

Abstract
We report a 53-year-old female who presented with complaints of sudden onset breathlessness, cough with expectoration for 6 months, and a right lung base lesion in the chest X-ray, which was diagnosed and treated as bronchopneumonia by the family physician. High-resolution computed tomography of the chest was done which revealed a large heterogeneously enhancing mass in the right thoracic cavity. She underwent thoracotomy and was found to have a giant encapsulated and well-circumscribed mass arising from the pleura. Excision biopsy of the mass revealed it to be an ancient schwannoma. Ancient schwannoma of the pleura is a very rare entity. Complete surgical resection is curative.
KEY WORDS: Neurilemmoma/surgery, peripheral nerve sheath tumor, schwannoma
INTRODUCTION
Schwannomas are benign tumors originating from Schwann cells of the neural sheath. Ancient schwannoma is a variant of schwannoma which is an encapsulated tumor with benign nature usually located in the retroperitoneum. These tumors are usually asymptomatic and can attain large size before presentation. Ancient schwannomas arising from the pleura is a rare condition. Less than twenty cases of pleural schwannomas have been reported in the literature.[1]
CASE REPORT
A 53-year-old female came to the emergency department with sudden onset of breathlessness since 1 day. She had cough with expectoration since 6 months and dull right chest pain. She was diagnosed and treated as bronchopneumonia by the family physician.
On general examination, she was tachypneic and afebrile. Chest examination revealed absent breath sounds in the right mid and lower zone. Chest X-ray showed homogeneous opacity in the middle and lower zone of the right hemithorax. Contrast-enhanced computed tomography thorax showed a large spherical shaped heterogeneously enhancing mass lesion (12 cm) with calcifications in the lower half of posterior third of the right thoracic cavity [Figure 1a]. Bronchoscopy did not reveal any intraluminal pathology. Ultrasound-guided needle biopsy of the mass revealed a spindle cell tumor. Since there was no invasion of surrounding structure, it was considered to be a totally resectable mass.
Figure 1.
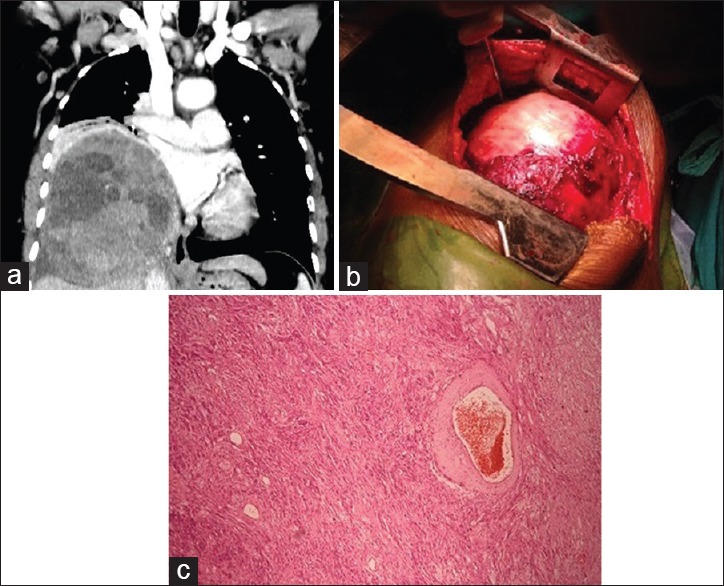
(a) Contrast-enhanced computed tomography thorax coronal section shows a large spherical heterogeneously enhancing mass lesion in the right hemithorax with calcifications within. (b) Intraoperative image shows a well-circumscribed encapsulated mass. (c) Histopathologic slide of specimen shows calcification, cystic degeneration, and infiltration by lymphomononuclear cells and histiocytes
The patient was taken up for surgery after informed consent. Under general anesthesia and single lung ventilation, the patient was placed in a left lateral decubitus position and right posterolateral thoracotomy was done. The latissimus dorsi muscle was divided, and the serratus anterior muscle was elevated and retracted anteriorly. The pleura was entered through the sixth intercostal space. We evaluated preoperatively the likelihood of adhesions to the surrounding structures. A large firm to hard mass measuring around 20 cm × 20 cm × 15 cm, with wide attachment to pleura was originating from parietal pleura dorsally [Figure 1b]. We carefully dissected the tumor from diaphragm, lower lobe, and esophagus. The encapsulated mass was removed in toto. The postoperative course was uneventful. The patient was asymptomatic at 1, 3, and 6 months follow-up. Postoperative histopathological examination revealed gross to large nodular encapsulated specimen. Cut section of the tumor was ninety percent solid and ten percent cystic with lobulated yellowish brown areas of necrosis. Tumor showed areas of calcification and cystic degeneration. Microscopy revealed extensive areas of degeneration, ischemic necrosis with cystic degeneration, and infiltration by lymphomononuclear cells and histiocytes. The tumor cells were relatively monomorphic and showed plump spindle to oval nuclei, dispersed granular chromatin, and moderate amount of eosinophilic cytoplasm with indistinct cytoplasmic boundaries. A few areas show vague nuclear palisading and syncytia formation. Many hyalinized vessels were seen. The tumor was reported as ancient schwannoma [Figure 1c].
DISCUSSION
Our case report is rare as the ancient schwannoma arising from the pleura is not a common entity. Schwannomas account for 95% of the posterior mediastinal neurogenic tumors.[2,3] Ancient schwannomas are a variant of schwannoma that constitutes 0.8% of all soft tissue tumors.[4] They usually occur between the age group of thirty and sixty years and are solitary. Multiple masses when present are associated with Von Recklinghausen's disease. Patients become symptomatic when the tumor attains large size like in our patient.[5] These tumors can occur in intracranial sites, retroperitoneum, flexor surfaces of the limbs, and posterior spinal roots. High-resolution computed tomography is the investigation of choice. Surgical excision of a solitary schwannoma is curative and has excellent prognosis.
Incomplete excision causes recurrence. Malignant transformation is rare but has been reported. Ancient schwannoma shows prominent degeneration changes such as cyst formation, calcification, hyalinized vessels, hemorrhage, and cytologic atypia. Calcification and cystic degeneration are seen only in a few cases in the literature.[6]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Abou Al-Shaar H, Qutob S, Abu-Zaid A, Azzam A, Amin T, Mohammed S. Primary pleural benign myxoid schwannoma in an 18-year-old female: A case report and literature review. Case Rep Oncol Med. 2014;2014:296961. doi: 10.1155/2014/296961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Whooley BP, Urschel JD, Antkowiak JG, Takita H. Primary tumors of the mediastinum. J Surg Oncol. 1999;70:95–9. doi: 10.1002/(sici)1096-9098(199902)70:2<95::aid-jso6>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]
- 3.Reeder LB. Neurogenic tumors of the mediastinum. Semin Thorac Cardiovasc Surg. 2000;12:261–7. doi: 10.1053/stcs.2000.16738. [DOI] [PubMed] [Google Scholar]
- 4.Kara M, Ozkan M, Sak SD, Aksu O, Kavukçu S. Giant ancient schwannoma of the posterior mediastinum cytologically misdiagnosed as a malignant tumour. A case report. Acta Chir Belg. 2002;102:464–6. doi: 10.1080/00015458.2002.11679353. [DOI] [PubMed] [Google Scholar]
- 5.Ortigara L, Rosemberg N, Siqueira R, Neto F. Resection of a mediastinal schwannoma using video-assisted thoracoscopy. J Bras Pneumol. 2006;32:172–5. doi: 10.1590/s1806-37132006000200013. [DOI] [PubMed] [Google Scholar]
- 6.Dodd LG, Marom EM, Dash RC, Matthews MR, McLendon RE. Fine-needle aspiration cytology of “ancient” schwannoma. Diagn Cytopathol. 1999;20:307–11. doi: 10.1002/(sici)1097-0339(199905)20:5<307::aid-dc12>3.0.co;2-f. [DOI] [PubMed] [Google Scholar]