

Abstract
Background
Early withdrawal or exclusion from the labor market leads to significant personal and societal costs. In Norway, the increasing numbers of young adults receiving disability pension is a growing problem. While a large body of research demonstrates positive effects of Supported Employment (SE) in patients with severe mental illness, no studies have yet investigated the effectiveness of SE in young adults with a range of social and health conditions who are receiving benefits.
Methods/design
The SEED-trial is a randomized controlled trial (RCT) comparing traditional vocational rehabilitation (TVR) to SE in 124 unemployed individuals between the ages of 18-29 who are receiving benefits due to various social- or health-related problems. The primary outcome is labor market participation during the first year after enrollment. Secondary outcomes include physical and mental health, health behaviors, and well-being, collected at baseline, 6, and 12 months. A cost-benefit analysis will also be conducted.
Discussion
The SEED-trial is the first RCT to compare SE to TVR in this important and vulnerable group, at risk of being excluded from working life at an early age.
Trial registration
Clinicaltrials.gov, registration number NCT02375074. Registered on December 3rd 2014
Keywords: Disability, Employment, Individual Placement and Support, Randomized Controlled Trial, Supported Employment, Vocational Rehabilitation, Unemployment, Work Disability, Youth
Background
Early disability
The number of young adults receiving permanent disability pension in Norway has recently accelerated. While the overall percentage of disability pensioners in the population has remained steady for the last decade, there has been an increase in the proportion of young disability pensioners (between 18 and 29 years old) and a continuous decline in older disability pensioners throughout the same period [1, 2]. From 2006 to 2015 there was an increase of 77 % in young disability pensioners [3] while the population in the same age group increased by 23 % [4], making the development evident even when population growth is accounted for. Additionally, during the same period, an increased rate of labor immigration (mainly young males) has inflated the number of working young adults, which may have suppressed the percentage growth and led to an underestimation of the development [1].
Musculoskeletal and common mental disorders account for about 2/3 of sickness benefits and disability pensions issued in Norway [5, 6], but within the subgroup of disability pensioners aged 18–29, 59 % are receiving disability pensions due to mental illness and behavior disorders alone [7]. This type of early withdrawal or exclusion from the labor market leads to vast personal and societal costs, especially when seen in context with the aging of the Norwegian population causing a disparity between the supply of available workforce and the need of work capacity [8]. Furthermore, the importance of work for health and well-being is well-documented [4–6], and evidence shows that unemployment is not only caused by mental health problems, but also causes them [7, 8].
Long-term sickness absence is a risk factor for unemployment and permanent disability that goes beyond the effect of health status, suggesting that long-lasting absence may itself initiate a process of marginalization from the labor market [9]. Few recipients of long-term sickness benefits return to working life, seemingly due to mechanisms other than age, diagnosis, gender and public health [10]. This may be particularly relevant for young people in need of special assistance to obtain work, who are at risk of being excluded from working life before having had the chance to establish themselves on the labor market. Previous studies document that a small percentage of the population accounts for the majority of sickness absence, and that broad interventions targeting the workforce as a whole may not reach these small but high-risk groups [11]. Focusing on the group of young people who are receiving temporary benefits, but have not reached the point of more permanent disability pensions, thus appears to be a viable way to move forward.
Perspectives in vocational rehabilitation
Vocational rehabilitation has traditionally been characterized by a train-then-place principle, involving prevocational training in sheltered environments before attempting to enter the open labor market [12]. In the train-then-place approach, clients try different forms of work adapted to their skills and challenges, while undergoing a stepwise process of targeted training to prepare them for competitive employment. Training is usually provided in group settings along with other workers with challenges or disabilities, and with close follow-up from an advisor. While the goal is to improve clients’ opportunities for obtaining work, the approach has been criticized for promoting dependency and demoralization [13], and for having a negative effect on different stakeholders expectations of the clients’ work ability and productivity [14].
In the 1980s, rehabilitation leaders in the U.S. introduced an approach based on the place-then-train principle, with a main goal of competitive employment and immediate work integration, without prevocational training [12]. This approach challenged common assumptions about people with serious disabilities being able to work only in workshops or other sheltered environments. Approaches within this perspective are known as Supported Employment (SE), and the evidence-based and manualized methodology of SE is called Individual Placement and Support (IPS). The model was originally developed for people with severe mental illness (SMI), and is supported by evidence from randomized controlled trials (RCT’s) in the US [15–24] as well as internationally [25–37], showing SE to be effective in this disability group on a range of vocational outcome measures. IPS involves individual support from a trained job specialist, incorporating eight evidence-based principles: focus on competitive employment in ordinary paid positions; rapid job search, starting the job search on average within one month after program entry; attention to the client’s choices and preferences; integrating work with mental health treatment; personalized benefits counseling; systematic job development; individualized long-term job support; and eligibility based on the client’s choice [38]. The latter involves a zero exclusion criteria, which states that everyone who has an expressed desire to work should have access to IPS services regardless of factors such as previous employment history, history of violent behavior, personal presentation, or substance abuse, and that the service does not screen for work readiness [39].
Evidence-based knowledge of the effectiveness of the services being offered through public agencies is of vital importance in future planning of vocational rehabilitation of young adults. Although there is a large and growing body of research demonstrating the effectiveness of the IPS approach in other populations, no studies have yet examined the effectiveness of IPS specifically for young adults at risk of becoming permanent disability pensioners.
Methods/Design
The study is conducted by Uni Research Health, in collaboration with the Norwegian Labor and Welfare Administration (NAV).
Aims and objectives
The aim of the project Supported Employment and preventing Early Disability (SEED-trial) is to compare two interventions to increase labor market participation in young people at risk of early work disability: Traditional Vocational Rehabilitation (TVR) versus Supported Employment (SE).
Background measures
Each participant will be asked to complete questionnaires including background information on demographics and employment history.
Outcome measures
Primary outcome: competitive employment
The primary outcome of the SEED-trial is competitive employment at any time during the 12 months after enrollment in the study. Competitive employment is here defined as working in a job on the competitive labor market, at usual wages, with regular supervision.
Additionally, success in employment will be defined using a range of standardized indicators of employment outcomes used in IPS studies [40], including rate of job acquisition, amount and duration of work, total wages, and number of days from enrollment in the study to employment. Information about receipt of social security benefits (sickness and disability benefits, unemployment, work assessment allowance), income, financial assistance, and educational activity (started or completed education), will also be collected.
We will use three sources of information for competitive employment: Survey data for hours worked and success in employment; register data from the NAV for receipt of social security benefits and income; and register data from Statistics Norway (SSB) for financial assistance and educational activity.
Secondary outcomes: self-reported health and well-being
Questionnaires distributed to all participants will further measure a range of secondary and non-vocational outcomes related to health and well-being, including interventions and treatment received for the last 6 months, experiences with bullying and violence, sleep problems, and the following variables:
Alcohol and drug abuse will be measured using the 3-item Alcohol Use Disorders Identification Test (AUDIT-C) [41] screening for problem drinking, and the 11-item Drug Use Disorders Identification Test (DUDIT) [42] screening for drug-related problems and drug dependence.
Coping will be measured using the 7-item Theoretically Originated Measure of the Cognitive Activation Theory of Stress (TOMCATS) [43], consisting of 3 subscales: coping (1 item), helplessness (3 items), and hopelessness (3 items).
Disability will be measured using the 12-item version of the WHO Disability Assessment Schedule 2.0 (WHODAS 2.0), measuring functioning in 6 domains of life: cognition (2 items), mobility (2 items), self-care (2 items), getting along (2 items), life activities (2 items), and participation (2 items) [44].
Fatigue will be measured using the 11-item Chalder Fatigue Questionnaire (CFQ) consisting of 2 subscales: physical fatigue (7 items) and mental fatigue (4 items) [45].
Illness perceptions will be measured using the 9-item Brief Illness Perception Questionnaire (B-IPQ) [46], measuring 9 dimensions of illness perceptions: consequences (1 item), timeline (1 item), personal control (1 item), treatment control (1 item), identity (1 item), coherence (1 item), emotional representation (1 item), and concern (1 item), in addition to an open-ended item concerning causal factors (1 item).
Mental health will be measured using the 25-item Hopkins Symptom Checklist (HSCL-25) [47], consisting of 2 subscales: anxiety symptoms (10 items) and depression symptoms (15 items).
Social support will be measured using a revised 11-item version of the Social Support Inventory [48, 49] using 2 subscales as suggested by Øyeflaten et al. [50]: directive social support (4 items) and nondirective social support (7 items).
Subjective health complaints will be measured using the 29-item Subjective Health Complaints Inventory (SHC), consisting of 5 subscales: musculoskeletal pain (8 items), pseudoneurology (7 items), gastrointestinal problems (7 items), allergy (5 items), and flu (2 items) [51].
Quality of life will be measured using the 5-item EuroQol questionnaire (EQ-5D) including a visual analogue scale (EQ-VAS) [52].
Participants and randomization
Inclusion and exclusion
Eligible participants will consist of unemployed individuals aged < 30 years old, who are receiving temporary benefits due to various social- or health-related problems. Attending employment services overseen by the NAV is a requirement for recipients of these benefits, and we will invite all those who are intended for the specific traditional employment service called “traineeship in a sheltered business”. The only additional exclusion criteria are that participants must have an expressed desire to work and sufficient language skills to answer questionnaires in Norwegian.
Recruitment and randomization
Nine local NAV-offices throughout the Hordaland County are involved in the project. Caseworkers at each office will refer all eligible participants to general information meetings organized by researchers at Uni Research Health in collaboration with NAV. The meetings include detailed information about the project and invitation to participate in the study. Interested individuals will be asked to read and give informed consent, and researchers will record their personal information (name, contact details, and national identification number) and provide each participant with an ID-number on the spot. ID-numbers will be randomized at Uni Research Health after the meetings, using premade computer-generated lists with a 1:1 randomization ratio. Information about randomization outcome will be communicated by e-mail or telephone to the relevant caseworker at NAV, who contacts their client and the relevant vocational rehabilitation organization.
Data collection and data management
Survey data will be collected at baseline, 6 and 12 months. Baseline questionnaires will be administered at the information meetings, and participants complete their information electronically on iPads with secure software (Qualtrics®), or in paper format if preferred. Follow-up questionnaires will be administered electronically to participants providing their e-mail address at baseline, or in paper format via regular mail.
Data collected using iPads will automatically be electronically transferred to and stored in a secure online database. Data collected in paper form will be entered manually by the data manager at Uni Research Health and sent to the same database, after which the original questionnaires will be stored in a locked filing cabinet.
Register data will be collected retrospectively for 3 years before baseline, and for a 5-year period after enrollment date. The information will be de-identified and merged with survey data, while the identifier is secured in a locked and fireproof safe.
Study design
The SEED-trial is designed as a randomized controlled trial (RCT), and participants are randomly assigned to 1 of 2 interventions (Fig. 1).
Fig. 1.
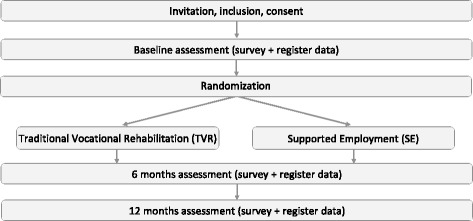
Study design
Interventions
Both interventions in this trial are offered by VR organizations overseen by the NAV, and are part of the various employment schemes offered to people on temporary benefits in Norway. Participants continue to receive temporary benefits while attending the services, which are normally offered for up to two or three years, depending on the specific intervention and individual needs.
Traditional Vocational Rehabilitation (TVR)
The first group will be referred to a TVR organization, where they will receive a traineeship in a sheltered business with follow-up from trained advisors and department supervisors.
This intervention is service as usual for the study participants, and is currently offered to clients who are considered by their caseworker to have need for special assistance to obtain work. The specific approach falls within the train-then-place principle, and participants receive preparatory work training in a sheltered environment before pursuing employment. The goal of the intervention is to improve the participant’s work skills and opportunities for entering the labor market, and includes follow-up geared towards finding a job. The traineeships are offered by various sheltered businesses in the area with a range of departments including canteens and catering, car repair, day-care services, upholstery and interior decoration, transport, laundry services, welding, and warehouse handling. The distribution of participants to the various departments will follow usual practice, and is conducted at NAV based on the individual caseworker’s description of the client’s interests and goals, as well as availability and waiting-lists.
Supported Employment (SE)
The second group will be referred to the vocational rehabilitation organization Fretex Vest-Norge, where they will receive SE by trained job specialists following the evidence-based principles of IPS SE.
The intervention is based on the place-then-train principle, aiming to help people with health problems or other challenges participate in the competitive labor market, without the use of prevocational training, stepwise and sheltered approaches, or make-work jobs. It aims to find a good job match for the individual followed by on-the-job support after employment, and is based on a belief that anyone who wants to work can hold a job in the normal labor market as long as it is the right job and work environment for that individual.
Adaptions to the IPS SE model
As the manualized intervention of IPS SE was originally developed for patients with SMI, job specialists will need to make some adjustments to the services offered based on the individual participant’s challenges. One necessary adjustment concerns the principle of integrating employment services with mental health treatment, as that will not be applicable for participants that do not suffer from mental illness. In cases where participants are receiving treatment for other health problems, job specialists will establish contact with their respective health practitioners instead.
The implementation will be led by an experienced IPS trainer, who will also be in charge of the fidelity reviews, using the IPS fidelity scale [53], which is a standardized and validated scale for measuring adherence to the IPS model [54]. Fidelity reviews will be conducted using document review, calendar review, observations, and interviews of the different stakeholders, in order to determine to what degree the SE intervention fulfills the criteria for IPS SE. These evaluations will be used for quality improvement of services throughout the study period, aiming to adhere to the manualized and evidence-based treatment in spite of the necessary adaptions.
Sample size calculation
Our estimates of sample size are based on international input-data from previous IPS-studies where a mean competitive employment rate of 61 % has been found for IPS and 23 % for controls [55]. If we use 61 and 23 % as possible employment rates, we will need 31 participants in each group in order to obtain a statistical significant difference (with a 5 % significance level and power of 90 %). In order to enable stratified analyses to investigate treatment effects for sub-groups (e.g. for gender), we aim at including a total of 124 participants. The inclusion period will last for up to 2 years and close when the targeted number of participants has been reached.
Statistical analyses
Assessment of treatment effects will be analyzed using standard statistical methods, including t-tests for continuous data and chi-square tests for categorical data. Logistic regression will be performed to study potential moderators of treatment effects. For repeated measures over time (e.g. for sick leave), the statistical analyses may be extended to generalized estimation equations (GEE), to account for correlated data. All analyses will follow the intention to treat principle.
Cost-benefit analysis
Economic returns will be calculated based on treatment effects obtained from the statistical analyses, and will be evaluated using a standard cost benefit formula [56–58], as used by Hagen et al. [59].
Benefit will be measured in terms of increases in the net present value of production, as indicated by an increase in labor market participation. This is calculated as the product of the treatment effect, i.e. the increase in labor market participation and the productivity gains for the society when a person is employed as opposed to receiving social security benefits. Cost of the intervention is measured by treatment cost and costs related to follow-up outside the intervention in the different treatment groups. Health care utilization will be measured using survey data from the participants providing information about health and use of health services.
Discussion
The SEED-trial will provide new knowledge about the effect of TVR versus SE in increasing labor market participation among young unemployed with various social- and health related problems. It will be the first RCT to look at SE for this important and vulnerable group at risk of being excluded from the labor market even before they have had the chance to establish themselves on the labor market.
Abbreviations
APS, traineeship in a sheltered business; IPS, individual placement and support; NAV, Norwegian labor and welfare administration; RCN, Research Council of Norway; RCT, randomized controlled trial; REC, Norwegian Regional Committees for Medical and Health Research Ethics; SE, Supported Employment; SSB, Statistics Norway; TMG, trial management group; TSC, trial steering committee; TVR, Traditional Vocational Rehabilitation
Acknowledgements
The Trial Steering Committee (TSC) is the scientific advisory board responsible for the general overview of the project and its progress. The Trial Management Group (TMG) is the project group responsible for the daily management and coordination of the trial. It involves researchers and other people of resource associated with the project.
The TSC consists of:
• Ph.D. Silje Endresen Reme (principal investigator)
• Ph.D. Torill H. Tveito (co-principal investigator)
• Professor Hege Eriksen (Uni Research Health)
• Associate professor Astrid Grasdal (responsible for the cost/benefit analysis)
• Professor Gary Bond (international collaborator from the Dartmouth Psychiatric Research Center, advisor and consultant on IPS implementation and methodological expertise)
• Ph.D. Cécile Boot (international collaborator from the EMGO Institute for Health and Care Research at the University of Amsterdam, advisor and consultant on effect-evaluation)
• Professor Patric Loisel (international collaborator from the Dalla Lana School of Public Health, University of Toronto, advisor and consultant on feasibility and implementation)
The TMG consists of:
• Principal investigators:
PhD Silje E. Reme
PhD Torill H. Tveito
• Trial coordinator:
MSc Vigdis Sveinsdottir
• Co-workers:
Associate professor Astrid Grasdal
Associate professor Camilla Løvvik
Professor Gary R. Bond
Professor Stein Atle Lie
PhD Eline Ree
PsyD Ingrid B. Olsen
MD Line R. Solberg
BSc Thomas Knutzen
• Administrative personnel:
Nina Konglevoll (data manager)
Mariann Apelseth (accountant)
Funding
The project is externally funded by the government agency Research Council of Norway (RCN), program for sickness absence, work and health. The funding source does not have any role in the design of the study, data collection, analysis and interpretation of data, or decisions to submit articles for publication.
Availability of data and materials
Data from the trial will not be shared, seeing as the study participants have not agreed to sharing of any data or materials upon enrollment and collection. The study also involves data from Norwegian national registries that the authors are not allowed to share by law.
Authors’ contributions
SER and VS developed the initial protocol and applied for funding. All authors contributed in the planning of the project, and in preparing, reading and approving the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable
Ethical approval and consent to participate
The Norwegian Regional Committees for Medical and Health Research Ethics (REC) concluded that the SEED-trial did not fall under the Health Research Act and therefore did not require ethics approval. The project was approved by the Norwegian Social Science Data Services (project number: 38271), and is registered in the international trial register ClinicalTrials.gov (NCT02375074). The trial adheres to the ethical principles of the Helsinki declaration. Prior to inclusion, all participants receive oral as well as written information about the trial, the randomization process, personal confidentiality, and the right to withdraw from the project at any time, and sign declarations of informed consent and voluntary participation.
Endnotes
Not applicable
Contributor Information
Vigdis Sveinsdottir, Email: Vigdis.Sveinsdottir@uni.no.
Torill Helene Tveito, Email: Torill.Tveito@uni.no.
Gary R. Bond, Email: Gary.R.Bond@dartmouth.edu
Astrid Louise Grasdal, Email: Astrid.Grasdal@econ.uib.no.
Stein Atle Lie, Email: Stein.Lie@iko.uib.no.
Silje Endresen Reme, Email: Silje.Reme@uni.no.
References
- 1.Bragstad T, Ellingsen J, Lindbøl MN. Hvorfor blir det flere uførepensjonister? Arbeid og velferd. 2012;2012(1):26–39. [Google Scholar]
- 2.NAV . The development of disability pension, by December 15th 2015. Oslo: Norwegian Labour and Welfare Administration (NAV); 2016. [Google Scholar]
- 3.NAV . Recipients of disability pension by gender and age, 31.12.2005-2014. Oslo: Norwegian Labour and Welfare Administration (NAV); 2015. [Google Scholar]
- 4.Statistics Norway (SSB) Statbank, table 10211: Population, by sex and age. Oslo: Statistics Norway (SSB); 2016. [Google Scholar]
- 5.NAV . Recipients of disability pension by diagnosis, age, and gender, per 31.12.2011. Oslo: Norwegian Labour and Welfare Administration (NAV); 2012. [Google Scholar]
- 6.NAV . Days of sick leave 4th quarter 2005-2014. Diagnosis and gender. Numbers and percent. Oslo: Norwegian Labour and Welfare Administration (NAV); 2014. [Google Scholar]
- 7.Lindbøl M. The development in disability pension, December 31st 2011 (statistics note) Oslo: The Norwegian Labor and Welfare Administration (NAV); 2012. [Google Scholar]
- 8.Brunborg H. Increasing life expectancy and the growing elderly population. Norsk Epidemiologi. 2012;22(2):75–83. doi: 10.5324/nje.v22i2.1552. [DOI] [Google Scholar]
- 9.Hultin H, Lindholm C, Möller J. Is there an association between long-term sick leave and disability pension and unemployment beyond the effect of health status? – A cohort study. PLoS One. 2012;7:4. doi: 10.1371/journal.pone.0035614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.NAV. (2013). Arbeid kan hindre langvarig sykefravær. Oslo: The Norwegian Labour and Welfare Administration (NAV).
- 11.Tveito TH, Halvorsen A, Lauvålien JV, Eriksen HR. Room for everyone in working life? 10 % of the employees – 82 % of the sickness leave. Norsk Epidemiologi. 2002;12(1):63–8. [Google Scholar]
- 12.Wehman P, Moon MS. Vocational rehabilitation and supported employment. Baltimore: Paul Brookes; 1988. [Google Scholar]
- 13.Bond GR, Drake RE. Making the Case for IPS Supported Employment. Adm Policy Ment Health. 2014;41(1):69-73. [DOI] [PubMed]
- 14.Nazarov ZE, Golden TP, Schrader S. Prevocational services and supported employment wages. J Vocat Rehabil. 2012;37(2):119–29. [Google Scholar]
- 15.Bond GR, Salyers MP, Dincin J, Drake R, Becker DR, Fraser VV, Haines M. A randomized controlled trial comparing two vocational models for persons with severe mental illness. J Consult Clin Psychol. 2007;75(6):968–82. doi: 10.1037/0022-006X.75.6.968. [DOI] [PubMed] [Google Scholar]
- 16.Davis LL, Leon AC, Toscano R, Drebing CE, Ward LC, Parker PE, Kashner TM, Drake RE. A randomized controlled trial of supported employment among veterans with posttraumatic stress disorder. Psychiatr Serv. 2012;63(5):464–70. doi: 10.1176/appi.ps.201100340. [DOI] [PubMed] [Google Scholar]
- 17.Drake RE, McHugo GJ, Becker DR, Anthony WA, Clark RE. The New Hampshire study of supported employment for people with severe mental illness. J Consult Clin Psychol. 1996;64(2):391–9. doi: 10.1037/0022-006X.64.2.391. [DOI] [PubMed] [Google Scholar]
- 18.Drake RE, McHugo GJ, Bebout RR, Becker DR, Harris M, Bond GR, Quimby E. A randomized clinical trial of supported employment for inner-city patients with severe mental disorders. Arch Gen Psychiatry. 1999;56(7):627–33. doi: 10.1001/archpsyc.56.7.627. [DOI] [PubMed] [Google Scholar]
- 19.Lehman AF, Goldberg R, Dixon LB, McNary S, Postrado L, Hackman A, McDonnell K. Improving employment outcomes for persons with severe mental illnesses. Arch Gen Psychiatry. 2002;59(2):165–72. doi: 10.1001/archpsyc.59.2.165. [DOI] [PubMed] [Google Scholar]
- 20.Mueser KT, Clark RE, Haines M, Drake RE, McHugo GJ, Bond GR, Essock SM, Becker DR, Wolfe R, Swain K. The Hartford study of supported employment for persons with severe mental illness. J Consult Clin Psychol. 2004;72(3):479–90. doi: 10.1037/0022-006X.72.3.479. [DOI] [PubMed] [Google Scholar]
- 21.Gold PB, Meisler N, Santos AB, Carnemolla MA, Williams OH, Keleher J. Randomized trial of supported employment integrated with assertive community treatment for rural adults with severe mental illness. Schizophr Bull. 2006;32(2):378–95. doi: 10.1093/schbul/sbi056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nuechterlein KH. 7th International Conference on Early Psychosis, Early Psychoses: A lifetime Perspective. Amsterdam: Blackwell Publishing Asia; 2010. Individual placement and support after an initial episode of schizophrenia: the UCLA randomized controlled trial; pp. 1–15. [Google Scholar]
- 23.Bond GR, Kim SJ, Becker DR, Swanson SJ, Drake RE, Krzos IM, Fraser VV, O’Neill S, Frounfelker RL. A controlled trial of Supported Employment for people with severe mental illness and justice involvement. Psychiatr Serv. 2015;66(10):1027–34. doi: 10.1176/appi.ps.201400510. [DOI] [PubMed] [Google Scholar]
- 24.Drake RE, Frey W, Bond GR, Goldman HH, Salkever D, Miller A, Moore TA, Riley J, Karakus M, Milfort R. Assisting Social Security Disability Insurance beneficiaries with schizophrenia, bipolar disorder, or major depression in returning to work. Am J Psychiatry. 2013;170(12):1433–41. doi: 10.1176/appi.ajp.2013.13020214. [DOI] [PubMed] [Google Scholar]
- 25.Killackey EJ, Allott KA, Cotton SM, Chinnery GL, Sun P, Collins Z, Massey J, Baksheev G, Jackson HJ. Vocational recovery in first episode psychosis: first results from a large controlled trial of IPS. Early Interv Psychiatry. 2012;6(Supplement 1):13. [Google Scholar]
- 26.Bejerholm U, Areberg C, Hofgren C, Sandlund M, Rinaldi M. Individual Placement and Support in Sweden-A randomized controlled trial. Nord J Psychiatry. 2014;1:1–10. doi: 10.3109/08039488.2014.929739. [DOI] [PubMed] [Google Scholar]
- 27.Oshima I, Sono T, Bond GR, Nishio M, Ito J. A randomized controlled trial of individual placement and support in Japan. Psychiatr Rehabil J. 2014;37(2):137–43. doi: 10.1037/prj0000085. [DOI] [PubMed] [Google Scholar]
- 28.Viering S, Jager M, Bartsch B, Nordt C, Rossler W, Warnke I, Kawohl W. Supported Employment for the reintegration of disability pensioners with mental illnesses: a randomized controlled trial. Front Public Health. 2015;3:237. doi: 10.3389/fpubh.2015.00237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Waghorn G, Dias S, Gladman B, Harris M, Saha S. A multi-site randomised controlled trial of evidence-based supported employment for adults with severe and persistent mental illness. Aust Occup Ther J. 2014;61(6):424–36. doi: 10.1111/1440-1630.12148. [DOI] [PubMed] [Google Scholar]
- 30.Heslin M, Howard L, Leese M, McCrone P, Rice C, Jarrett M, Spokes T, Huxley P, Thornicroft G. Randomized controlled trial of supported employment in England: 2 year follow-up of the Supported Work and Needs (SWAN) study. World Psychiatry. 2011;10(2):132–7. doi: 10.1002/j.2051-5545.2011.tb00035.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Burns T, Catty J, Becker T, Drake RE, Fioritti A, Knapp M, Lauber C, Rossler W, Tomov T, van Busschbach J, et al. The effectiveness of supported employment for people with severe mental illness: a randomised controlled trial. Lancet. 2007;370(9593):1146–52. doi: 10.1016/S0140-6736(07)61516-5. [DOI] [PubMed] [Google Scholar]
- 32.Killackey E, Jackson HJ, McGorry PD. Vocational intervention in first-episode psychosis: individual placement and support v. treatment as usual. Br J Psychiatry. 2008;193(2):114–20. doi: 10.1192/bjp.bp.107.043109. [DOI] [PubMed] [Google Scholar]
- 33.Latimer EA, Lecomte T, Becker DR, Drake RE, Duclos I, Piat M, Lahaie N, St-Pierre MS, Therrien C, Xie H. Generalisability of the individual placement and support model of supported employment: results of a Canadian randomised controlled trial. Br J Psychiatry. 2006;189:65–73. doi: 10.1192/bjp.bp.105.012641. [DOI] [PubMed] [Google Scholar]
- 34.Wong KK, Chiu R, Tang B, Mak D, Liu J, Chiu SN. A randomized controlled trial of a supported employment program for persons with long-term mental illness in Hong Kong. Psychiatr Serv. 2008;59(1):84–90. doi: 10.1176/ps.2008.59.1.84. [DOI] [PubMed] [Google Scholar]
- 35.Hoffmann H, Jackel D, Glauser S, Mueser KT, Kupper Z. Long-term effectiveness of supported employment: 5-year follow-up of a randomized controlled trial. Am J Psychiatry. 2014;171(11):1183–90. doi: 10.1176/appi.ajp.2014.13070857. [DOI] [PubMed] [Google Scholar]
- 36.Michon H, van Busschbach JT, Stant AD, van Vugt MD, van Weeghel J, Kroon H. Effectiveness of individual placement and support for people with severe mental illness in The Netherlands: a 30-month randomized controlled trial. Psychiatr Rehabil J. 2014;37(2):129–36. doi: 10.1037/prj0000061. [DOI] [PubMed] [Google Scholar]
- 37.Twamley EW, Vella L, Burton CZ, Becker DR, Bell MD, Jeste DV. The efficacy of supported employment for middle-aged and older people with schizophrenia. Schizophr Res. 2012;135(1-3):100–4. doi: 10.1016/j.schres.2011.11.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Drake RE, Bond GR, Becker DR. Individual placement and support: an evidence-based approach to Supported Employment. New York: Oxford University Press, USA; 2012. [Google Scholar]
- 39.Becker DR, Swanson S, Bond GR, Merrens MR. Evidence-based supported employment fidelity review manual. 2. Lebanon: Dartmouth Psychiatric Research Center; 2011. [Google Scholar]
- 40.Bond GR, Campbell K, Drake RE. Standardizing measures in four domains of employment outcomes for individual placement and support. Psychiatr Serv. 2012;63(8):751–7. doi: 10.1176/appi.ps.201100270. [DOI] [PubMed] [Google Scholar]
- 41.Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med. 1998;158(16):1789–95. doi: 10.1001/archinte.158.16.1789. [DOI] [PubMed] [Google Scholar]
- 42.Berman AH, Bergman H, Palmstierna T, Schlyter F. DUDIT (Drug Use Disorders Identification Test) manual. Stockholm: Karolinska Institutet; 2003. [Google Scholar]
- 43.Odeen M, Westerlund H, Theorell T, Leineweber C, Eriksen HR, Ursin H. Expectancies, socioeconomic status, and self-rated health: use of the simplified TOMCATS questionnaire. Int J Behav Med. 2012;1:1. doi: 10.1007/s12529-012-9221-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Üstün TB, Kostanjsek N, Chatterji S, Rehm J. Measuring health and disability: manual for WHO Disability Assessment Schedule (WHODAS 2.0): World Health Organization; 2010.
- 45.Chalder T, Berelowitz G, Pawlikowska T, Watts L, Wessely S, Wright D, Wallace EP. Development of a fatigue scale. J Psychosom Res. 1993;37(2):147–53. doi: 10.1016/0022-3999(93)90081-P. [DOI] [PubMed] [Google Scholar]
- 46.Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–7. doi: 10.1016/j.jpsychores.2005.10.020. [DOI] [PubMed] [Google Scholar]
- 47.Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L. The Hopkins Symptom Checklist (HSCL): a self-report symptom inventory. Behav Sci. 1974;19(1):1–15. doi: 10.1002/bs.3830190102. [DOI] [PubMed] [Google Scholar]
- 48.Fisher EB, Bickle C, Harber K, Hughes CR, Jeffe DB, Kahl L, La Greca AM. Benefits of Directive and Nondirective Support are moderated by severity of circumstances. San Francisco: Annual Meeting of Society of Behavioral Medicine; 1997. [Google Scholar]
- 49.Fisher EB, La Greca AM, Greco P, Arfken C, Schneiderman N. Directive and nondirective social support in diabetes management. Int J Behav Med. 1997;4(2):131–44. doi: 10.1207/s15327558ijbm0402_3. [DOI] [PubMed] [Google Scholar]
- 50.Øyeflaten I, Gabriele JM, Fisher EB, Eriksen HR. Social support and subjective health complaints in occupational rehabilitation. Int J Ther Rehabil. 2010;17(8):424–35. doi: 10.12968/ijtr.2010.17.8.49291. [DOI] [Google Scholar]
- 51.Eriksen HR, Ihlebaek C, Ursin H. A scoring system for subjective health complaints (SHC) Scand J Public Health. 1999;27(1):63–72. doi: 10.1177/14034948990270010401. [DOI] [PubMed] [Google Scholar]
- 52.The EuroQol Group EuroQol-a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208. doi: 10.1016/0168-8510(90)90421-9. [DOI] [PubMed] [Google Scholar]
- 53.Becker DR, Swanson S, Reese SL, Bond GR, McLeman BM. Evidence-based supported employment fidelity review manual. 3. Lebanon: Dartmouth Psychiatric Research Center; 2016. [Google Scholar]
- 54.Bond GR, Peterson AE, Becker DR, Drake RE. Validation of the Revised Individual Placement and Support Fidelity Scale (IPS-25) Psychiatr Serv. 2012;63(8):758–63. doi: 10.1176/appi.ps.201100476. [DOI] [PubMed] [Google Scholar]
- 55.Bond GR, Drake RE, Becker DR. An update on randomized controlled trials of evidence-based supported employment. Psychiatr Rehabil J. 2008;31(4):280–90. doi: 10.2975/31.4.2008.280.290. [DOI] [PubMed] [Google Scholar]
- 56.Berkowitz M. Measuring the effects of public programs. Cost and benefits in vocational rehabilitation. Philadelphia: Temple University Press; 1988. [Google Scholar]
- 57.Haveman RH, Halberstadt V, Burhauser RV. Public policy toward disabled workers. Cross-national analyses of Economic Impacts. Ithaca: Cornell University Press; 1984. [Google Scholar]
- 58.Risa AE. Economic evaluation of vocational rehabilitation programs. In: Social policy and the labor market. edn. Edited by de Jong PR, Marmor TR: Aldershot: Ashgate; 1997;191–203.
- 59.Hagen EM, Grasdal A, Eriksen HR. Does early intervention with a light mobilization program reduce long-term sick leave for low back pain: a 3-year follow-up study. Spine. 2003;28(20):2309–15. discussion 2316. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data from the trial will not be shared, seeing as the study participants have not agreed to sharing of any data or materials upon enrollment and collection. The study also involves data from Norwegian national registries that the authors are not allowed to share by law.