

Abstract
Liver Imaging Reporting and Data System (LI-RADS) is a system for interpreting and reporting of computed tomography and magnetic resonance imaging of the liver in patients at risk for hepatocellular carcinoma (HCC). LI-RADS has been developed to address the limitations of prior imaging-based criteria including the lack of established consensus regarding the exact definitions of imaging features, binary categorization (either definite or not definite HCC), and failure to consider non-HCC malignancies. One of the most important goals of LI-RADS is to facilitate clear communication between all the personnel involved in the diagnosis and treatment of HCC, such as radiologists, hepatologists, surgeons, and pathologists. Therefore, clinicians should also be familiar with LI-RADS. This article reviews the LI-RADS diagnostic algorithm, and the definitions and management implications of LI-RADS categories.
Keywords: Hepatocellular, Carcinoma, Guideline, Diagnosis, Algorithms
INTRODUCTION
Liver Imaging Reporting and Data System (LI-RADS) is a system for interpreting and reporting of computed tomography (CT) and magnetic resonance imaging (MRI) examinations of the liver in patients at risk for hepatocellular carcinoma (HCC).
As imaging plays an important role in the management of patients with or at high risk for HCC, several worldwide scientific organizations and societies have issued guidelines for appropriate utilization of imaging for HCC diagnosis [1-6]. However, the current imaging-based diagnostic criteria have several limitations, including the lack of established consensus regarding the exact definitions of imaging features, binary categorization (either definite or not definite HCC), and failure to address non-HCC malignancies and vascular invasion. To address the limitations of prior systems, American College of Radiology (ACR) supported the development of LI-RADS with a goal of standardizing the interpreting, reporting, and data collection of HCC imaging, and its first version was officially launched in 2011.
Prior imaging-based diagnostic systems have not precisely defined or illustrated the imaging features used to assess hepatic lesions, which leads to ambiguity in implementation and limits reproducibility both in clinical care and in research [7]. For example, should arterial phase hyperenhancement rely on higher attenuation/signal in the arterial phase or calculated change in intensity/signal between pre- and post-contrast enhancement? In contrast, LI-RADS provides the detailed descriptions and supporting illustrations of all imaging features defined [8].
Prior systems generally categorize hepatic lesions as positive, negative, or indeterminate for HCC; for the latter biopsy is suggested. However, in these systems, the indeterminate category can be very broad and include lesions that are likely to be benign and thus could safely be followed up without biopsy. By expanding the “indeterminate” category into probably benign, intermediate probability of HCC, and probably HCC (LI-RADS categories 2, 3, and 4, respectively), LI-RADS aims for more nuanced and personalized clinical decision-making.
Prior systems only focus on HCC, rather than address the entire spectrum of hepatic lesions. However, it is clinically important to differentiate between HCC and other malignancies such as intrahepatic cholangiocarcinoma (ICC) or hepatobiliary biphenotypic tumor, because the prognosis and management differ considerably. In addition, existing systems neglect the imaging criteria for the diagnosis of gross vascular invasion, which has major implications in staging and treatment [9]. In contrast, LI-RADS provides separate categories that can be assigned to suspected non-HCC malignancies or macrovascular invasive HCC.
LI-RADS is a dynamic system, developed as the product of existing data and expert radiological and clinical consensus, that will continue to be refined and updated as experience and validating data accrue and in response to multidisciplinary expert input and actively solicited user feedback [10]. Since its introduction in 2011, LI-RADS has been updated once in 2014. The latest version (currently ver. 2014) of LI-RADS is available online with extensive supporting information (http://www.acr.org/Quality-Safety/Resources/LIRADS).
This article aims to introduce LI-RADS to clinicians who are not radiologists, emphasizing how to use the diagnostic algorithm, interpret LI-RADS categories, and apply LI-RADS to clinical practice.
THE SCOPE OF APPLICATION
LI-RADS applies only to individuals at high risk for HCC who are candidates for or already enrolled in a surveillance program for HCC. Thus, LI-RADS should not be applied to those who are not at risk for HCC development, and this was to preserve high positive predictive value for HCC diagnosis. For example, hepatic adenoma or angiomyolipoma can also show the typical enhancement pattern of HCC (arterial hyperenhancement and washout appearance), but in most cases these cases are found in individuals who are not at high risk for HCC and thus should not be diagnosed based on imaging diagnosis criteria. It should be noted that LI-RADS does not specifically define this at-risk population, nor prescribe the criteria or frequency for HCC surveillance, because these issues are already addressed by the American Association for the Study of Liver Diseases (AASLD) and other organizations [10].
LI-RADS is intended to be used with both liver CT and MRI. However, recent studies reported substantial discordance between CT and MRI in LI-RADS categorization, mainly because of the superiority of MRI in detection of the presence of imaging features or lesions themselves [11,12]. Other studies validating the diagnostic performance of LI-RADS published so far have been performed using MRI, which reported high (>95%) positive predictive value and specificity [13,14]. Therefore, it is probably safe to assume that LI-RADS categorization of focal liver observations is dependent on imaging modality, at least until proven otherwise.
There are two main types of contrast media currently used for MRI, extracellular and hepatobiliary agents (such as gadoxetic acid disodum [Primovist, Bayer Schering Pharma, Berlin, Germany]); the latter initially distribute in the extracellular fluid compartment, just as extracellular agents do, and are subsequently taken up by hepatocytes, providing the dual benefit of dynamic imaging capability as well as delayed hepatobiliary phase imaging. Although the 2014 version of LI-RADS has incorporated hepatobiliary contrast agents into the diagnostic algorithm, the fact that LI-RADS has been established from our experiences with extracellular agents has not changed, and some features unique to hepatobiliary phase imaging are included only as ancillary features. More importantly, evaluation of major features is highly likely to be affected by the use of hepatobiliary agents, but this has not yet been sufficiently investigated [15]. For example, early parenchymal enhancement after administration of hepatobiliary agents may cause ‘pseudo-washout’ or mask the presence of capsule appearance [15-17], but we do not know its exact influences on LI-RADS categorization yet. For example, some hepatic hemangiomas might show relatively low signal intensity because of the uptake of hepatobiliary contrast agent by the surrounding liver parenchyma in the delayed phase, not because of true washout, thus is called pseudo-washout and can mimic HCC. In addition, delayed enhancement of tumor capsule can be masked by concurrent enhancement of surrounding liver parenchyma, making it difficult to recognize the capsule appearance.
LI-RADS DIAGNOSTIC ALGORITHM
How to use the diagnostic algorithm
The LI-RADS diagnostic algorithm is intended to mimic the natural thought process of a radiologist who evaluates a hepatic observation found in patients at risk for HCC. An observation refers to an area with imaging features that differ from those of adjacent liver parenchyma. The term “observation” is preferred over the term “lesion”, because some observations are not true lesions but pseudo-lesions such as perfusion alterations or imaging artifacts.
The current (v. 2014) LI-RADS has a 5-step hierarchical diagnostic algorithm (Fig. 1). In the first step, you must determine whether a hepatic observation has previously been treated. If this is the case based on history and imaging findings, it is categorized as LR-Treated. If not, move on to the second step, in which you must determine whether the imaging features are diagnostic of benign lesions (LR-1) or suggestive but not diagnostic (LR-2). If so, LR-1 and LR-2 categories are assigned accordingly. If you think that it is neither definitely nor probably benign, move on to the next step. In the third step, if you think that even a small possibility of non-HCC malignancies exists based on the imaging features, LR-M category is assigned. If a malignancy other than HCC is thought to be unlikely, move on the fourth step, in which you must seek the presence of enhancing tumor in vein which indicates the presence of macrovascular invasive tumor (LR-5V). If the hepatic observation does not belong to any of the above-mentioned categories, you are in the final step. In this step, the observation is categorized as LR-3 (indeterminate), LR-4 (probably HCC), or LR-5 (definitely HCC) according to the likelihood of HCC, based primarily on the presence or absence of major imaging features (described below). The final category may be adjusted using ancillary features and some specified decision rules (described below).
Figure 1.
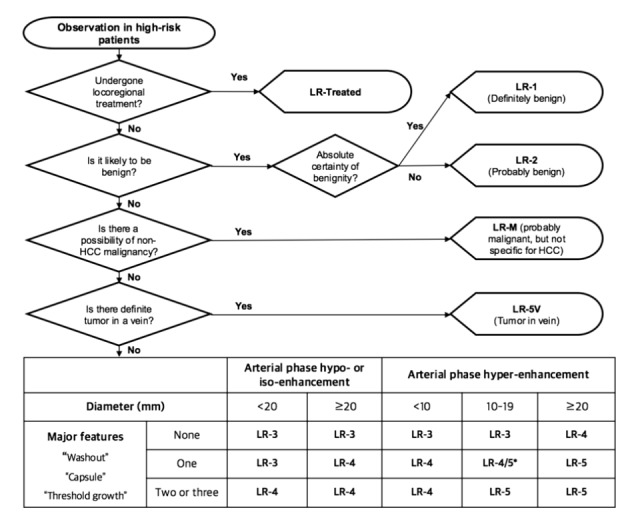
Summary schematic of LI-RADS 2014 diagnostic algorithm (adapted and modified from ACR LI-RADS content at: http://www.acr.org/Quality-Safety/Resources/LIRADS). LI-RADS, liver imaging reporting and data system; ACR, American College of Radiology; LR, LI-RADS. *Observations in this cell are categorized as LR-4 except as follows: LR-5g, if there is ≥50% diameter increase in ≤6 months, and LR-5us, if there is both “washout” and visibility as discrete nodules at antecedent surveillance ultrasound.
LI-RADS categories
Brief explanation of each LI-RADS category is presented here and also summarized in Table 1. A full description can be found at the official website of ACR (http://www.acr.org/Quality-Safety/Resources/LIRADS).
Table 1.
Definition, examples, and suggested management for each LI-RADS category
| LI-RADS category | Definition | Examples | Management |
|---|---|---|---|
| LR-1 | Definitely benign | Cyst, hemangioma, perfusion alteration, focal fat deposit or sparing, observation that disappears at follow-up | Continued routine surveillance |
| LR-2 | Probably benign | Confluent fibrosis, hypertrophic pseudomass, perfusion alteration, some cirrhosis- associated nodule | Continued routine surveillance |
| LR-3 | Indeterminate | Variable follow-up | |
| LR-4 | Probably HCC | Close follow-up, additional imaging, biopsy, or treatment | |
| LR-5 | Definitely HCC | Treatment without biopsy, radiologic T-staging | |
| LR-5V | Definitely tumor invading vein | Treatment without biopsy, radiologic T-staging | |
| LR-M | Probably malignancy but not specific for HCC | Intrahepatic cholangiocarcinoma (CC), combined HCC-CC, metastasis, lymphoma, post-transplant lymphoproliferative disease | Close follow-up, additional imaging, biopsy, or treatment |
| LR-Treated | Treated observation | Close follow-up to assess treatment response. May require re-treatment if persistent or recurrent tumor. |
LI-RADS, liver imaging reporting and data system; LR, LI-RADS; HCC, hepatocellular carcinoma.
LR-1 category is assigned only when there is 100% certainty that the observation is benign. Examples of definitely benign entities that can be categorized as LR-1 include hemangiomas, cysts, perfusion alterations, fat deposition or sparing, or focal scars. It must be noted that cirrhosis-associated nodules must not be categorized as LR-1, because non-invasive imaging is unable to reliably exclude the presence of neoplastic changes within nodules [9]. Instead, cirrhosis-associated nodules are either ignored (if they are indistinguishable from other background nodules) or, as described below, they are categorized as LR-2 or higher.
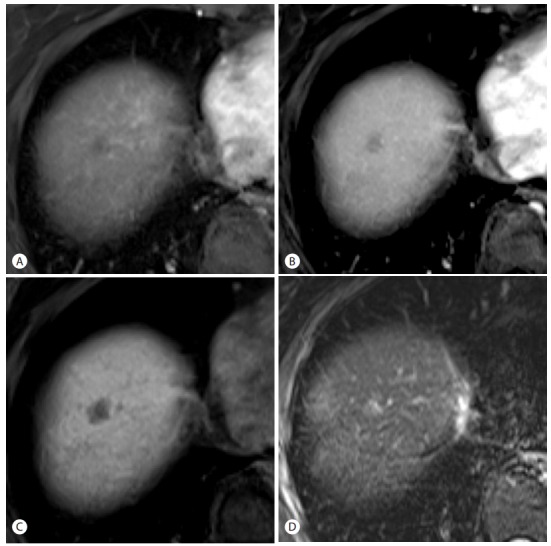
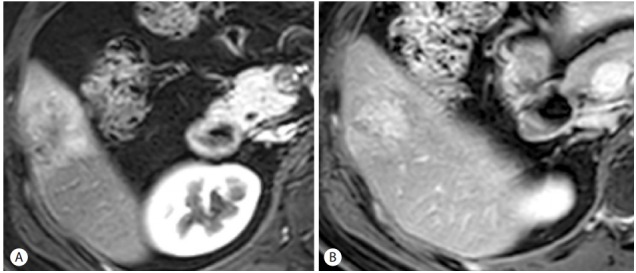
LR-2 category is assigned when the imaging features are suggestive, but not diagnostic, of a benign entity. Examples include hemangioma with an atypical enhancement pattern and some cirrhosis-associated nodules. In order for a cirrhosis-associated nodule to be categorized as LR-2, it should be homogeneous, less than 2 cm in diameter, and iso-enhancing relative to background liver (Fig. 2). Nodules that do not meet these criteria should be categorized as LR-3 or higher depending on their imaging features (Fig. 3).
Figure 2.

An observation that can be categorized as LR-2. At gadoxetic acid-enhanced MRI, a hepatic observation in the segment 5 of liver is distinguished from background liver as a 1.7 cm hyperintense nodule on pre-contrast T1-weighted image (arrow) (A), but shows no hyperenhancement in the arterial phase (B), no washout appearance in the portal venous phase (C), and iso-intensity on T2-weighted image (D).
Figure 3.
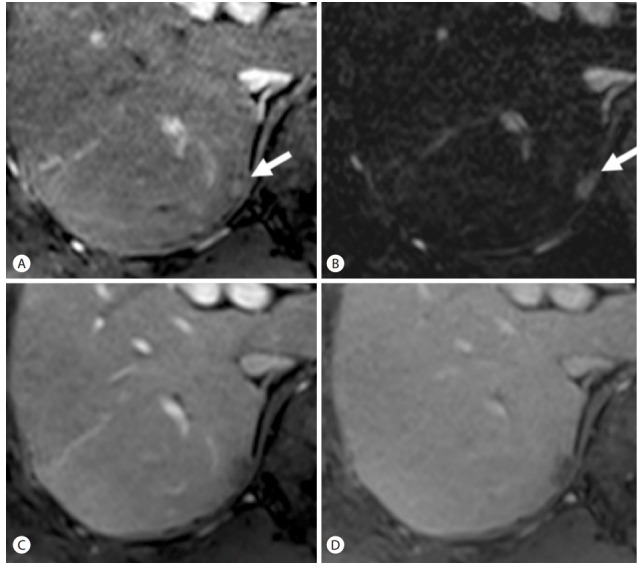
An observation that can be categorized as LR-3. At gadoxetic acid-enhanced MRI, a 1.2 cm nodule in the hepatic dome shows no arterial hyperenhancement (A). However, this observation would be better categorized as LR-3 than as LR-2, because of the presence of washout appearance in the portal venous phase (B) and some ancillary features such as hepatobiliary phase hypointensity (C) and moderate T2 hyperintensity (D).
LR-3 category is assigned to observations that do not meet the criteria for other LI-RADS categories and have a moderate probability of both HCC or a benign entity. Entities that can be categorized as LR-3 include hypovacular nodules larger than 2 cm or showing ancillary features such as moderate T2 hyperintensity, or subcentimeter arterially enhancing nodules without other imaging features favoring HCC (Fig. 3).
LR-4 category is assigned when the imaging features are suggestive, but not diagnostic, of HCC (Fig. 4). If there is a high probability of HCC but not 100% certainty, the observation must be categorized as LR-4, not as LR-5.
Figure 4.
An observation that can be categorized as LR-4, LR-5us, or LR-5g depending on the clinical situation. In the arterial phase of gadoxetic acid-enhanced MRI (arrow) (A), this 1.2 cm subcapsular lesion in the segment 7 of liver shows hyperenhancement, which is more definite in the subtraction image (arrow) (B), which is more definite in the subtraction image (B). In the portal venous (C) and delayed (D) phases, the lesion shows washout appearance but no capsule appearance. Because the nodule is smaller than 2 cm, this lesion cannot be categorized as LR-5 despite the presence of the radiologic hallmark of hepatocellular carcinoma (arterial hyperenhancement and washout). However, this 1- to 2-cm nodule with the radiologic hallmark can be categorized as LR-5, if it was previously detected at US (LR-5us) or showed ≥50% diameter increase in ≤6 months (LR-5g).
LR-5 category is assigned only when there is 100% certainty that the observation is HCC or it is proven to be HCC at histology (Fig. 5). For HCC 2 cm or larger, LR-5 observations are equivalent to class 5 using the OPTN-UNOS (Organ Procurement and Transplantation Network-United Network for Organ Sharing) system [4,18] and, depending on their size and number, could be used to assign priority for liver transplantation in eligible patients [10]. As a consequence, some small or early HCCs may be categorized as LR-4 or lower. Therefore, clinicians should be aware that an LI-RADS category lower than LR-5 does not exclude HCC.
Figure 5.
An observation that can be categorized as LR-5. In the pre-contrast T1-weighted image (A) and arterial (B), portal venous (C), and delayed (D) phases of gadoxetic acid-enhanced MRI, this 1.3 cm nodule unequivocally shows arterial hyperenhancement (B), washout appearance (C), and capsule appearance (C and D).
As explained above, one of the goals of LI-RADS is to render false-positive diagnoses of HCC as exceedingly rare in patients eligible for liver transplantation. To achieve such high specificity, the imaging criteria for LR-5, particularly for 1- to 2-cm observations, are more stringent than the AASLD criteria or others. Most 1- to 2-cm observations with arterial-phase hyperenhancement and a single additional major imaging feature are categorized as LR-4. However, they can be categorized as LR-5us (‘us’ stands for ‘ultrasound’) or LR-5g (‘g’ stands for ‘growth’) depending on the clinical situation (Fig. 4). This practice is to maintain congruency with the AASLD’s and the UNOS-OPTN’s diagnostic systems, respectively. LR-5us refers to observations that meet the AASLD diagnostic criteria, that is, those that measure 1 to 2 cm, with arterialphase hyperenhancement and washout appearance, and were visible as discrete nodules at antecedent surveillance US [2]. LR-5g refers to observations that meet the criteria for OPTN Class 5A-g, that is, those that present ≥50% diameter increase in ≤6 months [4].
LR-5V category is assigned when there is definite enhancing soft tissue in a vein irrespective of the presence or absence of visible intraparenchymal HCC (Fig. 6). This category was created because macrovascular invasion usually constitutes a contraindication to curative treatments such as liver transplantation and hepatic resection.
Figure 6.
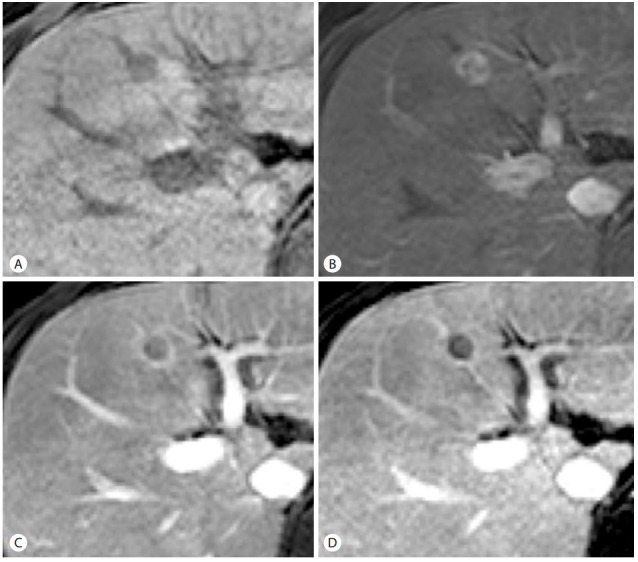
An observation that can be categorized as LR-5V. In the pre-contrast (A), arterial (B), portal venous (C), and delayed (D) phases of dynamic liver CT, ill-defined infiltrative lesions are diffusely involving the right posterior hepatic section (arrow), with expansile tumor thrombi in both main portal vein branches (arrowheads).
LR-M category is assigned to observations that are probably malignant but not specific for HCC, such as those with imaging features suggestive of ICC, biphenotypic tumor, lymphoma, metastasis, or post-transplant lymphoproliferative disorder (Fig. 7).
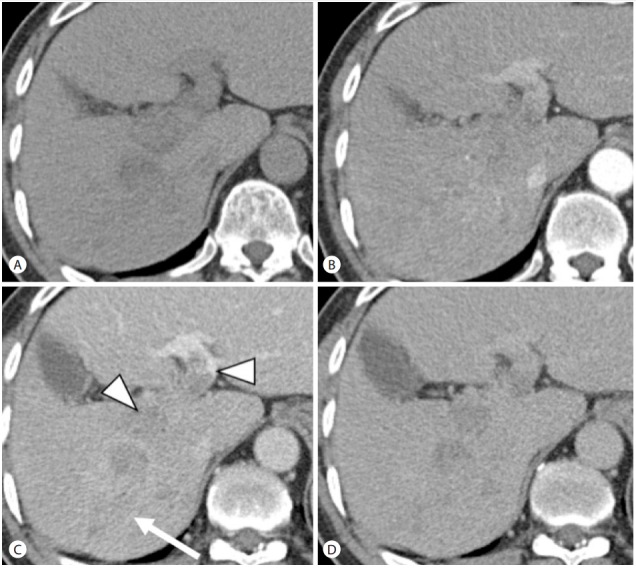
Figure 7.
An observation that can be categorized as LR-M. At gadopentetate-enhanced MRI, a 4-cm mass in the segment 5 of liver shows irregular peripheral enhancement and peritumoral parenchymal enhancement in the arterial phase (A) and peripheral washout and central enhancement in the delayed phase (B). These imaging features favor other malignancy over hepatocellular carcinoma (HCC).
LR-Treated category is assigned to treated observations, and is currently under development. Criteria for assessment of residual or recurrent disease based on the type of therapy will be released in future versions of LI-RADS [7].
Major imaging features
Major features are imaging features used to categorize LR-3, LR-4, and LR-5 observations, and include arterial-phase hyperenhancement, tumor diameter, washout appearance, capsule appearance, and threshold growth. Major features should be considered present only if their presence is unequivocal, in order to maintain high specificity for HCC.
Tumor diameter is defined as the largest dimension of an observation, measured from outer edge to outer edge in the imaging sequence, phase, and plane in which the margins are most sharply demarcated. In LI-RADS, observations are classified into two or three categories according to the size criteria (<2 cm vs. ≥2 cm for hypovascular observations, and <1 cm vs. 1-2 cm vs. ≥2 cm for hypervascular observations), because larger observations are associated with a higher likelihood of HCC and progression [19,20]. In LI-RADS, observations <1 cm cannot be categorized as definitely HCC (LR-5).
Arterial phase hyperenhancement is defined as contrast-enhancement in the arterial phase that is unequivocally greater than that of the surrounding liver parenchyma (Figs. 4 and 5). This is thought to reflect the gradual change in blood supply from portal to arterial due to capillarization and neoarterialization that accompanies the development of progressed HCC [21]. Arterial phase hyperenhancement is an essential prerequisite for definitely HCC (LR-5). However, it is non-specific and may be observed in benign entities such as hemangiomas, focal nodular hyperplasia, high-grade dysplastic nodules, and arterioportal shunts. Therefore, arterial phase hyperenhancement is required but not sufficient for LR-5 categorization; it must be observed in combination with other major features discussed below.
Washout appearance is defined as temporal reduction in contrast-enhancement relative to liver from an earlier to a later phase resulting in hypoenhancement in portal venous or delayed phase (Fig. 5). This may reflect multiple concomitant phenomena: rapid venous drainage, reduced portal venous supply to progressed HCC [22] and later enhancement of the background liver especially with hepatobiliary agents used as MRI contrast media [16]. Like arterial phase hyperenhancement, washout appearance by itself is not specific for HCC, as this feature may be observed in cirrhosis-associated nodules or pseudolesions such as focal areas of parenchymal distortion and enhancing fibrosis [9].
Capsule appearance is defined as a peripheral rim of smooth hyperenhancement in the portal venous or delayed phase that is unequivocally thicker or more conspicuous than the rims surrounding background nodules (Fig. 5). The rim of enhancement does not always represent a true tumor capsule, but may instead represent a pseudocapsule corresponding to loose fibrous tissue and dilated sinusoids around a nodule [23]. The capsule appearance may permit the diagnosis of HCC in the absence of definite wash-out appearance, although it is usually seen in combination with other major imaging features [24,25].
Threshold growth is defined as an increase in the diameter of an observation by both a minimum of 5 mm and a sufficient rate. The required growth rate is either at least a 50% increase in diameter compared with baseline within 6 months or at least a 100% increase in diameter over more than 6 months.
LI-RADS Table
The decision to assign LR-3, LR-4, or LR-5 categories to observations is based on the selection of appropriate columns and rows in the LI-RADS table embedded in Figure 1. The column is selected according to the enhancement pattern (arterial phase hypo- or iso-enhancement vs. hyperenhancement) and diameter. The row is selected according to the number of major features present among the following: washout appearance, capsule appearance, and threshold growth. The appropriate category is found at the intersection of column and row selected. As stated earlier, 1-2 cm observations with arterial-phase hyperenhancement and a single additional major feature are categorized as either LR-4, LR-5us (if it was visible at antecedent US), or LR-5g (if diameter increased by ≥50% in ≤6 months).
Ancillary imaging features
Ancillary features are imaging features that can be used to adjust the LI-RADS category at users’ discretion (Fig. 3). In isolation, these features do not permit reliable categorization of observations. There is not yet sufficient scientific evidence to mandate their use. Ancillary features favoring malignancy (including diffusion restriction, mosaic architecture, and moderate T2 hyperintensity) can be used to upgrade category by one or more categories, but not beyond LR-4 in order to maintain high specificity for HCC and congruency with the UNOS-OPTN and other guidelines. In contrast, ancillary features favoring benignity (including homogenous marked T2 hyperintensity or hypointensity, and diameter reduction or stability) can be used to decrease category down to LR-1 as appropriate.
A complete description of the major and ancillary imaging features is beyond the scope of this article, but detailed descriptions and supporting illustrations are available online (http://www.acr.org/Quality-Safety/Resources/LIRADS).
Tie-breaking rules
Tie-breaking rules can be used to adjust the category, if, after application of the algorithm and ancillary features, a user is still unsure about the final category for an observation (Fig. 8). These rules move observations to a category with a lower degree of certainty. For example, if unsure whether an observation should be categorized as LR-4 or LR-3, the rules would recommend the observation be categorized as LR-3. If there is concern that an LR-4 or LR-5 observation may represent a non-HCC malignancy, then it should be categorized as LR-M so as to avoid inappropriate management.
Figure 8.
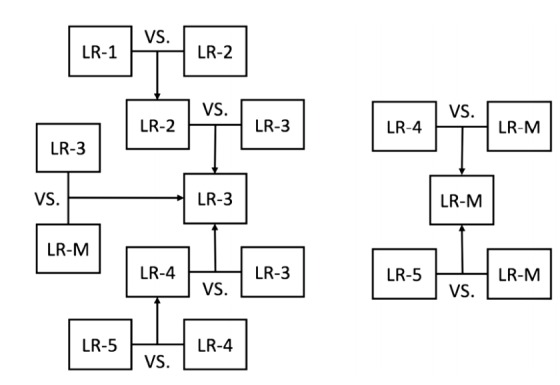
Tie breaking rules to adjust category. If still unsure about the final category for an observation after application of ancillary features, these tie-breaking rules should be applied. LR, LI-RADS.
MANAGEMENT IMPLICATIONS
For observations without a definite diagnosis by imaging (LR-2, LR-3, and LR-4), a clinician’s estimated probability of HCC should not depend solely on the LI-RADS category, but also on factors such as tumor markers and the patient’s previous probability of developing or having HCC [10]. Furthermore, the decision regarding the next step in a patient’s management should also depend on factors other than the likelihood of HCC, such as comorbidities, patient preference, or technical difficulty of biopsy. Thus, decisions between accelerated follow-up, alternative imaging, biopsy, or treatment without biopsy do not follow directly from the LI-RADS category or from a clinician’s estimated probability of HCC, but rather from a clinical assessment that integrates all available medical information. However, the LI-RADS category may facilitate management decisions by clearly communicating the contribution of imaging toward determining the likelihood of HCC. It should be noted that LI-RADS does not address management of nodules with a definite diagnosis of HCC (LR-5), because this is covered by the other guidelines.
CONCLUSIONS
LI-RADS is a comprehensive system for interpreting and reporting the full spectrum of hepatic observations in patients at high risk for HCC. One of the most important goals is to facilitate clear communication between all the personnel involved in the diagnosis and treatment of HCC, such as radiologists, hepatologists, surgeons, and pathologists. Therefore, in order to achieve this goal, clinicians should also be familiar with the LI-RADS diagnostic algorithm, and with the definitions and management implications of LI-RADS categories.
LI-RADS, like the other imaging-based diagnostic systems, does have limitations and problems to be addressed. However, LI-RADS is being constantly refined and updated in response to advances in our knowledge and technology. Therefore, LI-RADS will continue to evolve as a comprehensive and up-to-date system that will provide standardized imaging assessment of liver diseases for clinical care and research.
Acknowledgments
This study was supported by a grant from the National R&D Program for Cancer Control, Ministry of Health & Welfare, Republic of Korea (Grant #1520160).
Abbreviations:
- AASLD
the American association for the study of liver diseases
- ACR
American College of Radiology
- CT
computed tomography
- HCC
hepatocellular carcinoma
- ICC
intrahepatic cholangiocarcinoma
- LI-RADS
liver imaging reporting and data system
- MRI
magnetic resonance imaging
- OPTN-UNOS
organ procurement and transplantation network-united network for organ sharing
Footnotes
Conflicts of Interest: The authors have no conflicts to disclose.
REFERENCES
- 1.Omata M, Lesmana LA, Tateishi R, Chen PJ, Lin SM, Yoshida H, et al. Asian Pacific Association for the Study of the Liver consensus recommendations on hepatocellular carcinoma. Hepatol Int. 2010;4:439–474. doi: 10.1007/s12072-010-9165-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020–1022. doi: 10.1002/hep.24199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56:908–943. doi: 10.1016/j.jhep.2011.12.001. [DOI] [PubMed] [Google Scholar]
- 4.Wald C, Russo MW, Heimbach JK, Hussain HK, Pomfret EA, Bruix J. New OPTN/UNOS policy for liver transplant allocation: standardization of liver imaging, diagnosis, classification, and reporting of hepatocellular carcinoma. Radiology. 2013;266:376–382. doi: 10.1148/radiol.12121698. [DOI] [PubMed] [Google Scholar]
- 5.Kudo M, Matsui O, Izumi N, Iijima H, Kadoya M, Imai Y. Surveillance and diagnostic algorithm for hepatocellular carcinoma proposed by the Liver Cancer Study Group of Japan: 2014 update. Oncology. 2014;87:S7–S21. doi: 10.1159/000368141. [DOI] [PubMed] [Google Scholar]
- 6.Lee JM, Park JW, Choi BI. 2014 KLCSG-NCC Korea Practice Guidelines for the management of hepatocellular carcinoma: HCC diagnostic algorithm. Dig Dis. 2014;32:764–777. doi: 10.1159/000368020. [DOI] [PubMed] [Google Scholar]
- 7.Santillan CS, Tang A, Cruite I, Shah A, Sirlin CB. Understanding LI-RADS: a primer for practical use. Magn Reson Imaging Clin N Am. 2014;22:337–352. doi: 10.1016/j.mric.2014.04.007. [DOI] [PubMed] [Google Scholar]
- 8.American College of Radiology Liver Imaging Reporting and Data System Version 2014. ACR Web site < http://www.acr.org/Quality-Safety/Resources/LIRADS > Accessed 2016.04.15.
- 9.Tang A, Valasek MA, Sirlin CB. Update on the Liver Imaging Reporting and Data System: What the Pathologist Needs to Know. Adv Anat Pathol. 2015;22:314–322. doi: 10.1097/PAP.0000000000000089. [DOI] [PubMed] [Google Scholar]
- 10.Mitchell DG, Bruix J, Sherman M, Sirlin CB. LI-RADS (Liver Imaging Reporting and Data System): summary, discussion, and consensus of the LI-RADS Management Working Group and future directions. Hepatology. 2015;61:1056–1065. doi: 10.1002/hep.27304. [DOI] [PubMed] [Google Scholar]
- 11.Corwin MT, Fananapazir G, Jin M, Lamba R, Bashir MR. Differences in Liver Imaging and Reporting Data System Categorization Between MRI and CT. AJR Am J Roentgenol. 2016;206:307–312. doi: 10.2214/AJR.15.14788. [DOI] [PubMed] [Google Scholar]
- 12.Zhang YD, Zhu FP, Xu X, Wang Q, Wu CJ, Liu XS, et al. Liver Imaging Reporting and Data System:: Substantial Discordance Between CT and MR for Imaging Classification of Hepatic Nodules. Acad Radiol. 2016;23:344–352. doi: 10.1016/j.acra.2015.11.002. [DOI] [PubMed] [Google Scholar]
- 13.Darnell A, Forner A, Rimola J, Reig M, Garcia-Criado A, Ayuso C, et al. Liver Imaging Reporting and Data System with MR Imaging: Evaluation in Nodules 20 mm or Smaller Detected in Cirrhosis at Screening US. Radiology. 2015;275:698–707. doi: 10.1148/radiol.15141132. [DOI] [PubMed] [Google Scholar]
- 14.Choi SH, Byun JH, Kim SY, Lee SJ, Won HJ, Shin YM, et al. Liver Imaging Reporting and Data System v2014 With Gadoxetate Disodium-Enhanced Magnetic Resonance Imaging: Validation of LI-RADS Category 4 and 5 Criteria. Invest Radiol. 2016 Feb 16; doi: 10.1097/RLI.0000000000000258. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 15.Hope TA, Fowler KJ, Sirlin CB, Costa EA, Yee J, Yeh BM, et al. Hepatobiliary agents and their role in LI-RADS. Abdom Imaging. 2015;40:613–625. doi: 10.1007/s00261-014-0227-5. [DOI] [PubMed] [Google Scholar]
- 16.Doo KW, Lee CH, Choi JW, Lee J, Kim KA, Park CM. “Pseudo washout” sign in high-flow hepatic hemangioma on gadoxetic acid contrast-enhanced MRI mimicking hypervascular tumor. AJR Am J Roentgenol. 2009;193:W490–496. doi: 10.2214/AJR.08.1732. [DOI] [PubMed] [Google Scholar]
- 17.Suh YJ, Kim MJ, Choi JY, Park YN, Park MS, Kim KW. Differentiation of hepatic hyperintense lesions seen on gadoxetic acid-enhanced hepatobiliary phase MRI. AJR Am J Roentgenol. 2011;197:W44–52. doi: 10.2214/AJR.10.5845. [DOI] [PubMed] [Google Scholar]
- 18.Pomfret EA, Washburn K, Wald C, Nalesnik MA, Douglas D, Russo M, et al. Report of a national conference on liver allocation in patients with hepatocellular carcinoma in the United States. Liver Transpl. 2010;16:262–278. doi: 10.1002/lt.21999. [DOI] [PubMed] [Google Scholar]
- 19.Kumada T, Toyoda H, Tada T, Sone Y, Fujimori M, Ogawa S, et al. Evolution of hypointense hepatocellular nodules observed only in the hepatobiliary phase of gadoxetate disodium-enhanced MRI. AJR Am J Roentgenol. 2011;197:58–63. doi: 10.2214/AJR.10.5390. [DOI] [PubMed] [Google Scholar]
- 20.Takayama Y, Nishie A, Nakayama T, Asayama Y, Ishigami K, Kakihara D, et al. Hypovascular hepatic nodule showing hypointensity in the hepatobiliary phase of gadoxetic acid-enhanced MRI in patients with chronic liver disease: prediction of malignant transformation. Eur J Radiol. 2012;81:3072–3078. doi: 10.1016/j.ejrad.2012.05.008. [DOI] [PubMed] [Google Scholar]
- 21.Park YN, Kim MJ. Hepatocarcinogenesis: imaging-pathologic correlation. Abdom Imaging. 2011;36:232–243. doi: 10.1007/s00261-011-9688-y. [DOI] [PubMed] [Google Scholar]
- 22.Efremidis SC, Hytiroglou P. The multistep process of hepatocarcinogenesis in cirrhosis with imaging correlation. Eur Radiol. 2002;12:753–764. doi: 10.1007/s00330-001-1142-z. [DOI] [PubMed] [Google Scholar]
- 23.Ishigami K, Yoshimitsu K, Nishihara Y, Irie H, Asayama Y, Tajima T, et al. Hepatocellular carcinoma with a pseudocapsule on gadolinium-enhanced MR images: correlation with histopathologic findings. Radiology. 2009;250:435–443. doi: 10.1148/radiol.2501071702. [DOI] [PubMed] [Google Scholar]
- 24.Kim TK, Lee KH, Jang HJ, Haider MA, Jacks LM, Menezes RJ, et al. Analysis of gadobenate dimeglumine-enhanced MR findings for characterizing small (1-2-cm) hepatic nodules in patients at high risk for hepatocellular carcinoma. Radiology. 2011;259:730–738. doi: 10.1148/radiol.11101549. [DOI] [PubMed] [Google Scholar]
- 25.Rimola J, Forner A, Tremosini S, Reig M, Vilana R, Bianchi L, et al. Non-invasive diagnosis of hepatocellular carcinoma </= 2 cm in cirrhosis. Diagnostic accuracy assessing fat, capsule and signal intensity at dynamic MRI. J Hepatol. 2012;56:1317–1323. doi: 10.1016/j.jhep.2012.01.004. [DOI] [PubMed] [Google Scholar]