

Abstract
Background:
Lack of attention to the proper barcode using leads to lack of use or misuse in the hospitals. The present research aimed to investigate the requirements and barrier for using barcode technology and presenting suggestions to use it.
Methods:
The research is observational-descriptive. The data was collected using the designed checklist which its validity was assessed. This check list consists of two parts: “Requirements” and “barrier” of using the barcodes. Research community included 10 teaching hospitals and a class of 65 participants included people in the hospitals. The collected data was analyzed using descriptive statistics.
Results:
Required changes of workflow processes in the hospital and compliance them with the hospital policy are such requirements that had been infringed in the 90 % of hospitals. Prioritization of some hospital processes for barcoding, system integration with Hospital Information system (HIS), training of staff and budgeting are requirements for the successful implementation which had been infringed in the 80% of hospitals. Dissatisfaction with the quality of barcode labels and lacks of adequate scanners both whit the rate of 100 %, and the lack of understanding of the necessary requirements for implementation of barcodes as 80% were the most important barrier.
Conclusion:
Integrate bar code system with clinical workflow should be considered. Lack of knowledge and understanding toward the infrastructure, inadequate staff training and technologic problems are considered as the greatest barriers.
Keywords: Barcode, Hospital, Process, Recommendation, Use
1. INTRODUCTION
Medical Errors are one the major concerns of on-site health care (1). These errors can reduce with the automatic identification technologies such as barcode (2, 3). Barcode technology can prevent medical errors by providing detailed and reliable information in the site of patient care (4, 5).
Barcodes usually don’t include descriptive data; however they are the reference numbers which computers use them in order to search a record containing descriptive data and other important related information (6, 7). Although the bar code is one of the most powerful and the most economical methods of improving the patient safety, while many health care organizations do not tend to apply the bar code system due to lack of proper understanding through the technology and its system requirements (8). Effective and successful implementation of bar code technology depends on the various issues including financial planning, organizational readiness, required changes for the workflow of health care providers, and also existing information technology infrastructure. Therefore although barcoding in hospitals can help avoid the cost of medical errors, however barcode establishment should be based on the principals in order to achieve this purpose (6). Considering the importance of effective using the bar codes and removing the barrier of using this technology, this study aimed to examine the requirements and barriers for using the barcode technology in hospitals. Finally some practical suggestions have been presented in order to improve the problems.
2. PATIENTS AND METHODS
This is an observational and descriptive study which has been performed in 10 teaching hospitals, affiliated with medical Tabriz University of Medical Sciences. The primary checklist was designed by the researchers in order to collect data by studying scientific sources (3, 6, 8-14) and regarding to three factors including: organization, technology, and budget. Check list consists of two parts: “Requirements” and “barrier” of using the barcodes. The research was validated according to the opinions of the knowledgeable experts toward the subject. For this purpose validity assessment form of quantitate content was prepared where each component of the check list were assessed using three criteria including: “The relevance of the question”, “clearance of question” and “simplicity of question” based on the four-part Likert scale including quite relevant, relevant, fairly relevant, and irrelevant for CVI (content validity index) and criterion of “question requirement” for CVR (content validity Rate). Experts community was composed of 10 people including nursing, health Information management, medical informatics, health services management and medical records education).
The results of CVR value were greater than the number of Lawshe table for all components (0. 62). In the other words, all experts were agreed with necessity of all questions in the check list. CVI was obtained as 0.9 with the calculation formula.
The final tool was set in the form of two check lists including the requirements with 26 components and barrier with 13 components. Data was collected by the researcher and using the observational method and questioning of staff in the studied hospitals. The selection basis of personnel was relevance of their duties to the most important processes of hospitals requiring the use of barcode. Therefore medical record, IT pharmacy, quality improvement, drug store departments and the head of the laboratory in every hospital were selected to complete the check list.
In total 65 people participated including 34 directors of the mentioned departments and 31 experts and other staff for data gathering. The collected data was analyzed using descriptive statistics methods in the form of frequency tables.
3. RESULTS
According to Table 1, 90 % of assessed hospitals didn’t evaluate the required changes in the workflow processes of hospital. The required changes for using the bar code wristband in the patient identification can be presented to the nurses and physicians by documented flow charts and can inform them, but none of the hospitals were used these flowcharts.
Table 1.
Requirements and essentials for use of barcode technology in hospitals
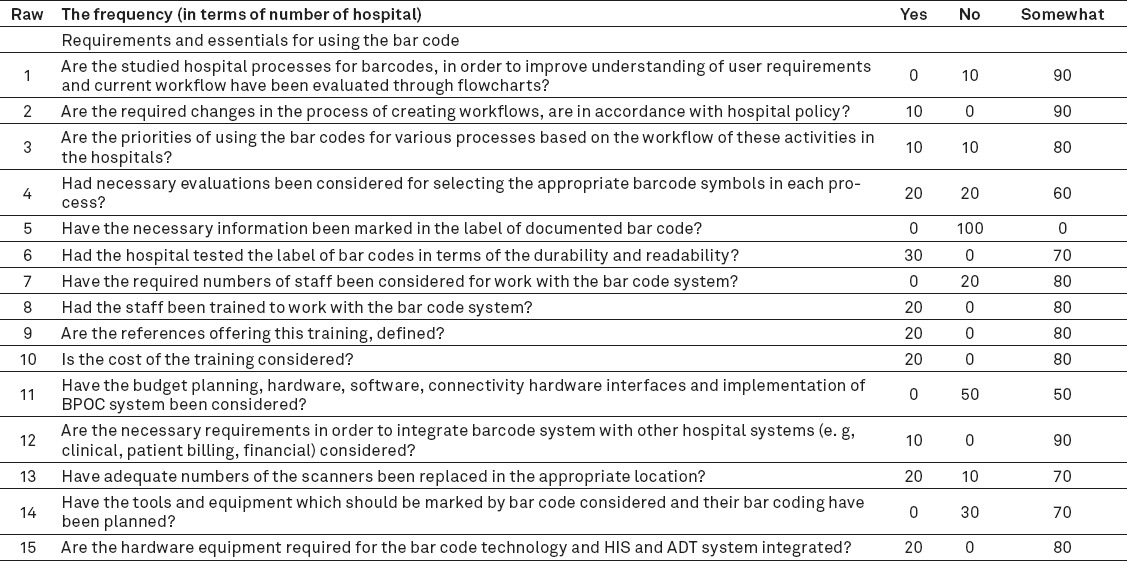
Additionally according to Table 1, although the property of the barcode symbols were evaluated in 40 % of hospitals, however there was no knowledge of international standards for barcodes including the GS1 (Global Language of Business) and HIBCC (Health Industry Business Communications Council) in order to use them in the development of bar code system in none of the hospitals. The content of the patient bar code wristband had been defined, while the content of label lab specimens was incomplete due to the opinions of employees and some informative items should be added. Only 20 % of hospitals considered the issues related to staffing for working with the bar codes such as the cost and training.
Barrier of using the bar codes
The barriers for using the bar codes were studied in two aspects. First, the barriers which hospitals may deal with prior to the implementation of bar codes; and the second, the difficulties and barriers that could have arisen after the adoption of bar codes and can stop using them. According to Figure 1, 50 % of studied hospitals had not the using of bar code policy. However although in the other 50% of hospitals, there was the use of barcode policy, but neglect, poor attention, and also the absence or weakness of identified and detailed planning in the process of implementing prevents its application. In the 80% of the studied hospitals, there was not understanding of the requirements for implementation.
Figure 1.
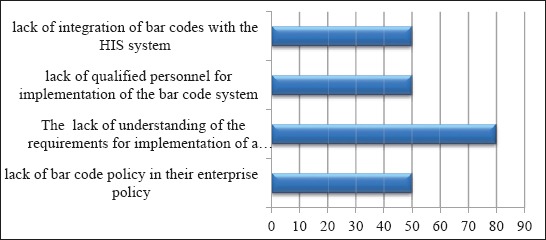
Barriers in the studied hospitals, before the implementation of bar code
According to the opinions of technical staff in the hospital, since the implementation of the bar code system does not need the sophisticated technologies and its cost is less compared to other similar technologies and the other hospital costs, then the majority of hospitals (90 percent) had no budget problems to implement. Additionally the lack of knowledge of staff towards the benefits of bar code is one of the most obvious causes for the negligence in the use of a bar code. AThe problems related to lack of adequate bar code scanners, inadequate bar code equipment, low quality of bar code labels, and weakness of policy establishing by the authorities are only studied in the hospitals which they used bar codes in at least one of their hospital processes and it was only observed in five hospitals. Among these problems, dissatisfaction was observed due to the inadequate numbers of scanners and the poor quality of bar code labels in all five hospitals (100%).
Noteworthy 70% of participants believed that lack or weakness of policy establishing by the authorities along with the neglect of the hospital management prevent the planning for application of the bar codes. Additionally 80 percent of them stated that lack of knowledge towards the concept and importance of using bar codes cause to negligence of applying this technology. They were dissatisfied due to the problems of the bar code label including its information content, failure to compliance in the patient identification code with the code on the bar code content, and illegible barcode labels.
4. DISCUSSION
Nowadays, the advantages of applying the technology of automatic identification including bar codes have been established for improvement of patient safety. However, the success of this technology projects depends on the knowledge of a comprehensive planning for the management of the requirements, risks and, barriers for its implementation (10).
Justification of organization managers to accept and apply the policies of this technology, allocation of priorities, and monitoring its application are the most important steps for the successful implementation of IT in the organization (6). The results of the research suggests that bar code application policy has not been considered in the organizational policy establishment while sufficient priorities have not been allocated for implementation of these policies.
Another important issue for the implementation of technology is the necessity of attention to the priorities of usage processes and their redesign (6, 10). The results showed that although some processes with more requirements to the bar code have been detected in some hospitals, however no planning is found for redesigning and prioritizing these processes. Medication management process and blood sampling and laboratory processes were the processes which need the implementation of bar code system. However, prioritization of these processes for the implementation of bar code has not been considered.
In the majority of hospitals neglect to notify changes in the workflow for employees leads to lack of awareness through the use of barcodes. The results of the present study and similar studies (3, 6, 11) showed that prioritizing the processes which require using the bar codes, re-engineering the processes, and also developing a flowchart model for the new workflow and delivering it to users through the education which can play a significant role for successful implementation.
Training the staff is one of the major issues for justifying and deployment of technology in the organization (1, 6, 11, 15, 16). Training of people can increase understanding, acceptance, and proper using of the technology both to understand the benefits and usage. In this research it was shown that the staff was not been trained adequately in 80 % of hospitals, the references of training was unknown, and most importantly the sufficient cost was not allocated for the training. In the study of Chan et al. the necessity of training the staff involved in the implementation of bar code project has been considered in order to manage and enhance safety through the blood transfusion process (16). Therefore, training the end-users can facilitate acceptance of changes in the processes and leads to greater efficiency in the new processes. Well-trained users can also cooperate for elimination of errors in technology and support (16). Hence training the users by a competent authority is one of the most important requirements for implementing the bar code and integrity of the system (17, 18).
Funding the technological projects play a major role in the success of these projects. Funds can be spent for mere technical or operational issues (16). Budget is essential in order to establish the necessary infrastructures, buying the equipment, support, and staff training (19). In the present study, budgetary problems are clearly examined. In the studies by Ilie-Zudor and colleagues (12) and García and Huerta (20) the cost of using bar codes was strongly emphasized. Therefore, allocate adequate funding for the bar code projects can provide necessary hardware and software platforms for proper functioning of the bar code, equipment, and also support and training the staff, effectively.
Cultural barriers are another reason for the failure of bar code technology. Dzik and colleagues found that lack of culture for the use of bar code technology by physicians and nurses was due to the lack of techniques for the audit information on medication and blood, misunderstanding of the logic of using this technology, tendency to ignore the severity and frequency of errors, inhuman realizing the use of this technology for patient care, and weakness in the designing have been mentioned as the main barriers for success implementation of the bar code in the hospitals (21). Despite the results of the Deziks research, in the present research it was found that although there were requirement announcements in the various official departments, however neglect and mismanagement in the prioritization of and planning the budgets for the barcode technology leads to block the next steps for the implementation. Also the results revealed that not only there is no cultural problem for using the bar code, but also employees who were aware of the benefits of bar code, showed a great desire.
Another important factor in the bar code projects were the selection of bar code equipment types including type of labels, scanners, required networks for successful implementation and other hardware and software (6, 7). Selection of the bar code type, appropriate to content and the processes along with the selection of the appropriate scanner seems very important. The study of Zudor and colleagues (12) revealed that agreement on a common identification system is the most basic type of requirements which should be eliminated before the implementation of automatic identification systems. In this research “Label reliability” is also mentioned as one of the issues that should be considered in the exchange of information. For example, the content of the documented information on the bar code labels of drugs in the management process for the medication bar code is different with the information content of bar code label of tubes and the blood samples which leads to select a different bar code symbol. Snyder and colleagues stated the possibility of a mistaken identification of the patient by the bar code which may be minimized by carefully controlling the characteristics of scanning equipment and printing the bar codes (22). We showed that the problems related to lack of adequate bar code scanners in terms of ergonomics, scanners, weight, size, speed, and the problems related to low quality of bar code labels were considered due to the illegibility and low durability.
Another important barriers in the usage of bar code, is the inefficient software numbers of hospital information system (HIS) (8). In this research it was proved that the integration of bar code system and HIS was not considered in 80 % of hospitals. The lack of integration does not causes employed bar code system can completely show its potential in the potentials. Therefore inability of the HIS software related to the bar code system causes bar code system fails access to the patient information.
5. CONCLUSION
We concluded that lack of knowledge and understanding toward the infrastructure, required equipment, and support is the most important problem of the technology issues. Inadequate staff training and allocation of funds for training and purchasing equipment are important issues of education and the cost class, which are considered as the greatest barriers of the successful implementation of bar code system.
Recommendations
Establishing any policy for changing the process of medication management requires direct notification from the relevant ministry due to the direct supervision of medical and treatment health ministry deputy.
Explaining the importance of bar codes and return of the investment or the costs of this technology for managers and heads of hospitals may be effective for prioritization of the using this technology.
Change the workflow must be carefully evaluated. It is suggested that readiness to integrate bar code system with clinical workflow should be considered. In this regard, documentation of workflow changes is affected by applying the bar codes while its notification to the hospital staff can increase acceptance and security of the hospital staff for using the bar codes.
It is noted that all clinical staff who deal with the bar code should be prepared for its implementation. Teaching the staff is necessary to be performed at an acceptable and applicable level. As well as it is recommended that it is necessary the bar code system should be primarily performed trial and in a much smaller area such as in a specific clinical department before using in the all hospital processes.
The ease of access to the needed equipment is one of the most important factors in order to increase the use of bar codes. Experienced sellers should be prioritized and long-term collaboration and communication should be considered for the seller.
It is recommended that the unit content and format should be agreed for bar code labels between the blood transfusion organization and hospital blood banks.
It can be expressed that development of policies and guidelines for top position managers and directors, the allocation of sufficient funds by managers, create new changes in the hospital processes in order to implement bar code, and staff training in practice are some of the requirements for the successful implementation of bar code system.
Finally, it is suggested that capabilities should be considered during the development or buying Hospital Information System software. A process should be defined in order to respond the software and hardware problems so that it has ability to respond quickly to the imperfections of the system when system is applied.
Acknowledgments
This study as MS thesis was supported and funded by School of Health Management and Medical Informatics of Tabriz University of Medical Sciences (NO: 5/9/948).
Footnotes
• Author’s contribution: Leila Zyaei: substantial contribution to acquisition of data, substantial contribution to analysis and interpretation of data. All authors were included in other phases of preparing this article including contribution to conception, design and final proof reading.
• Conflict of interest: There is no conflict of interest of any of listed authors.
REFERENCES
- 1.Nichols J, Bartholomew C, Brunton M, Cintron C, Elliott S, McGirr J, et al. Reducing medical errors through barcoding at the point of care. Clinical leadership & management review:the journal of CLMA. 2003;18(6):328–34. [PubMed] [Google Scholar]
- 2.Sheppard I, Hyland S, Koczmara C. Medication Bar Code System Implementation Planning A Resource Guide. ISMP Canada. 2008 [Google Scholar]
- 3.Nanji KC, Cina J, Patel N, Churchill W, Gandhi TK, Poon EG. Overcoming barriers to the implementation of a pharmacy barcode scanning system for medication dispensing:a case study. Journal of the American Medical Informatics Association. 2009;16(5):645–50. doi: 10.1197/jamia.M3107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Astion M. Right patient, wrong sample. Agency for Healthcare Research and Quality Case and Commentary. 2006. http://www.webmm ahrq gov/case.aspx .
- 5.Ball MJ, Douglas JV. Hospital information systems (HIS):looking into the future. Proceedings of the Annual Symposium on Computer Application in Medical Care. American Medical Informatics Association. 1991 [PMC free article] [PubMed] [Google Scholar]
- 6.Lewis RF, Simpson N. Implementation guide for the use of barcode technology in healthcare. Healthcare Information and Management Systems Society Conference. 2003 [Google Scholar]
- 7.Bix L, Clarke R. From Information Silo to Bridge, Part 2:Creating a UDI System. Medical Device and Diagnostic Industry. 2007;29(11):62–71. [Google Scholar]
- 8.Hills v. Issues and Opportunities for Introducing Bar Code Systems in Hospitals. ZIH Corp. 2006 [Google Scholar]
- 9.GS1 Canada. Bar Code Scanning Equipment Selection Criteria:A guide to choosing appropriate scanning equipment. 2010 [Google Scholar]
- 10.McKesson Corporation. Operational Recommendations to Support Barcode Scanning Effectiveness across the Medication Use System. 2012 [Google Scholar]
- 11.Henriksen K, Battles JB, Marks ES, Lewin DI, Wideman MV, Whittler ME, et al. Barcode medication administration:Lessons learned from an intensive care unit implementation. 2005 [PubMed] [Google Scholar]
- 12.Ilie-Zudor E, Kemény Z, van Blommestein F, Monostori L, van der Meulen A. A survey of applications and requirements of unique identification systems and RFID techniques. Computers in Industry. 2011;62(3):227–52. [Google Scholar]
- 13.Lutton E, Regan B, Skinner G. Patient identification within a healthcare system:the role of radio frequency identification and barcode technologies. Proceedings of the 11th WSEAS international conference on Mathematical methods and computational techniques in electrical engineering; 2009. World Scientific and Engineering Academy and Society (WSEAS) 2009 [Google Scholar]
- 14.GS1 Canada. Bar Code Scanning Equipment Selection Criteria:A guide to choosing appropriate scanning equipment. 2010 [Google Scholar]
- 15.Brown JE, Smith N, Sherfy BR. Decreasing mislabeled laboratory specimens using barcode technology and bedside printers. Journal of nursing care quality. 2011;26(1):13–21. doi: 10.1097/NCQ.0b013e3181e4e6dd. [DOI] [PubMed] [Google Scholar]
- 16.Chan L, Greeley W, Klingen D, Machado B, Padula M, Sum J, et al. Barcode Medication Administration Implementation in the FIAT Health System. Transforming Health Care Through Information:Case Studies:Springer. 2010:85–96. [Google Scholar]
- 17.Ohsaka A, Kobayashi M, Abe K. Causes of failure of a barcode based pretransfusion check at the bedside:experience in a university hospital. Transfusion Medicine. 2008;18(4):216–22. doi: 10.1111/j.1365-3148.2008.00868.x. [DOI] [PubMed] [Google Scholar]
- 18.Nolen AL, Rodes WD. Barcode medication administration system for anesthetics:effects on documentation and billing. American Journal of Health-System Pharmacy. 2008;65(7):655–9. doi: 10.2146/ajhp070167. [DOI] [PubMed] [Google Scholar]
- 19.Turner C, Casbard A, Murphy M. Barcode technology:its role in increasing the safety of blood transfusion. Transfusion. 2003;43(9):1200–9. doi: 10.1046/j.1537-2995.2003.00428.x. [DOI] [PubMed] [Google Scholar]
- 20.García-Betances RI, Huerta MK. A review of automatic patient identification options for public health care centers with restricted budgets. Online journal of public health informatics. 2012;4(1) doi: 10.5210/ojphi.v4i1.4011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dzik WH. New technology for transfusion safety. British Journal of Haematology. 2007;136(2):181–90. doi: 10.1111/j.1365-2141.2006.06373.x. [DOI] [PubMed] [Google Scholar]
- 22.Snyder ML, Carter A, Jenkins K, Fantz CR. Patient misidentifications caused by errors in standard barcode technology. Clinical chemistry. 2010;56(10):1554–60. doi: 10.1373/clinchem.2010.150094. [DOI] [PubMed] [Google Scholar]