

Abstract
Though the number of female medical graduates has increased throughout the world, their postgraduate professional achievements are said to be suboptimal. Our aim is to look into the achievements of Sudanese female pediatricians and compare them with their male counterparts. A cross sectional study was undertaken using a questionnaire involving pediatricians working in the universities and Ministry of Health, Sudan. Ninety five (65.1%) out of 146 pediatricians responded; 73 (76.8%) were females and 22 (23.2%) were males. Thirty (41%) Of the females were in the academic career. Only 2 (8.3%) out of 24 assistant professors were promoted to associate professors and non of the four associate professors managed to become a professor compared to 68% and 25% among males, respectively. Twenty three (76.6%) of females compared to 31% of males had no publications. Nineteen out of 21 females (90.4%) who have been offered training opportunities abroad declined the offer for family reasons. Fifty four (93%) female pediatricians declined to work outside the capital state. No nursery facilities were available at work place. The main reasons for inadequate achievements included family issues, cultural obstacles, lack of mentorships and unsatisfying work environment and facilities. Suggestions were put forward to improve on these problems. Though female doctors are the majority of undergraduate and graduate students in Sudan, their professional and academic achievements after specialization are not optimal mainly for socio-cultural reasons and these need to be addressed.
Keywords: Female doctors, Women, Pediatrics, Sudan
Introduction
Up to the beginning of the 20th century in many western countries, women were barred from joining the medical schools and even after qualification they were short of jobs [1]. Interestingly, one of the most vigorous opponents of women in medicine was the founder of Great Ormond Street Hospital, Charles West [1]. But since 1950 the number of female graduates increased steadily in most countries. In 2007, 57% of places to medical schools went to women in the UK and more than 50% in the United States. This is specially so for the field of pediatrics. In 2002 women comprised nearly 70% of pediatrician in training and 50% of all practicing pediatricians in the US [2]. However, although the percentage of women in medicine have more than quadrupled, there is substantial evidence that women have not advanced in academic rank as rapidly as men in medical schools and are less likely to be considered for or hold leadership posts, and many factors including balancing family life, male domination and lack of mentorship were mentioned among others [3]. The first two Sudanese female doctors graduated in 1952 and since then, a similar pattern was experienced and the impression was that female doctors in Sudan face similar problems. The objective of this study was to see the current status of female pediatricians in Sudan including their numbers, achievement and problems. To the best of our knowledge, this issue has not been addressed before in Sudan.
Materials and Methods
This is a cross sectional, descriptive study, including pediatricians working at different universities and at institutes of Ministry of Health (MOH) in Sudan. In 2010 we conducted a cross-sectional survey using a specially designed questionnaire. The questionnaire was distributed by hand and emailed to 146 Sudanese pediatricians. They were asked to provide data on their achievements, progression and problems. Our main target was females but males were included for comparison. Other related data were collected from University of Khartoum student’s registry, Graduate College-Medical and Health Board, University of Khartoum, Sudan Medical Council (SMC), Sudan Medical Specialization Board (SMSB) and through personal contacts. Data were analyzed using SPSS version 19 and summarized as pro-portions, means and median values.
Results
The first medical school in Sudan, Kitchener Medical School, now Faculty of Medicine, University of Khartoum (U of K) was established in 1924. Within the academic regulations nothing was against the enrolment of women to the medical school but it took almost 23 years before the first two Sudanese women were graduated. Since then the number of females has increased steadily reaching (69.5%) in 2009 (Figure 1). The total number of females who graduated from the Faculty of Medicine, U of K till 2009 was 3021 out of 7870 (38.4%). This percentage increased gradually from 8.9% in the period 1928-1980 to 32.6% and 64.7% in the periods 1981-1999 and 2000-2009, respectively.
Figure 1.
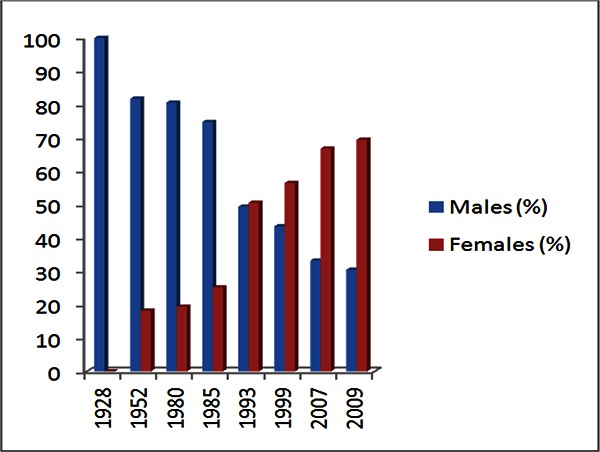
Percentage and gender of the medical students who graduated from the Faculty of Medicine, University of Khartoum (period 1928 – 2009)
The local postgraduate training of pediatrics in Sudan started in 1976 at the University of Khartoum. The total number of graduates from 1980 – 2008, before the training was shifted to Sudan Medical Specialization Board (SMSB), was 249 of whom 149 (59.8%) were females. Among the first graduates batch there were four (28%) females and 14 (72%) males. The number of females increased to 80.5% in the period 2006-2008 (Figure 2). Before 1980 there were only four or five Sudanese pediatricians who were trained abroad. The Sudan Medical Specialization Board (SMSB) graduated its first pediatrician’s batch in 1999. The total number of pediatricians who graduated till 2010 was 212 of whom 112 (52.8%) were females. The number of pediatricians registered at Sudan Medical Council (SMC) up to 2010 was 567, out of whom 265 (46.7%) were females.
Figure 2.
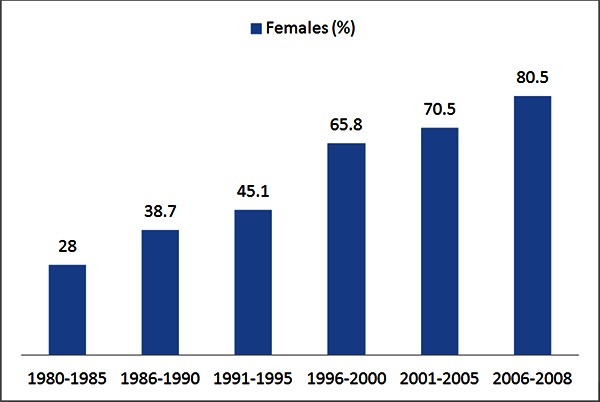
Percentage of female pediatricians who graduated from the Faculty of Medicine, University of Khartoum in the period 1980 – 2008
At the Faculty of Medicine, U of K the total number of the academic staff was found to be 209 of whom 52 (24.9%) were females and 157 (75.1%) were males. The females represented only 11.5% of the associate professors and 4.9% of the full professors. In the Department of Pediatrics and Child Health, there were 16 (75%) males and 8 (25%) females of whom only one (12.5%) was an associate professor, seven (87.5%) assistant professors and no female professor. Out of 146 pediatricians to whom the questionnaire was sent, 95 (65.1%) responded. Seventy three (76.8%) were females and 22 (23.2%) males. Out of 73 females, 30 (41%) were in the academic career compared to 16 (72.7%). Among the academic group, only 7/30 (23.1%) of the female doctors had publications compared to 17/22 (68.9%) of the male doctors. In terms of academic promotion, while 4/20 (20%) of males were promoted, 2 as associate professors and 2 as full professors, only 2/28 (7.1%) of the females were promoted to become associate professors but none was to full professor. Out of the 30 females in academic career, 16 (53.3%) are working in a subspecialty unit but without formal subspecialty training. Twenty one out of 30 (70%) females in academic career were given opportunities to travel abroad for further training, 19/21 (90.4%) declined the offer. Concern about their children in 9/21 (47.4%) and objection by family in 8/21 (42.1%) were mentioned among other reasons for this. The females in academic career tend to participates in different committees as well as administrative jobs especially at departmental level, but to a lesser degree than males (Table 1). Nineteen out of 30 (63.3%) females apologized joining these committees. Among the reasons mentioned were that a lot of meetings are held outside the working hours and this conflicted with their family commitments.
Table 1.
Participation of academic staff in administrative jobs and University committees (N=49)
Males (N=16) N (%) |
Females (N=30) N (%) |
P - Value |
|
|---|---|---|---|
Administrative job |
14 (87.5) |
20 (66.7) |
0.053 |
Departmental committees |
14 (87.5) |
22 (73.3) |
0.112 |
College committees |
08 (50.0) |
13 (43.3) |
0.340 |
University committees |
06 (37.5) |
10 (33.3) |
0.366 |
Forty three (49%) of females and 8 (36.3%) males were working for the MOH. Thirty out of 43 (69.8%) females, had been asked to move to work outside the Capital State, but 25 (83.3%) declined to do so. The commonest reasons mentioned were family commitments, objection by their families mainly because of lack of secure residence. Suggestions put to encourage females to work in peripheral hospitals are shown in Table 2.
Table 2.
Suggestions given to encourage females to work outside the Capital State (N=95)
Suggestions |
No (%) |
|---|---|
Solving family issues (husband work, children education) |
69 (72.6) |
Improve working facilities and environments |
69 (72.6) |
Secure residence |
60 (63.2) |
Improve salaries and financial incentives |
58 (61.0) |
More transfer to original home(town and states |
56 (58.9) |
To be considered as part of promotion criteria |
49 (51.6) |
Work for short periods of time |
24(25.3) |
Others |
19 (20.0) |
Table 3.
Suggestions to improve the professional achievements of female pediatricians after specialization (N=95)
Suggestions |
(%) N |
|---|---|
Shared job, part time jobs, less working hours without part time job |
45 (47.4) |
High quality child care units at working place |
42 (44.2) |
Flexible training years |
40 (42.1) |
Local subspecialties training |
40 (42.1) |
Short courses in different subspecialties - abroad |
38 (40.0) |
Senior guidance and motivation |
30 (31.5) |
Different promotion criteria for females |
21 (22.1) |
Longer maternity leaves |
21 (22.1) |
Others |
13 (13.7) |
Fifty eight (79.5%) of the total female doctors were married, 11(15.1%) single, two (2.7%) widow and 2(2.7%) divorced; in comparison to males who were all married. Fifty four (93.1%) of the married females and 19(86.3%) of males had children. Out of 73 females 30 (41.1%) had long breaks during their career practice, of whom 13(43.3%) had difficulties in practicing again. Thirty (41.1%) females and six (27.3%) males thought that males are preferentially treated at work place. Twenty (27.4%) females and six (27.3%) males thought that males tend to be dominant in the work place. Thirty seven (50.7%) females, compared to (13.7%) of males were not satisfied with their mentorship. Only two (2.1%) out of 95 had nursery facility at their work place.
Fifty six (76.7%) of total females were not satisfied by their achievement after specialization, compared to 10(45.5%) of males. Among the commonest reasons mentioned were family issues, lack of subspecialty training programs in Sudan, lack of senior guidance and supervision.
Discussion
Primary education in Sudan was started by the British in 1898 and formal female education started in 1907 by Sheikh Babiker Badri, a social activist. Initially it took place at his home including nine of his own daughters and eight of those of his neighbours, and then it received a government subsidy. The main direction of the schooling was towards better nutrition and healthcare, with a view to ensuring healthier children [4]. By 1920 there were five state elementary schools for girls. In view of conservatism of Sudanese society, female education remained restricted to the elementary level until 1940 when the first intermediate school for girls, the Omdurman Girls’ Intermediate School was opened. By 1955, ten intermediate schools for girls were in existence. Since that time Sudanese women had a major share in public work and community development. The main reasons that motivated Sudanese women in 1940s and 1950s to work were the economic benefits and family needs. Women in 1960s onwards had other motivators such as the belief in women participation in public life and the desire to realize self-actualization [5]. Though there was nothing against females joining the medical school, it took almost 24 years before the first two Sudanese female doctors - Khalda Zahir and Z Serkisiani-to graduate from Kitchener School of Medicine in 1952.
In this study we have taken the Faculty of Medicine, University of Khartoum as a model, being the mother medical school, thus reflecting the changes through different generations over more than 80 years. It is worth mentioning that there are almost 23 medical schools now in Sudan. Our study has shown that the proportion of female medical students has increased up to 69.5% forming almost 64.7% of the total graduates in the period 2000–2009. This is very similar to experiences from different parts of the world; for example the number of women who graduated from US medical schools has risen from 6.9% in 1966 to 47.1% in 2005 [6]. In Saudi Arabia, females constituted 40% of the graduates in the period from 1981 to 2003 and figures are possibly higher now [7]. In United Kingdom, the proportion of female medical graduates increased from 25% in 1960s to 61% in 2009 [8]. Many reasons are given including preference of females to medicine, hard work with less adolescence out of home distracters compared to males [7].
Pediatrics is one of the medical specialities that mostly attract women. In our study the proportion of females who got enrolled in the pediatric training program at University of Khartoum increased from 28% in 1976 to 83% in 2007. Similarly, females constituted 52% of the graduates from Sudan Medical Specialization Board. Currently females constitute 46.7% of the Sudanese pediatricians registered in Sudan Medical Council. In Sudan with increase in number of female graduates and migration of more men than women to the Gulf and other parts of the world, females might soon form two thirds of the working force. In UK, women account for almost 40% of the consultant paediatricians and specialist registrars, compared to 7% in surgery [8]. In Saudi Arabia, pediatrics and pathology were the most attractive specialities to females [7]. In 1993 in Canada, 62% of paediatrics residents, 33% of the total paediatricians and 50% of those under 45 years of age were women [9]. In US in 1974 women held 24% of the physicians taking paediatric speciality board examination, reaching 50% in 1987 and possibly higher now [10].
In this study 30 (41%) of the female pediatricians were in academic medicine and there was no reported prejudice against females joining academic departments. However, their academic achievements, publications and representation in leadership and higher posts were less than males. This is similar to the experience from the West [11-14] and Middle East countries [7]. The main reasons given were difficulties in balancing between family commitments and profession in addition to lack of mentorship. In United States only 10% of full professors were females and in United Kingdom women represented only 11% of professors in medicine [11,15,16]. In University of Khartoum females represent only 4.1% of all professors. Female doctors were reported to dedicate a greater proportion of their professional effort to teaching and patients care as opposed to research [17], though the latter is considered to be the most important pre-requisite for promotion. In addition, women with children were also found to participate less in international conferences than their male colleagues, thus making them to have less academic exposure [7]. Another reason mentioned by the study group is lack of mentorship. It has been reported that women with mentors reported more publications, had more time spent on research activities than those without mentors and reflected higher overall career satisfaction [8]. It might therefore be tempting to suggest that the promotion criteria for women in academic institutions should not necessarily be similar to men. Fried et al [18] described a multifaceted initiative in Johns Hopkins University including problem identification, leadership courses and education, mentoring, rewards and steps to reduce isolation and structural career impediments. It resulted in women being retained and promoted and a five – fold increase in women at associate professorial rank over five years [18].
Various studies have shown that females are less represented in administrative jobs and university committees [19-22]. In our study although there was no significant difference between male and female doctors regarding participation in committees, there was significant difference in their participation in administrative jobs and 19 females (63.3%) had apologized joining or heading committees, as the majority of the meetings were held outside the core time and or no fixed days. Women often have multiple roles beyond work, including family commitments. If the meetings were held within core time and on fixed days, it may encourage them to join these committees and held leadership posts. Recently, a working force in United States put forwards some suggestions to improve the status of women in academic institutions including part time work options, availability of high quality day-care and childcare, flexibility in tenture-track positions and recruitment of qualified women into leadership positions [14].
The professional and academic achievements of females working in the non-academic institutions, namely Ministry of Health was even worse. Only 6.9%of them had publications and 12% had opportunities to work in subspecialty units. The main reasons given were work overload, lack of mentorship and poor environment including nursing and childcare facilities.
With the increase in the number of women graduates and migration of men to other parts of the world, women will form the main working force. For many reasons, women prefer working in urban areas and big cities. This situation may leave the rural areas (65% of Sudan populations) with few doctors. In this study, 43 (69.8%) of the females pediatricians were transferred to areas outside the Capital State, but 83% of them declined to go. The main reasons given were family commitments, lack of secure accommodation, financial issues and poor work facilities. Almost 80% of them were married with children and they wanted to make sure that there would be jobs for their husbands, good schooling for their children and a guarantee to be transferred back after staying for few years. Most of Sudanese families are very conservative and would not accept their unmarried daughters (even pediatricians) to travel to work alone in a remote area particularly if there is a problem of security, and almost 50% of our study group families objected the transfer of their daughters to work in urban areas. Active steps should therefore be taken to solve these problems, including secure proximal residency, short stay transfer, financial and professional incentives, working in their original home towns and securing jobs for their husbands particularly if they are doctors. Most of the females in this study were not able to get formal subspecialty training even those in the academic institutions. Twenty one out of 30 (70%) of those in the universities were given opportunities to travel abroad for further training but 19 (90.4%) declined mainly because of their children and cultural reasons. The best answer for the problem would, therefore, be to establish local subspecialty training programs or find training opportunities in countries with similar cultural background as some current experiences have shown.
Most of the study group complained about male dominance in the work place. This is similar to the experience in many Eastern and Western countries where they faced problems with some male mentors who do not understand the family issues [12,13,23,24].. Women also face prejudice as many male seniors regard female colleagues as burdens, and culturally men look at themselves as superior with better judgment and decision – making abilities [7]. This unwritten code belies intimidation and dissemination that affects performance and productivity of women predictable outcomes including premature abandonment of careers by some of them. This is particularly because most rules and regulations of work are setup by men including promotion criteria and working hours [25]. In this study some felt burned- out and left their career and had long breaks, 43% of them had difficulty in practicing again.
Similar to the experience elsewhere, 76% of the female pediatricians in this study were not satisfied with their professional achievements. Many reasons including family and work environment issues were mentioned. To answer these problems people have to understand that women have more responsibilities than their profession. Their productivity is said to be M-shaped, being active at the beginning, down at child bearing age, picking up again later. Therefore, these facts should be seriously considered [26-29].
Conclusion
Similar to experiences from different parts of the world, the number of Sudanese medical graduates is increasing. However their academic achievements and representation in leadership and higher posts are less than males. The main reasons are difficulties in balancing between family commitments and profession, inadequate work environment and sociocultural factors. Some rules and regulations including promotion criteria and work load to suit females should be considered.
Acknowledgement
We would like to thank all pediatricians who participated in this study.
References
- 1.Bride Stevens D., prejudice and paediatrics. Women in paediatrics in England before 1950. Arch Dis Child 2006; 91: 866–870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Leadley J. Women in U.S. academic medicine, statistics and medical school benchmarking 2009. Available at: https://www.aamc.org/download/53502/data/wimstatisticsreport2009.pdf
- 3.Brown A, Swinyard W, Ogle J. Women in Academic Medicine: A Report of Focus Groups and Questionnaires, with Conjoint Analysis. J Women’s Hlth 2003; 12: 999–1008. [DOI] [PubMed] [Google Scholar]
- 4.Kenyon S. Introduction The Sudanese Women, Ist ed Khartoum: Postgraduate College Publications; 1989;1–7. [Google Scholar]
- 5.Abdel-Azim M. The History and Development of Women in Clerical Work in Sudan. Ahfad J 2002; 900–904.
- 6.Heather A, Phillips Mc, Burke Ann E., Sheppard Kate, Pallant Adam, Bruder F., et al. Toward Creating Family-Friendly Work Environments in Pediatrics: Baseline Data from Pediatric Department Chairs and Pediatric Program Directors. Pediatrics 2007; 119: e596–e602. [DOI] [PubMed] [Google Scholar]
- 7.Al-Tamimi Dalal M.. Saudi Women in academic medicine, Are they succeeding? Saudi Med J 2004; 25(11): 1564–567. [PubMed] [Google Scholar]
- 8.Allen A. Education and debate, women doctors and their careers: what now? BMJ 2005; 331: 569–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Laurent St-, Gangon T, Dural RC, Lippe J, Cóté-Bioleau T. Women in paediareics: The experience in Quebec. Can MED Assoc J 1993; 148(5): 773–778. [PMC free article] [PubMed] [Google Scholar]
- 10.DeAngelis K. Trends and Implications of Women in Paediatrics. Am J Dis Child 1990; 144: 173–76. [DOI] [PubMed] [Google Scholar]
- 11.Bickel J, Wara D, Atkinson F, Cohen LS, Dunn M, Hostler S, et al. Increasing women’s leadership in academic medicine: report of the AAMC project implementation committee. Acad Med 2002; 77: 1043–61 [DOI] [PubMed] [Google Scholar]
- 12.Women Chairs of the Association of Medical School Pediatric Department Chairs. Women in Pediatrics: Recommendations for the Future. Pediatrics May 2007; 119(5): 1000–5. [DOI] [PubMed] [Google Scholar]
- 13.Benz E. Increasing academic internal medicine’s investment in female faculty. Am J Med Sci 1998:105; 459–63. [DOI] [PubMed] [Google Scholar]
- 14.Bellini L, Abbuhl S, Grisso J, Lavizzo-Mourey R, Shea J. Stresses and workplace resources for academic junior faculty: track and gender comparisons. Acad Med 2001; 76: 62–4. [DOI] [PubMed] [Google Scholar]
- 15.Nonnemaker L. Women physician in academic medicine: new insights from cohort studies. N Engl J Med 2000; 342: 399–405 [DOI] [PubMed] [Google Scholar]
- 16.Ash AS, Carr PL, Goldstein R, Friedman RH. Compensation and advancement of women in academic medicine: is there equality? Ann Intern Med 2004; 141: 205–12. [DOI] [PubMed] [Google Scholar]
- 17.Shea S, Nickerson KG, Tenenbaum J. Morris TQ, Rabinowitz D, O’Donnell K, et al. Compensation to a department of medicine and its faculty members for the teaching of medical students and house staff. N Engl J Med 1996; 334: 162–67. [DOI] [PubMed] [Google Scholar]
- 18.Fried LP, Francomano CA, MacDonald SM, Wagner EM, Stokes EJ, Carbone KM, et al. Career development for women in academic medicine: Multiple interventions in a department of medicine. JAMA 1996; 276(11): 898–905. [PubMed] [Google Scholar]
- 19.Uhlenberg P, Cooney TM. Male and female physicians: Family and career comparisons. Soc Sci Med 1990; 30: 373–78. [DOI] [PubMed] [Google Scholar]
- 20.Mayer AP, Files JA, Ko MG, Blair JE. Academic advancement of women in medicine: Do socialized gender differences have a role in mentoring? Mayo Clin Proc 2008; 83: 204–7. [DOI] [PubMed] [Google Scholar]
- 21.Levinson W, Kaufman K, Clark B, Tolle SW. Mentors and role models for women in academic medicine. West J Med 1991; 154: 423–26. [PMC free article] [PubMed] [Google Scholar]
- 22.Carr PL, Ash AS, Friedman RH. Relation of family responsibilities and gender to the productivity and career satisfaction of medical faculty. Ann Intern Med 1998; 129: 532–38. [DOI] [PubMed] [Google Scholar]
- 23.Levinson W, Tolle SW, Lewis C. Women in academic medicine. Combining career and family. N Engl J Med 1989; 321: 1511–517. [DOI] [PubMed] [Google Scholar]
- 24.Warde C, Allen W, Gelberg L. Physician role conflict and resulting career changes. Gender and generational differences. J Gen Intern Med 1996; 11: 729–35. [DOI] [PubMed] [Google Scholar]
- 25.Russell W. Chesney PJ. Women paediatricians: can facts shed light on prejudices and myths? J Pediatr 2004; 144: 413–14. [DOI] [PubMed] [Google Scholar]
- 26.Schofield C, Schofield Z. Flexible training for men and women – is this the way forward for medicine? BMJ 2005; 331: 1211–211. [Google Scholar]
- 27.David C, Goodman. The Pediatrician Workforce: Current Status and Future Prospects DOI: 10.1542/peds.2005-0874. Pediatrics 2005; 116: e156. [DOI] [PubMed] [Google Scholar]
- 28.Cull WL, Mulvey HJ, O’connor KG, Sowell DR, Berkowitz CD, Britton CV. Pediatricians working part time: past, present, and future. Pediatrics 2002; 109: 1015–20. [DOI] [PubMed] [Google Scholar]
- 29.Shanafelt TD, West CP, Sloan JA, Novotny PJ, Poland GA, Menaker R, et al. Career fit and burnout among academic faculty. Arch Intern Med 2009; 169: 990–95. [DOI] [PubMed] [Google Scholar]