

Abstract
The birth of a child with ambiguous genitalia is a matter of a medical and social emergency to decide the appropriate sex rearing and eventually to prevent the associated metabolic disturbances. It must be taken with immediacy and great sensitivity. The pediatric endocrinologist should share the care with a team consists of a pediatric urologist, or surgeon, a pediatric radiologist, geneticist and a child psychiatrist or psychologist who should work closely with the family. Ultrasonograpy is the primary modality for demonstrating internal organs while genitography is used to assess the uterus, vagina, and any fistulas or complex tracts. Magnetic resonance imaging (MRI) is used as an adjunct modality to assess the internal gonads and genitalia. Early and appropriate gender assignment is necessary for healthy physical and psychological development of children with ambiguous genitalia.
Keywords: Ambiguous genitalia, Disorders of sex development, Radiological imaging, Ultrasound, Genitogram, Magnetic resonance
Introduction
Disorder of sexual development (DSD) formerly termed intersex conditions, are among the most fascinating conditions encountered by the clinicians. The ability to diagnose these conditions has advanced rapidly in recent years. It is a matter of a medical and social emergency to decide the appropriate sex of rearing and eventually to prevent the associated metabolic disturbances [1–11].
Embryology of Sexual Differentiation (Figure 1)
Figure 1.
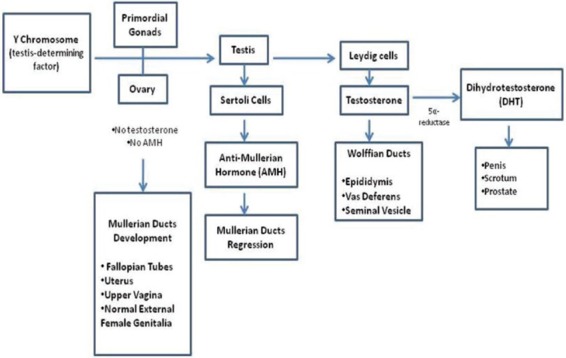
Simplified module for sexual differentiation and development of internal and external genitalia.
Gonadal Differentiation
During the second month of fetal life, the undifferentiated gonads are guided by the genetic information present on the short arm of the y chromosome into a testes. This is determined by the so-called Testis-determining factor (TDF), which is a 35 kilobase pair sequence on the 11.3 subband of the Y chromosome and the named sex-determining region of Y chromosome (SRY). When the region is absent, the undifferentiated gonad develops into an ovary. Other genes important to testicular development include DAXI on the x-chromosome, SFI on band 9q33 WTI on band 11 p 13, so x 9 on bands 17 q 24–25, and Anti Mullerian hormone (AMH) on band 19q13.3 i.e., fetal ovaries develop when TDF gene (genes) is absent.
Differentiation of Internal ducts
Development of the internal ducts results from a paracrine effect from the ipsilateral gonads. When testicular tissue is absent, the fetus morphologically develops into the internal female organs and external phenotypic female. When testicular tissue is present, that produces testosterone and Mullerian-inhibiting substance (MIS) or AMH, which appears to be critical for development of sex ducts and external male phenotype. Testosterone is produced by testicular Leydig cells and subsequently the primordial Wolffian (mesonephric) duct develops into epididymis, vas deferens, and seminal vesicle.
High local testosterone appear to be necessary for Wolffian duct differentiation because maternal ingestion of androgens does not cause male internal differentiation in a female fetus, or does this differentiation occur in females with congenital adrenal hyperplasia (CAH). MIS is produced by the Sertoli cells of the testis by the 8th week and is critical to normal male internal duct development and appears to have a repress passive development of Mullerian ducts.
Differentiation of external genital
The external genitalia of both sexes are identified during the first 8 weeks of gestation, without the hormonal action of testosterone and dihydrotestosterone (DHT), external genitalia appear phenotypically female. In the gonadal male, differentiation to a male phenotype actively occurs. The testosterone rise, at the time, in response to luteinizing hormone (LH) from the placenta [1,3,11].
Classification of Disorders of Sexual Development and Nomenclature
Recently, the Lawson Wilkins Pediatric Endocrine Society (LWPES) and the European Society for Pediatric Endocrinology (ESPE) have published proposed changes to the nomenclature and definition of disorders of sex development (DSD) to reflect the recent advances in our understanding (Table 1) [12–14].
Table 1.
Change in Nomenclature of disorders of sex development
Previous |
Revised |
|---|---|
Female pseudohermaphrodite |
46 XX DSD |
Male pseudohermaphrodite |
46 XY DSD |
True Hermaphrodite |
Ovotesticular DSD |
XX – male |
46, XX testicular DSD |
XY – sex Reversal |
46, XY Complete gonadal dysgenesis |
DSD have been defined as congenital conditions in which development of chromosome, gonad, or anatomic sex is atypical. DSD vary in frequency depending on their etiology (Table 2). Congenital adrenal hyperplasia CAH is the most common of ambiguous genitalia in the newborn worldwide, while, mixed gonadal dysgenesis (MGP) is the second most common cause of DSD. Hypospadias occur at a rate of 1 case per 300 live male [1–11,15,16].
Table 2.
Major causes of Disorders of Sex Development (DSD) according to karyotype
46, XX Karyotype |
|
|
|
|
Enzyme Deficiency: |
|
Congenital Adrenal |
21α-Hydroxylase |
46 XX DSD |
Hyperplasia (CAH) |
11β-Hydroxylase |
|
|
3 β-Hydroxysteroid dyhydrogenase |
|
Ovarian/Adrenal Tumors (mother-child) |
|
|
Exposure to exogenous medication (synthetic progestin preparation) |
|
Ovotesticular DSD |
|
|
46, XY DSD |
Lack of synthesis of testosterone |
|
|
Lack of synthesis of dihydrotestosterone |
5α-reductase deficiency |
|
End-organ-unresponsiveness (resistance) |
|
Ovotesticular DSD |
|
|
Multiple or local congenital anomalies |
|
|
Mixed Karyotype |
|
|
Ovotesticular DSD 46, XX/46 XY | ||
Mixed gonadal dysgenesis 45 X/46 XY | ||
Radiological Imaging
Management starts with the initial contact with the family by a member of DSD team and taking a detailed medical history. An assessment of the genital appearance and whether gonadal tissue is present are crucial. Chromosomal and other genetic studies if needed and specific hormonal studies should be undertaken.
The disorders of sex development (DSD) team is consisted of a pediatrician, a pediatric endocrinologist, a pediatric urologist, or surgeon, geneticist, a pediatric psychiatrist or psychologist, and a pediatric radiologist [17].
Imaging plays an important role in evaluating the internal organs and urogenital anatomy in children with ambiguous genitalia. Ultrasonography remains the primary modality for evaluation of the internal reproductive organs, whereas genitography and voiding cystourethrography are used for evaluation of urethral and vaginal tracts and fistulas and hence used as an important marker for surgical strategy. MR imaging may serve as a problem solving modality for clarifying the internal anatomy and searching for internal gonads [18–32].
Ultrasonography
Ultrasonolgraphy remains the primary modality for establishing the presence or absence of a uterus, Figure 2. It is safe and quickly performed without sedation and it does not expose the patient to radiation. An ultrasound examination should include the inguinal, perineal, renal, and adrenal. In US, identification of a uterus was found in 90%, while ovary has been seen in 40%. Adrenal glands, with a limb over 20 mm long and 4 mm wide, with normal cortico-medullary differentiation are suggestive of congenital adrenal hyperplasia (CAH) (Figure 2).
Figure 2.

A Sagittal view of a pelvic ultrasound of a newborn female baby with ambiguous genitalia caused by congenital adrenal hyperplasia, due to 21 hydroxylase deficiency showing a uterus (Ut) with echogenic endometrium.
However, the presence of normal-sized adrenal glands will not exclude the diagnosis. It is believed that it is not just the size of the gland, but a combination of a limb with greater than 4 mm, a lobulated surface (cerebriform appearance) (Figure 3), and increased enchogenicity are suggestive the diagnosis of CAH [18–23]. Alwan et al, found a combination of a limb greater than 4 mm, a lobulated surface and stippled echogenicity with a sensitivity of 92% and a speicificity of 100% [21].
Figure 3.

An ultrasound image of adrenal glands showing an enlarged, lobulated with maintained normal corticomedullary differentiation (A). It has a “cerebriform” appearance (B) in a newborn with congenital adrenal hyperplasia due to 21 hydroxylase deficiency.
Fluoroscopy-Genitography
This helps determining ductal anatomy. A catheter can be inserted into the distal urogenital sinus. It is more invasive and exposes the patient to much radiation. Genitography demonstrates a male or female type urethral configuration and any fistulous communication with the vagina or rectum [Figure 4]. An adequate genitogram should help identifying the exact location where the urethra and the vagina are joined. These anatomic characteristic are very important for mapping surgical strategy [24].
Figure 4.

A genitography of a newborn baby with ambiguous genitalia due to 21 hydroxylase deficiency congenital adrenal hyperplasia showing contrast material filling the urethra, bladder (Bl), vagina (V) and uterus (Ut) and cervix.
Magnetic Resonance (MR)
T1 and T2 weighted MR imaging sequences with their multiplanar capability superior tissue characteristics can provide detailed anatomic information. MR imaging was found useful in evaluating ambiguous genitalia with detecting the uterus in 93% of cases, the vagina in 95%, the penis in 100%, the testis in 88%, and the ovary in 74% (Figure 5α, b). MR imaging is more sensitive than US in the evaluation of the gonads [25–32].
Figure 5.

A T2 weighted magnetic resonance imaging (MRI) of the pelvis (a) showing no uterus and (b) showing testicles within the inguinal canals in a patient with complex androgen insensitivity.
MR imaging and US are considered equally sensitive in the evaluation of intrapelvic structures. However, MR imaging is more sensitive than US in detecting the gonads [29].
Acknowledgement
The author would like to thank Ms. Hanna Grace G. Olvido and Ms. Cecile S. Sael for their secretarial assistance in typing this manuscript.
References
- 1.Rappaport R, Forest MG. Disorders of sexual differentiation In: Bertrand J, Rappport R, Sizomenko PC, editors Paediatric endocrinology: physiology, pathophysiology, and clinical aspects. 2nd ed. London (GB): Williams and Wilkins; 1993;447–470. [Google Scholar]
- 2.Abdullah MA, Katugampola M, Al-Habib S, Al Jurayyan N, Al-Samarrai A, Al-Nuaim A, Ambiguous genetalia: Medical, socio-cultural and religious factors affecting management in Saudi Arabia. Ann Trop Pediatr. 1991; 11 (4): 343–348. [DOI] [PubMed] [Google Scholar]
- 3.Saenger PH. Physiology of sexual determination and differentiation In: Brook CGD, Hindmarsh PC, editors Clinical Pediatric Endocrinology. 4th ed. Oxford (GB): Blackwell Scientific Publisher; 2001; 60–76. [Google Scholar]
- 4.Lambert SM, Vilain EJ, Kolon TF. A practical approach to ambiguous genitalia in the newborn period. Urol Clin North America. 2010; 37 (2): 195–205. [DOI] [PubMed] [Google Scholar]
- 5.Houk CP, Lee PA. Update a Disorders of sex Development. Curr. Opin. Endocrine Diabetes obes. 2012; 19(1): 28–32. [DOI] [PubMed] [Google Scholar]
- 6.Al–Mutair A, Iqbal, Sakatti N, Ashwal A. Cytogenetics and Etiology of Ambiguous Genitalia in 120 Pediatric Patients. Ann. Saudi Med. 2004; 24: 368–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abdullah MA, Saeed U, Abass A, Lubna K, Weam A, Ali A.S, et al. Disorders of Sex Development among Sudanese Children; 5-year experience of pediatric Endocrinology Clinic. J Pediatric Endocrinol Metab. 2012; 25: 1065–72. [DOI] [PubMed] [Google Scholar]
- 8.Al-Jurayyan NAM. Ambiguous Genitalia: Two decides of Experience. Ann. Saudi Med. 2011; 31: 284–88 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sax L. How common is Intersex? A response to Anna Fausto-Sterling. J Sex Res. 2002; 39: 174–78. [DOI] [PubMed] [Google Scholar]
- 10.Al-Jurayyan NAM. Disorders of sex Development: Diagnostic approaches and Management Options: An Islamic Perspective. Malaysian J Med Sci 2011; 18: 4–12. [PMC free article] [PubMed] [Google Scholar]
- 11.Jost A, Vigier B, Prepin J, Prechellet JP. Studies on sex differentiation in mammals. Rec Prog Horn Res 1973; 29: 1–41. [DOI] [PubMed] [Google Scholar]
- 12.Hughes IA. Disorders of Sex Development: A new definition and classification. Best Pract Res Clin Endocrinol Metab. 2008; 22(1): 119–134. [DOI] [PubMed] [Google Scholar]
- 13.Hughes IA, Houk C, Ahmed SF, Lee PA. Consenus Statement on Management of Intersex Disorders. J Peditr Urol. 2006; 2(3): 148–162. [DOI] [PubMed] [Google Scholar]
- 14.Hughes IA, Nihoul-Fekete C, Thomas B, Chohenkettenis PT. Consequences of the ESPE/LWPES guidelines for diagnosis and treatment of disorders of sex development. Best Pract Res Clin Endocrinol Metab. 2007; 21 (3): 351–365. [DOI] [PubMed] [Google Scholar]
- 15.Al-Jurayyan NAM, Al-Herbish AS, Abo Bakr AM, Al-Rabeeah AA, Al-Samarrai AI, Jawad AJ. Congenital Adrenal Hyperplasia in a Referral Hospital in Saudi Arabia: Epidemiology, Pattern and Clinical Presentation. Ann Saudi Med. 1995; 15(5): 447–450. [DOI] [PubMed] [Google Scholar]
- 16.Lubaini MM, Isaa ARA, Bushnag R, Al-Saleh QA, Dudin KI, Reavy PC, et al. Prevalence of Congenital Adrenal Hyperplasia in Kuwait. Eur J Pediatr. 1990; 149 (6): 391–392. [DOI] [PubMed] [Google Scholar]
- 17.Moshiri M, Chapman T, Fechner PY, Dubinsky TJ, Shnorhavorian M, Osman S, et al. Evaluation and Management of Disorders of Sex Development: Multidisciplinary Approach to a Complex Diagnosis. Radiographics 2012; 32: 1509–1018. [DOI] [PubMed] [Google Scholar]
- 18.Chavhan GB, Parra DA, Oudjhana K, Miller SF, Babyn PS, Pippi-Salle FL. Imaging of Ambiguous Genitalia: Classification and Diagnostic Approach. Radiographics 2008; 28: 1891–1904. [DOI] [PubMed] [Google Scholar]
- 19.Sivit CJ, Hurg W, Taylor GA, Catena LM, Brown-Jones C, Kushner DC. Sonography in Neonatal Congenital Adrenal hyperplasia. AJR AM J Roentgenol 1991; 156: 141–143. [DOI] [PubMed] [Google Scholar]
- 20.Avni EF, Rypens F, Smet MH, Galetty E. Sonographic Demonstration of Congenital Adrenal Hyperplasia in the Neonate: The Cerebriform Pattern: Pediatr. Radiol 1993:23: 88–90. [DOI] [PubMed] [Google Scholar]
- 21.Al-Alwan I, Navarro O. Daneman D, Daneman A. Clinical Utility of Adrenal Ultrasonography in the Diagnosis of Congenital Adrenal Hyperplasia. J Pediatr 1999; 135: 71–75. [DOI] [PubMed] [Google Scholar]
- 22.Wright NB, Smith C, Rickwood AM, Carty HM. Imaging Children with Ambiguous Genitalia and Intersex state. Clin Radiol. 1995; 50: 823–28. [DOI] [PubMed] [Google Scholar]
- 23.Cohen HL, Shapiro MA, Mandel FS, Shapiro ML. Normal Ovaries in Neonates and Infants. A Sonographic Study of 77 patients 1 day to 24 months old. AJR Am J Roentgenol 1993; 160: 583–586. [DOI] [PubMed] [Google Scholar]
- 24.Al Jurayyan NA, Patel PJ, Al Herbish AS, Abdullah MA, Abo-Bakr AM, Al Rabeeah AA. Ambiguous Genitalia: Comparative Role of Pelvic Ultrasonography and Genitography. Ann Trop Pediatr. 1995; 15(3): 203–207. [DOI] [PubMed] [Google Scholar]
- 25.Secaf E, Hricak H, Gooding CA, Ho VW, Gorczyca DP, Ringertz H, et al. Role of MRI in the Evaluation of Ambiguous Genitalia. Pediatr Radiol 1994; 24: 231–35. [DOI] [PubMed] [Google Scholar]
- 26.Hricak H., Marotti M, Gilbert TJ, Lue TF, Wetzel LH, McAninch JW, et al. Normal Penile Anatomy and abnormal Penile conditions: evaluation with MR Imaging. Radiology 1988; 169: 683–690. [DOI] [PubMed] [Google Scholar]
- 27.Choi HK, Cho K, Lee H, Kim KS. MR imaging in intersexuality. Radiographics 1998; 18: 83–91. [DOI] [PubMed] [Google Scholar]
- 28.Kanemoto K, Hayashi Y, Kojima Y, Maruyama T, Ito M, Kohri K. Accuracy of Ultrasonography and Magnetic Resonance Imaging in the Diagnosis of non-palpable testis. Int J Urol 2005; 12: 668–72. [DOI] [PubMed] [Google Scholar]
- 29.Mansour SM, Hamed ST, Adel L, Kamal RM, Ahmed DM. Does MRI add to ultrasound in the assessment of Disorders of sex development? Eur J Radiol 2012; 81 (9); 2403–10. [DOI] [PubMed] [Google Scholar]
- 30.Biswas K, Kapoor A, Karak AK Kripplani A, Gupta DK, Kucheria K, et al. Imaging Intersex Disorders. J Pediatr Endo Met. 2004; 17(6): 841–845. [DOI] [PubMed] [Google Scholar]
- 31.Gambino J, Caldwell B, Dietrich R, Walot I, Kangarloo H. Congenital Disorders of Sexual Differentiation; MR Findings. AJR AM J Roentgenol 1992. 158; 363–367. [DOI] [PubMed] [Google Scholar]
- 32.Hiricak H, Chang YC, Thumher S. Vagina Evaluation with MR imaging. Normal Anatomy and Congenital Anomalies. Radiology 1988; 169: 169–174. [DOI] [PubMed] [Google Scholar]