

Abstract
Introduction
Middle East Respiratory Syndrome (MERS) is a disease caused by beta corona virus. From April 11th to 9th June 2014, World Health Organization (WHO) reported a total of 402 laboratory confirmed cases of MERS from KSA, out of which 132 cases were reported from Riyadh alone.
Aim
The aim of this study was to assess the knowledge and apprehension of patients about MERS visiting Al Farabi College of Dentistry, Riyadh, Saudi Arabia.
Materials and Methods
A cross-sectional questionnaire based survey was conducted which consisted of 10 self-prepared questions. A total of 404 patients participated in this study.
Results
Three hundred and forty patients had heard about MERS. Nearly a quarter of the patients (25.74%) were apprehensive about undergoing dental treatment because of MERS. A little more than half of the patients (50.99%) knew that camel was a source of Middle East Respiratory Syndrome-Corona virus. Most of the patients (80.72%) were aware of the infection control measures to be followed by dentist and 138 patients claimed they took some precaution when present inside the dental college.
Conclusion
Majority of the patients had heard about MERS and was aware of the infection control measures. However, some patients were apprehensive about undergoing dental treatment because of MERS. Further steps need to be taken to educate the patient’s about transmission of MERS and infection control measures in a dental hospital.
Keywords: Aerosol infection, Coronavirus, Respiratory infection
Introduction
Middle East Respiratory Syndrome (MERS) was first reported from a patient in Saudi Arabia who died of pneumonia due to a novel beta corona virus in September 2012 [1]. WHO has reported a total of 699 laboratory confirmed cases of MERS and 209 deaths due to MERS as in June 2014. Most of the cases were reported in Middle East countries Jordan, Kuwait, Oman, Qatar, Saudi Arabia (KSA), United Arab Emirates (UAE) and Yemen [2]. All the cases of MERS reported outside the Middle East were people who recently travelled from countries inside of the Middle East. Most of the cases reported were males and the median age was 49-year-old [3].
Corona viruses are a group of viruses which primarily infect the upper respiratory and gastrointestinal tract of birds and mammals [4]. Scientists identified a new type of corona virus belonging to the lineage C betacorona viruses, which was initially called novel coronavirus 2012 and now termed as Middle East Respiratory Syndrome Corona Virus (MERS-CoV) [1,5,6]. Research has confirmed that dromedary camels throughout the Arabian Peninsula and in parts of north and east Africa carry these viruses and further analysis concluded that camels can be infected with MERS-COV [7]. Dipeptidyl peptidase4 (DPP4, CD26) has been recognized as the cellular receptors for MERS-CoV, which is distributed regularly in mammal’s kidney and lung [8,9].
Clinical features of MERS closely resemble to those seen in Severe Acute Respiratory Syndrome (SARS). Most common symptoms are cough, fever and dyspnea. Apart from these, other symptoms seen are chills, headache, rigors, myalgia and malaise. Major complication of MERS is respiratory failure. It was also seen that more than half of the cases in KSA have had some underlying conditions [10].
A 75% of the reported cases are likely to acquire infection through human-human transmission (secondary cases) and 25% of the cases are likely to be acquired from animals (primary cases) [11]. Most common mode of transmission of MERS in KSA was through human to human transmission in health care settings. Epidemiologic investigations are in progress to understand the transmission pattern of this virus and risk of transmission between animals and humans [2].
According to WHO, MERS seems to follow a seasonal pattern with a sudden spurt in the incidence of new cases from March-April onwards. From 11th April to 9th June 2014, WHO reported a total of 402 laboratory confirmed cases of MERS from KSA, out of which 132 cases were reported from Riyadh alone and 114 cases of confirmed death were reported from KSA during the same period. Majority of the secondary cases were healthcare workers who were infected within the hospital and patients who had been to hospital for other reasons and were considered to have been infected with MERS-CoV in the hospital [2,11].
Aim
The aim of this survey was to analyze the knowledge and apprehension about MERS among the dental patients visiting Al Farabi College of Dentistry, Riyadh, KSA.
Materials and Methods
A cross-sectional questionnaire based survey was conducted from 2nd April 2014 to 25th May 2014. Ethical clearance was obtained from the institutional review board of Al Farabi College of Dentistry. A pilot study was conducted on 38 patients at Al Farabi College of Dentistry. Based on the response, appropriate adjustments were made. The findings of pilot study revealed that 81.5% of the patients were aware of MERS. Based on this, sample size was calculated at 99% confidence level with a margin of error of 5%
Z= Z value (2.576 for 99% confidence level)
P=percentage of picking a choice, expressed as a decimal (0.815).
C= confidence interval or margin of error expressed as decimal. (.05)
Sample size required was calculated as 400.20. In the present study, we included a total of 404 dental patients, who were selected randomly from the general outpatient Department of Al Farabi College of dentistry, Riyadh. Informed consent was obtained from the patients before the interview.
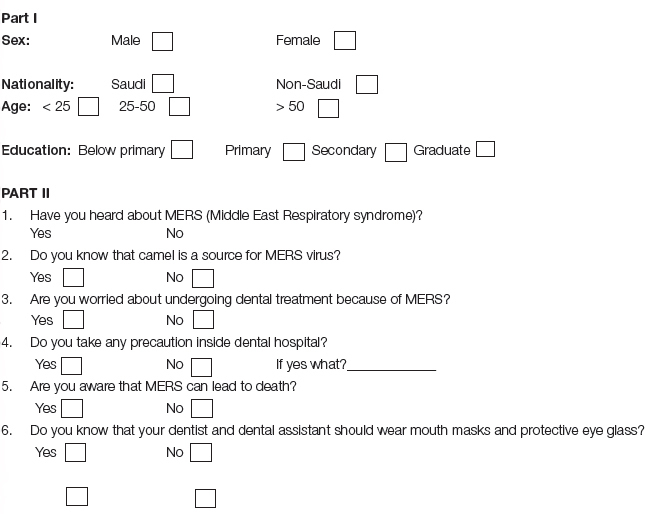
Questionnaire Design: The questionnaire consisted of 10 self-prepared questions and had two parts. The first part gathered personal information (four questions): age, sex, nationality, and education. According to nationality, patients were categorized as Saudi citizen or non-Saudi. Based on age, patients were categorized into three groups; <25, 25-50 and >50 years. Based on education level, patients were categorized as below primary, primary, secondary and graduate. The second part had six questions. Of these, five questions (four closed ended and one open ended) were used to assess the patient’s knowledge and apprehension about MERS and one question was used to assess patient’s knowledge about infection control. An option of ‘yes’ or ‘no’ was given to answer these questions.
Statistical Analysis
Statistical software used in the study was SPSS 21.0 version. Chi-square analysis was used to analyze statistical significance difference in the response between different groups. Statistical significance was set at p-value <0.05.
Results
A total of 404 patients participated in the study. Out of the 450 questionnaires delivered, 404 were returned (response rate was 89.78%). [Table/Fig-1] depicts the demographics of the participating patients.
[Table/Fig-1]:
Demographics of the patients.
| Factors | No. of respondents | % of respondents |
|---|---|---|
| Sex | ||
| Male | 268 | 66.34 |
| Female | 136 | 33.66 |
| Citizen | ||
| Saudi | 192 | 47.52 |
| Non-Saudi | 212 | 52.48 |
| Age group (years) | ||
| <25 | 132 | 32.67 |
| 25-50 | 204 | 50.50 |
| >50 | 68 | 16.83 |
| Education | ||
| Below primary | 0 | 0 |
| Primary | 70 | 17.33 |
| Secondary | 166 | 41.09 |
| Graduate | 168 | 41.58 |
| Total | 404 | 100.00 |
When asked whether they have heard about MERS, 340 patients (84.16%) responded positively. [Table/Fig-2] shows the response of the patients to this question based on age, sex, education and nationality. A statistically significant difference was seen in the response between male and females, with females responding more positively. Saudi citizens were more likely to have heard about MERS compared to non-Saudis. Younger age groups (<25 and 25-50 age group) have heard about MERS more than >50 age group. A significant difference was seen in the response between graduate, secondary educated and primary educated participants (p=0.0001)
[Table/Fig-2]:
Response of the patients when asked whether they heard about MERS.
| Factors | Yes (%) | No (%) | Chi-square | p-value |
|---|---|---|---|---|
| Sex | ||||
| Male | 214 (79.85) | 54 (20.15) | 11.081 | 0.0010* |
| Female | 126 (92.64) | 10 (7.36) | ||
| Citizen | ||||
| Saudi | 182 (94.79) | 10 (5.21) | 31.030 | 0.0001* |
| Non-Saudi | 158 (74.53) | 54 (25.47) | ||
| Age group (years) | ||||
| <25 | 122 (92.42) | 10 (7.58) | 20.67 | 0.0001* |
| 25-50 | 172 (84.31) | 32 (15.69) | ||
| >50 | 46 (67.64) | 22 (32.36) | ||
| Education | ||||
| Primary | 45(64.29) | 25 (35.71) | 44.274 | 0.0001* |
| Secondary | 132 (79.52) | 34 (20.48) | ||
| Graduate | 163 (97.02) | 5 (2.98) | ||
| Total | 340 (84.16) | 64 (15.84) | ||
* Statistically significant (p<0.05)
When asked whether they are aware that camel is a source of MERS virus, 206 patients responded positively (50.99%). [Table/Fig-3] shows the response of the patients to the question based on age, sex, education and nationality. A significant difference in response was seen in different categories of citizens and education.
[Table/Fig-3]:
Response of the patients on asked whether they know camel is a source of MERS virus.
| Factors | Yes (%) | No (%) | Chi-square | p-value |
|---|---|---|---|---|
| Sex | ||||
| Male | 140 (52.24) | 128(47.76) | 0.497 | 0.4810 |
| Female | 66 (48.53) | 70 (51.47) | ||
| Citizen | ||||
| Saudi | 116 (60.42) | 76 (39.58) | 13.010 | 0.0001* |
| Non-Saudi | 90 (42.45) | 122 (57.55) | ||
| Age group (years) | ||||
| <25 | 72 (54.55) | 60 (45.45) | 1.953 | 0.3771 |
| 25-50 | 104 (50.98) | 100 (49.02) | ||
| >50 | 30 (44.12) | 38 (55.88) | ||
| Education | ||||
| Primary | 18(25.71) | 52 (74.29) | 21.745 | 0.0001* |
| Secondary | 92 (55.42) | 74 (44.58) | ||
| Graduate | 96 (57.14) | 72 (42.86) | ||
| Total | 206 (50.99) | 198 (49.01) | ||
* Statistically significant (p<0.05)
One hundred and four patients (25.74%) claimed they were apprehensive about undergoing dental treatment because of MERS. [Table/Fig-4] depicts the response of the patients of different category to this question based on demographic characteristics. Apprehension was seen more among females (44.11%) compared to men (16.42%) and graduates (38.69%) compared to secondary (19.88%) and primary (8.57%) educated patients.
[Table/Fig-4]:
Response of the patients on asked whether they are worried about undergoing dental treatment because of MERS.
| Factors | Yes (%) | No (%) | Chi-square | p-value |
|---|---|---|---|---|
| Sex | ||||
| Male | 44 (16.42) | 224 (83.58) | 36.212 | 0.0001* |
| Female | 60 (44.11) | 76 (55.89) | ||
| Citizen | ||||
| Saudi | 56 (29.17) | 136 (70.83) | 2.244 | 0.1344 |
| Non-Saudi | 48(22.64) | 164 (77.36) | ||
| Age group | ||||
| <25 | 48 (36.36) | 84 (63.64) | 1.953 | 0.3771 |
| 25-50 | 50 (24.51) | 154 (75.49) | ||
| >50 | 6 (8.82) | 62 (91.18) | ||
| Education | ||||
| Primary | 6(8.57) | 64 (91.43) | 28.516 | 0.0001* |
| Secondary | 33 (19.88) | 133 (80.12) | ||
| Graduate | 65 (38.69) | 103 (61.31) | ||
| Total | 104 (25.74) | 300 (74.26) | ||
* Statistically significant (p<0.05)
[Table/Fig-5] shows the response of the patients when asked whether they take any precaution inside dental hospital. One hundred and thirty eight respondents (34.16%) claimed they took some kind of precaution. A significant difference was seen in response among three age groups. Also, subjects who were graduated seem to take more precaution when compared to secondary educated or primary educated. This was an open ended question and participants who responded positively were asked to mention what kind of precaution they took. A total of 61 participants (44.20%) claimed they cover the face with cloth and 36 respondents (26.09%) claimed they use mouth mask in the dental office while 41 respondents didn’t mention anything.
[Table/Fig-5]:
Response of the patients when asked whether they take any precaution inside dental college.
| Factors | Yes (%) | No (%) | Chi-square | p-value |
|---|---|---|---|---|
| Sex | ||||
| Male | 84 (31.34) | 184 (68.66) | 2.805 | 0.0946 |
| Female | 54 (39.71) | 82 (60.29) | ||
| Citizen | ||||
| Saudi | 72 (37.5) | 120 (62.5) | 1.817 | 0.1788 |
| Non-Saudi | 66(31.13) | 146(68.87) | ||
| Age group | ||||
| <25 | 66 (50.0) | 66 (50.0) | 27.457 | 0.0001* |
| 25-50 | 62 (30.39) | 142 (69.61) | ||
| >50 | 10(14.71) | 58 (85.29) | ||
| Education | ||||
| Primary | 8(11.43) | 62(88.57) | 21.778 | 0.0001* |
| Secondary | 58 (34.94) | 108 (65.06) | ||
| Graduate | 72 (42.86) | 96 (57.14) | ||
| Total | 138 (34.16) | 266 (65.84) | ||
* Statistically significant (p<0.05)
When asked whether they knew MERS could lead to death, 270 patients (66.83%) said they were aware of it [Table/Fig-6]. Saudi citizens (79.17%) were more likely to know this compared to non-Saudis (55.66%). There was significant difference in the response within different age group and education level.
[Table/Fig-6]:
Response of the patients when asked whether they knew MERS could lead to death.
| Factors | Yes (%) | No (%) | Chi-square | p-value |
|---|---|---|---|---|
| Sex | ||||
| Male | 172 (64.18) | 96 (35.82) | 2.527 | 0.1124 |
| Female | 98(83.82) | 38 (16.18) | ||
| Citizen | ||||
| Saudi | 152 (79.17) | 40 (20.83) | 25.114 | 0.0001* |
| Non-Saudi | 118(55.66) | 94(44.34) | ||
| Age group | ||||
| <25 | 98 (74.24) | 34 (25.76) | 19.806 | 0.0001* |
| 25-50 | 142 (69.61) | 62 (30.39) | ||
| >50 | 30(44.11) | 38 (55.88) | ||
| Education | ||||
| Primary | 12(17.14) | 58(82.86) | 116.413 | 0.0001* |
| Secondary | 108 (65.06) | 58 (34.94) | ||
| Graduate | 150(89.29) | 18 (10.71) | ||
| Total | 270 (66.83) | 134 (33.17) | ||
* Statistically significant (p<0.05)
Three hundred and twenty four respondents (80.2%) were aware that dentists and dental assistants should wear mouth masks and protective eye glasses during treatment. The response of the patients to this question based on age, sex, nationality and education is given in [Table/Fig-7].
[Table/Fig-7]:
Response of the patients when asked whether they know that dentist and dental assistant should wear protective masks and eye goggles.
| Factors | Yes (%) | No (%) | Chi-square | p-value |
|---|---|---|---|---|
| Sex | ||||
| Male | 210 (78.35) | 58(21.65) | 1.697 | 0.1937 |
| Female | 114(83.82) | 22 (16.18) | ||
| Citizen | ||||
| Saudi | 174 (90.62) | 18 (9.38) | 25.049 | 0.0001* |
| Non-Saudi | 150(70.75) | 62(29.25) | ||
| Age group | ||||
| <25 | 116 (87.88) | 16 (12.12) | 66.775 | 0.0001* |
| 25-50 | 168 (82.35) | 36 (17.65) | ||
| >50 | 40(58.82) | 28 (41.18) | ||
| Education | ||||
| Primary | 33(47.14) | 37(52.86) | 66.775 | 0.0001* |
| Secondary | 134 (80.72) | 32 (19.28) | ||
| Graduate | 157 (93.45) | 11 (6.55) | ||
| Total | 324 (80.20) | 80 (19.80) | ||
* Statistically significant (p<0.05)
Discussion
Although research is being carried out to confirm the transmission pattern of MERS-CoV, most of the cases are likely to be acquired from another infected person especially in the health care setting. A similar study was conducted previously in Hong Kong to evaluate the knowledge and attitude of dental patients towards SARS during SARS outbreak [12]. Kharma et al., carried out a study, where they tried to assess the knowledge of dental students towards MERS [13]. To the best of our knowledge, this is the first time a survey has been conducted to assess the awareness and apprehension of dental patients towards MERS.
It is highly encouraging that majority of the subjects (84.16%) who participated in this survey had heard about MERS before. Awareness about MERS was more among females compared to males. According to 2010 population census, Riyadh has a population of nearly 5 million, of which Saudi citizens accounted for 65%of population and remaining 35% were non-Saudis [14]. It has to be noted that awareness among non-Saudis (74.53%) was less compared to Saudi citizens (94.79%). This could be because of less proficiency of non-Saudis in Arabic and English which is the commonly used medium of communication in media and notifications. Younger age groups (<25 and 25-50) had heard more about MERS when compared to >50 age group which could be attributed to the higher exposure of these age groups to social media and mass media. This result is similar to the study done by Yip et al., during SARS outbreak where they found a higher awareness among age group 20-30 years [12].
Latest studies provide evidence that camels are a likely primary source of MERS-CoV and genomic sequencing suggests that MERS-CoV infection is transmitted to human through close contact with infected camel [7,15–17]. It has been advised by WHO that any person who visits places where camels are there should follow hygiene measures like regular hand washing after touching animals and avoiding touching mouth, nose or eyes with hands and avoiding contact with sick animals. It has also been recommended that people who consume camel products as food should process it through cooking or pasteurization before consumption [17]. It is highly appreciable that more than half of the respondents (50.99%) were aware that camel is a source of MERS-CoV. Much like the previous questions, knowledge among Saudi citizens was much higher compared to non-Saudis. Graduates were better informed compared to primary and secondary educated subjects. In a survey done on dental students by Kharma et al., a similar proportion of respondents (48%) reported that source of MERS –CoV is camel [13].
Most probable route of transmission for acute viral respiratory tract infection like MERS are large respiratory droplets spread during coughing and sneezing or hand contamination or contact with fomite. There is a potential risk for transmission in dental office because of aerosol production during certain dental procedures, but no case has been reported so far [18,19]. Female subjects (44.11%) appeared to be more apprehensive about undergoing dental treatment procedures because of MERS than their male counterparts (16.42%), which was similar to findings given by Yip et al., [12]. In contrast, another study observed males to be more apprehensive than females for undergoing dental treatment due to cross infection fear [20]. Apprehension was more among <25 age group and graduates compared to the others in their respective groups, which could be because of better awareness in these categories.
According to WHO update given on June 2014, 299 deaths have been reported from a total of 699 laboratory confirmed cases of MERS [2]. Respiratory failure is the major complication of MERS [10]. In this study we observed that 66.83% of the cases were aware that MERS could lead to death. Again in this regard, awareness was more among Saudi citizens, <25 age group and graduates compared to others in their respective groups.
For probable or confirmed cases of MERS, infection prevention and control measures includes wearing N95 mask within 1m diameter of patient and wearing gown, gloves and eye protection. Apart from these, air borne precaution should be applied when performing aerosol generating procedures [18,21,22]. In a survey conducted in a dental college, it was found that most of the students used gloves and masks always, but the students who used protective eye wear and gowns regularly were 27% and 69% respectively [23]. Patients when asked whether they were aware that dentists should wear surgical masks, gloves, gowns and eye protection during treatment, 324 (80.20%) patients responded positively whereas 80 patients (19.80%) were ignorant of the infection control measures. Awareness of the patients in this regard was comparatively higher when compared to a questionnaire conducted in Glasgow in 1990, where only 60% of the respondents were aware of infection control measures [24]. A significant positive response was seen among Saudi citizens, <25 age group and graduates in their groups respectively.
One hundred and thirty eight respondents claimed they took some kind of protection in dental college because of MERS. This was an open ended question and on asking what kind of precaution they take in dental office, some patients said they wore mouth mask while others claimed they used cloth to cover their face.
To prevent transmission of respiratory infections like MERS in hospital, visual alerts should be provided in appropriate language at the entrance, clinics and waiting area of hospitals that instructs patient to inform of any respiratory illness when they register for care for the first time. Patients should be instructed to cover his/ her mouth with a tissue when coughing or sneezing, perform hand hygiene after contacting contaminated materials or respiratory secretions and dispose the used tissue in the waste receptacle. Masks should be offered to patients who are coughing and coughing persons should be encouraged to sit at least one meter away from others in waiting room. Overcrowding should be avoided as far as possible in clinical areas to prevent cross infection. Standard procedures should be followed in waste disposal and cleaning and disinfection of environmental surface and patient-care equipment [25].
Limitation
The main limitation of this study was that most of the questions included in the questionnaire were related to awareness and the apprehension of the dental patients towards MERS and there were fewer questions related to infection control measures and clinical aspect of MERS.
Conclusion
From the present study it can be concluded that most of the patients who came to the dental college were aware about MERS. A quarter of patients were apprehensive about undergoing dental treatment because of MERS, while most of them were aware of the infection control measures to be followed by the dentists. MERS is a new entity and researches are being undertaken to understand the pathology and transmission of disease. So it is quiet important for health workers to educate and update the patients regarding MERS.
Questionnaire Design
Financial or Other Competing Interests
None.
References
- [1].Zaki AM, Van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367(19):1814–20. doi: 10.1056/NEJMoa1211721. [DOI] [PubMed] [Google Scholar]
- [2]. WHO. Middle East respiratory syndrome coronavirus (MERS-CoV) summary and literature update-11 June 2014. http://www.who.int/csr/disease/coronavirus_infections/MERS-CoV_summary_update_20140611.pdf?ua=1 (accessed on July 1st 2014)
- [3]. WHO. Middle east respiratory syndrome corona virus((MERS-CoV) summary and literature update-9 May 2014. http://www.who.int/csr/disease/coronavirus_infections/MERS_CoV_Update_09_May_2014.pdf (accessed on June 3rd 2014)
- [4].Holmes KV, Lai MMC. Fields Virology. 3rd ed. Philadelphia, Pa: Lippincott-Raven Publishers; 1996. Coronaviridae. In: Fields BN et al., editors; pp. 1075–1093. [Google Scholar]
- [5].Cotton M, Watson SJ, Kellam P, Al-Rabeeah AA, Makhdoom HQ, Assiri A, et al. Transmission and evolution of the Middle East respiratory syndrome coronavirus in Saudi Arabia: a descriptive genomic study. Lancet. 2013;382(9909):1993–2002. doi: 10.1016/S0140-6736(13)61887-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].CDC. Update: severe respiratory illness associated with a novel coronavirus — worldwide, 2012-2013. MMWR Morb Mortal Wkly Rep. 2013;62(10):194–95. [PMC free article] [PubMed] [Google Scholar]
- [7].Haagmans BL, Al Dhahiry SH, Reusken CB, Raj VS, Galiano M, Myers R, et al. Middle East respiratory syndrome coronavirus in dromedary camels: an outbreak investigation. Lancet Infect Dis. 2014;14(2):140–45. doi: 10.1016/S1473-3099(13)70690-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Raj VS, Mou H, Smits SL, Dekkers DH, Muller MA, Dijkman R, et al. Dipeptidyl peptidase 4 is a functional receptor for the emerging human coronavirus-EMC. Nature. 2013;495(7440):251–54. doi: 10.1038/nature12005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Lu G, Hu Y, Wang Q, Qi J, Gao F, Li Y. Molecular basis of binding between novel human coronavirus MERS-CoV and its receptor CD26. Nature. 2013;500(7461):227–31. doi: 10.1038/nature12328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10]. WHO. Middle East respiratory syndrome coronavirus Joint Kingdom of Saudi Arabia/WHO mission Riyadh, 4-9 June 2013. http://www.who.int/csr/disease/coronavirus_infections/MERSCov_WHO_KSA_Mission_Jun13_.pdf (accessed on march 23rd 2014)
- [11]. WHO. WHO RISK ASSESSMENT. Middle East respiratory syndrome coronavirus (MERS-CoV). 24 April 2014. http://www.who.int/csr/disease/coronavirus_infections/MERS_CoV_RA_20140424.pdf (accessed on may 20th 2014)
- [12].Yip HK, Tsang PCS, Samaranayake LP, Li HP. Knowledge of and attitudes toward severe acute respiratory syndrome among a cohort of dental patients in Hong Kong following a major local outbreak. Community Dental Health. 2007;24:43–48. [PubMed] [Google Scholar]
- [13].Kharma MY, Alalwani MS, Amer MF, Tarakji B, Aws G. Assessment of the awareness level of dental students toward Middle East Respiratory Syndrome-coronavirus. J Int Soc Prev Community Dent. 2015;5(3):163–69. doi: 10.4103/2231-0762.159951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14]. “Riyadh City”. Saudi Arabia- Ministry of Interior Riyadh Principality. http://www.riyadh.gov.sa/en/pages/riyadhcity.aspx (accessed on 11/07/2014)
- [15].Azhar EI, El-Kafrawy SA, Farraj SA, Hassan AH, Al-Saeed MS, Hashem AM, et al. Evidence for camel-to-human transmission of mers coronavirus. N Engl J Med. 2014;370(26):2499–505. doi: 10.1056/NEJMoa1401505. [DOI] [PubMed] [Google Scholar]
- [16].Holmes D. MERS-CoV enigma deepens as reported cases surge. Lancet. 2014;383(9931):1793. doi: 10.1016/S0140-6736(14)60866-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17]. WHO. Middle East respiratory syndrome: Update on MERS-CoV transmission from animals to humans, and interim recommendations for at-risk groups. http://www.who.int/csr/disease/coronavirus_infections/MERS_CoV_RA_20140613.pdf?ua=1 (accessed on July 5th 2014)
- [18].Zumla A, Hui DS. Infection control and MERS-CoV in health-care workers. Lancet. 2014;383(9932):1869–71. doi: 10.1016/S0140-6736(14)60852-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Seto WH, Conly JM, Pessoa-Silva CL, Malik M, Eremin S. Infection prevention and control measures for acute respiratory infections in healthcare settings: an update. East Mediterr Health J. 2013;19(suppl 1):S39–47. [PubMed] [Google Scholar]
- [20].Porter SR, Peake G, Scully C, Samaranayake LP. Attitudes to cross-infection measures of UK and Hong Kong patients. Br Dent J. 1993;175:254–57. doi: 10.1038/sj.bdj.4808292. [DOI] [PubMed] [Google Scholar]
- [21]. Siegel JD, Rhinehart E, Jackson M, Chiarello L, the Healthcare Infection Control Practices Advisory Committee. 2007 guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings. 2007. http://www.cdc.gov/hicpac/2007IP/2007isolationPrecautions.html (accessed May 18, 2014)
- [22]. CDC. Interim infection prevention and control recommendations for hospitalized patients with Middle East respiratory syndrome coronavirus (MERS-CoV). May 15, 2014. http://www.cdc.gov/coronavirus/mers/infection-prevention-control.html (accessed july 18th, 2014)
- [23].Rahman B, Abraham SB, Alsalami AM, Alkhaja FE, Najem SI. Attitudes and practices of infection control among senior dental students at college of dentistry, university of Sharjah in the United Arab Emirates. Eur J Dent. 2013;7(Suppl 1):S15–19. doi: 10.4103/1305-7456.119058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Samaranayake LP, McDonald KC. Patient perception of cross-infection prevention in dentistry. Oral surg Oral med Oral Pathol. 1990;69(4):457–60. doi: 10.1016/0030-4220(90)90379-7. [DOI] [PubMed] [Google Scholar]
- [25]. Ministry of health, Kingdom of Saudi Arabia. Infection prevention and control guidelines for Middle East Respiratory Syndrome corona virus (MERS-CoV) infection. http://www.moh.gov.sa/Documents/2015 update.pdf (accessed on Jan 4th 2016)