

Abstract
Background:
Survival of the semi-allograft fetus during pregnancy opens a new area for the immunological based causes of recurrent spontaneous abortion (RSA). Cytotoxic T lymphocyte-associated antigen 4 (CTLA4) is a negative regulator of the T-cell activation, which may modulate peripheral self-tolerance of the allogeneic fetus. The present study aimed to investigate the +49 A/G CTLA4 genetic polymorphism and predisposition to RSA.
Methods:
The total participants were 120 women with at least two miscarriages and 120 healthy post-menopausal women as the control group. The +49 A/G polymorphism was genotyped using PCR-RFLP method. Required demographic information was collected through filling out a questionnaire. The obtained data were fed into SPSS software version 16.
Results:
The results showed a significant association between the minor alleles (G) with the decreased risk of the RSA. The frequency of the G allele in controls and patients was 25% and 12%, respectively. A GG genotype in the co-dominance model (OR: 0.25, 95%CI: 0.09–0.66) and in the dominant model for allele G (GG+AG vs. AA) (OR: 0.84, 95%CI: 0.8–0.87) showed significant association with RSA by imposing the protective role. The frequency of miscarriage is significantly (p=0.04) higher among the relatives of RSA women (33.3%) in comparison with the women in the control group (21.7%).
Conclusion:
It can be concluded that +49G allele may act as a dominant allele and reduce the risk of RSA. Family history of miscarriage increased the risk of RSA among women.
Keywords: CTLA4, PCR-RFLP, Polymorphism, Recurrent spontaneous abortion
Introduction
Recurrent spontaneous abortion (RSA) is one of the most common pregnancy complications with the prevalence of 1–2% among pregnant women in reproductive life, which is defined as the occurrence of 2 or more consecutive spontaneous abortions (1). RSA is a heterogeneous condition and its complexity is the result of the defects in several genes, and their interactions with each other and with environmental factors (2).
From the perspective of the immunology of pregnancy, the major concern is related to immunological factors and sequence variants of immunologic components in the etiology of miscarriage (3). Medawar (1953) proposes the paradox of fetal allograph which helps the investigators to review the immunological mechanisms that operate during pregnancy as such the result ensures the survival of the semi-allograft fetus (4). T-cells are the most important mediators of immune response. Naïve T lymphocytes leave the thymus and after receiving necessary signals, their activation, expansion, differentiation and cytokine production start. These two signals are the result of interaction between antigen-specific T-cell receptor (TCR; CD3 complex) with MHC class II-bound antigen on the surface of antigen-presenting cells (APCs) and the co-stimulatory signal provided by the B7 (CD80 and CD86)/CD28 interaction (5). CTLA4 is the homolog of CD28 molecule which interacts with the same ligands but with different affinity. In comparison to CD28, CTLA4 inactivates T-cells by mediating antigen-specific apoptosis. Thus, CTLA4 provides immunosuppressive function in modulating T-cell proliferation and plays a role in immune self-tolerance, which can be mimicked in the maintenance of tolerance to allogeneic antigens (5–7). As mentioned above, the fetus is semi-allograft, consisting of one maternal and one paternal human leukocyte antigen (HLA) or major histocompatibility complex (MHC). Therefore, the maintenance of this allograft is in part related to the mechanisms and molecules involved in naturally programmed self-tolerance (8). The expression of the CTLA4 gene in the placental fibroblasts and decidual cells throughout gestation has raised the possibility of involvement of the CTLA4 molecule in the maintenance of tolerance at the maternal-fetal interface (9). Case-control studies also present the lower proportions of CD4 (+) CD25 regulatory T-cells in both peripheral blood and deciduas in miscarriage in comparison to that of a normal pregnancy (3). So, deeper analysis of CTLA4 variants or expression could lead to significant results. The gene encoding for CTLA4 maps on chromosome 2q33-34. It contains 4 coding exons and expresses to 1977 bp transcript with the translation product of 223 residues (10).
Several polymorphisms in the CTLA4 gene are found by sequencing the complete length of the gene with its regulatory elements. Three of them are more common and their involvement in diseases can be investigated better. One of the most widely studied of these genetic variants is the SNP at position +49 (A/G) in exon-1 of CTLA4, which leads to a threonine-to-alanine change in the leader peptide which is considered as a sequence variant that affects the gene expression and disturbs the immune regulation (11, 12). This study aimed to investigate the distribution of the CTLA4 A49G (dbSNP: rs231775) polymorphism and its association with RSA.
Methods
Subjects:
In this case-control study, comparison between 120 women with the history of at least two spontaneous abortions and 120 healthy postmenopausal women with at least two live births as control group with no history of miscarriage as described previously by Unfried et al. (2003), was done based on the genotype distribution of the polymorphic site at +49A/G in CTLA4 gene and the positive family history of miscarriage (family history among first and second degree relatives just considered) (13). Anatomic abnormalities of the genital tract and cervical incompetence detected by hysteroscopy, endocrinologic dysfunctions, abnormal karyotypes and cervical infection for chlamydia and mycoplasma were considered as exclusion criteria, therefore these etiologies of recurrent pregnancy loss are known to have a close cause-and-effect relationship. A questionnaire was used to elicit detailed information on demographic variables, the number of miscarriages, and history of miscarriage.
Genotyping:
DNA was isolated from peripheral blood lymphocytes using classical phenol/chloroform extraction method. Polymorphic variant of CTLA4 gene (rs231775) was analyzed through using PCR-restriction fragment length polymorphism (PCR-RFLP). Primers, annealing temperature and restriction endonuclease used in the study are listed in table 1. PCR amplification was done using the thermal cycler Applied Biosystems (Perkin Elmer 9600) with a total volume of 25 μl, containing 12.5 μl universal master mix (Ampliqon, Denmark), 1 μl forward primer, 1 μl reverse primer, together with 9.5 μl distilled water (DW). The PCR condition was as follows: initial denaturation at 95°C for 5 min, followed by 35 cycles of denaturation at 94°C for 30 s, annealing at 58.5°C for 30 s and extension at 72°C for 30 s and then one cycle of final extension at 72°C for 5 min. The PCR product was digested with BSeX I (Bbv I) restriction enzyme (Fermentas, France) and put at 37°C for 20 hr. The amplified fragment after digestion with BSeX I restriction enzymes, gave rise to two fragments of 130 bp and 159 bp indicating the presence of polymorphic genotype (GG), and the appearance of one undigested 289 bp fragment indicates the presence of homozygous wild type (AA), while the presence of 3 fragments at 130 bp, 159 bp and 289 bp indicates the heterozygous manner (AG) (Figure 1). The products were then resolved on 2% agarose gel electrophoresis and stained with SYBR gold DNA safe stain dye, then visualized using a UV transilluminator. DNA molecular weight marker (Fermentas, 100 bp Ladder) was used to assess the size of PCR-RFLP products.
Table 1.
The sequence and other characteristics of the primer pairs used in the amplification process
| Primer name | Sequence 5’ to 3’ | Tm (°C) | Restriction enzyme |
|---|---|---|---|
| rs231775-F | CTTGATTCTGTGTGGGTTC | 58.5 | BSeX I 5’... GCAGC (N) 8↓...3’ 3’... CGTCG (N)12↓... 5’ |
| rs231775-R | CACTGCCTTTGACTGCTG |
Figure 1.
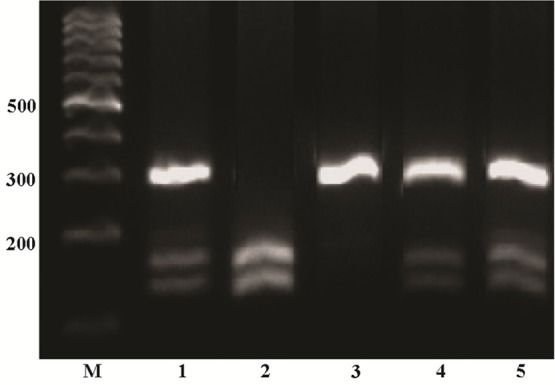
PCR-based restriction analysis of the +49 A/G polymorphism was shown on 2% agarose electrophoresis. The polymorphic region was amplified by PCR resulting in a 289 bp fragment (AA wild type homozygote) in line 3 after size marker. Digestible fragments, 159 and 130 bp, represent the GG mutant homozygote (line 2). The presence of three bands 289, 159 and 130 which belong to heterozygote individuals (line 1, 4 and 5). M: mar
Statistical analysis:
Statistical analyses were carried out using the SPSS 16.0 (SPSS, Inc., Chicago, IL, USA). Quantitative data were expressed as mean±standard deviation (SD). Differences between groups were assessed by Student’s t-test (two -tailed). Categorical variables were presented using frequency counts and compared with a logistic regression. Deviation from Hardy-Weinberg equilibrium was analyzed by χ2 test. Odds ratio (OR) and 95% confidence interval (CI) were calculated as an estimate of risk. The p<0.05 was considered statistically significant.
Results
The product of restriction enzyme digestion on 289 bp amplified fragment is shown in figure 1. A total of 120 women with the history of miscarriage and 120 healthy postmenopausal women of control group were included in this study. The baseline characteristics are shown in table 2. The mean number of miscarriages in the patients was 3.3±1.2 (range: 2–10), in which 18% had 2 miscarriages and 82% had 3 or more. The history of miscarriage among the relatives of women was significantly higher in comparison to the control group (OR=1.8, 95% CI: 1.01–3.2).
Table 2.
Baseline characteristics
| variables | Cases n=120 | Controls n=120 |
|---|---|---|
| Age (M±SD) * | 35.4±1.25 | 57.9±5.8 |
| Age range | 17–85 | 43–76 |
| Abortion (M±SD) | 3.3±1.2 | -- |
| No. of abortion | ||
| 2 | 22 (18%) | -- |
| ≥3 | 98 (82%) | -- |
| Family history ** | ||
| Yes | 40 (33.3%) | 26 (21.7%) |
| No | 80 (66.7%) | 94 (78.3%) |
P<0.05 were considered to indicate statistical significance,
p<0.001,
p<0.05
Details on the frequency of alleles and genotypes of the polymorphic marker +49A/G are presented in table 3. The frequency of the G allele positive individuals significantly decreased in RSA patients relative to controls (21.7% and 43.3%, respectively; OR: 0.84, 95% CI: 0.8–0.87). The G allele frequency was 12% in RSA patients compared with 25% in controls (p<0.001). The frequency of the GG genotype among controls and patients was significantly less than other two genotypes. The GG genotype was observed in only 2.5% of RSA patients compared with 5.8% of controls (OR: 0.25, 95% CI: 0.09–0.66). The genotype frequencies for both patients and controls in the studied SNP were not significantly different from those expected for populations in Hardy-Weinberg equilibrium.
Table 3.
Distribution of +49A/G genotypes and allelic frequencies among cases and controls
| rs231775 polymorphism | controls (120) n, % | RSA (120) in, % | P-value | OR * | 95%CI |
|---|---|---|---|---|---|
| Genotypes | |||||
| GG | 7 (5.8) | 3 (2.5) | 0.005 | 0.25 | 0.09–0.66 |
| GA | 45 (37.5) | 23 (19.2) | 0.17 | 0.19 | 0.01 – 2.07 |
| AA | 68 (56.7) | 94 (78.3) | -- | -- | -- |
| GG+AG | 52 (43.3) | 26 (21.7) | 0.003 | 0.84 | 0.8–0.87 |
| AA+AG | 113 (94.2) | 117 (97.5) | 0.3 | 0.3 | 0.02–3.05 |
| Alleles | |||||
| G | 59 (25) | 29 (12) | 0.001 | 0.42 | 0.25–0.69 |
| A | 181 (75) | 211 (88) | -- | -- | -- |
OR: Odds ratio; CI: Confidence interval;
Logistic regression
Discussion
Pregnancy loss is one of the serious complications of the pregnancy, which affects 1–2% of women in reproductive age (14). Despite years of effort to determine the factors involved in the miscarriage, the cause remains unknown in 50% of the cases, hence it reflects the heterogeneous nature of the condition (15). Among all known etiologic factors, anatomical defects, chromosomal rearrangement, infections, etc. are the typical ones and based on them, scientists are more interested in the field of reproductive immunology (16). Establishment and maintenance of pregnancy represent a challenge for the maternal immune system since it has to defend against pathogens and tolerate paternal alloantigens expressed in fetal tissues (17). Medawar (1953) for the first time proposed that there is an anatomical separation between mother and fetus which protects the semi-allograft fetus from the mother’s immune response. Since fetal cells are in close contact to mother cells, he pointed to the maternal lymphocyte suppression. Finally, it became clear that the function of lymphocytes changes during pregnancy instead of suppression (4).
It is not completely clear whether the history of spontaneous abortion (SA) among relatives can predispose women to RSA. To the best of our knowledge, this is the first study in Iran that evaluates the relationship between RSA in 120 women and the history of SA among their relatives. The frequency of SA among the relatives of the participants was 33.3% and 21.7%, respectively. The study of Miskovic (2012) on the relationship between RSA in 567 couples and the frequency of SA among their relatives, resulted in two or three times higher frequency of SA occurrences among relatives of RSA couples than that of the general population (18).
CTLA4 is an effector molecule which negatively regulates the T lymphocyte proliferation (19). CTLA4 gene expression was mainly restricted to both CD4+ and CD8+ T cells with significantly higher expression in CD4+ (18). CTLA4 gene knockout mice experiments support the role of the CTLA4 in the regulation of T-cell tolerance or autoimmunity (20). Removing CTLA4 inhibition using anti-CTLA4 mAb results in the earlier activation of the self- reactive T-cells, thus allowing the earlier migration of the increased numbers of the activated cells to the peripheral organs where they can mediate tissue damage (21). All these suggested roles are supported by the association between autoimmune diseases and the CTLA4 gene polymorphisms. About 100 polymorphisms were reported for the CTLA4 gene, but the A to G substitution resulted in threonine-to-alanine replacement at codon 17 of the leader peptide. Extracted data from the NCBI database showed the minor allele (G) frequency (MAF) of 0.42 for this polymorphic site (22). This variant of the gene is strongly associated with many autoimmune diseases and tumors such as Graves’ disease, systemic lupus erythematosus, type 1 diabetes, gastric and pancreatic cancers (23–28). Expression of CTLA4 in placental fibroblast cells and deciduas was confirmed by different analysis, and then its role in pregnancy loss can be considered (9). Few investigations have been performed that focus on the possible roles of the +49A/G SNP in recurrent spontaneous abortion. Wang et al. (2005) found the significant relationship between the G allele and the GG genotype of the +49A/G polymorphism with the risk of unexplained recurrent spontaneous abortion in the Chinese population. Frequency of the G allele dramatically increased in patients compared to the controls, which suggested the role of this allele in the reduction of the CTLA4 gene expression and decreased inhibitory function of the CTLA4 on T-lymphocytes (29). This research duplicated other studies done in Tunisian RSA women, and they also achieved the same results on the role of G allele in the susceptibility of RSA (30). In another study, Gupta et al. (2012) found that mutant homozygous genotype GG in the recessive model (GG vs. AG+AA) increases the risk of RM among women of North India (OR: 1.71, 95%, CI: 1.07–2.74, p=0.02). No relationship between any of the G or A allele was observed in their study (31). In contrast to the results of the previous studies, the frequency of the G allele in our patients and controls was very low and was 12% and 25%, respectively in comparison to the A allele frequency and our statistical data emphasized the protective role of G allele against the RSA. This contradiction may be due to the differences in the ethnicity, the sample size as well as the inclusion and exclusion criteria of the study. On the other hand, disease heterogeneity may affect involvement and nature of genetic susceptibility factors. Enhanced T-cell activation and proliferation may prevent semi-allograft fetal cells to escape from cytotoxic T lymphocyte killing and therefore may induce miscarriage. The CTLA4 G allele enhances the interaction between CTLA4 and B7.1 on antigen- presenting cells, resulting in stronger CTLA4-triggered inhibition of T-cell activation and proliferation (28). This may be the underlying mechanism that facilitates the fetal cell escape and increasing the survival of the semi-allograft fetus.
There are some investigations in favor of the role of +49A/G polymorphism in the etiology of some diseases. The following are examples of such diseases which resulted in the same role for CTLA4 gene polymorphism. In the study of the relationship between +49A/G CTLA4 polymorphism and celiac disease, Djilali-Saiah et al. (1998) found also the protective role for the G allele in the pathogenesis of the disease (32). A meta-analysis by Xu et al. (2013) was done to unravel the relationship between +49A/G CTLA4 with the chronic infection with hepatitis B virus. Comprehensive analysis of existing data supports the protective role of G allele in the risk of chronic HBV infection compared with A allele (OR 0.77; 95% CI 0.68, 0.88). They hypothesized that CTLA4 G allele may enhance the scavenging of virus (33).
Although the precise mechanisms through which G allele exerts its effect on CTLA4 gene expression remain unclear, the rs231775 (+49A/G) polymorphism in exon 1 of the CTLA4 gene appears to show an example of an exon-located functional polymorphism with potential clinical significance.
Conclusion
Taken together, it may be hypothesized that the +49 G allele acts as a dominant allele in relation to decreasing the risk of recurrent spontaneous abortion among Iranian women of southwest. Positive family history can also be considered as a criterion for identification of high risk women.
Acknowledgement
The authors would like to express their sincere gratitude to Dr. Minoo Zolghadri, the gynecologist, and her staff whose collaboration paved the way for collecting the data. Special appreciation is also expressed to Mohammad Moghadam, geneticist, for his technical assistance.
Footnotes
Conflict of interest
The data are provided from the thesis of the Z. Rasti, MSc student of developmental biology in Islamic Azad University, Arsanjan Branch. The authors have no conflict of interest.
This study was supported by Islamic Azad University, Arsanjan Branch.
References
- Chaithra PT, Malini Suttur S, Sharath Kumar C. An overview of genetic and molecular factors responsible for recurrent pregnancy loss. Int J Hum Genet. 2011; 11( 4): 217– 25. [Google Scholar]
- Rai R, Regan L. Recurrent miscarriage. Lancet. 2006; 368( 9535): 601– 11. [DOI] [PubMed] [Google Scholar]
- Veenstra van Nieuwenhoven AL, Heineman MJ, Faas MM. The immunology of successful pregnancy. Hum Reprod Update. 2003; 9( 4): 347– 57. [DOI] [PubMed] [Google Scholar]
- Medawar PB. Some immunological and endocrineological problems raised by the evolution of viviparity in vertebrates. Symp Soc Exp Biol. 1953: 320– 8. [Google Scholar]
- Frauwirth KA, Thompson CB. Activation and inhibition of lymphocytes by costimulation. J Clin Invest. 2002; 109( 3): 295– 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pedicord VA, Montalvo W, Leiner IM, Allison JP. Single dose of anti-CTLA-4 enhances CD8+ T-cell memory formation, function, and maintenance. Proc Natl Acad Sci USA. 2011; 108( 1): 266– 71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson HM, Hedgcock CJ, Aufiero BM, Wilson AJ, Hafner MS, Tsokos GC , et al. , Induction of the CTLA-4 gene in human lymphocytes is dependent on NFAT binding the proximal promoter. J Immunol. 2007; 179( 6): 3831– 40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anjos SM, Polychronakos C. Functional evaluation of the autoimmunity-associated CTLA4 gene: the effect of the (AT) repeat in the 3’untranslated region (UTR). J Autoimmun. 2006; 27( 2): 105– 9. [DOI] [PubMed] [Google Scholar]
- Kaufman KA, Bowen JA, Tsai AF, Bluestone JA, Hunt JS, Ober C. The CTLA-4 gene is expressed in placental fibroblasts. Mol Hum Reprod. 1999; 5( 1): 84– 7. [DOI] [PubMed] [Google Scholar]
- Vaidya B, Pearce S. The emerging role of the CTLA-4 gene in autoimmune endocrinopathies. Eur J Endocrinol. 2004; 150( 5): 619– 26. [DOI] [PubMed] [Google Scholar]
- Chistiakov DA, Turakulov RI. CTLA-4 and its role in autoimmune thyroid disease. J Mol Endocrinol. 2003; 31( 1): 21– 36. [DOI] [PubMed] [Google Scholar]
- Ueda H, Howson JM, Esposito L, Heward J, Snook H, Chamberlain G, et al. , Association of the T-cell regulatory gene CTLA4 with susceptibility to autoimmune disease. Nature. 2003; 423( 6939): 506– 11. [DOI] [PubMed] [Google Scholar]
- Unfried G, Bocskor S, Endler G, Nagele F, Huber JC, Tempfer CB. A polymorphism of the interleukin-6 gene promoter and idiopathic recurrent miscarriage. Hum Reprod. 2003; 18( 2): 267– 70. [DOI] [PubMed] [Google Scholar]
- Hogge WA, Byrnes AL, Lanasa MC, Surti U. The clinical use of karyotyping spontaneous abortions. Am J Obstet Gynecol. 2003; 189( 2): 397– 400. [DOI] [PubMed] [Google Scholar]
- Li TC, Makris M, Tomsu M, Tuckerman E, Laird S. Recurrent miscarriage: aetiology, management and prognosis. Hum Reprod Update. 2002; 8( 5): 463– 81. [DOI] [PubMed] [Google Scholar]
- Laird SM, Tuckerman EM, Cork BA, Linjawi S, Blakemore AI, Li TC. A review of immune cells and molecules in women with recurrent miscarriage. Hum Reprod Update. 2003; 9( 2): 163– 74. [DOI] [PubMed] [Google Scholar]
- Mor G, Cardenas I. The immune system in pregnancy: a unique complexity. Am J Reprod Immunol. 2010; 63( 6): 425– 33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miskovic S, Culic V, Konjevoda P, Pavelic J. Positive reproductive family history for spontaneous abortion: predictor for recurrent miscarriage in young couples. Eur J Obstet Gynecol Reprod Biol. 2012; 161( 2): 182– 6. [DOI] [PubMed] [Google Scholar]
- Bashyam H. CTLA-4: From conflict to clinic. J Exp Med. 2007; 204( 6): 1243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chan DV, Gibson HM, Aufiero BM, Wilson AJ, Hafner MS, Mi QS, et al. , Differential CTLA-4 expression in human CD4+ versus CD8+ T cells is associated with increased NFAT1 and inhibition of CD4+ proliferation. Genes Immun. 2014; 15( 1): 25– 32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kolar P, Knieke K, Hegel JK, Quandt D, Burmester GR, Hoff H, et al. , CTLA-4 (CD152) controls homeostasis and suppressive capacity of regulatory T cells in mice. Arthritis Rheum. 2009; 60( 1): 123– 32. [DOI] [PubMed] [Google Scholar]
- Wang C, Jiang T, Wei L, Li F, Sun X, Fan D, et al. , Association of CTLA4 gene polymorphisms with susceptibility and pathology correlation to pulmonary tuberculosis in Southern Han Chinese. Int J Biol Sci. 2012; 8( 7): 945– 52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kavvoura FK, Ioannidis JP. CTLA-4 gene polymorphisms and susceptibility to type 1 diabetes mellitus: a HuGE Review and meta-analysis. Am J Epidemiol. 2005; 162( 1): 3– 16. [DOI] [PubMed] [Google Scholar]
- Zhao SX, Pan CM, Cao HM, Han B, Shi JY, Liang J, et al. , Association of the CTLA4 gene with Graves’ disease in the Chinese Han population. PLoS One. 2010; 5( 3): e9821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee YH, Harley JB, Nath SK. CTLA-4 polymorphisms and systemic lupus erythematosus (SLE): a meta-analysis. Hum Genet. 2005; 116( 5): 361– 7. [DOI] [PubMed] [Google Scholar]
- Balic I, Angel B, Codner E, Carrasco E, Perez-Bravo F. Association of CTLA-4 polymorphisms and clinical-immunologic characteristics at onset of type 1 diabetes mellitus in children. Hum Immunol. 2009; 70( 2): 116– 20. [DOI] [PubMed] [Google Scholar]
- Hou R, Cao B, Chen Z, Li Y, Ning T, Li C, et al. , Association of cytotoxic T lymphocyte-associated antigen-4 gene haplotype with the susceptibility to gastric cancer. Mol Biol Rep. 2010; 37( 1): 515– 20. [DOI] [PubMed] [Google Scholar]
- Yang M, Sun T, Zhou Y, Wang L, Liu L, Zhang X, et al. , The functional cytotoxic T lymphocyte-associated Protein 4 49G-to-A genetic variant and risk of pancreatic cancer. Cancer. 2012; 118( 19): 4681– 6. [DOI] [PubMed] [Google Scholar]
- Wang X, Lin Q, Ma Z, Hong Y, Zhao A, Di W, et al. , Association of the A/G polymorphism at position 49 in exon 1 of CTLA-4 with the susceptibility to unexplained recurrent spontaneous abortion in the Chinese population. Am J Reprod Immunol. 2005; 53( 2): 100– 5. [DOI] [PubMed] [Google Scholar]
- Messaoudi S, Houas I, Yaseen Kh, Dandana M, Mahjoub T. CTLA-4 gene polymorphisms and risk of idiopathic recurrent pregnancy loss in a Tunisian population. BMC Genomics. 2014; 15( Suppl 2): P11. [DOI] [PubMed] [Google Scholar]
- Gupta R, Prakash S, Parveen F, Agrawal S. Association of CTLA-4 and TNF-α polymorphism with recurrent miscarriage among North Indian women. Cytokine. 2012; 60( 2): 456– 62. [DOI] [PubMed] [Google Scholar]
- Djilali-Saiah I, Schmitz J, Harfouch-Hammoud E, Mougenot JF, Bach JF, Caillat-Zucman S. CTLA-4 gene polymorphism is associated with predisposition to coeliac disease. Gut. 1998; 43( 2): 187– 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xu H, Zhao M, He J, Chen Z. Association between cytotoxic T-lymphocyte associated protein 4 gene +49 A/G polymorphism and chronic infection with hepatitis B virus: a meta-analysis. J Int Med Res. 2013; 41( 3): 559– 67. [DOI] [PubMed] [Google Scholar]