vaccines is health education and behavior change.[13] Informing the society can be very effective in reducing HIV infections.[14] Designing and implementing an effective HIV prevention and control program based on reducing high-risk behavior has turned into a major challenge for health workers and researchers all over the world.[15] The value of educational health programs are assessed based on their effectiveness and their effectiveness is highly dependent on the correct utilization of theories and models in teaching health education. In other words, the existence of an appropriate support theory in accordance with the major health needs increases the effectiveness of educational health programs.[16]
The effectiveness of the health belief model (HBM), which has been used as a theoretical framework in this study has been proved to be very useful in predicting AIDS preventive behaviors by different researchers. The HBM constructs have also proved to be effective in HIV/AIDS education programs as it helps understand behaviors that prevent AIDS and drug abuse.[17,18] The health belief model is one of the oldest health behavior theories and different researchers have applied it in different behavioral fields in order to design and evaluate behavioral interventions. Plus the effectiveness of this model has been proved in the area of AIDS education in different internal and foreign researches.[19,20,21]
Based on this model, a person's decision to adopt a certain health behavior is influenced by three main categories of variables; individual perceptions, modifying factors and the likelihood of action. Individual perceptions refer to the subjective ideas regarding one's well-being, factors that affect the understanding of the disease or illness and the consequences of adopting a certain health behavior. Modifying factors are those variables, which affect an individual's appraisal of risk for disease or illness and include demographic variables, perceived threat of disease and ques to action: Which are influences external to the individual that provide a stimulus for activity.[10,16,22,23] Likelihood of action discusses the collective weighing of risks, benefits and costs in order to determine whether to take action or not. In fact, the health belief model allows us to study the probable psychological factors that influence individuals’ decision-making process.[22]
According to this model in order to implement HIV prevention methods, people should understand their chances of being infected by AIDS (perceived susceptibility), understand the seriousness of its symptoms in all physical, social, psychological, and economical aspects (perceived severity) and with the how-to information they receive from others or in the form of incentives (cues to action) they believe in the efficacy of the advised action, its benefits and applicability (perceived benefits) and find the deterring factors in taking the action less costly (perceived barriers), so that ultimately they take the measures.
The researcher considers the HBM constructs of self-efficacy, perceived benefits and perceived barriers as important factors that influence health behaviors, specifically HIV/AIDS prevention behaviors. The constructs of self-efficacy, perceived benefits and perceived barriers are common in most health behavior theories and are three of the major components of the health belief model. Self-efficacy refers to the depth of one's trust in his/her ability.[24] The association between self-efficacy and AIDS prevention behaviors has been proved in different researches and can be effective in reducing high-risk behavior, which leads to HIV infection.[25] The shallow analysis of benefits minus barriers can happen in a situation where individual assess the benefits of taking of an action more costly, dangerous, unlikeable, saddening, and time-consuming compared with the barriers to it. Based on such an analysis, an individual adopts a certain behavior or refrains from doing so.[3] In order to change and improve health behaviors, professional health workers apply the constructs of self-efficacy, perceived benefits and perceived barriers as a theoretical basis in many of their health education programs. In fact, understanding factors that influence health behaviors can develop better health promoting strategies and success indicators can be chosen in a more logical manner.[26] A study by Mahmoud Karimi[3] and researches[27,28,29,30,31] prove the predictive nature of the health belief model. This research was carried out due to the fact that there have been very few educational intervention programs as to lower high-risk behaviors in drug addicts based on this very model. The current research studies the influence of education on knowledge, perceived self-efficacy, perceived benefits and barriers as well as the performance of Khorramabad drug addicts when it comes to AIDS prevention behaviors.
MATERIALS AND METHODS
A quasi-experimental and pre- to post-test research design was used to assess the impact of the HIV/AIDS educational intervention program. The selected population included 88 male addicts that were being kept in a rehabilitation center. The samples were selected from four different centers; 44 out of 2 of the centers were regarded as the intervention group and 44 of the 2 other centers as the control group. Due to limitations in the sample size, the samples were selected through the census method. And all of the addicts were being kept in the rehabilitation centers were entered to research.
In the rehabilitation centers, HIV prevention and education programs are not offered. Patients are monitored 24 h, 7 days a week by trained staff. Apart from addicts that are under treatment by caregivers, no specific drugs are given to other patients. The researcher presented an official introduction letter from Isfahan University of Medical Sciences to the drug rehabilitation center in Khorramabad. In the beginning of the study, sufficient information regarding the aim of the study was given to the participants, and they were reassured that their data will remain confidential.
Data gathering was undertaken by a questionnaire designed in four sections including:[1] Personal information (age, marital status, occupation, and…);[2] the second segment consisted of 10 questions to evaluate the knowledge level about HIV/AIDS pointed on a scale from 0 and 1 meaning that for a correct answer, 1 point and for a wrong answer or “I don’t know no” no point was given.[3] The third segment consisted of 10 questions related to the perceived self-efficacy regarding AIDS preventive measures using a 4-point Likert scale, which ranged from “strongly agree” to “strongly disagree.” Four-eight questions regarding the perceived benefits related to AIDS preventive measures with their answers scored on a 4 Likert scale that ranged from strongly agree to strongly disagree. Five-seven questions related to the perceived barriers related to AIDS preventive, which were also measured on a 4 Likert scale. Six-six yes/no questions related to the Practice, which were scored 0 and 1 therefore the maximum points acquired was 6 and the minimum.
A knowledge and practice questionnaire was developed by the researcher. In order to evaluate the scientific validity of the questionnaire it was handed out to a couple of professional and experienced health education professors working at Isfahan University of Medical Sciences. As to examine the scientific reliability of the questionnaire the internal consistency test was used and the Cronbach's alpha was calculated (Cronbach's alpha = 76.3%).
The self-efficacy, perceived benefits and barriers questionnaire used in this research was devised by Mahmoud Karimi under the title “Perceived benefits and perceived barriers to preventive behaviors of AIDS in addicts in Zarandieh”.[26] Its validity and reliability of the questionnaire through content validity and test–retest methods was evaluated. Thus, the questionnaire was designed with the resources and scientific articles and polls research experts and use their feedback has been confirmed. Its reliability test–retest correlation coefficient Cronbach's alpha was calculated as 76% of health belief model.
The information from the research departments were gathered through interviews (from the illiterate or less literate) and written responses from the samples themselves and analyzed through the SPSS 20 (IBM Corp. in Armonk, NY) descriptive analyses (means, standard deviations, and ranges) and analytical statistical methods (paired t-tests, independent t-test, Chi-square, and analysis of covariance).
After extracting the necessary information from the pretest questionnaires, the results were analyzed and an educational model was designed. Pirzadeh conducted a study on students (27) in which educational interventions were implemented in 2 × 45 min sessions. These sessions were based on acquainting drug addicts with AIDS, its transmission and prevention along with improving the perceived self-efficacy, benefits of and barriers to this disease. The educational sessions was carried out among groups of 10–12 inside the center by means of speeches, face to face Q and As, group discussions and displaying educational films. Every group had 3 × 1.5 h sessions. To sustain the educational program, pamphlets, booklets, and educational films were distributed among the treatment group. The control group received no kind of education. Given that the addicts were retained in the center for an average 1 month period, to carry out the research phone contacts had to be made with the samples to complete the data gathering process. Therefore, 2 months after the educational intervention, the samples were invited to come over to complete posttest questionnaires through phone or personal visits.
RESULTS
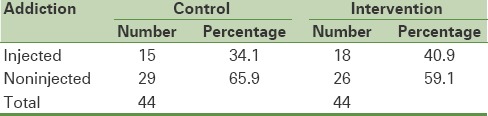
The mean age of the study participants was 33.31 years. Chi-square tests showed that there was no statistically significant difference between the two groups in terms of their marital status (P = 0.32), with married participants having the highest frequency and widowed participants, the lowest. The tests also showed that there was no significant difference between the two groups in terms of substance abuse (injectable and noninjectable drugs) (P = 0.5). The Mann-Whitney test showed that there was no significant difference between the two samples based on education level (P = 0.34) with the participants having less than a high school diploma having the highest frequency and participants with a master's degree the least [Tables 1–3].
Table 1.
Marital status of participants (intervention and control groups)
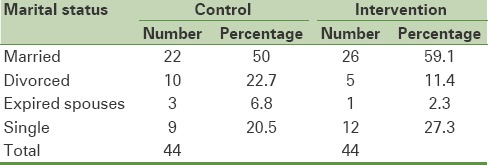
Table 3.
Distribution of participants based on their educational status
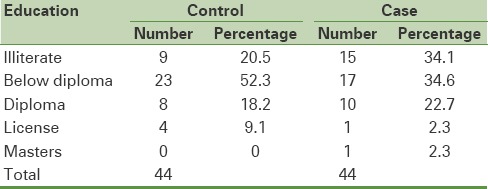
Table 2.
distribution of participants based on their addiction status
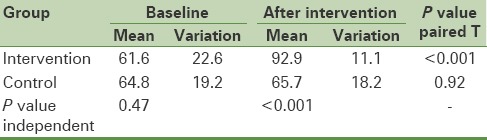
Paired t-test in the intervention group showed that after the intervention, the mean score for knowledge had increased; however, it was not statistically significant [Table 4]. Besides, this test showed that there was no significant difference in the mean score for perceived self-efficacy in the control group before and after the intervention. The independent t-test showed that before the intervention, the mean scores of perceived self-efficacy in the two groups had no significant differences with one another but after the intervention, the intervention group showed higher scores than the control group.
Table 4.
The mean score of knowledge about HIV preventive behaviors before and after intervention in the two groups
The paired t-test showed that the mean score of perceived benefits had increased significantly in the intervention group after the intervention, but it was not statistically significant (P = 0.17). This test also showed that there was no significant difference in the control group's mean score of perceived self-efficacy before and after the intervention (P = 0.18). The independent t-test showed that there was no significant difference between both groups’ mean score of perceived self-efficacy before the intervention (P = 0.91), but following the intervention the mean score of perceived self-efficacy in the intervention group was significantly higher than the control group (P = 0.04) [Table 5].
Table 5.
Mean scores of health belief model constructs before and after intervention in the treatment group
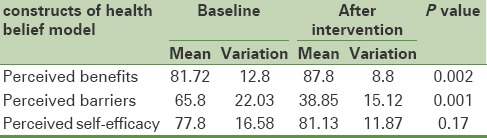
The paired t-test showed that in the intervention group, the mean score of perceived benefits had significantly increased after the intervention compared to before it (P = 0.002) but in the control group, no significant difference was seen (P = 0.16). The independent t-test showed that before the intervention, there was no significant difference between both groups’ mean score of perceived benefits (P = 0.49), but after the intervention the mean score of perceived benefits in the intervention group was significantly higher than the control group (P = 0.02) [Table 5].
The paired t-test showed that after the intervention the mean score of perceived barriers had significantly decreased in both the intervention and control groups, compared to before the intervention (P < 0.001). The independent t-test showed that before the intervention, there was no significant difference between the mean scores of perceived barriers in both groups (P = 0.59), but after the intervention the mean score of perceived barriers had significantly decreased in both groups (P = 0.004) [Table 5].
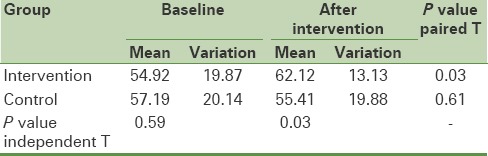
The paired t-test showed that in the intervention group, the mean score of performance regarding Aids preventive behaviors increased significantly after the intervention (P = 0.03), but in the control group there was no significant difference between the mean score of performance before and after intervention (P = 0.61). The independent t-test showed that before the intervention there was no significant difference between the mean scores of performance in both groups (P = 0.59), but after the intervention the mean score of performance in the intervention group had raised significantly higher than the control group (P = 0.03) [Table 6].
Table 6.
The mean score of performance about HIV preventive behaviors before and after intervention in the two groups
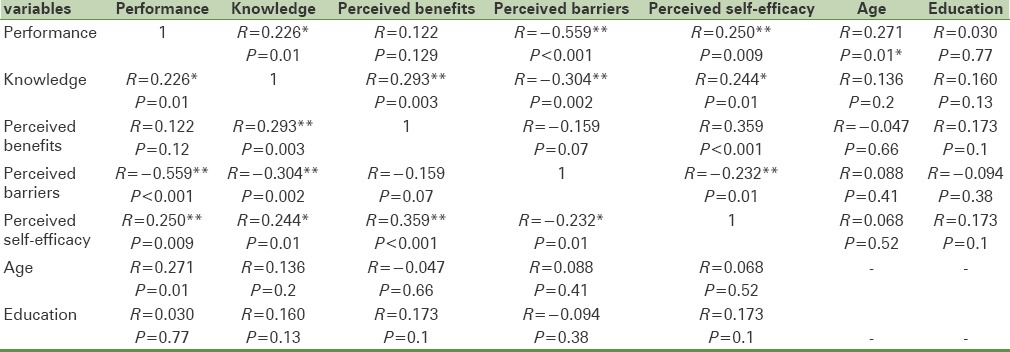
The correlation coefficient showed that age correlated positively with performance (P = 0.01) but there was no correlation between education with knowledge, performance, self-efficacy, and perceived benefits, barriers.
Knowledge positively correlated with performance (P = 0.01). Perceived self-efficacy correlated positively with performance (P = 0.009). Knowledge correlated positively with perceived benefits (P = 0.003). Knowledge correlated negatively with perceived barriers (P = 0.002). Benefits positively correlated with perceived self-efficacy (P < 0.001) [Table 7].
Table 7.
Correlations
DISCUSSION AND CONCLUSION
Poor health behaviors are seen in all kinds of societies whether illiterate, literate, rich, or poor. Culture imbibes into us the knowledge of good and bad behavior. People's readiness to recognize and pursue positive lifestyles in order to maintain their health and prevent diseases requires the shaping of their behaviors.[32]
The results of this study showed that educating male drug addicts based on the health belief model, increases their knowledge, perceived benefits and barriers, and improves their overall performance. The knowledge levels of drug addicts in the intervention group before and after the intervention showed a significant difference. This change shows the effects of the educational intervention in increasing the awareness of addicts. The results of this study showed that implementing the health education program had a significant effect on improving the awareness and performance of the researched samples concerning the AIDS disease. These results comply with the results of studies carried out by Niknami et al. on the addicts in Kermanshah,[8] Zareban's study on the seamen of Chabahar,[12] and Clark's study on American women.[33] Informing people about the ways of HIV transmission, the preventive measures to take against it and its acceptance from people as to change dangerous and risky behavior is effective and would control and contain the disease.[32]
In this study, there was a significant relationship between knowledge and perceived benefits of and barriers to adopting AIDs prevention behavior meaning that when a person's knowledge regarding the preventive behaviors against AIDS increases, the perceived benefits derived from taking preventive measures against AIDS would rise and the barriers to carry out these measures would decrease.
The results of this study show that the mean score of perceived benefits after the intervention significantly increased in the intervention group (P = 0.002). The effectiveness of education on increasing the perceived benefits related to the preventive behaviors of AIDS in addicts was also seen in the studies conducted by Koopman and Voll.[20] Lollis et al., (23) and Karimi et al. (3).
Various studies have shown the strong relationship between perceived benefits and taking preventive measures; an individual's understanding of the benefits of a specific measure paves the way for him/her to take it.[34]
The results of this study showed that the mean score of perceived barriers before education was 65.8, which reduced significantly to 38.85 (P = 001). The effectiveness of education on decreasing the perceived barriers-related to AIDS prevention was seen in studies by Karimi et al. on drug addicts and Pirzadeh and Sharifiradon students.[27] In other studies, it has also been confirmed that educational programs have a positive and significant effect on reducing the perceived barriers, which complies with our study.[3,35,36] A study by Adij in Ghana also demonstrated that people with low perceived barriers use condoms in their sexual intercourses almost 6 times more than other people.[37]
The results of this study showed that before the intervention, there was no significant difference between the mean score of perceived self-efficacy in both groups (P = 0.91), but after the intervention, the mean score of perceived self-efficacy in the intervention group was significantly higher than the control group (P = 0.04). Studies examining the relationship between perceived self-efficacy and healthy behaviors have shown that self-efficacy has a strong effect on health behaviors and some studies suggest that self-efficacy determines >50 % variance of health behaviors.[38] The role of self-efficacy as an important basis for reducing risky behavior related to AIDS has been confirmed in studies conducted by Zamboni,[39] Smith[40] Bandora.[41] Improving self-efficacy is proposed as an intermediate goal to reduce HIV infection. According to the social cognitive theory, a person who has low self-efficacy is more probable to engage in a dangerous-risky behavior compared to a person with high self-efficacy.[42] In Adih's study in Ghana, people with high self-efficacy had used condoms 3 times more than those with low self-efficacy.[37] Kasen's study showed that students who had a low self-efficacy had engaged in sexual activity twice more than students with high self-efficacy and they had used condoms 5 time less.[43] Lin's study in Taiwan also showed that self-efficacy is the most reliable predictor in safe or unsafe sexual behavior.[28]
The results of this study showed that there is a significant relationship between the perceived benefits of applying preventive AIDS behavior and perceived self-efficacy meaning that with the growth of the perceived benefits of a person regarding AIDS preventive behaviors, the self-efficacy of the person toward practicing this behavior increases. Besides, with the growth of perceived self-efficacy, practicing preventive behaviors also increases. According to the results of this study, there is a significant relationship between the perceived self-efficacy toward taking preventive measures and the actual adopting of those behaviors.
Future studies should contain strategies to increase perceived self-efficacy and benefits as well as strategies to decrease perceived barrier to adopt preventive behaviors.[3]
The results of this study show that there is a significant relationship between the demographic variable of age and the variable of performance in a way that the higher the age, the performance of the samples improved. Plus the demographic variable of age had no relationship with knowledge or any other studied construct and from this aspect it complies with the results attained by Momenion the students in Yasouj city[44] and Mahmoud Karimi on Zarandiyeh addicts.[3] In addition, the results showed that there was no significant relationship between the samples’ education and awareness, performance and any of the other studied constructs in this study, which does not comply with studies by Karimi on the students of Yazd[45] and Niknami on self-proclaimed addicts in Kermanshah[8] in the aspect that there is a significant relationship between the education level and performance. However, it did comply with Mahmoud Karimi's study[3] in the sense that there was no significant relationship between the level of education and performance.
Among the limitations of this study: There was a lack of cooperation among officials at the addicts rehabilitation centers due to their dislike of the educational subject (AIDS), the physical and psychological sickness of the addicts did not made it unlikely for them to take part in the educational sessions or complete the questionnaires, the time-consumingness of filling out the questionnaires for illiterate and less literate addicts, summoning up addicts to complete posttest questionnaires and their lack of cooperation.
The results of this study show that the health education program designed based on the health belief model had a significant effect on improving the level of awareness of addicts as well as their perceived benefits, barriers and self-efficacy toward adopting preventive AIDS behavior in Khorramabad, which is in compliance with the results of[2,3,27,28,29,30,31] studies.
Financial support and sponsorship
Deputy of Research and Technology of Isfahan University of Medical Sciences.
Conflicts of Interest
There are no conflicts of interest.
REFERENCES
- 1.Taeri K, Kasaeian N, Nobari RF, Ataei B. The prevalence of hepatitis B, hepatitis C and associated risk factors in intravenous drug addicts (IVDA) with HIV in Isfahan. Journal of Isfahan Medical School. 2008;26(90) [Google Scholar]
- 2.Rahmati Najarkolaei F, Niknami S, Amin Shokravi F, Ahmadi F, Jafari M, Rahnama P. The implication of health belief model in planning educational programmes for preventing HIV/AIDS among university students. Payesh. 2009;8(4):349–59. [Google Scholar]
- 3.KARIMI M, Ghofranipour F, HEYDARNIA AR. The effect of health education based on health belief model on preventive actions of AIDS on addict in Zarandieh. 2009 [Google Scholar]
- 4.Sanaei Moghadam E, Sargolzaie N, Karami Sh SM, Khosravi S, Fadaie M. Knowledge, attitude and practice regarding blood donation among Sistan and Baluchistan province blood donors about HIV. Journal of Blood. 2009;6(2):117–23. [Google Scholar]
- 5.Dolan KA, Niven H. A review of HIV prevention among young injecting drug users: A guide for researchers. Harm Reduction Journal. 2005;2(1):5. doi: 10.1186/1477-7517-2-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Safdar S, Mehmood A, Abbas SQ. Prevalence of HIV/AIDS among jail inmates in Sindh. Prevalence. 2009 [PubMed] [Google Scholar]
- 7.Amani F, Sadeghieh S, Salamati P. Features addicts referred to their centers referrals Ardabil (Persian) J Iran Inst Health Sci Res. 2005;4(5):55–9. [Google Scholar]
- 8.Niknami S, Hatami A, Heidarnia A. The Effect of Health Educational Program on Preventing AIDS in Self-reported Addicts’ Wives (Kermanshah 2004) Journal of Kermanshah University of Medical Sciences. 2007;11(2) [Google Scholar]
- 9.Health Mo. Tehran: Center for Disease Control; 2013. Recent Statistics on HIV/AIDS in Iran. [Google Scholar]
- 10.Ghafari M, Niknami S, Kasemnejad A. Design and validity HIV/AIDS questionnaire in teen Kermanshah. Journal of Behbood. 2005;11(1):38–43. [Google Scholar]
- 11.Fahoodi B. Tehran: Nashrehseda Publication; 2003. HIV/AIDS and Injection Drug Users Tehran. [Google Scholar]
- 12.Zareban I, Hedarnia A, Rakhshani F, Jabbari H, Abdollahi-Mohammad A. The effect of health educational program on the knowledge and practice sailors towards HIV/AIDS in Chabahar. J Univ Med Sci Health Serv. 2006;8(1):29–33. [Google Scholar]
- 13.Gashtasbi A, Vahanisadat M, Rezai N. Survey of knowledge towards HIV/AIDS among Rasht city women. Armaghan Danesh J Khorasanrazavi Univ Med Sci Health Serv. 2007;10(1):29–33. [Google Scholar]
- 14.Nojoomi M, Anbari K. Acomparison of quality of life in HIV/AIDS patients and control group. Iran J Univ Med Sci Health Serv. 15(1):169–75. [Google Scholar]
- 15.Rhodes T, Platt L, Sarang A, Vlasov A, Mikhailova L, Monaghan G. Street policing, injecting drug use and harm reduction in a Russian city: A qualitative study of police perspectives. Journal of Urban Health. 2006;83(5):911–25. doi: 10.1007/s11524-006-9085-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sharifi-rad G, Hazavei MM, Hasan-zadeh A, Danesh-amouz A. The effect of health education based on health belief model on preventive actions of smoking in grade one, middle school students. Arak Medical University Journal. 2007;10(1):79–86. [Google Scholar]
- 17.Gahanloo A, Ghofranipour F, Vafaei M, Kimiagar M, Heidarnia A, Sobhani A. Assessment HBM structures along with DBA1C in diabetic patients with optimum and un-favorable diabetic. Hormozgan Medical Journal. 2008;12(1):37–42. [Google Scholar]
- 18.Karimy M, Hasani M, Khoram R, Ghaffari M, Niknami S. The effect of education, based on health belief model on breast self-examination in health liaisons of Zarandieh city. Zahedan Journal of Research in Medical Sciences. 2008;10:0. [Google Scholar]
- 19.Kinsler J, Sneed CD, Morisky DE, Ang A. Evaluation of a school-based intervention for HIV/AIDS prevention among Belizean adolescents. Health education research. 2004;19(6):730–8. doi: 10.1093/her/cyg091. [DOI] [PubMed] [Google Scholar]
- 20.Volk JE, Koopman C. Factors associated with condom use in Kenya: A test of the health belief model. AIDS education and prevention. 2001;13(6):495–508. doi: 10.1521/aeap.13.6.495.21438. [DOI] [PubMed] [Google Scholar]
- 21.Glanz K, Rimer BK, Viswanath K. Health behavior and health education: Theory, research, and practice: John Wiley and Sons. 2008 [Google Scholar]
- 22.Rahmati F, Niknami S, Aminshokravi F, editors. Evaluation HBM Model on planning preventive of HIV/AIDS in the students. Tehran University. Proceedings of the 3rd National Congress on Health Education and Promotion. 2008 [Google Scholar]
- 23.Lollis CM, Johnson EH, Antoni MH. The efficacy of the health belief model for predicting condom usage and risky sexual practices in university students. AIDS Education and Prevention. 1997 [PubMed] [Google Scholar]
- 24.Peyman N, Heidarnia A, Ghofranipour F, Kazemnejad A, Khodaee GH, Amin Shokravi F. The relationship between perceived self-efficacy and contraceptive behaviors among Iranian women referring to health centers in Mashad in order to decrease unwanted pregnancies. Journal of Reproduction and Infertility. 2007:78–90. [Google Scholar]
- 25.Murphy DA, Stein JA, Schlenger W, Maibach E. Conceptualizing the multidimensional nature of self-efficacy: Assessment of situational context and level of behavioral challenge to maintain safer sex. Health Psychology. 2001;20(4):281. [PubMed] [Google Scholar]
- 26.Karimi M, Niknami S. Self-efficacy and perceived benefits/barriers on the AIDs preventive behaviors. Journal of Kermanshah University of Medical Sciences. J Kermanshah Univ Med Sci. 2011;15(5) [Google Scholar]
- 27.Pirzadeh A, GhR S. Effect of educational program on knowledge and health belief model structures about acquired immune deficiency syndrome (AIDS) among high school female student in Isfahan, Iran. Journal of Gorgan University of Medical Sciences. 2012;14(3):66–71. [Google Scholar]
- 28.Lin P, Simoni JM, Zemon V. The health belief model, sexual behaviors, and HIV risk among Taiwanese immigrants. AIDS Education and Prevention. 2005;17(5):469–83. doi: 10.1521/aeap.2005.17.5.469. [DOI] [PubMed] [Google Scholar]
- 29.Falck RS, Siegal HA, Wang J, Carlson RG. Usefulness of the health belief model in predicting HIV needle risk practices among injection drug users. AIDS Education and Prevention. 1995 [PubMed] [Google Scholar]
- 30.Yep GA. HIV prevention among Asian-American college students: Does the health belief model work? Journal of American College Health. 1993;41(5):199–205. doi: 10.1080/07448481.1993.9936326. [DOI] [PubMed] [Google Scholar]
- 31.Miri M, Fani M, MOTALEBI M, Nazemi H. USING HEALTH BELIEF MODEL ST DS ON MEDICAL STUDENTS. 2002 [Google Scholar]
- 32.Karimy M, Niknami S, Hedarnia A. The effect of health educational program on preventing AIDS in addicts prisoners Geserhesar Tehran. Ghazvin J Univ Med Sci Health Serv. 2004;8(1):40–8. [Google Scholar]
- 33.Clark JN, Van Eck RN, King A, Glusman B, McCain-Williams A, Van Eck S, et al. HIV/AIDS education among incarcerated youth. Journal of Criminal Justice. 2000;28(5):415–33. [Google Scholar]
- 34.Organization WH. New approaches to health education in primary health care: Report of a WHO expert committee [meeting held in Geneva from 12 to 18 October 1982] 1983 [Google Scholar]
- 35.Hounton SH, Carabin H, Henderson NJ. Towards an understanding of barriers to condom use in rural Benin using the Health Belief Model: A cross sectional survey. BMC Public Health. 2005;5(1):8. doi: 10.1186/1471-2458-5-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Eshrati B, Asl RT, Dell CA, Afshar P, Millson P, Kamali M, et al. Preventing HIV transmission among Iranian prisoners: Initial support for providing education on the benefits of harm reduction practices. Harm Reduct J. 2008;5(21):1–7. doi: 10.1186/1477-7517-5-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Adih WK, Alexander CS. Determinants of condom use to prevent HIV infection among youth in Ghana. Journal of Adolescent Health. 1999;24(1):63–72. doi: 10.1016/s1054-139x(98)00062-7. [DOI] [PubMed] [Google Scholar]
- 38.Mazloomy M, Mehri A, Morowatisharifabad M. The relationship of health behavior with Self-esteem and self-efficacy in students of Yazd Shahid Sadooghi University of Medical Sciences. Journal of Kerman university of medical sciences. 2006;3(2):111–7. [Google Scholar]
- 39.Zamboni BD, Crawford I, Williams PG. Examining communication and assertiveness as predictors of condom use: Implications for HIV prevention. AIDS education and prevention. 2000 [PubMed] [Google Scholar]
- 40.Smith KW, McGraw SA, Costa LA, McKinley JB. A self-efficacy scale for HIV risk behaviors: Development and evaluation. AIDS Education and Prevention. 1996 [PubMed] [Google Scholar]
- 41.Bandura A. Perceived self-efficacy in the exercise of control over AIDS infection. Evaluation and program planning. 1990;13(1):9–17. [Google Scholar]
- 42.Ghafari M. Tehran: Tarbiat Modares university; 2007. Comparing the efficacy of health belief model and its integrated model in AIDS education among male high school students in Tehran. [Google Scholar]
- 43.Kasen S, Vaughan RD, Walter HJ. Self-efficacy for AIDS preventive behaviors among tenth grade students. Health Education and Behavior. 1992;19(2):187–202. doi: 10.1177/109019819201900204. [DOI] [PubMed] [Google Scholar]
- 44.Momeni E, Karimi Z, Malekzadeh J, Moshfe H. The knowledge level and attitude of pre-university students of Yasuj city towards AIDS in 2003. Dena, Quarterly Journal of Yasuj Faculty of Nursing And Midwifery. 2006;1(1):41–9. [Google Scholar]
- 45.Karimy M, Sadatgoo L. Survey knowledge and atittude towards HIV among Yazd City. Yazd J Univ Med Sci Health Serv. 2003;11(1):5–10. [Google Scholar]