

Abstract
Objective
This study estimates the numbers of new cancer cases and cancer deaths in Hebei province using incidence and mortality data from 9 population-based cancer registries in 2012.
Methods
The data of new diagnosed cancer cases and cancer deaths in 2012 were collected from 9 population-based cancer registries of Hebei province in 2015. All the data met the National Central Cancer Registry of China (NCCR) criteria of data quality. The pooled data analysis was stratified by areas (urban/rural), gender, age group (0, 1.4, 5.9, 10.14, …, 85+) and cancer type. New cancer cases and deaths in Hebei province were estimated using age-specific rates and corresponding provincial population in 2012. The 10 most common cancers in different groups and the cumulative rates were calculated. Chinese population census in 2000 and Segi’s population were used for age-standardized incidence/mortality rates.
Results
All cancer registries covered 4,986,847 populations, 6.84% of Hebei provincial population (2,098,547 in urban and 2,888,300 in rural areas). The percentage of cases morphologically verified (MV%) and death certificate-only cases (DCO%) were 76.40% and 4.72%, respectively. The mortality to incidence rate ratio (M/I) was 0.64. In 2012, it is estimated that there were about 187,900 new diagnosed cancer cases and 119,800 cancer deaths in Hebei province. The incidence rate of cancer was 258.12/100,000 (275.75/100,000 in males, 239.78/100,000 in females), and the age-standardized incidence rates by Chinese standard population (ASIRC) and by world standard population (ASIRW) were 210.65/100,000 and 208.50/100,000, with the cumulative incidence rates (0.74 years old) of 24.46%. The cancer incidence and ASIRC were 256.99/100,000 and 211.32/100,000 in urban areas and 258.94/100,000 and 209.99/100,000 in rural areas, respectively. The cancer mortality rate was 164.63/100,000 (201.85/100,000 in males, 125.92/100,000 in females). Agestandardized mortality rates by Chinese standard population (ASMRC) and by world standard population (ASMRW) were 137.30/100,000 and 137.39/100,000 with the cumulative mortality rate (0.74 years old) of 14.58%, respectively. The cancer mortality rate in rural areas (167.16/100,000) was higher than that in urban areas (161.16/100,000). The most common cancers were lung cancer, stomach cancer, breast cancer, esophageal cancer, liver cancer and colorectal cancer, which accounted for 72.31% of all cancer cases. Lung cancer, stomach cancer, liver cancer, esophageal cancer and colorectal cancer were the major causes of cancer death in Hebei province, which accounted for 75.24% of all cancer deaths. The cancer spectrum differs between urban and rural, males and females in both incidence and mortality rates.
Conclusions
The most common cancers were lung cancer, stomach cancer, esophageal cancer, breast cancer, liver cancer and colorectal cancer in Hebei province.
Keywords: Cancer registry, cancer, incidence, mortality, Hebei province
Introduction
Cancer is a major non-communicable disease, which is a serious threat to human health. It’s important to monitor incidence, mortality and time trends of cancer. The data of cancer registries could provide the basic information for cancerprevention, control and clinical research. Hebei provinceis located in the north of China with approximately 6% of whole national population, and is known as a high-risk area foresophageal cancer in China and worldwide. Hebei Provincial Cancer Registry Center is in charge of population-based cancer registries with the responsibility of data collection, evaluationand publication in Hebei province. A total of 9 population-based cancer registries in Hebei province submitted thecancer data of 2012, which were checked and analyzed in ways described below, to Hebei Provincial Cancer Registry Center.
Material and methods
Data source
Hebei Provincial Cancer Registry Center is a department of Hebei Provincial Cancer Center. By June 1,2015, there were 9 population-based cancer registries submitted the cancer data of 2012, including 3 cities (Baoding, Qinhuangdao and Cangzhou) and 6 counties (Cixian, Shexian, Qianxi, Wuan, Zanhuang and Fengning), covering 4,986,847 (2,542,514 in males, 2,444,333 in females) population and accounting for 6.84% of Hebei provincial population. The cancer data which were reported to cancer registries were from local hospitals, community health service centers, the Basic Medical Insurances for Urban Residents, the New-Rural Cooperative Medical System and the Death Surveillance. All cancer cases were classified by the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) and the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10).
Quality control
Hebei Provincial Cancer Registry Center checked and evaluated the quality and comparability of submitted data based on "Guideline for Chinese Cancer Registration" and "Cancer Incidence in Five Continents Volume IX" by International Agency for Research on Cancer/International Association of Cancer Registration (IARC/IACR) (1). The data of 9 cancer registries included in the final analysis should meet the following criteria: the percentage of cases morphologically verified (MV%) was not lower than 66%; the percentage of death certificate-only cases (DCO %) was lower than 15%; the mortality to incidence ratio (M/I) was between 0.6 and 0.8; and the percentage of the diagnosis of unknown basis (UB %) was lower than 5%.
Hebei provincial population estimates
The population of Hebei province in 2012 was estimated based on the fifth National Census data (2000) which was provided by the Statistics Bureau of Hebei province, taking into account of the changes of age composition, gender ratio and the proportion of urban and rural transformation released by the Bureau of Statistics of Hebei province (<a href="http://www.hetj.gov. cn/">http://www.hetj.gov. cn/</a>). The population of Hebei province in 2012 was stratified by area (urban/rural), gender (male/female) and age groups (0-,1-4,5-84 by 5 years, 85+ years). The age-specific death probability was adjusted by the Sixth National Census in 2010. Linear changes were assumed in each age group between the fifth and sixth population census.
Statistical analysis
Incidence and mortality rates were calculated by area, gender and age groups. The numbers of new cases and deaths were estimated using the 5-year age-specific cancer incidence/ mortality rates. The Chinese population in 2000 and World Segi’s population were used for age-standardized rates. Software including MS-Excel and IARCcrg Tools 2.05 issued by IARC and IACR was used for data checking and evaluation (2). SAS software (Version 9.3, SAS Institute Inc., Cary, USA) was used to calculate the incidence and mortality rates. New cancer cases and cancer deaths in Hebei province were estimated using age-specific rates and corresponding provincial population in 2012. The data could reflect cancer burden of Hebei province to a certain degree, even though the population covered is not large enough.
Results
Data quality
There were 9 population-based cancer registries accepted by this analysis. The overall indicators of MV%, DCO% and M/I ratio were 76.40%,4.72% and 0.64, respectively. They were 76.38%,6.88% and 0.63 in urban registries, and 76.44%,3.17% and 0.65 in rural registries. The quality evaluation for major cancers is presented in Table 1.
1.
Quality evaluation of cancer registration data in Hebei province, 2012
| Site | All areas | Urban | Rural | ||||||||
| M/I | MV% | DCO% | M/I | MV% | DCO% | M/I | MV% | DCO% | |||
| MV%, percentage of morphological verification; DCO%, percentage of cancer cases identified with death certification only; M/I, mortality to incidence rate ratio; CNS, central nervous system. | |||||||||||
| Oral & pharyngx | 0.38 | 87.66 | 1.30 | 0.41 | 90.80 | 1.15 | 0.34 | 83.58 | 1.49 | ||
| Nasopharynx | 0.48 | 90.38 | 0.00 | 0.64 | 92.86 | 0.00 | 0.29 | 87.50 | 0.00 | ||
| Esophagus | 0.72 | 84.44 | 2.21 | 0.77 | 84.98 | 9.39 | 0.71 | 84.36 | 1.13 | ||
| Stomach | 0.72 | 80.02 | 2.91 | 0.81 | 82.60 | 9.87 | 0.70 | 79.52 | 1.59 | ||
| Colorectum | 0.50 | 86.49 | 4.65 | 0.57 | 89.20 | 5.40 | 0.43 | 83.49 | 3.83 | ||
| Liver | 0.86 | 43.49 | 11.19 | 0.80 | 40.26 | 15.32 | 0.92 | 46.03 | 7.93 | ||
| Gallbladder | 0.76 | 52.75 | 17.58 | 0.85 | 44.23 | 26.92 | 0.64 | 64.10 | 5.13 | ||
| Pancreas | 1.06 | 41.40 | 15.05 | 1.15 | 34.86 | 16.51 | 0.95 | 50.65 | 12.99 | ||
| Throat | 0.66 | 77.27 | 5.68 | 0.59 | 73.91 | 8.70 | 0.74 | 80.95 | 2.38 | ||
| Lung | 0.80 | 64.34 | 7.50 | 0.82 | 62.42 | 9.29 | 0.78 | 66.49 | 5.48 | ||
| Other organs in chest | 0.18 | 75.76 | 3.03 | 0.38 | 87.50 | 0.00 | 0.00 | 64.71 | 5.88 | ||
| Bone | 0.67 | 70.10 | 5.15 | 0.75 | 69.44 | 5.56 | 0.62 | 70.49 | 4.92 | ||
| Skin melanoma | 0.75 | 75.00 | 16.67 | 0.60 | 80.00 | 20.00 | 1.50 | 50.00 | 0.00 | ||
| Breast | 0.21 | 93.80 | 1.62 | 0.20 | 96.31 | 0.89 | 0.23 | 89.22 | 2.96 | ||
| Cervix | 0.30 | 92.78 | 1.29 | 0.26 | 93.26 | 0.56 | 0.33 | 92.38 | 1.90 | ||
| Uterus | 0.29 | 92.21 | 4.33 | 0.14 | 96.67 | 2.50 | 0.44 | 87.39 | 6.31 | ||
| Ovary | 0.25 | 92.62 | 0.82 | 0.35 | 92.25 | 1.55 | 0.14 | 93.04 | 0.00 | ||
| Prostate | 0.44 | 78.63 | 3.42 | 0.42 | 81.93 | 2.41 | 0.50 | 70.59 | 5.88 | ||
| Testis | 0.22 | 100.00 | 0.00 | 0.25 | 100.00 | 0.00 | 0.20 | 100.00 | 0.00 | ||
| Kidney | 0.39 | 80.98 | 3.80 | 0.38 | 84.62 | 3.08 | 0.41 | 72.22 | 5.56 | ||
| Bladder | 0.32 | 79.52 | 3.33 | 0.28 | 82.09 | 3.73 | 0.39 | 75.00 | 2.63 | ||
| Brain, CNS | 0.64 | 60.06 | 7.03 | 0.68 | 63.38 | 9.86 | 0.60 | 57.31 | 4.68 | ||
| Thyroid gland | 0.10 | 96.38 | 1.09 | 0.11 | 96.05 | 1.32 | 0.08 | 96.77 | 0.81 | ||
| Lymphoma | 0.58 | 93.90 | 2.44 | 0.65 | 95.19 | 1.92 | 0.45 | 91.67 | 3.33 | ||
| Leukemia | 0.88 | 94.70 | 2.65 | 0.84 | 96.23 | 3.14 | 0.93 | 92.38 | 1.90 | ||
| Other cancers | 0.97 | 69.31 | 5.20 | 1.25 | 71.00 | 6.49 | 0.60 | 67.05 | 3.47 | ||
| Total | 0.64 | 76.40 | 4.72 | 0.63 | 76.38 | 6.88 | 0.65 | 76.44 | 3.17 | ||
Incidence and mortality of overall cancers
Incidence
It was estimated that 187,900 new cancer cases (101,100 in males and 86,800 in females) were diagnosed in Hebei province in 2012. The crude incidence rate of all cancers was 258.12/100,000 (275.75/100,000 in males and 239.78/100,000 in females). The age-standardized incidence rates by Chinese standard population (ASIRC) and by world standard population (ASIRW) were 210.65/100,000 and 208.50/100,000, respectively. The cumulative incidence rate (0-74 years old) was 24.46%. The crude incidence rate (256.99/100,000) and the ASIRW (208.39/100,000) in urban areas were almost the same as that (258.94/100,000 and 208.50/100,000) in rural areas. The crude incidence rate for females in urban areas was higher than that in rural areas, while the incidence rate of males in urban areas was lower than that in rural areas (Table 2).
2.
Cancer incidence in Hebei province, 2012
| Areas | Sex | Cases (thousand) | Crude incidence(1/105) | ASIRC*(1/105) | ASIRW**(1/105) | Cumulativerate 0−64 (%) | Cumulativerate 0−74 (%) | TASR***(1/105) |
| Both | 187.9 | 258.12 | 210.65 | 208.50 | 12.46 | 24.46 | 350.13 | |
| *, age-standardized incidence rate (China standard population, 2000); **, age-standardized incidence rate (World standard population); ***, truncated age-standardized rate (World standard population). | ||||||||
| All areas | Male | 101.1 | 275.75 | 232.65 | 233.85 | 13.10 | 27.71 | 363.25 |
| Female | 86.8 | 239.78 | 191.81 | 186.34 | 11.89 | 21.36 | 338.74 | |
| Both | 87.6 | 256.99 | 211.32 | 208.39 | 11.67 | 24.19 | 328.93 | |
| Urban | Male | 43.9 | 254.09 | 219.10 | 219.98 | 10.87 | 24.98 | 299.87 |
| Female | 43.7 | 259.93 | 207.84 | 201.56 | 12.52 | 23.56 | 359.72 | |
| Both | 100.3 | 258.94 | 209.99 | 208.50 | 13.02 | 24.63 | 364.89 | |
| Rural | Male | 57.2 | 291.17 | 241.90 | 243.26 | 14.67 | 29.62 | 408.19 |
| Female | 43.1 | 224.83 | 179.97 | 175.35 | 11.41 | 19.73 | 322.51 | |
Age-specific incidence rate
The age-specific incidence rate was relatively lower before 40 years old, then increased dramatically and peaked at age group of 85+ years. The pattern was similar between urban and rural areas, except that the age-specific incidence rate peaked at the age of 75 years for the males in rural areas and females in urban areas. Compared the age-specific incidence rate between urban and rural areas, except for age from 45-74 years old, urban areas had higher incidence rate than that in rural areas. Most age groups of females in urban areas had higher incidence rate than that in rural areas. (Figure 1, Table 3).
1.
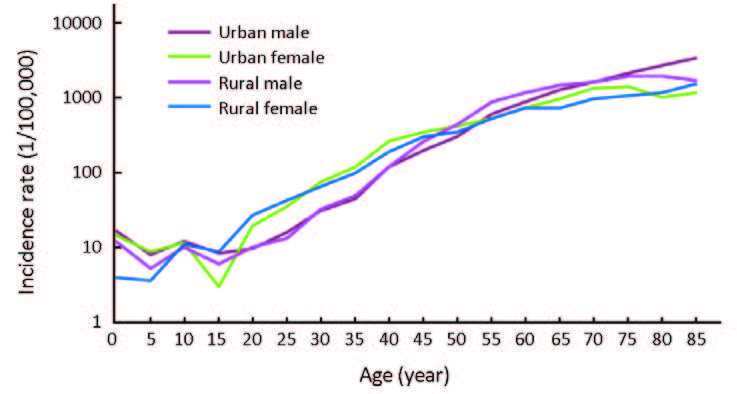
Age-specific cancer incidence rates in urban and rural areas, 2012.
3.
Age-specific incidence rates of overall cancers in Hebei province, 2012 (1/105)
| Age groups | All areas | Urban | Rural | ||||||||
| Both | Male | Female | Both | Male | Female | Both | Male | Female | |||
| Total | 258.12 | 275.75 | 239.78 | 256.99 | 254.09 | 259.93 | 258.94 | 291.17 | 224.83 | ||
| 0− | 7.94 | 8.94 | 6.80 | 19.39 | 18.29 | 20.63 | 2.36 | 4.42 | 0.00 | ||
| 1− | 11.07 | 14.33 | 7.36 | 14.52 | 16.00 | 12.87 | 9.48 | 13.57 | 4.79 | ||
| 5− | 5.65 | 5.95 | 5.31 | 8.00 | 7.60 | 8.44 | 4.37 | 5.06 | 3.56 | ||
| 10− | 10.75 | 10.65 | 10.87 | 11.57 | 11.91 | 11.19 | 10.28 | 9.95 | 10.68 | ||
| 15− | 6.50 | 6.83 | 6.14 | 5.61 | 8.27 | 2.85 | 7.15 | 5.82 | 8.62 | ||
| 20− | 16.14 | 9.51 | 22.97 | 14.05 | 9.21 | 19.07 | 17.55 | 9.71 | 25.60 | ||
| 25− | 25.85 | 14.18 | 37.67 | 25.20 | 15.80 | 34.27 | 26.41 | 12.86 | 40.69 | ||
| 30− | 48.94 | 30.64 | 68.31 | 51.58 | 30.43 | 73.45 | 46.47 | 30.83 | 63.40 | ||
| 35− | 74.86 | 46.02 | 104.62 | 78.31 | 43.55 | 113.36 | 71.56 | 48.34 | 96.07 | ||
| 40− | 163.47 | 114.77 | 213.56 | 182.03 | 115.41 | 250.58 | 148.85 | 114.27 | 184.42 | ||
| 45− | 268.73 | 229.46 | 309.44 | 260.11 | 195.02 | 327.59 | 275.28 | 255.66 | 295.62 | ||
| 50− | 369.50 | 368.34 | 370.70 | 349.19 | 288.79 | 410.92 | 384.21 | 425.27 | 341.16 | ||
| 55− | 627.72 | 739.24 | 517.27 | 546.82 | 576.82 | 517.98 | 686.81 | 854.85 | 516.73 | ||
| 60− | 863.34 | 1,030.17 | 703.13 | 785.22 | 855.18 | 718.95 | 917.31 | 1,149.67 | 692.08 | ||
| 65− | 1,070.55 | 1,350.64 | 803.60 | 1,084.08 | 1,250.49 | 930.08 | 1,061.27 | 1,417.57 | 714.79 | ||
| 70− | 1,329.07 | 1,572.18 | 1,091.09 | 1,421.14 | 1,570.61 | 1,277.96 | 1,260.63 | 1,573.32 | 949.55 | ||
| 75− | 1,527.57 | 1,932.71 | 1,156.21 | 1,681.32 | 2,055.35 | 1,345.59 | 1,423.58 | 1,851.27 | 1,025.96 | ||
| 80− | 1,544.02 | 2,171.91 | 1,058.33 | 1,682.56 | 2,571.51 | 979.22 | 1,434.93 | 1,850.01 | 1,119.53 | ||
| 85+ | 1,720.13 | 2,320.98 | 1,333.02 | 1,962.66 | 3,260.42 | 1,144.64 | 1,528.16 | 1,594.90 | 1,484.42 | ||
Mortality
It was estimated that 119,800 (74,500 in males and 45,300 in females) patients had died from cancer in Hebei province in 2012. The crude mortality rate of all cancers was 164.63/100,000 (201.85/100,000 in males and 125.92/100,000 in females). The age-standardized mortality rates by Chinese standard population (ASMRC) and by world standard population (ASMRW) were 137.30/100,000 and 137.39/100,000, respectively. Among the deaths aged 0-74 years, the cumulative mortality rate was 14.58%. The crude cancer mortality rate (167.16/100,000) and the ASMRW (137.63/100,000) in rural areas were higher than that (161.16/100,000 and 136.36/100,000) in urban areas (Table 4).
4.
Cancer mortality in Hebei province, 2012
| Areas | Sex | Cases (thousand) | Crude incidence(1/105) | ASIRC*(1/105) | ASIRW**(1/105) | Cumulativerate 0−64 (%) | Cumulativerate 0−74 (%) | TASR***(1/105) |
| *, age-standardized mortality rate (China standard population, 2000); **, age-standardized mortality rate (World standard population); ***, truncated age-standardized rate (World standard population). | ||||||||
| Both | 119.8 | 164.63 | 137.30 | 137.39 | 6.05 | 14.58 | 166.75 | |
| All areas | Male | 74.5 | 201.85 | 177.63 | 178.32 | 7.75 | 18.82 | 214.04 |
| Female | 45.3 | 125.92 | 100.28 | 100.20 | 4.37 | 10.45 | 119.89 | |
| Both | 55.0 | 161.16 | 136.37 | 136.36 | 5.29 | 13.31 | 145.77 | |
| Urban | Male | 33.4 | 193.10 | 173.79 | 174.69 | 6.57 | 16.65 | 180.20 |
| Female | 21.6 | 128.72 | 103.64 | 103.53 | 4.05 | 10.13 | 112.39 | |
| Both | 64.8 | 167.16 | 137.58 | 137.63 | 6.59 | 15.47 | 181.41 | |
| Rural | Male | 41.1 | 208.08 | 179.42 | 179.89 | 8.57 | 20.31 | 237.57 |
| Female | 23.7 | 123.85 | 97.86 | 97.64 | 4.60 | 10.67 | 125.00 | |
Age-specific mortality rate
The age-specific mortality rate was relatively lower before 40 years and then dramatically increased, peaking at 85+ years old. The mortality rate in rural areas was higher than that in urban areas at age of 45-74 years, while the mortality rate in urban areas had higher mortality rate after 75 years old. The mortality rate in the age group of 85+ years in rural areas was the highest. In males, the age-specific mortality in urban areas was lower than that in rural areas at age group of 45-74 years. In females, the mortality in rural areas was higher than that in urban areas for age of 45-69 and 80+ years old (Figure 2, Table 5).
2.
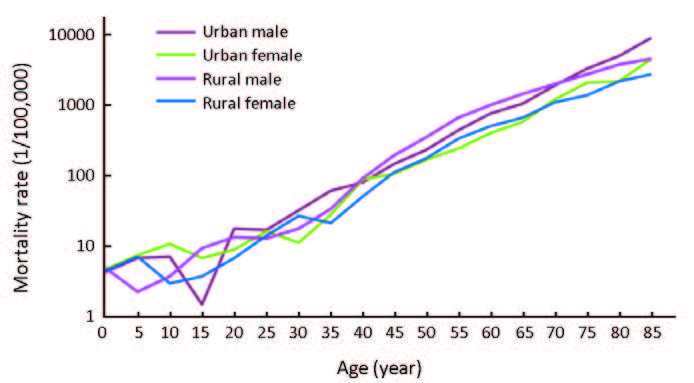
Age-specific cancer mortality rates in urban and rural areas, 2012.
5.
Age-specific mortality of overall cancers in Hebei province, 2012 (1/105)
| Age groups | All areas | Urban | Rural | ||||||||
| Both | Male | Female | Both | Male | Female | Both | Male | Female | |||
| Total | 164.63 | 201.85 | 125.92 | 161.16 | 193.10 | 128.72 | 167.16 | 208.08 | 123.85 | ||
| 0− | 3.18 | 2.98 | 3.40 | 4.85 | 9.15 | 0.00 | 2.36 | 0.00 | 5.07 | ||
| 1− | 4.20 | 4.30 | 4.09 | 3.63 | 2.29 | 5.15 | 4.46 | 5.22 | 3.59 | ||
| 5− | 4.59 | 3.30 | 6.07 | 6.00 | 5.70 | 6.33 | 3.82 | 2.03 | 5.93 | ||
| 10− | 4.61 | 4.26 | 5.02 | 7.36 | 5.95 | 8.95 | 3.02 | 3.32 | 2.67 | ||
| 15− | 4.73 | 5.13 | 4.30 | 3.51 | 1.38 | 5.71 | 5.62 | 7.76 | 3.23 | ||
| 20− | 9.43 | 12.40 | 6.38 | 10.93 | 14.33 | 7.41 | 8.43 | 11.09 | 5.69 | ||
| 25− | 12.26 | 11.96 | 12.56 | 13.57 | 13.82 | 13.33 | 11.14 | 10.45 | 11.87 | ||
| 30− | 17.69 | 19.89 | 15.37 | 17.77 | 25.92 | 9.33 | 17.63 | 14.39 | 21.13 | ||
| 35− | 28.10 | 36.23 | 19.71 | 34.58 | 46.59 | 22.47 | 21.90 | 26.54 | 17.01 | ||
| 40− | 59.14 | 66.25 | 51.83 | 64.44 | 62.47 | 66.46 | 54.97 | 69.23 | 40.31 | ||
| 45− | 104.91 | 126.91 | 82.10 | 95.67 | 109.26 | 81.59 | 111.93 | 140.35 | 82.48 | ||
| 50− | 174.62 | 217.89 | 129.74 | 149.45 | 172.72 | 125.68 | 192.87 | 250.22 | 132.73 | ||
| 55− | 310.07 | 407.37 | 213.69 | 244.61 | 315.88 | 176.08 | 357.88 | 472.50 | 241.87 | ||
| 60− | 475.73 | 635.00 | 322.78 | 406.23 | 537.29 | 282.07 | 523.75 | 701.73 | 351.23 | ||
| 65− | 659.09 | 889.06 | 439.92 | 563.28 | 726.73 | 412.02 | 724.77 | 997.55 | 459.51 | ||
| 70− | 1,047.23 | 1,324.69 | 775.61 | 1,041.06 | 1,287.73 | 804.79 | 1,051.81 | 1,351.64 | 753.51 | ||
| 75− | 1,508.15 | 1,943.53 | 1,109.07 | 1,726.24 | 2,116.40 | 1,376.04 | 1,360.65 | 1,828.75 | 925.46 | ||
| 80− | 2,047.10 | 2,809.99 | 1,456.98 | 2,235.32 | 3,231.57 | 1,447.07 | 1,898.89 | 2,470.37 | 1,464.65 | ||
| 85+ | 3,017.27 | 4,102.20 | 2,318.30 | 3,989.15 | 5,695.42 | 2,913.63 | 2,248.04 | 2,870.81 | 1,839.85 | ||
Incidence and mortality for major cancers
Cancer incidence for the top 10 most common cancers
Cancers of lung, stomach, breast, esophagus and liver were the top 5 common cancers when both genders were combined, with estimated new cases of 35,200,24,900,15,650,15,100 and 15,100, respectively. In males, lung cancer was the most common cancer, followed by stomach cancer, esophageal cancer, liver cancer and colorectal cancer. Breast cancer was the most common cancer in females, followed by lung cancer, stomach cancer, colorectal cancer and cervical cancer (Table 6).
6.
Top 10 cancer incidence in Hebei province, 2012
| Rank | Both sexes | Male | Female | ||||||||||||||
| Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | |||
| *, age-standardized incidence rate(China population, 2000); CNS; central nervous system. | |||||||||||||||||
| 1 | Lung(C33-C34) | 35.20 | 47.34 | 18.34 | 38.43 | Lung(C33-C34) | 21.90 | 57.93 | 21.01 | 49.12 | Breast(C50) | 15.65 | 41.93 | 17.49 | 33.46 | ||
| 2 | Stomach(C16) | 24.90 | 34.17 | 13.25 | 27.26 | Stomach(C16) | 18.40 | 49.81 | 18.20 | 41.18 | Lung(C33-C34) | 13.30 | 36.33 | 15.15 | 28.52 | ||
| 3 | Breast(C50) | 15.65 | 41.93 | 8.14 | 33.46 | Esophagus(C15) | 10.40 | 28.00 | 10.29 | 23.22 | Stomach(C16) | 6.50 | 17.68 | 7.49 | 14.10 | ||
| 4 | Esophagus(C15) | 15.10 | 20.79 | 8.06 | 16.80 | Liver(C22) | 10.30 | 27.73 | 10.06 | 22.98 | Colorectum(C18-C21) | 5.90 | 16.04 | 6.69 | 12.52 | ||
| 5 | Liver(C22) | 15.10 | 20.79 | 8.06 | 16.73 | Colorectum(C18-C21) | 7.30 | 19.23 | 6.97 | 16.19 | Cervix(C53) | 5.80 | 15.87 | 6.62 | 12.99 | ||
| 6 | Colorectum(C18-C21) | 13.20 | 17.67 | 6.84 | 14.27 | Bladder(C67) | 2.40 | 6.17 | 2.24 | 5.40 | Liver(C22) | 4.80 | 13.58 | 5.66 | 10.66 | ||
| 7 | Cervix(C53) | 5.80 | 15.87 | 3.01 | 12.99 | Brain,CNS(C70-C72) | 2.30 | 6.10 | 2.21 | 5.51 | Esophagus(C15) | 4.70 | 13.08 | 5.41 | 10.10 | ||
| 8 | Brain,CNS(C70-C72) | 4.60 | 6.28 | 2.43 | 5.46 | Leukemia(C91-C95) | 2.21 | 5.66 | 2.05 | 5.26 | Ovary(C56) | 3.65 | 9.98 | 4.16 | 8.33 | ||
| 9 | Thyroid(C73) | 4.15 | 5.53 | 2.14 | 4.93 | Kidney(C64-C66,68) | 1.87 | 4.76 | 1.73 | 3.98 | Uterus(C54-C55) | 3.40 | 9.45 | 3.94 | 7.23 | ||
| 10 | Leukemia(C91-C95) | 4.01 | 5.25 | 2.04 | 4.91 | Prostate(C61) | 1.81 | 4.60 | 1.67 | 4.14 | Thyroid(C73) | 3.01 | 8.26 | 3.45 | 7.31 | ||
| Total | All | 187.90 | 258.12 | 100.00 | 210.65 | All | 101.10 | 275.75 | 100.00 | 232.65 | All | 86.80 | 239.78 | 100.00 | 191.81 | ||
Cancer death of the top 10 cancers
Lung cancer was the first leading cause of death in Hebei province, followed by cancers of stomach, liver, esophagus and colorectum, with estimated deaths of 28,200,18,300,13,100,10,700 and 6,800 respectively. In males, lung cancer was the main leading cause followed by stomach cancer, liver cancer, esophageal cancer and colorectal cancer. In females, lung cancer was still the leading cause, followed by stomach cancer, liver cancer, esophageal cancer and breast cancer (Table 7).
7.
Top 10 cancer mortality in Hebei province, 2012
| Rank | Both sexes | Male | Female | ||||||||||||||
| Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | |||
| *, age-standardized mortality rate(China population, 2000); CNS, central nervous system. | |||||||||||||||||
| 1 | Lung(C33-C34) | 28.20 | 37.86 | 23.00 | 31.53 | Lung(C33-C34) | 18.50 | 49.01 | 24.28 | 43.73 | Lung(C33-C34) | 9.70 | 26.26 | 20.86 | 20.53 | ||
| 2 | Stomach(C16) | 18.30 | 25.11 | 15.28 | 20.65 | Stomach(C16) | 13.40 | 36.28 | 17.99 | 31.41 | Stomach(C16) | 4.90 | 13.63 | 10.82 | 10.73 | ||
| 3 | Liver(C22) | 13.10 | 17.99 | 10.93 | 14.77 | Liver(C22) | 9.10 | 24.74 | 12.26 | 21.19 | Liver(C22) | 4.00 | 10.96 | 8.71 | 8.67 | ||
| 4 | Esophagus(C15) | 10.70 | 14.68 | 8.93 | 12.10 | Esophagus(C15) | 7.40 | 20.03 | 9.93 | 17.57 | Esophagus(C15) | 3.30 | 9.18 | 7.28 | 7.11 | ||
| 5 | Colorectum(C18-C21) | 6.80 | 8.90 | 5.41 | 7.41 | Colorectum(C18-C21) | 3.90 | 10.03 | 4.97 | 8.69 | Breast(C50) | 3.24 | 8.75 | 6.95 | 6.89 | ||
| 6 | Leukemia(C91-C95) | 3.33 | 4.49 | 2.73 | 4.16 | Leukemia(C91-C95) | 2.02 | 5.39 | 2.67 | 4.99 | Colorectum(C18-C21) | 2.90 | 7.73 | 6.14 | 6.17 | ||
| 7 | Breast(C50) | 3.24 | 8.75 | 2.68 | 6.89 | Pancreas(C25) | 1.77 | 4.56 | 2.26 | 3.93 | Cervix(C53) | 1.71 | 4.79 | 3.80 | 3.80 | ||
| 8 | Brain,CNS(C70-C72) | 2.96 | 4.01 | 2.44 | 3.58 | Brain,CNS(C70-C72) | 1.63 | 4.33 | 2.14 | 3.96 | Brain,CNS(C70-C72) | 1.33 | 3.68 | 2.92 | 3.20 | ||
| 9 | Pancreas(C25) | 3.01 | 3.97 | 2.41 | 3.28 | Lymphoma(C81-C85,88,90,96) | 0.93 | 2.36 | 1.17 | 2.13 | Leukemia(C91-C95) | 1.31 | 3.56 | 2.83 | 3.41 | ||
| 10 | Cervix(C53) | 1.71 | 4.79 | 1.43 | 3.80 | Prostate(C61) | 0.80 | 2.05 | 1.01 | 2.01 | Pancreas(C25) | 1.24 | 3.35 | 2.66 | 2.66 | ||
| Total | All | 119.80 | 164.63 | 100.00 | 137.30 | All | 74.50 | 201.85 | 100.00 | 177.63 | All | 45.30 | 125.92 | 100.00 | 100.28 | ||
Cancer incidence of the 10 most common cancers in urban areas
In urban areas, lung cancer was the most frequently diagnosed cancers, followed by breast cancer, colorectal cancer, liver cancer and stomach cancer with incidence cases of 20,300,10,730,7,600,7,400 and 6,300. The main sites of cancer were lung, liver, colorectum, stomach and esophagus in males. While in females, cancers of breast, lung, colorectum, cervix and liver were the common cancers (Table 8).
8.
Top 10 cancer incidence in urban areas of Hebei province, 2012
| Rank | Both sexes | Male | Female | ||||||||||||||
| Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | |||
| *, age-standardized incidence rate(China population, 2000); CNS, central nervous system. | |||||||||||||||||
| 1 | Lung(C33-C34) | 20.30 | 59.47 | 23.14 | 48.52 | Lung(C33-C34) | 12.70 | 73.57 | 28.95 | 62.79 | Breast(C50) | 10.73 | 63.78 | 24.54 | 50.26 | ||
| 2 | Breast(C50) | 10.73 | 63.78 | 12.55 | 50.26 | Liver(C22) | 5.10 | 29.50 | 11.61 | 24.73 | Lung(C33-C34) | 7.60 | 45.15 | 17.37 | 35.60 | ||
| 3 | Colorectum(C18-C21) | 7.60 | 22.06 | 8.59 | 17.98 | Colorectum(C18-C21) | 4.30 | 24.68 | 9.71 | 20.96 | Colorectum(C18-C21) | 3.30 | 19.40 | 7.46 | 15.39 | ||
| 4 | Liver(C22) | 7.40 | 21.78 | 8.47 | 17.56 | Stomach(C16) | 4.10 | 23.64 | 9.30 | 20.69 | Cervix(C53) | 2.90 | 17.10 | 6.58 | 13.74 | ||
| 5 | Stomach(C16) | 6.30 | 18.35 | 7.14 | 15.27 | Esophagus(C15) | 2.40 | 14.09 | 5.55 | 12.10 | Liver(C22) | 2.30 | 13.93 | 5.36 | 10.88 | ||
| 6 | Esophagus(C15) | 3.40 | 10.15 | 3.95 | 8.39 | Bladder(C67) | 1.70 | 9.83 | 3.87 | 8.66 | Stomach(C16) | 2.20 | 12.97 | 4.99 | 10.42 | ||
| 7 | Cervix(C53) | 2.90 | 17.10 | 3.30 | 13.74 | Leukemia(C91-C95) | 1.50 | 8.42 | 3.31 | 7.53 | Ovary(C56) | 2.08 | 12.39 | 4.77 | 9.91 | ||
| 8 | Leukemia(C91-C95) | 2.60 | 7.48 | 2.91 | 6.76 | Kidney(C64-C66,68) | 1.39 | 8.04 | 3.16 | 6.72 | Uterus(C54-C55) | 1.90 | 11.53 | 4.43 | 8.66 | ||
| 9 | Thyroid(C73) | 2.47 | 7.24 | 2.82 | 6.18 | Prostate(C61) | 1.36 | 7.85 | 3.09 | 7.17 | Thyroid(C73) | 1.65 | 9.80 | 3.77 | 8.26 | ||
| 10 | Brain,CNS(C70-C72) | 2.30 | 6.77 | 2.63 | 5.78 | Brain,CNS(C70-C72) | 1.30 | 7.38 | 2.90 | 6.46 | Leukemia(C91-C95) | 1.10 | 6.53 | 2.51 | 6.07 | ||
| Total | All | 87.60 | 256.99 | 100.00 | 211.32 | All | 43.90 | 254.09 | 100.00 | 219.10 | All | 43.70 | 259.93 | 100.00 | 207.84 | ||
Cancer death of the top 10 cancer in urban areas
Lung cancer was the leading cause of cancer death in urban areas in males and females with deaths of 10,800 and 5,800, respectively. Other cancer types with high mortality in males were liver cancer, stomach cancer, colorectal cancer and esophageal cancer. In females, breast cancer was the second cause of cancer death, followed by liver cancer, colorectal cancer and stomach cancer (Table 9).
9.
Top 10 cancer mortality in urban areas in Hebei province, 2012
| Rank | Both sexes | Male | Female | ||||||||||||||
| Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | |||
| *, age-standardized mortality rate (China population, 2000); CNS, central nervous system. | |||||||||||||||||
| 1 | Lung(C33-C34) | 16.60 | 48.56 | 30.13 | 40.79 | Lung(C33-C34) | 10.80 | 62.70 | 32.47 | 56.51 | Lung(C33-C34) | 5.80 | 34.20 | 26.57 | 27.08 | ||
| 2 | Liver(C22) | 6.00 | 17.44 | 10.82 | 14.49 | Liver(C22) | 4.10 | 23.55 | 12.19 | 20.67 | Breast(C50) | 2.10 | 12.49 | 9.70 | 9.86 | ||
| 3 | Stomach(C16) | 5.10 | 14.87 | 9.23 | 12.59 | Stomach(C16) | 3.50 | 20.43 | 10.58 | 18.67 | Liver(C22) | 1.90 | 11.24 | 8.73 | 8.84 | ||
| 4 | Colorectum(C18-C21) | 4.30 | 12.53 | 7.78 | 10.47 | Colorectum(C18-C21) | 2.60 | 15.04 | 7.79 | 13.16 | Colorectum(C18-C21) | 1.70 | 9.99 | 7.76 | 7.99 | ||
| 5 | Esophagus(C15) | 2.70 | 7.81 | 4.85 | 6.77 | Esophagus(C15) | 2.00 | 11.44 | 5.93 | 10.59 | Stomach(C16) | 1.60 | 9.22 | 7.16 | 7.34 | ||
| 6 | Breast(C50) | 2.10 | 12.49 | 3.93 | 9.86 | Leukemia(C91-C95) | 1.30 | 7.57 | 3.92 | 7.01 | Pancreas(C25) | 0.79 | 4.71 | 3.66 | 3.78 | ||
| 7 | Leukemia(C91-C95) | 2.01 | 6.00 | 3.73 | 5.61 | Pancreas(C25) | 1.24 | 7.19 | 3.72 | 6.30 | Cervix(C53) | 0.76 | 4.51 | 3.51 | 3.55 | ||
| 8 | Pancreas(C25) | 2.03 | 5.96 | 3.70 | 4.98 | Brain,CNS(C70-C72) | 0.93 | 5.39 | 2.79 | 5.05 | Leukemia(C91-C95) | 0.71 | 4.42 | 3.43 | 4.35 | ||
| 9 | Brain,CNS(C70-C72) | 1.58 | 4.62 | 2.87 | 4.16 | Lymphoma(C81-C85,88,90,96) | 0.72 | 4.16 | 2.15 | 3.75 | Ovary(C56) | 0.70 | 4.32 | 3.36 | 3.36 | ||
| 10 | Lymphoma(C81-C85,88,90,96) | 1.24 | 3.62 | 2.25 | 3.12 | Prostate(C61) | 0.57 | 3.31 | 1.71 | 3.20 | Esophagus(C15) | 0.70 | 4.13 | 3.21 | 3.41 | ||
| Total All 55.00 161.16 100.00 136.37 All 33.40 193.10 100.00 173.79 All 21.60 128.72 100.00 103.64 | |||||||||||||||||
Cancer incidence of the top 10 common cancers in rural areas
Table 10 shows the top 10 common cancer incidence rates in rural areas. Stomach cancer was the most frequently diagnosed cancers with 18,600 cases, followed by lung cancer, esophageal cancer, liver cancer and colorectal cancer. The most common sites of cancer in males were stomach, lung, esophagus, liver and colorectum. While in females, they were cancers of lung, breast, stomach, esophagus and cervix (Table 10).
10.
Top 10 cancer incidence in rural areas of Hebei province, 2012
| Rank | Both sexes | Male | Female | ||||||||||||||
| Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | |||
| *, age-standardized incidence rate (China population, 2000); CNS, central nervous system. | |||||||||||||||||
| 1 | Stomach(C16) | 18.60 | 47.98 | 18.54 | 37.84 | Stomach(C16) | 14.30 | 72.77 | 25.00 | 59.37 | Lung(C33-C34) | 5.70 | 29.79 | 13.25 | 23.40 | ||
| 2 | Lung(C33-C34) | 14.90 | 38.53 | 14.88 | 31.25 | Lung(C33-C34) | 9.20 | 46.80 | 16.07 | 39.51 | Breast(C50) | 4.92 | 25.73 | 11.44 | 20.59 | ||
| 3 | Esophagus(C15) | 11.70 | 30.18 | 11.67 | 23.80 | Esophagus(C15) | 8.00 | 40.71 | 13.99 | 33.23 | Stomach(C16) | 4.30 | 22.49 | 9.98 | 17.36 | ||
| 4 | Liver(C22) | 7.70 | 20.08 | 7.76 | 16.23 | Liver(C22) | 5.20 | 26.46 | 9.09 | 21.83 | Esophagus(C15) | 3.70 | 19.35 | 8.58 | 14.78 | ||
| 5 | Colorectum(C18-C21) | 5.60 | 14.47 | 5.59 | 11.58 | Colorectum(C18-C21) | 3.00 | 15.35 | 5.27 | 12.77 | Cervix(C53) | 2.90 | 14.96 | 6.66 | 12.21 | ||
| 6 | Breast(C50) | 4.92 | 25.73 | 4.96 | 20.59 | Brain,CNS(C70-C72) | 1.00 | 5.19 | 1.78 | 4.75 | Colorectum(C18-C21) | 2.60 | 13.54 | 6.02 | 10.39 | ||
| 7 | Cervix(C53) | 2.90 | 14.96 | 2.81 | 12.21 | Leukemia(C91-C95) | 0.71 | 3.70 | 1.27 | 3.62 | Liver(C22) | 2.50 | 13.33 | 5.93 | 10.62 | ||
| 8 | Brain,CNS(C70-C72) | 2.30 | 5.92 | 2.29 | 5.26 | Bladder(C67) | 0.70 | 3.57 | 1.23 | 3.09 | Ovary(C56) | 1.57 | 8.20 | 3.65 | 7.29 | ||
| 9 | Thyroid(C73) | 1.68 | 4.29 | 1.66 | 4.00 | Oral&pharyngx(C00-C10;C12-C14) | 0.61 | 3.10 | 1.06 | 2.56 | Uterus(C54-C55) | 1.50 | 7.91 | 3.52 | 6.20 | ||
| 10 | Ovary(C56) | 1.57 | 8.20 | 1.54 | 7.29 | Larynx(C32) | 0.50 | 2.56 | 0.88 | 2.04 | Thyroid(C73) | 1.36 | 7.13 | 3.17 | 6.70 | ||
| Total All 100.30 258.94 100.00 209.99 All 57.20 291.17 100.00 241.91 All 43.10 224.83 100.00 179.97 | |||||||||||||||||
Cancer death of the top 10 cancers in rural areas
Stomach cancer was the leading cause of cancer death in rural areas for both genders and the number of stomach cancer deaths were 9,900 and 3,300 for males and females. The mortality of stomach cancer in rural was 50.38/100,000 and 17.26/100,000 for males and females. The other cancer types with high mortality were lung cancer, esophageal cancer, liver cancer and colorectal cancer in males, and lung cancer, stomach cancer, esophageal cancer, liver cancer and colorectal cancer in females (Table 11).
11.
Top 10 cancer mortality in rural areas of Hebei province, 2012
| Rank | Both sexes | Male | Female | ||||||||||||||
| Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | Site | Cases (thousand) | Incidence(1/105) | % | ASR*(1/105) | |||
| *, age-standardized mortality rate (China population, 2000); CNS, central nervous system. | |||||||||||||||||
| 1 | Stomach(C16) | 13.20 | 34.05 | 20.37 | 27.75 | Stomach(C16) | 9.90 | 50.38 | 24.09 | 43.03 | Lung(C33-C34) | 3.90 | 20.38 | 16.46 | 15.74 | ||
| 2 | Lung(C33-C34) | 11.60 | 30.09 | 18.00 | 24.79 | Lung(C33-C34) | 7.70 | 39.26 | 18.87 | 34.44 | Stomach(C16) | 3.30 | 17.26 | 13.92 | 13.51 | ||
| 3 | Esophagus(C15) | 8.00 | 20.63 | 12.35 | 16.78 | Esophagus(C15) | 5.40 | 27.48 | 13.14 | 23.80 | Esophagus(C15) | 2.60 | 13.60 | 10.97 | 10.38 | ||
| 4 | Liver(C22) | 7.10 | 18.38 | 11.00 | 14.99 | Liver(C22) | 5.00 | 25.59 | 12.30 | 21.54 | Liver(C22) | 2.10 | 10.76 | 8.69 | 8.61 | ||
| 5 | Colorectum(C18-C21) | 2.50 | 6.27 | 3.75 | 5.19 | Colorectum(C18-C21) | 1.30 | 6.46 | 3.11 | 5.50 | Colorectum(C18-C21) | 1.20 | 6.06 | 4.89 | 4.82 | ||
| 6 | Brain,CNS(C70-C72) | 1.38 | 3.57 | 2.13 | 3.18 | Leukemia(C91-C95) | 0.72 | 3.84 | 1.84 | 3.49 | Breast(C50) | 1.14 | 5.99 | 4.83 | 4.70 | ||
| 7 | Leukemia(C91-C95) | 1.32 | 3.39 | 2.03 | 3.11 | Brain,CNS(C70-C72) | 0.70 | 3.57 | 1.72 | 3.10 | Cervix(C53) | 0.95 | 4.99 | 4.03 | 3.97 | ||
| 8 | Breast(C50) | 1.14 | 5.99 | 1.80 | 4.70 | Pancreas(C25) | 0.53 | 2.69 | 1.29 | 2.24 | Brain,CNS(C70-C72) | 0.68 | 3.56 | 2.88 | 3.28 | ||
| 9 | Pancreas(C25) | 0.98 | 2.53 | 1.51 | 2.05 | Larynx(C32) | 0.36 | 1.82 | 0.87 | 1.46 | Uterus(C54-C55) | 0.67 | 3.49 | 2.82 | 2.70 | ||
| 10 | Cervix(C53) | 0.95 | 4.99 | 1.45 | 3.97 | Bone(C40-C41) | 0.32 | 1.62 | 0.78 | 1.39 | Leukemia(C91-C95) | 0.60 | 2.92 | 2.36 | 2.77 | ||
| Total | All | 64.80 | 167.16 | 100.00 | 137.58 | All | 41.10 | 208.08 | 100.00 | 179.42 | All | 23.70 | 123.85 | 100.00 | 97.86 | ||
Discussion
Hebei Cancer Registry Center was established in 2009 and has published cancer statistics annual reports based on cancer registries’ data (3, 4) since 2012. Among Hebei provincial cancer registries, Cixian cancer registry was established in 1973, and its data were published in Cancer Incidence in Five Continents (CI5VⅢ and CI5X) (5, 6). Shexian cancer registry was established in 2000 and the data were published in the Chinese Cancer Registry Annual Report (2008-2013). In 2015,9 cancer registries submitted 2012’s cancer data to Hebei Cancer Registry Center. This study provides a comprehensive overview of cancer incidence and mortality rates and estimates new cancer cases and cancer deaths in Hebei province in 2012. It’s necessary that cancer statistics were updated and published every year for monitoring the changes of cancer rates and taking measures on cancer prevention and control.
This study showed that the crude incidence rate of cancers was 258.12/100,000 in Hebei Cancer Registries areas in 2012 which was lower than the incidence level of China in 2012 (264.85/100,000), but after adjusted by age, the incidence was 1.11 times higher than the national level (7, 8). The estimated new cancer cases were 187,900. The mortality was slightly higher than the national level, and after adjusted by age, the mortality rate was 1.23 times higher than the national level with the estimated death number of 119,800. The trend of agespecific incidence and mortality in Hebei province was similar to that in China in 2012.
The top 10 most common cancers (lung cancer, stomach cancer, breast cancer, esophageal cancer, liver cancer, colorectal cancer, cervical cancer, brain cancer, thyroid cancer and leukemia) in 2012 were basically the same in the latest three years in Hebei province, but they were different from cancer structure (lung cancer, stomach cancer, liver cancer, colorectal cancer, esophageal cancer, breast cancer, thyroid cancer, cervical cancer, brain cancer and pancreatic cancer) in China in 2012. Lung cancer was the most common and the first leading cause of death in Hebei province in 2012, followed by stomach cancer, liver cancer, esophageal cancer and colorectal cancer. They were consistent with the cancer in the preceding three years and similar to national cancer spectrum (lung cancer, liver cancer, stomach cancer, esophageal cancer and colorectal cancer) in 2012.
The incidence of cancer in Hebei province showed a special characteristic pattern. The incidence of esophageal cancer in Hebei Cancer Registries in 2012 was 1.14 times higher than the national level. The estimated new cancer cases were 15,100 in the whole province. The incidence of stomach cancer (27.26/100,000) in Hebei Cancer Registries in 2012 was 1.24 times higher than the national level. There were about 24,900 new cancer cases in the whole province in 2012. We can infer that the burden of stomach and esophageal cancers in Hebei province is still heavy. One of the reasons is that Hebei province is the high-risk area of upper digestive cancers. The esophageal cancer incidence of Cixian is the highest in China and even in the world. Moreover, upper digestive system cancer screening started from 2000 and there are 17 project units in Hebei province now. Though the mortality of esophageal cancer was 1.14 times higher than the national level, the mortality rate of esophageal cancer has showed an obvious decreasing trend in the past 40 years in Hebei province (9). It decreased 40.19% from 48.69/100,000 in 1973-1975 to 29.12/100,000 in 2010- 2012. Cixian and Shexian are the high-risk areas for esophageal cancer in Hebei province. There was a decrease of 64.4% in mortality rate of esophageal cancer from 252.50/100,000 in 1988 to 89.81/100,000 in 2012 for males and 56.8% for females from 126.74/100,000 to 54.75/100,000 in Cixian. The data indicated that we have achieved great success in the screening, early detection and treatment of esophageal cancer in Hebei province, and we need continue efforts to reduce the mortality. However, the mortality of stomach cancer was 1.36 times higher than that in China which was a threat to the residents’ health in Hebei province. Cancers from upper digestive system are still the common cancers. Health education, promotion and early detection should be placed priority in cancer strategies.
The incidence of lung cancer in Hebei province was 1.06 times higher than the average level in China. The estimated incidence number was 35,200. Baoding area was with heavier air pollution and its population accounted for about 47.68% of urban registration population. As we all know, the southern Hebei has experienced severe outdoor air pollution in recent years, with PM2.5 concentration leveling at 200 μg/m3 on foggy days. It has been proven to be one of the most seriously polluted areas in China (10). The Ministry of Environmental Protection (MEP) released that the SO2 emissions in Hebei province were 1.28 million tons, ranking the third of all provinces in China. While the NOX emissions were 1.65 million tons, ranking the first in 2013. Moreover, smoke (powder) dust emissions in Hebei province took the top spot with more than 1.20 million tons (11). The American Cancer Society (ACS) showed that each 10 μg/m3 increment of fine particles (PM2.5) was associated with an 8%-14% increase in lung cancer (12). Environmental protection in Hebei province should be taken into attention.
Cigarette smoking, radon and secondhand smoke exposure would be major risk factors of lung cancer (13, 14). In Hebei province, 16,640 residents were randomly selected by multiple stages sampling and surveyed in 2003. The study showed that the cigarette smoking rate of both genders was 26.08%, while it was 48.09% for males (15). Scientific evidence clearly shows that tobacco exposure is significantly associated with the cause of lung cancer and among Chinese lung cancer patients, about 60%-70% are ever-smokers (16). In order to decrease the lung cancer, the efforts for tobacco control should be greatly intensified in Hebei province. The lung cancer mortality rate was 1.09 times higher than that in China and it has showed an obvious increasing trend in the past 40 years in Hebei province (17). It increased by 194.57% from 1973 to 2012, making it the leading cause of death in Hebei province. It should be strengthened to prevent and control the lung cancer.
The female breast cancer rate was similar to national level, and the estimated new diagnosed cases and deaths were 15,650 and 3,240 respectively. Hebei province also suffered a heavy burden of female breast cancer. The mortality rates in Hebei province increased by 1.55 times from 1973-1975 to 2010- 2012. The same increasing trend in the mortality rate was observed in Cixian with annual percentage change of 3.82% from 1988 to 2012. In order to increase the rates of early detection and treatment, reduce the mortality rate and improve the health status for females, a wide-scale screening program for breast cancer should be attempted in Hebei province (18).
Conclusions
This study analyzed only 9 national cancer registries’ data in 2012, and the coverage of registration needs to be further expanded, the completeness and effectiveness need to be further improved. Overall, it’s a heavier cancer burden in Hebei province, and the reduction of cancer incidence and mortality in Hebei province is still the top priority. Screening, early detection and treatment, reduction of air pollution and tobacco control are still the focus of our future work.
Acknowledgments
We gratefully acknowledged the cooperation of all the population-based cancer registries in providing cancer statistics, data collection, sorting, verification and database creation. Funding: This study was supported by grants from the National Natural Scientific Foundation of China (81272682), the Financial Department of Hebei Province [No.(2012)2056] and the Financial Department of Hebei province [No.(2014)1257].
Footnotes
The authors have no conflicts of interest to declare.
References
- 1.Curado MP, Edwards B, Shin HR, et al. Cancer Incidence in Five Continents. Lyon: IARC; 2008. pp. 1–837. [Curado MP, Edwards B, Shin HR, et al. Cancer Incidence in Five Continents. Vol. IX. Lyon: IARC, 2008:1-837.] [Google Scholar]
- 2.Ferlay J. The IARCcrg Tools Programs. Lyon: IARC; 2006. [Ferlay J. The IARCcrg Tools Programs. Lyon: IARC, 2006. Available online: <a href="http://www.iacr.com.fr/index. php?option=com_content&view=category&layout=blog&i d=68&Itemid=445">http://www.iacr.com.fr/index. php?option=com_content&view=category&layout=blog&i d=68&Itemid=445</a> ] [Google Scholar]
- 3.He Y, Liang D, Li D, et al. Incidence and mortality of cancers appeared in the Hebei provincial cancer registry system in 2011. Zhonghua Liu Xing Bing Xue Za Zhi (in Chinese) 2015;36:846–851. [He Y, Liang D, Li D, et al. Incidence and mortality of cancers appeared in the Hebei provincial cancer registry system in 2011. Zhonghua Liu Xing Bing Xue Za Zhi (in Chinese),2015,36:846-851.] [PubMed] [Google Scholar]
- 4.He Y, Liang D, Zhai J, et al. Analysis of cancer incidence and mortality in Hebei province, 2010. Zhonghua Yu Fang Yi Xue Za Zhi (in Chinese) 2014;48:1–3. [He Y, Liang D, Zhai J, et al. Analysis of cancer incidence and mortality in Hebei province, 2010. Zhonghua Yu Fang Yi Xue Za Zhi (in Chinese) 2014,48:1-3.] [Google Scholar]
- 5.Parkin DM, Whelan SL, Ferlay J, et al. Cancer Incidence in Five Continents CI5VⅢ. Lyon: IARC; 2005. [Parkin DM, Whelan SL, Ferlay J, et al. Cancer Incidence in Five Continents CI5VⅢ. Lyon: IARC, 2005.] [Google Scholar]
- 6.Forman D, Bray F, Brewster DH, et al. Cancer Incidence in Five Continents Vol. X. Lyon: IARC; 2014. [Forman D, Bray F, Brewster DH, et al. Cancer Incidence in Five Continents Vol. X. Lyon: IARC, 2014.] [Google Scholar]
- 7.Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–132. doi: 10.3322/caac.21338. [Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin, 2016,66:115-132.] [DOI] [PubMed] [Google Scholar]
- 8.Chen W, Zheng R, Zhang S, et al. Report of cancer incidence and mortality in China, 2012. Zhongguo Zhong Liu (in Chinese) 2016;25:1–8. doi: 10.3760/cma.j.issn.0253-3766.2018.01.002. [Chen W, Zheng R, Zhang S, et al. Report of cancer incidence and mortality in China, 2012. Zhongguo Zhong Liu (in Chinese),2016,25:1-8.] [DOI] [PubMed] [Google Scholar]
- 9.He Y, Wu Y, Song G, et al. Incidence and mortality rate of esophageal cancer has decreased during past 40 years in Hebei Province, China. Chin J Cancer Res. 2015;27:562–571. doi: 10.3978/j.issn.1000-9604.2015.10.06. [He Y, Wu Y, Song G, et al. Incidence and mortality rate of esophageal cancer has decreased during past 40 years in Hebei Province, China. Chin J Cancer Res, 2015,27:562-571.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yang J, Zhang P, Meng C, et al. Quantifying the sources of the severe haze over the Southern Hebei using the CMAQ model. Scientific World Journal. 2013;2013:812469. doi: 10.1155/2013/812469. [Yang J, Zhang P, Meng C, et al. Quantifying the sources of the severe haze over the Southern Hebei using the CMAQ model. Scientific World Journal, 2013,2013:812469.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ministry of Environmental Protection of the People’s Republic of China. Environment Statistical Review in 2013 (2014-11-24). Available online: <a href="http://zls.mep.gov.cn/hjtj/ nb/2013tjnb/201411/t20141124_291867.htm">http://zls.mep.gov.cn/hjtj/ nb/2013tjnb/201411/t20141124_291867.htm</a>
- 12.Straif K, Cohen A, Samet J. Air Pollution and Cancer. Lyon: IARC; 2014. [Straif K, Cohen A, Samet J. Air Pollution and Cancer. Lyon: IARC, 2014.] [Google Scholar]
- 13.Guo Y, Zeng H, Zheng R, et al. The association between lung cancer incidence and ambient air pollution in China: A spatiotemporal analysis. Environ Res. 2016;144:60–65. doi: 10.1016/j.envres.2015.11.004. [Guo Y, Zeng H, Zheng R, et al. The association between lung cancer incidence and ambient air pollution in China: A spatiotemporal analysis. Environ Res, 2016,144:60-65.] [DOI] [PubMed] [Google Scholar]
- 14.Chen Z, Peto R, Zhou M, et al. Contrasting male and female trends in tobacco-attributed mortality in China: evidence from successive nationwide prospective cohort studies. Lancet. 2015;386:1447–1456. doi: 10.1016/S0140-6736(15)00340-2. [Chen Z, Peto R, Zhou M, et al. Contrasting male and female trends in tobacco-attributed mortality in China: evidence from successive nationwide prospective cohort studies. Lancet, 2015,386:1447-1456.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lu A, Wang X, Gao G, et al. Comparative study on cigarette smoking between urban and rural residents in Hebei province. Zhongguo Gong Gong Wei Sheng (in Chinese) 2005;21:908–909. [Lu A, Wang X, Gao G, et al. Comparative study on cigarette smoking between urban and rural residents in Hebei province. Zhongguo Gong Gong Wei Sheng (in Chinese),2005,21:908-909.] [Google Scholar]
- 16.Zhou C. Lung cancer molecular epidemiology in China: recent trends. Transl Lung Cancer Res. 2014;3:270–279. doi: 10.3978/j.issn.2218-6751.2014.09.01. [Zhou C. Lung cancer molecular epidemiology in China: recent trends. Transl Lung Cancer Res, 2014,3:270-279.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.He Y, Li D, Song G, et al. Lung cancer burden has increased during the last 40 years in Hebei Province, China. Thorac Cancer. 2016;7:323–332. doi: 10.1111/1759-7714.12331. [He Y, Li D, Song G, et al. Lung cancer burden has increased during the last 40 years in Hebei Province, China. Thorac Cancer, 2016,7:323-332.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sivasubramaniam PG, Zhang BL, Zhang Q, et al. Breast Cancer Disparities: A Multicenter Comparison of Tumor Diagnosis, Characteristics, and Surgical Treatment in China and the U.S. Oncologist. 2015;20:1044–1050. doi: 10.1634/theoncologist.2014-0290. [Sivasubramaniam PG, Zhang BL, Zhang Q, et al. Breast Cancer Disparities: A Multicenter Comparison of Tumor Diagnosis, Characteristics, and Surgical Treatment in China and the U.S. Oncologist, 2015,20:1044-1050.] [DOI] [PMC free article] [PubMed] [Google Scholar]