

Abstract
Background
There is growing evidence that teamwork in hospitals is related to both patient outcomes and clinician occupational well-being. Furthermore, clinician well-being is associated with patient safety. Despite considerable research activity, few studies include all three concepts, and their interrelations have not yet been investigated systematically. To advance our understanding of these potentially complex interrelations we propose an integrative framework taking into account current evidence and research gaps identified in a systematic review.
Methods
We conducted a literature search in six major databases (Medline, PsycArticles, PsycInfo, Psyndex, ScienceDirect, and Web of Knowledge). Inclusion criteria were: peer reviewed papers published between January 2000 and June 2015 investigating a statistical relationship between at least two of the three concepts; teamwork, patient safety, and clinician occupational well-being in hospital settings, including practicing nurses and physicians. We assessed methodological quality using a standardized rating system and qualitatively appraised and extracted relevant data, such as instruments, analyses and outcomes.
Results
The 98 studies included in this review were highly diverse regarding quality, methodology and outcomes. We found support for the existence of independent associations between teamwork, clinician occupational well-being and patient safety. However, we identified several conceptual and methodological limitations. The main barrier to advancing our understanding of the causal relationships between teamwork, clinician well-being and patient safety is the lack of an integrative, theory-based, and methodologically thorough approach investigating the three concepts simultaneously and longitudinally. Based on psychological theory and our findings, we developed an integrative framework that addresses these limitations and proposes mechanisms by which these concepts might be linked.
Conclusion
Knowledge about the mechanisms underlying the relationships between these concepts helps to identify avenues for future research, aimed at benefiting clinicians and patients by using the synergies between teamwork, clinician occupational well-being and patient safety.
Electronic supplementary material
The online version of this article (doi:10.1186/s12913-016-1535-y) contains supplementary material, which is available to authorized users.
Keywords: Teamwork, Clinician well-being, Patient safety, Framework, Systematic review
Background
Patient safety is an important indicator of hospitals’ organizational performance. Approximately 10 % of patients suffer adverse events and half of those are deemed preventable [1]. Vincent defined patient safety as the absence of preventable adverse events – events that are a consequence of healthcare interventions rather than the patients’ condition [2]. Healthcare is predominantly provided by teams – two or more people each with specialized roles and responsibilities whilst interacting with the shared goal of patient care [3]. Consequently, in addition to medical competence, effective teamwork is critical for safe patient care [4–7]. This includes both observable team behaviors and clinicians’ perceptions of interpersonal team processes. For example, several studies have linked better coordination or team psychological safety to fewer medical errors and better patient outcomes such as length of stay [8–10]. Also, specific team behaviors, for example leadership, information sharing or decision making and team properties (e.g., shared mental models) are associated with performance indicators such as decision and execution latency or protocol adherence [5, 11, 12].
Teamwork is also an important predictor of another indicator of hospitals’ organizational performance: the well-being of healthcare providers [13, 14]. Reduced occupational well-being or high psychological strain may develop as an immediate or long-term response to stressors [15] and is highly prevalent in healthcare workers [16, 17]. Teamwork may constitute such a stressor. For instance, dysfunctional inter-professional teamwork predicts increased acute and chronic clinician strain [18, 19]. However, effective teamwork may protect team members from the effects of work stress, since positive perceptions of teamwork are associated with enhanced occupational well-being indicators such as better mental health in nurses and physicians [20, 21].
Lastly, clinicians’ occupational well-being and patient safety are interrelated. Reduced clinician occupational well-being is associated with objective and subjective patient safety indicators such as mortality ratios, clinician-rated safety and reported errors [13, 22, 23]. Highly strained clinicians might thus pose a threat to patient safety since patient safety incidents are stressors that may lead to decreased clinician well-being: clinicians report increased emotional distress following medical error [24].
Studies investigating associations between teamwork, clinician occupational well-being and patient safety originate from very different strands of research – medical, nursing, and psychology. So far, the evidence generated has not been drawn together for systematic evaluation. While this research showed that relationships exist between the independent associations of teamwork, clinician occupational well-being and patient safety, few studies investigated them simultaneously. Moreover, the mechanisms underlying the relationships and causalities between either two – and potentially all three – concepts are largely unknown.
To overcome this research gap, we aimed to provide an overview of the current state of research on relationships between at least two of the three concepts of teamwork, clinician occupational well-being, and patient safety in hospital settings. In a systematic review, we summarized theoretical foundations, sample, methodology, and empirical findings, and evaluated overall study quality. Based on relevant psychological theories and on the findings of the systematic review, we developed a conceptual framework integrating the three concepts. Specifically, we propose theoretically informed causal relationships between the concepts, describe focal points of past research, and identify gaps in the current knowledge. The framework is intended to serve as a blueprint both for future studies intended to benefit clinicians’ occupational well-being and patients’ safety.
Methods
Definition of central concepts
Teams and teamwork
In order to include a diverse array of healthcare teams, we used rather broad definitions of teams and teamwork. A team is defined as a group of two or more people embedded in an organizational system with specialized roles who are interdependent and socially interact with each other in order to reach a common goal [3]. Studies were included if the teams investigated matched these criteria. We based our definition of teamwork on the model by Marks and colleagues, which includes transition (planning, goal formulation), action (coordination, monitoring), and interpersonal processes (conflict management, motivation, or team members’ perceptions thereof, e.g., team climate) [25]. Thus, we excluded studies comparing the effects of team-based work to other forms of work organization. We included leadership if it was clearly directed at the team level, and excluded studies examining dyadic or organizational leadership processes. Lastly, we excluded studies assessing inter-team processes, because we were interested in how working within a team relates to patient safety and clinician well-being.
Clinician occupational well-being
Under occupational well-being, our aim was to identify studies investigating both positive and negative aspects [26–28]. We specifically included studies, based on Lazarus’ stress model, which investigated work-related psychological or physiological strain as an individual’s short- or long-term perception of, or response to, stressors at work, such as burnout [15]. In the case of workplace stressors, these are often referred to as job demands. According to the job demands-resources model, job demands are defined as physical, social, or organizational job characteristics that require increased effort, thereby depleting the individual’s energy and eventually decreasing occupational well-being or increasing strain [29]. We included studies examining mental fatigue (i.e., exhaustion or lack of energy that is not due to physical overexertion) if direct measures of mental fatigue were used rather than being inferred from external indicators such as shift duration [30]. Furthermore, we included general or work-related positive indicators of occupational well-being as an outcome of lack of job demands, or the abundance of job resources, such as work engagement. Job resources are physical, social, or organizational characteristics that help maintain the individual’s energy, thereby increasing occupational well-being or reducing the strain caused by job demands [29]. Our aim was to focus the review on studies examining occupational well-being as the result of appraisal of a stressor or lack thereof. For this reason, we excluded studies examining aspects of occupational well-being in the wider sense, i.e., studies investigating aspects that are the result of a large array of workplace characteristics, such as job satisfaction or organizational commitment. We furthermore excluded studies examining personality traits or psychopathological disorders. Lastly, we excluded long-term chronic somatic disorders such as lower back pain, as it is often unclear whether these conditions are caused by continuous psychological strain or physical activities.
Patient safety
We defined patient safety as “the avoidance, prevention, and amelioration of adverse outcomes or injuries stemming from the process of healthcare” [31]. We included studies covering variables that could directly affect a patient’s health status (i.e., reported or observed errors, key actions not being performed), as well as subjective patient safety ratings and objective morbidity-mortality-data. We excluded studies assessing quality of patient care or using safety climate as a substitute outcome measure.
Search strategy
We searched six databases (Medline, PsycArticles, PsycInfo, Psyndex, ScienceDirect, and Web of Knowledge) to identify relevant literature. Our a priori assumption was that teamwork, clinicians’ occupational well-being and patient safety are related to each other. Thus, we combined two of the three keywords TEAMWORK, PATIENT SAFETY, WELL-BEING with AND. We then combined the results with OR. In order to receive both relevant and manageable results, we applied a number of strategies (e.g., MeSH/thesaurus terms, related terms, alternative spellings, truncations or plural forms, and adjacency terms; the complete search strategy for one database can be viewed in Additional file 1). Further inclusion criteria were: peer-reviewed journal articles, published in English between January 2000 and June 2015, referring to a hospital setting. We included studies sampling practicing nurses or physicians. If multiple publications were based on the same dataset, we either selected the paper that was first published or reported the most extensive data analysis. Finally, we hand-searched reference lists of the selected articles and systematic reviews we identified in our initial search.
Screening and selection procedure
Two raters screened (AW and either MD, SS, or JV) all references independently. We scanned the title and abstract at the first stage and included studies investigating at least two of the three concepts (teamwork, patient safety, clinician well-being) in a hospital setting. At the second stage, we included studies reporting a statistical relationship between at least two of the relevant concepts, which clearly described measurement methods and were published in peer-reviewed journals. Disagreements between raters at the first screening stage led to inclusion, after which we resolved disagreements at the second stage by consensus discussion.
Quality rating
To systematically assess study quality, we combined and slightly adapted existing systems. [32, 33] Ratings were based on a maximum of 19 items (not all items were applicable for all studies) covering topics such as validity of measures or statistical analyses. Items were rated as 0 = major limitations/not applicable/not mentioned, 0.5 = some limitations, or 1 = fulfilled. Two raters (AW and MD) independently evaluated study quality and resolved disagreements through discussion. All quality rating items are available in Additional file 2.
Data extraction
We extracted study setting, study design, method of data collection, data analysis, and study outcomes from the selected studies. If results were described in sufficient detail but effect sizes were not reported, we calculated them according to convention [34, 35] to give an indication of whether a statistically significant relationship was large enough to infer practical significance (see Table 1 for an overview of effect size magnitudes) [36]. In some studies, teamwork, clinician occupational well-being and patient safety may have been analyzed within a larger context (e.g., nurse working environment), however, only relationships between the variables of interest to this review are reported.
Table 1.
| Effect size | Abbreviation | Small | Medium | Large |
|---|---|---|---|---|
| Coefficient of determination | R2 | .02 | .13 | .26 |
| Cohen’s ƒ | ƒ | .14 | .39 | .59 |
| Eta squared | η2 | .01 | .06 | .14 |
| Odds ratio | OR | 1.5 | 3.5 | 7.0 |
| Pearson correlation | r | .10 | .30 | .50 |
Framework development
Building on the results of our systematic review, the framework development followed two stages. Based on the assumption that teamwork, clinicians’ occupational well-being and patient safety are correlated, our aim was to provide a framework summarizing the current state of research and exploring the underlying mechanisms and causal directions between the concepts. First, we examined measures, samples, and definitions of teamwork, well-being and patient safety to provide an overview of the evidence, and to detect trends and shortcomings in current research. Second, we drew from the theoretical foundations of the reviewed studies and from psychological theories relevant to the topic to aid interpretation of the findings and formulate hypotheses regarding the causal relationships between teamwork, clinician occupational well-being and patient safety to point out avenues for future research.
Results
The database search from January 2000 to June 2015 yielded 26,870 results. We identified an additional 62 publications through other sources (e.g., hand-searching references lists). After removing duplicates, 21,186 publications remained. Following title and abstract screening, we retrieved the full text of 1697 publications. Examining full-texts and hand-searching reference lists led to the inclusion of 98 publications (see Fig. 1). Of these, 25 (26 %) investigated relationships between teamwork and well-being, 43 (44 %) between teamwork and patient safety, 25 (26 %) between well-being and patient safety, and five (5 %) included all three concepts.
Fig. 1.
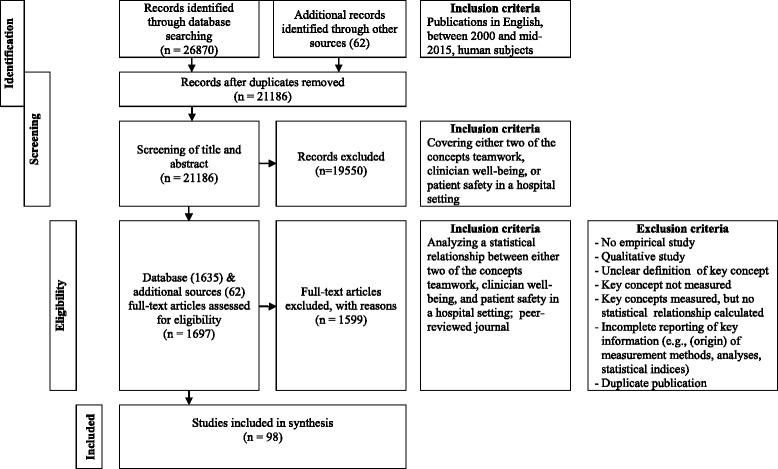
Flow diagram illustrating search method and inclusion/exclusion criteria
Quality rating
Selected studies were of medium (49 studies) or high quality (49 studies; see Tables 2, 3, 4 and 5 for individual quality scores). Average study quality was similar across the three concepts; teamwork, well-being and patient safety (i.e., 11.48 for teamwork/well-being [SD = 1.68], 11.03 for teamwork/patient safety [SD = 2.04], 10.92 for well-being/patient safety [SD = 2.013], and 11.20 [SD = 0.75] for teamwork/well-being/patient safety)). We excluded the low quality studies identified in this review at an early stage because the methodological description was insufficient for data extraction and assessment of quality (see Fig. 1).
Table 2.
Relationships between teamwork and well-being
| Study | Topic | Primary topic | Sample & setting | Design & data collection methods | Assessment of variables | Analyses | Findings | Outcomes & effect sizes | Quality scored |
|---|---|---|---|---|---|---|---|---|---|
| Bobbio et al., 2012 [38] | Mediation of relationship between empowering leadership/organizational support and burnout by trust in leader/organization | no | 273 nurses, general hospital, Italy | Cross-sectional self-report questionnaire | Team leadership: Empowering leadership scalea Well-being: Maslach Burnout Inventory (MBI)a | Path analysis | 1) Satisfactory model fit 2) Trust in leader mediates relationship leading by example and emotional exhaustion 3) Trust in leader mediates relationship between showing concern/ interacting with the team and a) emotional exhaustion b) cynicism 4) Trust in organization mediates relationship between informing and a) emotional exhaustion and b) cynicism 5) No mediation effects for reduced professional efficacy |
1) χ
2 (18) = 21.27, p = 0.27, χ
2/df = 1.18, RMSEA = 0.03, CFI = 1.00, SRMR = 0.02 Indirect effects: 2) β = −0.04, p < 0.05 3a) β = −0.23, p < 0.001 3b) β = −0.15, p < 0.001 4a) β = −0.03, p < 0.05 4b) β = −0.04, p < 0.02 5) NS |
11.5 (16) |
| Bratt et al., 2000 [39] | Relationships between nurse/unit characteristics, work environment and job satisfaction | no | 1973 nurses, 70 pediatric intensive care units, 65 pediatric hospitals, USA/Canada | Cross-sectional self-report questionnaire | Teamwork: a) Group cohesion: Group Judgment Scale b) Nurse-physician collaboration: Collaboration and Satisfaction about Care Decisionsa Well-being: Job Stress Scalea |
Pearson’s correlation | Job stress is negatively correlated with 1) group cohesion 2) nurse-physician collaboration |
1) r = −0.43, p < 0.001 2) r = −0.37, p < 0.001 |
9.5 (16) |
| Brunetto et al., 2011 [40] | Relationships between supervisor-subordinate relationship, teamwork, role ambiguity and well-being | yes | 1138 nurses, 3 public and 7 private urban and regional hospitals, Australia | Cross-sectional self-report questionnaire | Teamwork: Nurses’ Satisfaction with Teamwork Scale Well-being: Perception of Well-being Scale (self-developed) |
Pearson’s correlation | Positive correlation between nurses’ satisfaction with teamwork and well-being | Public sector: r = 0.35, p < 0.001 Private sector: r = 0.39, p < 0.001 |
9.5 (16) |
| Brunetto et al., 2013 [48] | Workplace relationships, engagement, well-being, commitment, and turnover | no | 1228 nurses, Australia / USA | Cross-sectional self-report questionnaire | Teamwork: Satisfaction with teamworka
Well-being: employee engagementa, well-being scale developed by first author |
Structural equation modeling (SEM) | Teamwork is positively associated with 1) engagement and 2) well-being in the a) Australian and b) US sample |
1a) B = .19, p < .001 1b) B = .24, p < .001 2a) β = .30, p < .001 2b) β = .37, p < .001 |
12 (16) |
| Bruyneel et al., 2009 [41] | Relationship between nurse working environment and nurse-perceived outcomes | no | 179 nurses, 12 units, 5 acute care hospitals, Belgium | Cross-sectional self-report questionnaire | Teamwork: Nursing Work Index-Revised (NWI-R)a subscale Nurse-Physician-Relations
Well-being: MBIa |
Multivariate logistic regression | Nurse-physician relations are not associated with emotional exhaustion | NS | 11.5 (16) |
| Budge et al., 2003 [20] | Relationships between nurses’ work characteristics, work relationships and health | no | 225 nurses, general hospitals, New Zealand | Cross-sectional self-report questionnaire | Teamwork: Nurse-Physician-Relations Scalea Well-being: Short-Form Health Survey (SF-36)a subscales mental health and vitality |
Pearson’s correlation | Positive correlation between nurse-physician relations and 1) mental health 2) vitality |
1) r = 0.29, p < 0.001 2) r = 0.36, p < 0.001 |
12.5 (16) |
| Cheng et al., 2013 [49] |
Relationships between team climate, emotional labor, burnout, quality of care, and turnover | no | 201 nurses, 1 hospital, Australia | Cross-sectional self-report questionnaire | Teamwork: Team Climate Inventory (TCI)a
Well-being: Oldenburg Burnout Inventory (OLBI)a |
Structural equation modeling | 1) Good overall model fit 2) Team climate is negatively associated with burnout |
1) χ
2 = 241.31; χ
2/df = 11.49; TLI = .95; CFI = .98; RMSEA = .051 2) β = −.37, p < .01 |
13 (16) |
| Gabriel et al., 2011 [18] | Collegial nurse-physician relations and psychological resilience moderate relationships between task accomplishment satisfaction and pre-/postshift affect | no | 57 nurses, 1 hospital, USA | Cross-sectional pen-and-paper diary-report | Teamwork: Nurse-Physician-Relations Scalea
Well-being: Affect scale, psychological resilience based upon Connor–Davidson Resilience Scale (CD-RISC)a |
Pearson’s correlation, multilevel modeling | 1) Nurse-physician relations are a) negatively correlated with preshift negative affect b) positively correlated with preshift positive affect 2) No correlations between nurse-physician-relations and psychological resilience 3) Nurse-physician relations a) negatively predict postshift negative affect b) positively predict postshift positive affect |
1a) r = 0.30, p < 0.05 1b) r = 0.33, p < 0.05 2) NS 3a) γ = −0.13, p < 0.01 3b) γ = 0.2, p < 0.01 |
12 (16) |
| Gevers et al., 2010 [54] | Relationship between acute/chronic job demands and acute job strain and relationship between the latter and individual teamwork behavior | yes | 48 nurses, nursing students and physicians, emergency department, The Netherlands | Cross-sectional self-report questionnaire | Teamwork and well-being: self-developed items adapted from existing measures | (Hierarchical) linear regression | 1) Acute a) cognitive strains b) emotional strains separately negatively predict individual teamwork behavior c) whereas physical strains do not 2) When all three predictors are analyzed simultaneously, only acute emotional strains remain significant |
1a) β = −0.35, p < 0.01, R
2 = 0.18, [f
2 = 0.22]b,c
1b) β = −0.44, p < 0.001, R 2 = 0.25, [f 2 = 0.33]b,c 1c) NS 2) β = −0.36, p < 0.05, R 2 = 0.26, [f 2 = 0.35]b,c, emotional & physical strains: NS |
13 (16) |
| Gunnarsdottir et al., 2009 [42] | Relationships between nurses’ work environment and work outcomes | no | 695 nurses, various specialties, university hospital, Iceland | Cross-sectional self-report questionnaire | Teamwork: Nurse-Physician-Relations Scalea
Well-being: Emotional Exhaustiona |
(Hierarchical) linear regression | 1) Nurse-physician relations are negatively associated with emotional exhaustion 2) Upon inclusion of four additional predictors, this association becomes non-significant |
1) β = −2.38, p < 0.001, []b
2) NS |
12.5 (16) |
| Kanai-Pak et al., 2008 [43] | Relationships between nurses’ work environment and work outcomes | yes | 5956 nurses, various specialties, 19 hospitals, Japan | Cross-sectional self-report questionnaire | Teamwork: Nurse-Physician-Relations Scalea
Well-being: Emotional Exhaustiona |
Multivariate logistic regression | Lower nurse-physician relations are associated with higher risk for emotional exhaustion | Adj. OR = 1.35, p < 0.05 | 10.5 (16) |
| Klopper et al., 2012 [44] | Relationships between nurses’ work environment, job satisfaction and burnout | no | 935 nurses, ICU, 62 hospitals, South Africa | Cross-sectional self-report questionnaire | Teamwork: Nurse-Physician-Relations Scalea
Well-being: MBIa |
Spearman’s rank correlation | 1) Negative correlation between nurse–physician relations and a) emotional exhaustion b) depersonalization 2) Positive correlation between nurse–physician relations and personal accomplishment |
1a) ρ = −0.255, p < 0.01 1b) ρ = −0.193, p < 0.01 2) ρ = 0.199, p < 0.01 |
8.5 (16) |
| Lehmann-Willenbrock et al., 2012 [45] | Mediation of relationships between appreciation of age diversity and nurse Well-being/team commitment by co-worker trust | yes | 138 nurses, 1 hospital, Germany | Cross-sectional self-report questionnaire | Teamwork: Team commitment scale Well-being: Workplace Irritation Scalea |
Pearson’s correlation | Negative correlation between team commitment and irritation | r = −0.33, p < 0.01 | 12.5 (16) |
| Li et al., 2013 [50] | Relationships between nurse work environment and burnout | no | 23 446 nurses, 2087 units, 352 hospitals, 11 European countries | Cross-sectional self-report questionnaire | Teamwork: Nurse-physician relationsa
Well-being: MBIa |
Multilevel regression | 1) As expected, nurse-physician relations on the a) unit, but not on the b) hospital or c) country level are negatively related to emotional exhaustion on the individual level 2) As expected, nurse-physician relations on the a) unit, but not on the b) hospital or c) country level are negatively related to depersonalization on the individual level 3) As expected, nurse-physician relations on the a) unit, but not on the b) hospital or c) country level are positively related to personal accomplishment on the individual level |
1a) B = −0.11; 95 % equal tail credibility interval (ETCI) -0.21 to −0.002 1b) NS 1c) NS 2a) B = −0.17; 95 % ETCI −0.27 to -.07 2b) NS 2c) NS 3a) B = 0.20; 95 % ETCI −0.29 to -.12 3b) NS 3c) NS |
13.5 (16) |
| Pisarski & Barbout, 2014 [37] | Relationships between team climate, roster control, work-life conflict and fatigue | yes | 166 nurses, 1 hospital, Australia | Longitudinal self-report questionnaire | Teamwork: 10 items adapted from teamwork climate measure developed by authors Well-being: 2 items from Standard Shiftwork Index (SSI) |
Multiple hierarchical regression | 1) Overall, team climate at time 1 does not predict fatigue at time 2 2) Team climate of day shift nurses is negatively related to fatigue |
1) NS 2) β = −.16, p < .05 |
13 (16) |
| Profit et al., 2013 [57] | Relationships between burnout and patient safety culture | yes | 2073 nurses and other healthcare professionals in 44 neonatal intensive care unit | Cross-sectional self-report questionnaire | Teamwork: Safety Attitudes Questionnaire (SAQ)a subscale teamwork climate
Well-being: 4-item version of MBIa |
Pearson correlation | Negative correlation between burnout and teamwork climate | r = −.38, p < .05 | 11 (16) |
| Rafferty et al., 2001 [46] | Relationship between interdisciplinary teamwork and nurse autonomy on patient and nurse outcomes and nurse assessed quality of care | yes | 5006 nurses, 32 hospitals, UK | Cross sectional self-report questionnaire | Teamwork: Items referring to teamwork on unit derived from NWI-Ra
Well-being: MBIa |
Pearson’s correlation | Negative correlation between teamwork and burnout | r = −0.219, p < 0.001 | 6.5 (16) |
| Raftopoulos et al., 2011 [53] | Relationships between safety and teamwork climate and stress | no | 106 midwives, public maternity units, Cyprus | Cross-sectional self-report questionnaire | Teamwork: Safety Attitudes Questionnaire (SAQ)a subscale teamwork climate
Well-being: job exhaustion, occupational stress (1 item each) |
Backward stepwise linear regression | 1) Job exhaustion negatively predicts teamwork climate (14 predictors altogether) 2) No association between teamwork and occupational stress |
1) β = −12.85, p = 0.046, R
2 = 0.117, [f
2 = 0.13]b,c
2) NS |
10 (16) |
| Rathert et al., 2012 [55] | Mediation of relationship between nurses’ work environment and workarounds by emotional exhaustion | no | 272 nurses & other medical care providers, acute care hospital, North America | Cross-sectional self-report questionnaire | Teamwork: 4 items from Agency for Healthcare Research and Quality (AHRQ) Patient Safety Culture Surveya
Well-being: Emotional Exhaustiona |
Path analysis | 1) Negative association between teamwork and emotional exhaustion within larger path model 2) Good final model fit |
1) β = −0.19, p < 0.01 2) GFI = 0.99, AGFI = 0.92, NNFI = 0.97, RMSEA = 0.06, χ 2 = 11.81 (df = 6) |
11.5 (16) |
| So et al., 2011 [56] | Cultural differences in relationships between team structure, job design, and Well-being | yes | 470 nurses & other medical care providers, acute hospitals, China & UK | Cross-sectional self-report questionnaire | Teamwork: items about team structure (roles, objectives, cooperation, performance reflection) Well-being: items about perceived work stress |
Path analysis | Negative association between team structure and work stress within larger path model 1) in the UK sample 2) but not in the Chinese sample 3) Good overall model fit |
1) β = −0.18, p < 0.05, R
2
all stress predictors = 0.302 2) NS 3) χ 2 = 787.94 (df = 246, p = 0.05), CFI = 0.91, NNFI = 0.91, RMSEA = 0.071, 90 % CI 0.065 – 0.076 |
12.5 (16) |
| Sutinen et al., 2005 [21] | Relationships between health, work and social characteristics and retirement attitudes | no | 447 physicians, several hospitals, Finland | Cross-sectional self-report questionnaire | Teamwork: TCIa
Well-being: General Health Questionnaire (GHQ-12)a |
Pearson’s correlation | Negative correlation between teamwork and minor psychiatric morbidity | r = −0.12, p < 0.05 | 10.5 (16) |
| Van Bogaert et al., 2009 [47] | Mediation of relationships between nurse work environment and nurse job outcomes and quality of care by burnout | no | 401 nurses, medical, 31 units, general and university hospital, Belgium | Cross-sectional self-report questionnaire | Teamwork: Nurse-Physician-Relations Scalea
Well-being: MBIa |
Pearson’s correlation Path analysis |
1) Negative correlation between nurse-physician relationship and a) depersonalization b) personal accomplishment 2) Within path model: negative association between nurse-physician relationship and emotional exhaustion 3) Adequate overall model fit |
1a) r = 0.155, p < 0.05 1b) r = −0.115, p < 0.01 2) β = −0.19 3) χ 2 = 548.1, df = 313, p < 0.001, CFI = 0.906, IFI = 0.903, RMSEA = 0.43 |
11.5 (16) |
| Van Bogaert et al., 2010 [19] | Relationships between nurse work environment, nurse job outcomes, quality of care, and burnout | no | 546 nurses, 42 units, general and university hospitals, Belgium | Cross-sectional self-report questionnaire | Teamwork: Nurse-Physician-Relations Scalea
Well-being: MBIa |
Linear mixed effects multilevel model | 1) Positive association between nurse-physician relationship and personal accomplishment 2) Negative association between nurse-physician relationship and a) emotional exhaustion b) depersonalization |
1) β = 1.98, p < 0.0001 2a) β = −3.79, p < 0.0001 2b) β = −1.09, p < 0.05 |
11.5 (16) |
| Van Bogaert et al., 2013 [52] | Relationships between nurse work environment, nurse characteristics, burnout, nurse job outcomes, and quality of care | no | 1201 nurses, 116 units, 8 hospitals, Belgium | Cross-sectional self-report questionnaire | Teamwork: nurse-physician relations subscale of NWIa
Well-being: MBIa |
Structural equation modelling (SEM) | 1) Satisfactory overall model fit 2) No relationship between nurse-physician relations and emotional exhaustion 3) Negative correlation between nurse-physician relations and depersonalization but no relationship in final SEM 4) Positive correlation between nurse-physician relations and personal accomplishment but no relationship in final SEM |
1) CFI = .90, IFI = .90, RMSEA = .43 2) NS 3) r = −.08, p < .01 4) r = .11, p < .01 |
13 (16) |
| Van Bogaert et al., 2014 [51] | Relationships between role-, job- and organizational characteristics, and occupational stress and well-being | no | 365 nurse unit managers, Belgium | Cross-sectional self-report questionnaire | Teamwork: nurse-physician relations subscale of Leiden Quality of Work Questionnaire for Nurses (LQWQ-N)a Well-being: emotional exhaustion subscale from MBIa; Utrecht Work Engagement Scale (UWES)a |
Hierarchical multiple regression | 1) Nurse-physician relations negatively predict emotional exhaustion 2) Nurse-physician relations do not predict work engagement |
1) β = −.22, p < .01 2) NS |
14 (16) |
We report not only significant but also non-significant relationships between predictor and outcome variables of interest in this review as hypothesized in the reviewed studies; even if not explicitly stated in the original publication
avalidated instrument
beffect sizes calculated by authors, calculation not possible if brackets empty
cCohen’sƒ 2 based on R2 instead of ΔR2
din brackets: maximal possible score
Table 3.
Relationships between teamwork and patient safety
| Study | Topic | Primary topic | Sample & setting | Design & data collection methods | Assessment of variables | Analyses | Findings | Outcomes & effect sizes | Quality scored |
|---|---|---|---|---|---|---|---|---|---|
| a) observational studies | |||||||||
| Burtscher et al., 2010 [61] | Relationships between coordination activities and team performance under differing situational demands | yes | 19 anesthetists and 14 anesthesia nurses, 40 cases, teaching hospital, Switzerland | Video observation of anesthesia induction | Teamwork: observation system used for coding coordination activities & clinical work Patient safety: team performance (self-developed checklist) |
Paired-sample t-test | 1) Compared to low-performing teams, high-performing teams increase task management during non-routine events 2) No changes in information management during non-routine events |
1) t(20) = −2.75, p < 0.05, []b
2) NS |
13.5 (15) |
| Burtscher et al., 2011 [12] | Relationships between adaptive team coordination during non-routine events and clinical performance during anesthesia induction | yes | 15 anesthesia teams (1 resident, 1 nurse), teaching hospital, Switzerland | Video observation of simulated anesthesia induction | Teamwork: team coordination (structured observation)a
Patient safety: decisions and execution latency (expert rating) |
Pearson’s correlation | 1) Information management is a) negatively correlated with decision latency b) but not with execution latency 2) No correlations between task management and a) decision latency b) execution latency |
1a) r = −0.49, p = 0.003 1b) NS 2a) NS 2b) NS |
12.5 (15) |
| Burtscher et al., 2011 [5] | Team mental model properties moderate link between monitoring behaviors and performance in anesthesia induction | yes | 31 teams (1 anesthesia resident, 1 anesthesia nurse), teaching hospital, Switzerland | Video observation of simulated anesthesia induction | Teamwork: Team mental model similarity and accuracy (concept mapping), monitoring behavior (structured observationa) Patient safety: adherence to anesthesia induction protocol (structured observationa) |
Multiple hierarchical regression | 1) Teams with similar mental models perform well irrespective of team monitoring level; teams with dissimilar mental models only perform well when team monitoring is low 2) Team mental model similarity is only related to performance when team mental model accuracy is also high 3) Team performance is high when either team or system monitoring is high and the other is low 4) Mental model accuracy does not moderate relationship between systems monitoring and performance |
1) β = 0.36, p = 0.04, ΔR
2 = 0.13, [ƒ
2 = 0.21]b
2) β = 0.42, p = 0.02, ΔR 2 = 0.17, [ƒ 2 = 0.12]b 3) β = −0.36, p = 0.04, ΔR 2 = 0.12, [ƒ 2 = 0.28]b 4) NS |
14 (15) |
| Catchpole et al., 2007 [64] | Relationships between non-technical skills and adverse events in the OR | yes | 42 operations (24 pediatric, 18 orthopedic), 2 hospitals, UK | Live & video observation | Teamwork: non-technical skills (NOTECHSa) Patient safety: Adverse events: minor problems, intraoperative performance, operating time |
Multiple linear regression | Non-technical skills negatively predict 1) minor problems but not 2) intraoperative performance or 3) operating time |
1) B = −3.3, t = −2.2, p = 0.035, []b
2) NS 3) NS |
8 (15) |
| Catchpole et al., 2008 [62] | Relationships between non-technical skills and errors in the OR | yes | 54 surgeons, anesthetists, and nurses, 48 operations (26 laparoscopic cholecystectomies, 22 carotid endarterectomies), 1 hospital, UK | Live observation of operation | Teamwork: NOTECHSa
Patient safety: errors in surgical technique (observation clinical human reliability assessment technique), other procedural problems and errors (checklist), operating time |
Multiple linear regression | 1a) Surgical leadership and management negatively predicts operating time, 1b) whereas anesthetic leadership and management in carotid endarterectomy positively predicts operating time 2a) nursing leadership and management negatively predict other procedural problems and errors 2b) whereas nursing leadership and management in carotid endarterectomy positively predicts operating time (2 predictors) 3a) surgical situation awareness negatively predicts errors in surgical techniques (3 predictors) 3b) whereas surgical situation awareness in carotid endarterectomy positively predicts operating time (3 predictors) 4) Teamwork dimensions a) leadership and management b) teamwork and cooperation c) problem solving and decision making d) situation awareness are not associated with patient safety dimensions e) errors in surgical technique f) other procedural problems and error g) operating time |
1a) β = −0.19, p = 0.023 1b) β = 0.81, p < 0.001, R 2 = 0.717, [ƒ 2 = 2.53]b,c 2a) β = −0.39, p = 0.012 2b) β = 0.41, p = 0.008, R 2 = 0.69 [ƒ 2 = 2.215]b,c 3a) β = −0.71, p < 0.001 3b) β = 1.97, p < 0.001, R 2 = 0.19, [ƒ 2 = 0.233]b,c 4ae-dg) 9 non-significant associations |
9 (15) |
| Catchpole et al., 2008 [63] | Relationships between non-technical skills and safety threats, errors, and operative duration | yes | Physicians and nurses, 44 operations (24 pediatric, 20 orthopedic), 2 hospitals, UK | Live & video observation | Teamwork: NOTECHSa
Patient safety: errors & threats (checklists and free observations) |
Spearman’s rank correlation | 1) Positive correlation between non-technical skills and 1a) safety threats 1b) operative duration 1c) but not technical errors in pediatric surgery 2) No correlations between non-technical skills and 1a) safety threats 1b) operating time 1c) technical errors in orthopedic surgery |
1a) ρ = 0.58, p < 0.005 1b) ρ = 0.58, p < 0.005 1c) NS 2a) NS 2b) NS 2c) NS |
10 (15) |
| Endacott et al., 2014 [81] | Relationships between leadership, teamwork and performance in medical emergencies | yes | 42 nurses, 15 teams, 1 hospital, Australia | Video observation of simulated emergency | Teamwork: Team Emergency Assessment Measure (TEAM) a
Patient safety: performance of key treatment actions |
Pearson correlation | Teamwork correlates positively with patient safety in the 1) respiratory distress and 2) hypovolemic shock but not in the 3) chest pain scenario |
1) r = .90, p < 0.001 2) r = .54, p < .05 3) NS |
11.5 (15) |
| Kolbe et al., 2012 [65] | Relationships between speaking up and technical team performance/team interaction | no | 31 anesthesia teams (1 nurse, 1 resident), teaching hospital, Switzerland | Video observation of simulated anesthesia induction | Teamwork: Coding scheme for (non-)verbal team interactions Patient safety: technical team performance (adherence to checklist of standard anesthesia induction and target values) |
Hierarchical linear regression | 1) Technical team performance is predicted by nurses’ levels of speaking up 2) but not by residents’ levels of speaking up |
1) β = 0.43, p = 0.017, R
2 = 0.18, [f
2 = 0.22]bc (2 predictors) 2) NS |
14 (15) |
| Kuenzle et al., 2010 [67] | Relationship between shared leadership and anesthesia team performance under high and low task load | yes | 12 anesthesia teams (1 resident, 1 nurse), teaching hospital, Switzerland | Video observation of simulated anesthesia induction | Teamwork: Coding scheme for content-oriented and structuring leadership behavior Patient safety: performance (reaction time after non-routine event) |
ANOVA | 1a) No differences in shared leadership behaviors of high-performing teams between nurses and residents 1b) during high- and low task load situations 2a) Residents show more leadership behaviors than nurses in low performing teams 2b) independent of task load |
1a) F(1, 20) = 0.00, p = 0.971, η2 = 0.000 1b) Interaction: NS 2a) F(1, 20) = 7.14, p = 0.015, η2 = 0.263 2b) Interaction: NS |
12.5 (15) |
| Kuenzle et al., 2010 [66] | Relationship between shared leadership and anesthesia team performance under high and low task load | yes | 12 anesthesia teams (1 resident, 1 nurse), 1 hospital, Switzerland | Video observation of simulated anesthesia induction | Teamwork: structuring and content oriented leadership: structured observation Patient safety: performance (speed of correct management after non-routine event = high task load) |
Spearman’s rank correlation Kruskal-Wallis-test |
1) Under high task load team performance and a) structuring and b) content-oriented leadership are not correlated 2) Under low task load, team performance and a) structuring, b) but not content-oriented leadership are negatively correlated 3) Interaction of leadership behavior and team experience is not associated with team performance |
1a) NS 1b) NS 2a) ρ = −0.56, p < 0.05 2b) NS 3) NS |
12 (15) |
| Lubbert et al., 2009 [68] | Relationship between team organization and treatment errors | yes | 378 video registrations of patients treated in the emergency room, 1 hospital, The Netherlands | Video observation | Teamwork & patient safety: Self-developed checklist measuring adherence to advanced trauma life support (ATLS) guidelines | t-test | 1) Errors in team organization dimension evident leadership are associated with more deviations from treatment protocol, whereas 2) errors in team organization dimension effective leadership are not |
1) p = 0.01 (no other indicators reported) 2) NS |
6 (15) |
| Manser et al., 2009 [11] | Relationships between different coordination patterns and team performance | yes | 46 anesthesia residents, 23 teams, USA | Video observation of simulated anesthesia emergency | Teamwork: self-developed coding scheme for coordination Patient safety: clinical performance (adherence to malignant hyperthermia treatment guidelines) |
Hierarchical regression analysis | 1) Time spent on coordination dimensions a) task management b) but not information management c) or coordination via work environment negatively predicts performance 2) Time spent on task management categories a) task distribution b) but not planning c) clarification d) initiating action e) or assistance negatively predicts performance 3) Time spent on information management categories a) situation assessment b) but not information transfer c) decision making d) or feedback/acknowledgement negatively predicts performance |
1a) β = −0.47, p < 0.01, ΔR
2 = 0.243, [f
2 = 0.32]b
1b) NS 1c) NS 2a) β = −0.54, p < 0.01, ΔR 2 = 0.340, [f 2 = 0.52]b 2b) NS 2c) NS 2d) NS 2e) NS 3a) β = −0.57, p < 0.05, ΔR 2 = 0.227, [f 2 = 0.29]b 3b) NS 3c) NS 3d) NS |
11.5 (15) |
| McCulloch et al., 2009 [6] | Relationships between non-technical skills and technical errors | yes | 54 surgeons, anesthetists and nurses, 48 observations before and 55 observations after training, teaching hospital, UK | Uncontrolled pre-post-training Live observations of operations |
Teamwork: NOTECHSa
Patient safety: technical errors (Observation Clinical Human Reliability Assessment, OCHRA)a |
Spearman’s rank correlation | 1) Negative correlation between a) overall non-technical skills and technical errors b) especially for surgical sub-team 2) Negative correlation between a) situational awareness and technical errors b) especially for surgical sub-team |
1a) ρ = −0.215, p = 0.024 1b) ρ = −0.236, p = 0.013 2a) ρ = −0.300, p = 0.001 2b) ρ = −0.436, p < 0.0001 |
11.5 (18) |
| Mishra et al., 2008 [69] | Relationships between non-technical skills and technical errors | yes | 26 observations (nurses, surgeons, anesthetists), teaching hospital, UK | Live observation of operation | Teamwork: NOTECHSa
Patient safety: OCHRAa |
Spearman’s rank correlation | 1) No correlation between technical errors and a) leadership & management b) teamwork & cooperation c) problem-solving and decision-making in the d) overall team, or e) surgeon f) anesthetists g) and nurses subgroup 2) Negative correlation between situation awareness and technical errors for a) overall team b) surgeon subgroup c) but not anesthetists d) and nurses subgroup |
1ad) NS 1ae) NS 1af) NS 1ag) NS 1bd) NS 1be) NS 1bf) NS 1bg) NS 1 cd) NS 1ce) NS 1cf) NS 1cg) NS 2a) ρ = −0.505, p = 0.009 2b) ρ = −0.718, p = 0.001 2c) NS 2d) NS |
10 (15) |
| Ottestad et al., 2007 [70] | Development and psychometric testing of tool to measure resuscitative skills and to compare interns and teams regarding ideal management of septic shock | no | 23 observations (ICU residents), USA | Video observation of emergency simulation | Teamwork: NOTECHSa
Patient safety: Adherence to Surviving Sepsis Campaign Guidelines |
Pearson’s correlation | Positive correlation between non-technical skills and team sepsis management | r = 0.4, p = 0.05 | 7.5 (15) |
| Schmutz et al., 2015 [79] | Relationships between coordination, task type and performance in medical emergencies | yes | 277 nurses, resident and senior physicians, 68 teams, 7 hospitals, Germany | Video observation of simulated pediatric emergency | Teamwork: Coordination behaviors via CoMeT–E (Coordination System for Medical Teams - Emergency) observation toola
Patient safety: Clinical performance via key treatment steps checklist |
Hierarchical linear regression | 1a) Coordination behavior closed-loop communication is positively associated with clinical performance, whereas 1b) coordination behaviors task distribution and 1c) providing information without request are not. 2a) Task type moderates relationship 1a) in that it is stronger in rule-based compared to knowledge-based tasks 2b) Task type did not moderate relationship 1b) 2c) Task type did not moderate relationship 1c) |
1a) β = .25, p < .05 1b) NS 1c) NS 2a) β = −.52, p < .01 2b) NS 2c) NS |
14 (15) |
| Schraagen et al., 2011 [85] | Relationships between non-routine events, teamwork and patient outcomes | yes | 1 pediatric cardiac surgery team, 40 operations, The Netherlands | Cross-sectional self-report questionnaire, live observation of operations, record review | Teamwork: observation tool derived from NOTECHSa, ANTSa, NOTSSa, and OTASa
Patient safety: 30-day postsurgical complications, operating time |
Pearson’s correlation, ANOVA |
1) Positive correlation between non-technical skills and a) operating time b) but not postsurgical complications 2) Explicit coordination of anesthetists is associated with higher levels of postsurgical complications |
1a) r = 0.45, p < 0.05 1b) NS 2) M uncomplicated = 12.88, M minor complications = 21.55, []b M major complications = 16.40, F(2,36) = 4.78, p < 0.01, []b |
10 (16) |
| Schraagen et al., 2011 [86] | Relationships between non-routine events, teamwork and patient outcomes | yes | 1 pediatric cardiac surgery team, 40 operations, The Netherlands | Cross-sectional self-report questionnaire, live observation of operations, record review | Teamwork: NOTECHSa
Patient safety: 30-day postsurgical complications |
Pearson’s correlation, ANOVA |
Teamwork and cooperation is associated with higher levels of postsurgical complications | M uncomplicated = 3.19, M minor complications = 3.44, M major morbidity = 3.28, F(2,36) = 3.85, p < 0.05, η2 = 0.18 | 8.5 (16) |
| Siassakos et al., 2010 [80] | Relationships between individual team members’ knowledge, skills, and attitudes and team performance | no | 19 teams (physicians and midwives), 6 maternity units, UK | Video observation of obstetric emergency simulation, self-report questionnaire | Teamwork: SAQ subscale team climatea
Patient safety: team performance (magnesium administration) |
Kendall’s rank correlation | No correlation between teamwork climate and performance | NS | 8 (16) |
| Siassakos et al., 2011 [72] | Relationships between teamwork skills and behaviors and team performance in emergency situations | yes | 47 teams (2 physicians and 4 midwives each), 6 maternity units, UK | Video observation | Teamwork: Team analytical toola
Patient safety: performing key actions |
Kendall’s rank correlation | 1) Positive correlation between speed of magnesium administration and a) skills b) behavior c) and overall teamwork 2) Negative correlation between time needed to put patient in recovery position and a) skills b) behavior c) but not overall teamwork 3) Negative correlation between time needed to administer oxygen and a) skills b) behavior c) and overall teamwork 4) Negative correlation between time needed to sample blood and a) skills b) behavior c) and overall teamwork |
1a) τ = 0.54, p < 0.001 1b) τ = 0.41, p = 0.001 1c) τ = 0.51, p < 0.001 2a) τ = −0.29, p = 0.012 2b) τ = −0.25, p = 0.026 2c) NS 3a) τ = −0.39, p < 0.001 3b) τ = −0.28, p = 0.014 3c) τ = −0.41, p < 0.001 4a) τ = −0.35, p = 0.002 4b) τ = −0.35, p = 0.002 4c) τ = −0.35, p < 0.002 |
8.5 (15) |
| Siassakos et al., 2011 [71] | Relationships between teamwork and clinical efficiency in emergency situations | yes | 114 physicians and nurses, 19 teams, 6 maternity units, UK | Video observation | Teamwork: self-developed observation system Patient safety: performing key action (speed of magnesium administration) |
Kendall’s rank correlation | 1) Positive correlation between closed-loop communication and clinical efficiency 2) Positive correlation between unambiguous communication and clinical efficiency 3) No correlations between clinical efficiency and a) SBAR communication style b) team coordination c) situational awareness d) leadership style e) supportive language f) task support by senior clinician |
1) τ = 0.46, p = 0.022 2) τ = 0.53, p = 0.004 3a) NS 3b) NS 3c) NS 3d) NS 3e) NS 3f) NS |
8 (15) |
| Thomas et al., 2006 [73] | Relationship between teamwork and quality of care | yes | 118 teams (physicians, nurses, respiratory therapists), resuscitation room, teaching hospital, USA | Video observation of neonatal resuscitation | Teamwork: Frequency of different teamwork behaviors Patient safety: Neonatal Resuscitation Program (NRP) Guidelines |
Spearman’s rank correlation | 1) Negative correlation between team communication and a) overall quality of resuscitation, b) non-compliance with all NRP steps, and c) non-compliance during preparation and initial steps 2) Negative correlation between team management and a) noncompliance with all NRP steps, and b) noncompliance during preparation and initial steps but not c) overall quality of resuscitation, 3) Negative correlation between team leadership and a) overall quality of resuscitation, but not with b) noncompliance with all NRP steps, and with c) non-compliance during preparation and initial steps |
1a) ρ = −0.236, p = 0.007 1b) ρ = −0.214, p = 0.014 1c) ρ = −0.230, p = 0.008 2a) ρ = −0.201, p = 0.021 2b) ρ = −0.252, p = 0.003 2c) NS 3a) ρ = −0.288, p < 0.001 3b) NS 3c) NS |
9.5 (15) |
| Tschan et al., 2006 [74] | Relationships between directive leadership, structuring inquiry and performance regarding different phases | yes | 109 clinicians (nurses, residents, senior physicians), 21 teams, ICU, university hospital, Switzerland | Video observation and transcription of emergency simulation | Teamwork: directive leadership and structuring inquiry Patient safety: clinical performance (key actions, hands-on time) |
Pearson’s correlation | 1) Phase 1 (nurses only): positive correlation between performance and a) directive leadership and b) structuring inquiry 2) Phase 2 (residents and nurses): positive correlation between performance and a) resident directive leadership during first 30 s, no correlation between performance and b) resident directive leadership per second c) resident structuring inquiry per second d) resident structuring inquiry during first 30 s 3) Phase 3 (nurses, residents, senior physicians): positive correlation between performance and a) senior physician structuring inquiry, no correlation between performance and b) resident structuring inquiry c) senior physician d) resident directive leadership |
1a) r = 0.445, p < 0.05 1b) r = 0.216, p < 0.05 2a) r = 0.522, p < 0.05 2b) NS 2c) NS 2d) NS 3a) r = 0.428, p < 0.01 3b) NS 3c) NS 3d) NS |
11.5 (15) |
| Tschan et al., 2009 [75] | Relationships between team communication and perceptual biases of individuals and accuracy of diagnosis | yes | 53 physicians, 20 teams, university hospital, Switzerland | Video observation of hand-over simulation | Teamwork: coding of communication and behavior Patient safety: diagnostic performance |
ANOVA | 1) Groups considering more diagnostic information are not more likely to find the correct diagnosis 2) Groups showing a) more explicit reasoning b) more talking to the room are more likely to find the correct diagnosis |
1) NS 2a) F(2, 15) = 5.750, p = 0.014 2b) χ 2 = 8.598, df = 2, p = 0.007 |
11 (15) |
| Westli et al., 2010 [76] | Relationship between teamwork skills/shared mental models and clinical performance | yes | 27 trauma teams, Norway | Video observation of emergency simulations | Teamwork: ANTSa and Anti-Air Teamwork Observation Measure (ATOM) Patient safety: Team global medical management, key actions of trauma management |
Pearson’s correlation | 1) Negative correlation between supporting behavior and performing key actions 2) Negative correlation between poor coordination and medical management 3) Positive correlation between information exchange and medical management 4) Negative correlation between poor situational awareness and performing key actions 5) Positive correlation between providing information and medical management 6a-u) 21 non-significant correlations between teamwork and patient safety variables |
1) r = −0.37, p < 0.05 2) r = −0.36, p < 0.05 3) r = 0.34, p < 0.05 4) r = −0.40, p < 0.05 5) r = 0.51, p < 0.01 6a-u) NS |
10.5 (15) |
| Wiegmann et al., 2007 [77] | Relationship between (teamwork-related) surgical flow disruptions and surgical error | yes | 31 cardiac operations, 1 hospital, USA | Live observation of operation | Teamwork: teamwork-related surgical flow disruptions Patient safety: surgical errors |
Multiple regression | Teamwork-related surgical flow disruptions positively predict surgical errors | β = 0.692, p < 0.001, adj. R
2 = 0.553, [f
2 = 1.24]bc
(5 predictors altogether) |
11 (15) |
| Williams et al., 2010 [78] | Relationships between teamwork behaviors and resuscitation errors | yes | 12 resuscitation teams, NICU, teaching hospital, USA | Video observation of resuscitation | Teamwork: frequency of different teamwork behaviors Patient safety: Neonatal Resuscitation Program (NRP) Guidelines |
Spearman’s rank correlation, generalized linear mixed model (GLM) | 1) Negative correlation between vigilance and NRP errors 2) No correlation between workload management and NRP errors 3) NRP errors are associated with a) more assertions before the error b) less teaching after the error 4) No associations between NRP errors and a) information sharing before error b) information sharing after error c) inquiry before error d) inquiry after error e) assertion after error f) teaching before error |
1) ρ = −0.62, p = 0.031 2) NS 3a) OR = 1.44, p = 0.008, 95 % CI 1.10 – 1.89 3b) OR = 0.59, p = 0.028, 95 % CI 0.37 – 0.94 4a) NS 4b) NS 4c) NS 4d) NS 4e) NS 4f) NS |
10 (15) |
| b) survey studies | |||||||||
| Brewer, 2006 [87] | Relationships between culture, team characteristics/processes and patient safety/hospital financial performance | yes | 430 nurses, physicians and other medical care providers, 16 surgical units, 4 acute care hospitals, USA |
Cross-sectional self-report questionnaire, record review |
Teamwork: Positive team processes: Relational Coordination Scalea Negative team processes scale Patient safety: patient falls (incident reporting system), length of stay (hospital records) |
Pearson’s correlation | 1) Positive intra-team processes correlate positively with a) length of stay b) but not with patient falls 2) No correlation between negative team processes and a) length of stay b) patient falls |
1a) r = 0.59, p < 0.05 1b) NS 2a) NS 2b) NS |
10 (16) |
| Chan et al., 2011 [88] | Validity of a team-based tool to assess success of a team-based intervention to reduce central line associated blood stream infections (CLABSI) | no | 46 ICUs, 35 hospitals, USA | Secondary analyses of longitudinal RCT, self-report questionnaire, record review | Teamwork: Team check-up tool (TCT) Patient safety: Central line associated bloodstream infections (CLABSI) |
Cox regression | No association between teamwork and duration to reach zero CLABSI’s after intervention | NS | 10 (19) |
| Chang & Mark, 2009 [89] | Antecedents (teamwork, nurse & patient factors) of severe and non-severe medication errors | yes | 1 671 nurses, 279 units, 146 hospitals, USA | Longitudinal self-report questionnaire, record review | Teamwork: Relational Coordination Scalea
Patient safety: medication errors (hospital incident reports) |
Generalized estimating equations (GEE) | Relational coordination predicts neither 1) severe nor 2) non-severe medication errors |
1) NS 2) NS |
9 (16) |
| Edmondson, 2004 [10] | Relationship between team/organizational characteristics, team leadership and medication errors | yes | 159 nurses, physicians and pharmacists, 8 hospitals, USA | Cross-sectional self-report questionnaire, record review | Teamwork: Team/organizational characteristics and team leadership (self-developed questionnaire) Patient safety: medication error (hospital incident reports & self-reported) |
Spearman’s rank correlation | Positive correlation between 1) nurse manager coaching 2) nurse manager direction setting and 3) unit relationship quality and a) detected and b) intercepted medication errors but not with c) non-preventable drug complications |
1a) ρ = 0.74, p < 0.03 1b) ρ = 0.71, p < 0.03 1c) NS 2a) ρ = 0.74, p < 0.03 2b) ρ = 0.83, p < 0.03 2c) NS 3a) ρ = 0.74, p < 0.03 3b) ρ = 0.76, p < 0.03 3c) NS |
11 (16) |
| Fasolino et al., 2012 [90] | Relationships between nurse characteristics, nurse practice environment, team member effectiveness and medication error | yes | 163 nurses, 11 surgical units, 1 hospital, USA | Cross-sectional self-report questionnaire, record review | Teamwork: team member effectiveness survey Patient safety: medication errors (hospital incident reports) |
Spearman’s rank correlation | Team member effectiveness is positively correlated with medication error | ρ = 0.19, p < 0.01 | 12 (16) |
| Hoffer Gittell et al., 2000 [9] | Relationship between relational coordination and quality of care/length of stay | yes | 338 physicians, nurses, and other medical care providers, 9 hospitals, USA | Cross-sectional self-report questionnaire, record review | Teamwork: Relational Coordination Scalea
Patient safety: Length of stay |
Hierarchical linear regression | Relational coordination is associated with decreased length of stay | B = −53.77, p < 0.001, []b | 13 (16) |
| Hwang & Ahn, 2015 [83] | Relationships between teamwork and error reporting | yes | 576 nurses, 2 acute care hospital, South Korea | Cross-sectional self-report questionnaire | Teamwork: Teamwork perceptions questionnaire (TPQ)a
Patient safety: occurrence of and reporting medical errors |
Logistic regression | Teamwork dimensions 1) team structure, 2) team leadership, 3) situation monitoring, 4) mutual support, and 5) communication are positively associated with error reporting No information on relationship between teamwork and occurrence of medical errors |
1) OR = 0.92, 95 % CI 0.50 –1.692) OR = 1.13, 95 % CI 0.78 –1.623) OR = 0.96, 95 % CI 0.52 – 1.78 4) OR = 1.23, 95 % CI 0.66 – 2.30) 5) OR = 1.82, 95 % CI 1.05 - 3.14 |
12.5 (16) |
| Kalisch & Lee, 2010 [60] | Relationship between teamwork and missed nursing care | yes | 2216 nurses, 40 acute care units, 4 hospitals, USA | Cross-sectional self-report questionnaire | Nursing Teamwork Surveya MISSCARE Surveya | Pearson’s correlation Multiple linear regression |
1) Negative correlation between missed nursing care and a) trust b) team orientation c) backup behavior d) shared mental model e) team leadership 2) After controlling for various covariates, overall teamwork scores negatively predict missed nursing care |
1a) r = −0.31, p < 0.01 1b) r = −0.28, p < 0.01 1c) r = −0.31, p < 0.01 1d) r = −0.32, p < 0.01 1e) r = −0.29, p < 0.01 2) B = −0.254, p < 0.001, ΔR 2 = 10.9, [f 2 = 0.124]b |
12.5 (16) |
| Leroy et al., 2012 [8] | Mediation and moderation relationships between leader behavioral integrity for safety, team psychological safety, team priority of safety, and treatment errors | yes | 580 nurses and head nurses, 4 hospitals, Belgium | Longitudinal self-report questionnaire | Teamwork: Team Psychological Safety Scalea
Patient Safety: head nurses’ reports of treatment errors |
Path analysis | 1) Good overall model fit 2) Within path model, team psychological safety at time 1 positively predicts treatment errors at time 2 |
1) χ
2 = 6.72, p = 0.03, SRMR = 0.07, RMSEA = 0.02, CFI = 0.98 2) β = 0.28, p = 0.02 |
14 (16) |
| Manojlovich et al., 2007 [82] | Relationships between perceived work environments, nurse-physician communication and patient outcomes | yes | 462 nurses, 25 ICUs, 8 hospitals, USA | Cross-sectional self-report questionnaire | Teamwork: parts of ICU Nurse-Physician Questionnairea
Patient safety: nurse-reported adverse events (medication errors, ventilator-associated pneumonia, catheter-associated sepsis) |
Random intercept multilevel models | Nurse-physician communication negatively predicts 1) ventilator-associated pneumonia 2) catheter-associated sepsis and 3) medication errors |
1) B = −0.045, p < 0.05, R
2 = 0.09, [f
2 = 0.1]b,c
2) B = −0.049, p < 0.05, R 2 = 0.14, [f 2 = 0.16]b,c 3) B = −0.047, p < 0.01, R 2 = 0.11, [f 2 = 0.12]b,c |
|
| Manojlovich et al., 2009 [91] | Relationship between nurse-physician communication and patient outcomes | yes | 462 nurses, 25 ICUs, 8 hospitals, USA | Cross-sectional self-report questionnaire, record review | Teamwork: ICU Nurse-Physician Questionnairea Patient safety: adverse outcomes ventilator-associated pneumonia, bloodstream infections, and pressure ulcers | Pearson’s correlation | No correlation between nurse-physician communication subscales 1) timeliness 2) accuracy 3) openness and 4) understanding and patient safety indicators a) ventilator-associated pneumonia b) bloodstream infections and c) pressure ulcers |
1a-4c) 12 non-significant associations | 11 (16) |
| Ogbolu et al., 2015 [84] | Relationships between nurse work environment and patient safety | no | 222 nurses, Nigeria | Cross-sectional self-report questionnaire | Teamwork: nurse-physician relationsa
Patient safety: Patient safety: one item from AHRQa |
Generalized linear mixed modeling | Relationship between nurse-physician relations and patient safety not reported (only relationship between aggregate NWI scale and patient safety) | - | 10 (16) |
| Taylor et al., 2012 [92] | Relationships between safety climate, teamwork and patient adverse events | no | Nurses in 29 units, 1 hospital, USA | Cross-sectional & longitudinal self-report questionnaire, record review | Teamwork: SAQ subscale team climatea
Patient safety: patient falls & injuries, deep vein thrombosis and pulmonary embolism records |
Multilevel logistic regression | Positive team climate is associated with 1) fewer decubitus ulcers, but not 2) less patient falls & injuries or 3) pulmonary embolisms and deep vein thrombosis one year later |
1) OR = 0.56, 95 % CI 0.30 - 0.82, p < 0.01 2) NS 3) NS |
13.5 (16) |
| Vogus et al., 2007 [93] | Moderation of relationship between team safety organizing behaviors and medication errors by trust in manager and existence of care pathways | yes | 1033 nurses & 78 nurse managers, 78 units, 10 acute-care hospitals, USA | Cross-sectional self-report questionnaire, record review | Teamwork: Safety Organizing Scale (SOS)a
Trust in manager: 2 items Care pathways: 1 item Patient safety: medication errors (number of errors reported to unit’s incident reporting system up to 6 months after survey data collection) |
Multilevel Poisson regression | 1) Safety organizing negatively predicts medication errors 2) Trust in manager has no impact on reporting of medication errors when level of safety organizing is high. When safety organizing is low and trust in manager is high, more errors are reported 3) Use of care pathways has no impact on reporting of medication errors when safety organizing is low. When safety organizing is high and care pathways are extensively used, fewer errors are reported |
1) β = −0.29, p < 0.01, 95 % CI −0.57 to −0.01 2) β = −0.68, p < 0.001, 95 % CI −1.03 to −0.32 3) β = −0.82, p < 0.001, 95 % CI −1.31 to −0.33 |
13 (16) |
| Wheelan et al., 2003 [94] | Relationship between teamwork and patient mortality | yes | 349 healthcare providers, 17 ICUs, 9 hospitals, USA | Cross-sectional self-report questionnaire, record review | Teamwork: Group Development Questionnairea
Patient safety: Standardized mortality rates |
Pearson’s correlation | Level of group development correlates negatively with mortality rates | r = −0.66, p = 0.004 | 12 (16) |
| Yun et al., 2005 [95] | Moderation of relationship between contingent leadership and team effectiveness by severity of patient trauma and team experience | yes | 91 members of trauma resuscitation teams, 1 hospital, USA | Cross-sectional self-report questionnaire, scenario method | Teamwork & patient safety: Team Effectiveness Scalea, Team leadership, severity of trauma and team experience manipulated across scenarios |
General linear model (GLM) | 1) Interaction of leadership/severity of injury: Team effectiveness dimension quality health care is high when patient was not severely injured/leadership is empowering or patient was severely injured/leadership was directive 2) Interaction of leadership/team experience: quality health care is highest when leadership is empowering, independent of team experience 3) 3-way-interaction: quality health care is highest when team is experienced and leadership is empowering, independent of patient condition. When team is inexperienced, quality health care is highest when leadership is empowering and patient is not severely injured, or when leadership is directive and patient is severely injured |
1) Severely injured patient: M directive leaders = 3.06, 95 % CI 2.83 – 3.27, M empowering leaders = 2.72, 95 % CI 2.50 – 2.95. Non-severely injured patient: M empowering leaders = 3.91, 95 % CI 3.69 – 4.13, M directive leaders = 2.16, 95 % CI 1.94 – 2.38, F = 119.48, p < 0.01, η2 = 0.26. 2) Experienced team: M empowering leadership = 3.65, 95 % CI 3.42 - 3.82, M directive leadership = 2.48, 95 % CI 2.25 - 2.70. Inexperienced team: M empowering leadership = 2.99, 95%CI 2.76 - 3.21, M directive leadership = 2.74, 95 % CI 2.51 - 2.96, F = 23.19, p < 0.01, η2 = 0.06. 3) Inexperienced team/severely injured patient: M directive leadership = 3.19, 95 % CI 2.89 - 3.49, M empowering leadership = 2.13, 95 % CI 1.82 - 2.44. Inexperienced team/non-severely injured patient: M empowering leadership = 3.85, 95 % CI 3.57 - 4.12, M directive leadership = 2.28, 95 % CI 2.00 - 2.56, F = 7.31, p < 0.01, η2 = 0.04. |
14.5 (16) |
We report not only significant but also non-significant relationships between predictor and outcome variables of interest in this review as hypothesized in the reviewed studies; even if not explicitly stated in the original publication
a validated instrument
b effect sizes calculated by authors, calculation not possible if brackets empty
c Cohen’sƒ 2 based on R2 instead of ΔR2
d in brackets: maximal possible score
Table 4.
Relationships between well-being and patient safety
| Study | Topic | Primary topic | Sample & setting | Design & data collection methods | Assessment of variables | Analyses | Findings | Outcomes & effect sizes | Quality scored |
|---|---|---|---|---|---|---|---|---|---|
| Arakawa et al., 2011 [98] | Relationships between nurses’ work, health, and lifestyle characteristics and medical errors and incidents | yes | 6445 nurses, 99 hospitals, Japan | Cross sectional self-report questionnaire | Well-being: SF-36 scales mental health and vitality
a
Patient safety: Number of incidents and errors during the previous 6 months |
Logistic regression | No association between 1) mental health 2) vitality and medical errors and incidents |
1) NS 2) NS |
9 (16) |
| Arimura et al., 2010 [99] | Relationships between work characteristics, sleepiness, mental health state and self-reported medical errors | yes | 454 nurses, 2 general hospitals, Japan | Cross sectional self- report questionnaire | Well-being: GHQ-28a, daytime sleepiness (Epworth sleepiness scale) Patient safety: medical errors during past month |
Multiple logistic regression | 1) Poorer mental health is associated with higher occurrence of medical errors 2) Daytime sleepiness is not associated with higher occurrence of medical errors |
1) OR = 1.1, p < 0.05, 95 % CI 1.0 – 1.1 2) NS (8 predictors altogether) |
105 (16) |
| Chen et al., 2013 [114] | Relationships between burnout, job satisfaction and medical malpractice | yes | 809 physicians, Taiwan | Cross-sectional self-report questionnaire | Well-being: MBIa
Patient safety: experiences of medical malpractice |
Univariate logistic regression | 1) Emotional exhaustion is associated with higher risk of medical malpractice, whereas 2) depersonalization and 3) personal accomplishment are associated with lower risk of medical malpractice |
1) OR = 1.50, 95 % CI 0.68 –1.95 2) OR = 0.74, 95 % CI 0.40 –1.36 3) OR = 0.76, 95 % CI 0.07 –1.05 |
6 (16) |
| Cimiotti et al., 2012 [104] | Relationships between nurse staffing, burnout, and hospital infections | yes | 7076 nurses, 161 hospitals, USA | Cross-sectional self-report questionnaire, hospital records |
Well-being: MBIa
Patient safety: catheter-associated urinary tract & surgical site infections |
Linear regression | Burnout is positively associated 1) catheter-associated urinary tract and 2) surgical site infections |
1) β = 0.82, p < .05 2) β = 1.56, p < .01 |
10.5 (16) |
| Fahrenkopf et al., 2008 [106] | Relationships between depression, burnout, and medication errors | yes | 123 residents, 3 pediatric hospitals, USA | Cross-sectional self-report questionnaire, record review | Well-being: MBIa
Patient safety: medical errors (self-report & chart reviews) |
Cluster adj. Poisson analysis, Fisher’s exact test |
1) Burnt out residents perceive their number of errors to be higher than residents who are not burnt out 2) Burnt out residents are more likely to attribute errors to sleep deprivation 3) No significant differences in error rates detected in chart reviews between both groups |
1) M
high burnout = 2.3, M
low burnout = 1.0, p = 0.002 2) 29 % vs. 10 %, p = 0.05 3) NS []b |
8 (16) |
| Garrouste-Orgeas et al., 2015 [116] | Relationships between medical errors, burnout, depression, and safety culture | yes | 1534 nurses, physicians, & other healthcare staff, 31 ICUs, France | Cross-sectional self-report questionnaire, hospital records and observations |
Well-being: MBIa
Patient safety: Medical error |
Negative binomial regression | Burnout is not associated with medical error | NS | 10.5 (15) |
| Halbesleben et al., 2008 [22] | Relationships between nurse burnout and patient safety perceptions/reporting behavior | yes | 148 nurses, 1 hospital, USA | Cross sectional self- report questionnaire | Well-being: Emotional Exhaustion and Depersonalizationa
Patient safety: AHRQ Patient Safety Culture Surveya & frequency of incident reports |
Multiple linear regression | 1) Emotional exhaustion and depersonalization predict patient safety dimensions a) safety grade b) safety perception c) near-miss reporting frequency 2a) Emotional exhaustion and b) depersonalization do not predict patient safety dimension event reports |
1a) βexhaustion = −0.40, p < 0.01, βdepersonlization = −0.16, p < 0.05, R 2 = 0.22, [f 2 = 0.28]b,c 1b) βexhaustion = −0.84, p < 0.001, βdepersonlization = −0.26, p < 0.05, R 2 = 0.36, [f 2 = 0.56]b, c 1c) βexhaustion = −0.14, p < 0.05, βdepersonlization = −0.36, p < 0.01, R 2 = 0.18, [f 2 = 0.22]b, c 2a) NS 2b) NS |
13.5 (16) |
| Halbesleben & Rathert, 2008 [107] | Relationship between physician burnout and patient satisfaction and patient recovery time after hospital discharge | yes | 178 patient and physician dyads, 1 hospital, USA | Cross-sectional self- report questionnaire | Well-being: MBIa, patients’ perception of physician depersonlization Patient safety: recovery time: 1-item patient self-report |
Path analysis, Pearson’s correlation |
1) Good overall model fit 2) Positive correlation between patient recovery time and a) depersonalization b) but not emotional exhaustion c) or personal accomplishment 3) Positive correlation between patients’ perception of physician depersonalization and recovery time 4) No correlation between physician emotional exhaustion and recovery time |
1) GFI = 0.99, CFI = 1.00, NNFI = 1.02, AIC = −2.98, BIC = −8.45, RMSEA = 0.00 2a) r = 0.44, p < 0.05 2b) NS 2c) NS 3) r = 0.32, p < 0.05 4) NS |
12 (16) |
| Hayashino et al., 2012 [108] | Hope moderates relationship between distress and medical errors | yes | 836 physicians, Japan | Longitudinal self-report questionnaire | Well-being: MBIa (time 1) Medical errors: self-report (time 2) |
Poisson regression | High scores in 1) emotional exhaustion 2) depersonalization and low scores in 3) personal accomplishment at time 1 are associated with medical errors at time 2 |
1) IRR = 2.34, p < 0.0001 2) IRR = 2.72, p < 0.0001 3) IRR = 0.62, p = 0.001 |
9.5 (16) |
| Hunziker et al., 2012 [109] | Influence of self-reported, biochemical and physiological stress on cardio-pulmonary resuscitation (CPR) performance | yes | 28 residents, teaching hospital, Switzerland | Self-report questionnaire, video observation of simulated resuscitation | Well-being: Stress/overload index (self-report; blood cortisol, heart rate) Patient safety: performance (time until CPR is started and hands-on time) |
Multiple linear regression | 1) Stress/overload is positively associated with a) time to start CPR b) but not hands-on-time during resuscitation 2) Heart rate is positively associated with a) hands-on-time b) and negatively with time to start CPR during resuscitation 3a) Cortisol level and b) heart rate variability do not predict c) hands-on-time and d) time to start CPR 4) The difference of a) stress/overload b) cortisol level c) heart rate variability before to during resuscitation do not predict d) hands-on-time or e) time to start CPR 5) The difference of heart rate before to during resuscitation predicts a) hands-on-time and b) time to start CPR |
1a) β/B = 12.01, 95 % CI 0.65 – 23.36, p = 0.04 1b) NS 2a) β/B = 2.22, 95 % CI 0.53 – 3.92, p = 0.015 2b) β/B = −0.78, 95 % CI 1.44 to −0.11, p = 0.027 3 ac) NS 3ad) NS 3bc) NS 3bd) NS 4ad) NS 4ae) NS 4bd) NS 4be) NS 4 cd) NS 4ce) NS 5a) β/B = 2.73, 95 % CI 0.48 – 4.99, p = 0.022 5b) β/B = −1.12, 95 % CI −1.91 to −0.33, p = 0.01 (no information regarding standardization of coefficients) |
12.5 (15) |
| Jones et al., 2012 [100] | Effect of incident seriousness and work-based support on negative positive affect | yes | 171 nurses, 4 hospitals, UK | Cross-sectional & longitudinal between & within-person design, diary study | Well-being: Positive & Negative Affect Scale (PANAS) and mood diary entriesa
Patient safety: nurse-reported incidents |
Random-effects multilevel model | 1) Interaction of incident occurrence and seriousness leads to elevated negative affect during remainder of shift 2a) Incident occurrence 2b) but not incident seriousness lead to reduced positive affect during remainder of shift |
1) β = 0.07, z = 3.5, p < 0.005 2a) β = −2.39, z = 1.99, p < 0.05 2b) NS |
13 (16) |
| Kirwan et al., 2013 [105] | Relationships between working environment, burnout and patient safety | no | 1397 nurses, 108 wards, 30 hospitals, Ireland | Cross-sectional self-report questionnaire | Well-being: MBIa
Patient safety: one item from AHRQa, adverse events |
Multilevel regression | Emotional exhaustion on ward level does not predict 1) nurse-rated patient safety or 2) reporting of adverse events |
1) NS 2) NS |
12.5 (16) |
| Klein et al., 2010 [110] | Relationship between burnout and self-reported quality of care | yes | 1311 surgeons, 489 hospitals, Germany | Cross sectional self- report questionnaire | Well-being: Copenhagen Burnout Inventory (CBIa) Patient safety: Quality of care: frequency of diagnostic and therapeutic errors (Chirurgisches Qualitätssiegel survey CQS) |
Multivariate logistic regression | 1) Burnout is associated with 1a) lower quality of diagnosis/therapy 1b) more diagnostic errors 1c) more therapeutic errors among males 2) Unclear association of burnout with 2a) lower quality of diagnosis/therapy 2b) more diagnostic errors 2c) more therapeutic errors among females |
1a) OR = 1.71, 95 % CI 1.10 – 2.64 1b) OR = 1.94, 95 % CI 1.35 – 2.79 1c) OR = 2.56, 95 % CI 1.66 – 3.96 2a-c) contradictory information regarding significance in text and table |
10.5 (16) |
| Maiden et al., 2011 [101] | Relationship between moral distress, compassion fatigue, and causes of medication errors | yes | 205 nurses, ICU, USA | Cross sectional self-report questionnaire, focus group | Well-being: Moral distress scalea
Compassion fatigue: Professional Quality of Life Scalea Patient safety: Medication Administration Error Surveya |
Pearson’s correlation | 1) Positive correlation between moral distress and a) transcription related medication errors and b) physician communication related medication errors c) but not with medication packaging d) pharmacy processes 2) Compassion fatigue is positively correlated with a) transcription related medication errors but not with medication error due to b) physician communication c) medication packaging d) pharmacy processes |
1a) r = 0.20, p = 0.05 1b) r = 0.24, p = 0.01 1c) NS 1d) NS 2a) r = 0.15, p = 0.05 2b) NS 2c) NS 2d) NS |
9 (16) |
| Merlani et al., 2011 [13] | Relationships between hospital, patient, and clinician characteristics and burnout/stress | yes | 3052 physicians, nurses, and nurse-assistants, 74 ICUs, Switzerland | Cross-sectional self-report questionnaire, record review | Well-being: MBIa, 1 stress item Patient safety: mortality rates and length of stay (unit records) |
Multivariate logistic regression | 1) Mortality is associated with higher level of burnout 2) Length of stay is not associated with burnout |
1) OR = 1.060, p = 0.04, 95 % CI 1.003 – 1.120 2) NS |
12.5 (16) |
| Prins et al., 2009 [97] | Relationships between self-reported errors, burnout, and engagement | yes | 2115 residents, The Netherlands | Cross-sectional self- report questionnaire | Well-being: Utrecht Burnout Scale (UBOS)a, Utrecht Work Engagement Scale (UWES)a
Patient safety: medical errors |
Pearson’s correlation | 1) Errors due to wrong actions/inexperience a) are positively correlated with emotional exhaustion b) depersonalization c) and negatively correlated with personal accomplishment 2) Errors due to wrong actions/inexperience are not correlated with d) vigor e) dedication f) absorption 3) Errors due to lack of time a) are positively correlated with emotional exhaustion b) depersonalization c) and negatively correlated with personal accomplishment 4) Errors due to lack of time are negatively correlated with a) vigor b) dedication c) absorption |
1a) r = 0.20, p < 0.001 1b) r = 0.29, p < 0.001 1c) r = −0.05, p < 0.001 2a) NS 2b) NS 2c) NS 3a) r = 0.43, p < 0.001 3b) r = 0.42, p < 0.001 3c) r = −0.08, p < 0.001 4a) r = −0.23, p < 0.001 4b) r = −0.24, p < 0.001 4c) r = −0.11, p < 0.001 |
10.5 (16) |
| Ramanujam et al., 2008 [102] | Relationship between nurses’ work characteristics, burnout, and patient safety | yes | 430 nurses, 2 hospitals, USA | Cross sectional self- report questionnaire | Well-being: Not described, although it can be deducted from the paper that the MBIa was used Patient safety: nurses’ safety perception |
Path analysis | 1) Unsatisfactory initial model fit statistics, final model statistics not reported 2) Positive association between depersonalization and perceived patient safety 3) No association between emotional exhaustion and perceived patient safety |
1) χ
2 = 1100.60, df = 455, χ
2
/df = 2.419, CFI = 0.876, RMSEA = 0.058 2) β = 0.189, p < 0.001 3) NS |
8.5 (16) |
| Shanafelt et al., 2002 [112] | Prevalence of burnout in medical residents and the relationship to self-reported patient care practices | yes | 115 internal medicine residents, USA | Cross sectional self- report questionnaire | Well-being: MBIa
Patient safety: self-developed patient care practices measure |
Stepwise logistic regression | 1) Overall burnout score is associated with higher levels of a) monthly b) weekly suboptimal patient care practices 2) Depersonalization is associated with higher levels of a) monthly b) weekly suboptimal patient care practices 3) No associations between a) emotional exhaustion b) personal accomplishment and c) monthly d) weekly suboptimal patient care practices |
1a) OR = 8.3, p < 0.001, 95 % CI 2.6 – 26.5 1b) OR = 4.0, p = 0.036, 95 % CI 1.1 – 14.2 2a) OR = 5.8, p < 0.001, 95 % CI 2.2 – 15.4 2b) OR = 2.8, p = 0.041, 95 % CI 1.1 – 7.7 3 ac) NS 3ad) NS 3bc) NS 3bd) NS |
10.5 (16) |
| Shanafelt et al., 2010 [111] | Relationship between burnout, quality of life, depression and perceived major medical errors | yes | 7905 surgeons, USA | Cross sectional self- report questionnaire | Well-being: MBIa
Patient safety: medical errors |
Logistic regression | 1a) Emotional exhaustion and b) depersonalization are associated with higher odds of reporting an error 2) Personal accomplishment is associated with lower odds of reporting an error |
1a) OR = 1.048, p < 0.0001, 95 % CI 1.042 – 1.055 1b) OR = 1.109, p < 0.0001, 95 % CI 1.096 – 1.122 2) OR = 0.965, p < 0.0001, 95 % CI 0.955 – 0.975 |
9 (16) |
| Squires et al., 2010 [103] | Relationships between nurse leadership, work environment, safety climate, and nurse and patient outcomes | no | 600 acute care nurses, USA | Cross sectional self- report questionnaire | Well-being: Emotional Exhaustiona
Patient safety: medication errors and ulcers |
Path analysis | 1) Very good final model fit 2) No association between pressure ulcers and emotional exhaustion 3) Positive association between medication errors and emotional exhaustion |
1) χ
2 = 217.6, p < 0.001, SRMR = 0.054, CFI = 0.947, RMSEA = 0.047, PCLOSE = 0.67 2) NS 3) β = 0.14, p < 0.05 |
12 (16) |
| Teng et al., 2010 [14] | Interactions between time pressure and burnout on patient safety | yes | 458 nurses, 90 units, 2 medical centers, Taiwan | Cross sectional self- report questionnaire | Well-being: MBIa
Patient safety: frequency of adverse events scale |
Multiple linear regression | 1) Burnout negatively predicts patient safety 2) The interaction of burnout and time pressure negatively predict adverse events |
1) β = −0.25, p = 0.00 2) β = −0.08, p = 0.03 R 2 = 0.06 [f 2 = 0.06]b, c (7 predictors altogether) |
13 (16) |
| Welp et al., 2015 [117] | Relationships between burnout, demographic and unit characteristics, and patient safety | yes | 1425 nurses and physicians, 54 intensive care units, Switzerland | Cross-sectional self-report questionnaire, hospital records |
Well-being: MBIa
Patient safety: standardized mortality ratios, length of stay, clinician-rated patient safety |
Hierarchical (multilevel) linear regression | 1a) Emotional exhaustion and 1b) depersonalization are negatively associated with clinician-rated patient safety; c) personal accomplishment is positively associated with clinician-rated patient safety 2a) Emotional exhaustion, but not 2b) depersonalization or 2c) personal accomplishment is positively associated with standardized mortality ratios 3a) Emotional exhaustion, 3b) depersonalization, and 3c) personal accomplishment are not associated with length of stay |
1a) B = −0.13, p < .001 1b) B = −0.07, p < .05 1c) B = 0.16, p < .01 2a) β = 0.39, p < .05 2b) NS 2c) NS 3a) NS 2b) NS 2c) NS |
15 (16) |
| West et al., 2006 [113] | Relationships between distress, quality of life and medical errors | yes | 184 internal medicine residents, teaching hospital, USA | Longitudinal cohort study, self-report questionnaire |
Well-being: MBIa, fatigue and sleepiness: 2 items Patient safety: medical errors |
Generalized estimation equations (GEE) | 1) Higher levels of a) emotional exhaustion b) depersonalization are associated with major medical errors in the c) previous d) following 3 months 2) Lower levels of personal accomplishment are associated with higher levels of major medical error in the a) previous b) following 3 months |
1 ac) PE = 4.58, p = 0.002 1bc) PE = 2.45, p = 0.002 1ad) OR = 1.07, p = < 0.001, 95 % CI 1.03 – 1.12 1bd) OR = 1.10, p = 0.001, 95 % CI 1.04 – 1.16 2a) PE = −2.59, p = 0.002 2b) OR = 0.93, p = 0.02, 95 % CI 0.88 – 0.99 |
12 (16) |
| West et al., 2009 [23] | Relationships between fatigue, distress, and medical errors | yes | 380 internal medicine residents, teaching hospital, USA | Longitudinal cohort study, self-report questionnaire | Well-being: MBIa, fatigue and sleepiness: 2 items Patient safety: medical errors |
Generalized estimation equations (GEE) | Higher levels of 1) sleepiness 2) fatigue 3) emotional exhaustion 4) depersonalization and 5) lower levels of personal accomplishment are associated with subsequent medical errors |
1) OR = 1.10, p = 0.002, 95 % CI 1.03 – 1.16 2) OR = 1.14, p < 0.001, 95 % CI 1.08 – 1.21 3) OR = 1.06, p < 0.001, 95 % CI 1.04 – 1.08 4) OR = 1.09, p < 0.001, 95 % CI 1.05 – 1.12 5) OR = 0.94, p < 0.001, 95 % CI 0.92 – 0.97 |
13 (16) |
| Wetzel et al., 2010 [115] | Relationships between stress and surgical performance | yes | 30 surgeons, 1 hospital, UK | Cross-sectional self-report questionnaire, observation of simulated operations |
Well-being: State-Trait Anxiety Inventory (STAI)a, heart rate, cortisol, oberver rating Patient safety: OTASa, End Product Assessment Rating Scale (EPA) |
Linear regression | Non-crisis simulation: No relationship between 1) STAI 2) heart rate 3) cortisol 4) observer stress rating and a) OTAS b) EPA Crisis simulation: 5) no results reported on relationships between the above variables 6) Interaction between low experience and “stress” (not clear how variable was calculated) predicts lower a) EPA and b) OTAS |
1a) NS 1b) NS 2a) NS 2b) NS 3a) NS 3b) NS 4a) NS 4b) NS 5) N/A 6a) β = .54, p < .01 6b) β = .65, p < .001 |
10 (15) |
We report not only significant but also non-significant relationships between predictor and outcome variables of interest in this review as hypothesized in the reviewed studies; even if not explicitly stated in the original publication
avalidated instrument
beffect sizes calculated by authors, calculation not possible if brackets empty
cCohen’sƒ 2 based on R2 instead of ΔR2
din brackets: maximal possible score
Table 5.
Relationships between teamwork, well-being and patient safety
| Study | Topic | Primary topic | Sample & Setting | Design & data collection methods | Assessment of variables | Analyses | Findings | Outcomes & effect sizes | Quality scoreb |
|---|---|---|---|---|---|---|---|---|---|
| Davenport et al., 2007 [118] | Relationships between team and safety climate, working conditions, emotional exhaustion and patient morbidity/mortality | yes | 6083 surgical team members, 52 hospitals, USA | Cross-sectional self-report questionnaire, record review | Teamwork: SAQ subscale team climatea, levels of communication and collaboration Well-being: Emotional Exhaustiona Patient safety: risk adjusted 30-day morbidity/mortality |
Spearman’s rank correlation | 1) Negative association between patient morbidity and a) clinician’s communication with attending doctors b) but not with clinician’s communication with residents c) nurses d) other health care providers 2) No associations between team climate and a) mortality b) morbidity 3) No associations between emotional exhaustion and a) mortality b) morbidity |
1a) ρ = −0.38, p < 0.01 1b) NS 1c) NS 1d) NS 2a) NS 2b) NS 3a) NS 3b) NS |
11.5 (16) |
| Laschinger & Leiter, 2006 [119] | Mediation of relationship between nursing work environment and patient safety outcomes by burnout | yes | 8597 nurses, acute care hospitals, Canada | Cross-sectional self- report questionnaire | Teamwork: Nurse-Physician-Relations Scalea
Well-being: MBIa Patient safety: adverse events scale |
Path analysis | 1) Good overall model fit 2) Nurse-physician-relations and a) emotional exhaustion b) depersonalization c) adverse events are negatively correlated d) personal accomplishment are positively correlated 3) Adverse events and a) emotional exhaustion b) depersonalization are positively correlated c) personal accomplishment are negatively correlated (only results from correlation matrix are reported) |
1) χ
2 = 16 438.19, df = 1.344, CFI = 0.908, IFI = 0.908, RMSEA = 0.037 2a) r = −0.22, p = <0.01 2b) r = −0.16, p = <0.01 2c) r = −0.14, p = <0.01 2d) r = 0.13, p = <0.01 3a) r = 0.30, p = <0.01 3b) r = 0.34, p = <0.01 3c) r = −0.22, p = <0.01 |
10.5 (16) |
| Rathert et al., 2009 [120] | Mediation of relationships between work environment and work engagement, commitment and patient safety by psychological safety | no | 306 nurses and other clinical care providers, acute care hospital, USA | Cross-sectional self-report questionnaire | Teamwork: Psychological Safety Scalea
Well-being: Work engagement scale Patient safety: scale adapted from AHRQ Patient Safety Culture Survey |
Path analysis | 1) Good overall model fit 2) Psychological safety does not mediate relationship between work environment and a) patient safety b) work engagement 3) Positive correlation between patient safety and a) work engagement b) psychological safety 4) No correlation between psychological safety and work engagement |
1) RMSEA = 0.06, NNFI = 0.92, CFI = 0.93 2a) NS 2b) NS 3a) r = 0.14, p > 0.013 3b) r = 0.39, p < 0.01 4) NS |
10.5 (16) |
| Van Bogaert et al., 2014 [122] | Relationships between nurse practice environment, work characteristics, burnout and job and patient outcomes | no | 1108 nurses, 96 units, 7 hospitals, Belgium | Cross-sectional self-report questionnaire | Teamwork: nurse-physician relationsa Well-being: MBIa
Patient safety: patient falls, hospital-acquired infections, medication errors |
Multilevel regression | 1) Good nurse-physician relations on the unit level are associated with fewer a) patient falls b) hospital-acquired infections and c) medication errors 2) Emotional exhaustion on the unit level is associated with more a) patient falls b) hospital-acquired infections and c) medication errors 3) Depersonalization on the unit level is associated with more a) patient falls b) hospital-acquired infections and c) medication errors 4) High personal accomplishment on the unit level is associated with fewer a) patient falls b) hospital-acquired infections and c) medication errors |
1a) Adj. OR = 0.70, 95 % CI 0.48 – 1.03 1b)) Adj. OR = 0.56, 95 % CI 0.41 – 0.78 1c) Adj. OR = 0.58, 95 % CI 0.41 – 0.82 2a) Adj. OR = 1.25, 95 % CI 1.06 – 1.48 2b) Adj. OR = 1.33, 95 % CI 1.15 – 1.53 2c) Adj. OR = 1.39, 95 % CI 1.20 – 1.61 3a) Adj. OR = 1.40, 95 % CI 1.15 - 1.70 3b) Adj. OR = 1.57, 95 % CI 1.31 - 1.87 3c) Adj. OR = 1.67, 95 % CI 1.40 - 2.00 4a) Adj. OR = 0.81, 95 % CI 0.64 - 1.02 4b) Adj. OR = 0.78, 95 % CI 0.64- 0.95 4c) Adj. OR = 0.88, 95 % CI 0.71 - 1.08 |
12.5 (16) |
| Wilkins et al., 2008 [121] | Relationships between nurses’ work environment, health status and medication errors | no | 4379 nurses, Canada | Cross-sectional self-report, phone interviews | Teamwork: Nurse-Physician-Relations Scalea
Well-being: mental health (1 item) Patient safety: medication error (1 item) |
Logistic regression | 1) Lower levels of nurse-physician relations are associated with more medication errors 2) Mental health status is not associated with medication errors |
1) OR = 1.6, 95 % CI 1.1 – 2.3, p < 0.05 2) NS |
11 (16) |
We report not only significant but also non-significant relationships between predictor and outcome variables of interest in this review as hypothesized in the reviewed studies; even if not explicitly stated in the original publication
a validated instrument
b in brackets: maximal possible score
Relationships between teamwork and clinician occupational well-being
Design & sample
Out of 25 studies examining relationships between teamwork and clinician occupational well-being, 24 (96 %) used cross-sectional self-report designs, with one study adding a pre-post-shift diary design (Table 2 and box A/B in Fig. 2) [18]. One study employed a longitudinal self-report design [37]. Of these 25 studies, 19 (76 %) surveyed only nurses [18–20, 37–52], one (4 %) physicians [21], one (4 %) midwives [53], and four (16 %) included a mixed sample [54–57].
Fig. 2.
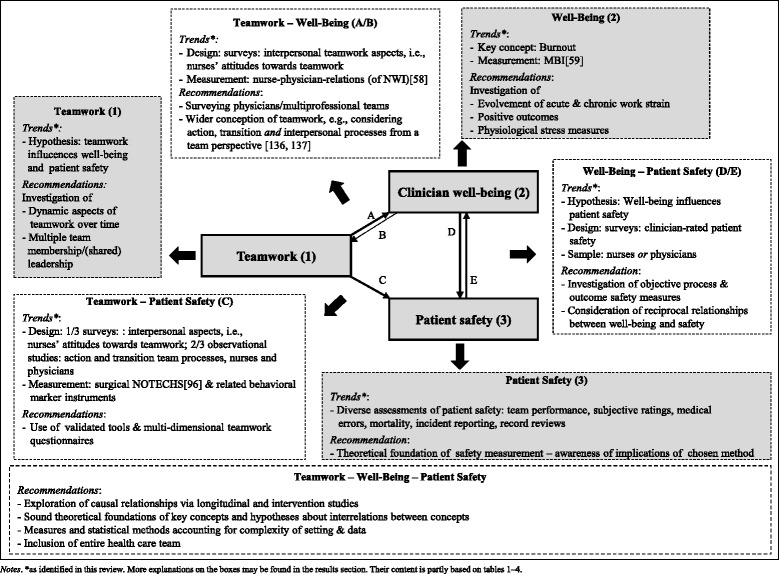
Integrative framework of teamwork, clinician occuptional well-being and patient safety in hospital settings Notes. *as identified in this review. More explanations on the boxes may be found in the results section. Their content is partly based on Tables 1, 2, 3 and 4
Measures
Studies operationalized teamwork most often with the nurse-physician-relations subscale of the Nursing Work Index (NWI; 12 studies/48 %) [18, 19, 41, 42, 44, 46, 47, 50, 52, 54, 55, 58]; and clinician occupational well-being with the Maslach Burnout Inventory or short versions thereof (MBI; 11 studies/44 %; see box A/B and box 2 in Fig. 2) [19, 38, 41–47, 55, 59].
Findings
Studies examining relationships between teamwork and well-being focused on interpersonal teamwork aspects (box A/B in Fig. 2). Most authors assumed that teamwork, a variable inherent to the working context, influences individuals’ general occupational well-being, rather than well-being influencing teamwork. Two studies (8 %) focused on acute strain [18, 54] one of which showed that it was negatively associated with team behaviors such as closed-loop communication or backup behavior [54, 60]. The only longitudinal study reported an effect of teamwork at time 1 on well-being at time 2. However, since this study did not conduct comprehensive analyses (i.e., testing for reverse causal relationships), we could not draw definite conclusions regarding causal relationships between teamwork and clinician occupational well-being [37].
Out of 25 studies examining relationships between teamwork and clinician occupational well-being, 19 (76 %) focused on interpersonal team processes in rather stable nursing teams, such as nurses’ perceptions of interprofessional teamwork or team cohesion [18–21, 37, 39, 41–47, 49–53, 57]. Four studies (20 %) did not address specific aspects of teamwork, but measured it on a general level [38, 40, 48, 54, 55]. One study (4 %) included a short questionnaire on all three team processes (i.e., action, transition, and interpersonal) [56].
Some studies examined the larger clinical work context without formulating assumptions about the specific relationships between teamwork and clinician occupational well-being, the respective findings thus being a by-product of the larger study context rather than a focus of investigation (see column ‘primary topic’ in Table 2). Across the 25 studies investigating associations between teamwork and clinician occupational well-being, 48 out of 62 (77 %) relationships reported were significant and matched author’s assumptions. Of these significant relationships, 15 (31 %) showed a positive association between both positive indicators of teamwork and well-being (e.g., work engagement), whereas 33 (69 %) showed a negative association between positive indicators of teamwork and negative indicators of well-being (e.g., burnout). Out of the 14 non-significant associations, six (43 %) were in accordance with hypotheses (i.e., teamwork on the hospital level is not related to individual burnout) [50]. Thus, overall findings indicate that clinicians perceiving higher quality of teamwork also reported higher occupational well-being or less strain. Effect sizes ranged from small (β = −12.85; f2 = 0.13) to medium (r = −0.47, Table 2).
Relationships between teamwork and patient safety
Design & sample
Studies examining relationships between teamwork and patient safety were very diverse regarding study design, construct operationalization, setting, data collection methods and strength of statistical relationships (see Table 3). Of 43 studies, 25 (58 %) employed video- or live-observation of nurses and physicians in real or simulated acute clinical situations (Table 3a) [5, 6, 11, 12, 61–81]. Five studies (12 %) utilized cross-sectional designs with self-report questionnaires (Table 3b and box C in Fig. 2) [8, 60, 82–84]. Another 13 studies (30 %) employed mixed-method designs (e.g., record reviews or observations plus questionnaires) [9, 10, 85–95]. These studies included one intervention (2 %) [88] and three studies (7 %) with longitudinal aspects [8, 88, 89]. Of the studies using questionnaires seven (16 %) surveyed either nurses [60, 82, 89–93] and seven (16 %) surveyed a mixed sample [9, 10, 83, 84, 87, 94, 95]. Observational studies, in contrast, analyzed teams usually consisting of nurses, physicians (and other healthcare professionals) with the exception of four studies (9 %) [11, 70, 75, 81].
Measures
Observational studies most frequently used the Surgical NOTECHS tool (a tool to observe non-technical skills or team behaviors in acute care settings; see box C in Fig. 2) [96] and its adaptations to various clinical settings to assess teamwork (21 %) [6, 62–64, 69, 70, 76, 85, 86]. Studies assessed patient safety using subjective ratings (6 studies/16 %) [8, 60, 82–84, 95], indicators based on hospital records (13 studies/30 %) [9, 74, 75, 85–94] and observational data (22 studies/52 %) [5, 6, 11, 12, 61–70, 73, 77–81, 85, 86]. These observational studies often used execution of key treatment actions (i.e., steps in the care process that are considered indispensable for successful treatment in potentially life threatening situations, such as the administration of magnesium sulfate for eclampsia) as a proxy measure for patient safety (10 studies/23 %) [11, 65, 68, 70–73, 79–81]. Only one study utilized both objective and subjective patient safety indicators [10].
Findings
Overall, findings were rather inconsistent for the relationship between teamwork and patient safety. All authors assumed that teamwork positively influenced patient safety. A longitudinal study confirmed this assumption (box 1 in Fig. 2) [8]. In the 43 studies investigating teamwork and patient safety, authors reported 239 relationships, 105 (44 %) of which were significant. The majority of survey and observational studies (23/53 %) reported positive associations between teamwork and patient safety [5, 6, 9, 12, 60, 61, 63–65, 67, 69–77, 79, 82, 92, 94, 95]. In line with this, the valence of 198 (83 %) of the 239 significant associations matched authors’ anticipations (i.e., a positive correlation between both positive indicators of teamwork and patient safety, such as coordination and clinical performance, or negative correlation between a positive indicator of teamwork and a negative indicator of patient safety, such as errors). However, the valence of 41 associations (17 %) was not in line with assumptions (i.e., a negative correlation between positive indicators of both teamwork and patient safety or a positive correlation between positive indicators of teamwork and negative indicators of patient safety). Thus, eight studies (19 %) contained findings suggesting that better teamwork was seemingly associated with lower patient safety [8, 10, 11, 62, 76, 85–87, 90]. Some of these findings may have been coincidental, but the majority may be explained by study design. In survey studies on medical errors, instead of the number of errors, authors measure participants’ propensity to report errors, which in turn may be fostered by positive interpersonal team relationships. In a similar vein, positive associations between teamwork and unfavorable patient outcomes like complications or operative duration in observational studies may simply reflect the necessity for increased coordinative behaviors in complicated cases (box 3 in Fig. 2). Moreover, studies investigating links between teamwork and objective or observational patient safety indicators were frequently unable to identify significant relationships (Table 3a, b). For example, two studies (5 %) used a sample of clinicians surveyed with a teamwork questionnaire to examine associations with objective and subjective patient safety indicators [82, 91]. While no association between teamwork and preventable adverse events extracted from hospital records was found [91], the effect was significant when using the frequency of these events reported by lead nurses [82].
Studies using observational tools to investigate teamwork in relation to patient safety focused on action and transition processes with nine (33 %) of altogether 27 studies examining just action processes [5, 11, 12, 61, 68, 74, 76, 77, 79], and six (22 % of observational studies) measuring both [62, 66, 67, 71–73]. Eight observational studies (30 %) measured action, transition, and interpersonal processes without clear distinction between these dimensions [6, 63, 64, 69, 70, 78, 85, 86]. Two observational studies (7 %) focused on interpersonal processes only [65, 80]. One study (4 %) examined transition processes [75]; and one study (4 %) did not provide further details on the teamwork measure [81].
Studies using questionnaires to examine teamwork in relation to patient safety were rather diverse with regard to teamwork processes. The largest part examined teamwork in general, with no clear distinction between action, transition, and interpersonal processes (8 studies/44 % of survey studies) [9, 60, 83, 87–90, 95],. followed by a focus on interpersonal processes (e.g., team climate or nurse-physician relations; 5 studies, 27 %) [8, 82, 84, 91, 92]. Two studies examined interpersonal and transition processes (13 %) [10, 94], and one study examined action and transition processes (6 %) (again, with no clear distinction between these dimensions) [93].
Effect sizes ranged from small (r = −0.08) to large (r = −0.66, Tables 3a, b).
Relationships between clinician occupational well-being and patient safety
Design & sample
The majority of the 25 studies examining relationships between clinician occupational well-being and patient safety (Table 4) targeted either nurses (10 studies/40 %) [14, 22, 98–105] or physicians (12 studies/48 %; box D/E in Fig. 2) [23, 97, 106–115], with only three studies (12 %) using a mixed sample [13, 116, 117]. Twenty studies (80 %) employed a cross-sectional design [13, 14, 22, 97–99, 101–107, 109–112, 114, 116, 117] and four (16 % used a design with longitudinal aspects [23, 100, 108, 113]. One study (4 %) combined survey and observational data [115].
Measures
Studies used the MBI [59] most frequently to assess psychological well-being (14 studies/56 %) [13, 22, 97, 102–106, 108, 111, 112, 114, 116, 117]. Studies measured patient safety using a variety of self-report measures (18 studies/72 %) [14, 22, 23, 97–103, 105, 107, 110–114], with 5 studies (24 %) using objective data such as mortality rates [13, 104, 106, 109, 117]. Two studies (8 %) assessed patient safety via observational data [115, 116].
Findings
Authors of the 25 studies examining clinician well-being and patient safety followed two lines of reasoning: Some assumed that committing an error (equaling reduced patient safety) induces (short-term, emotional) distress in clinicians (4 studies/16 %) [13, 97, 100, 103], while the majority of researchers theorized that high (chronic) strain causes employees’ performance to suffer, thus being detrimental to patient safety (20 studies/84 %; box D/E in Fig. 2) [22, 23, 98, 99, 101, 102, 104–113, 115–117]. Overall, results were mixed. Empirical evidence of longitudinal studies lends support to both perspectives [23, 100, 108, 113]. However, due to analytical limitations (i.e., testing for reverse causal relationships), we can draw no definite conclusions [23, 108, 113]. Authors of the 25 studies examining clinician occupational well-being and patient safety reported 123 relationships altogether, of which 64 (52 %) were significant and in line with hypotheses. Of these significant relationships, 42 (66 %) described a positive association between negative indicators of both clinician occupational well-being and patient safety, whereas one (2 %) described a positive association between a positive indicator of clinician occupational well-being and patient safety. Sixteen (25 %) of relationships were negative, describing associations between negative indicators of clinician occupational well-being and positive indicators of patient safety or vice versa. Another five (7 %) associations were unexpected, such as an association between burnout dimension depersonalization and perceived patient safety or heart rate (an indicator of stress) and time spent on cardio-pulmonary resuscitation (an indicator of performance) [102, 109]. However, the latter can be explained by the physically strenuous nature of resuscitation, which is likely to cause an elevated heart rate. Effect sizes ranged from small (OR = 1.09) to large (OR = 8.3, see Table 4).
Relationships between teamwork, clinician occupational well-being and patient safety
Design & sample
Five of the 98 reviewed studies examined teamwork, clinician occupational well-being and patient safety (Table 5), three of which (60 %) sampled nurses only [119, 121, 122]. All studies were cross-sectional self-report studies, with one study (20 %) using risk-adjusted morbidity and mortality rates as objective patient safety indicators.
Measures
Three of the studies (60 %) used the nurse-physician-relations scale of the NWI [58] to assess teamwork, and (parts of) the MBI [59] or its emotional exhaustion subscale to measure well-being [119, 120, 122].
Findings
Studies examining relationships between teamwork, clinician occupational well-being and teamwork focused exclusively on interpersonal team processes. One study (20 %) proposed a model with the teamwork variable psychological safety [123] serving as a mediator between work environment and work engagement, commitment, and patient safety [120]. However, this mediation effect was statistically non-significant. Another study found a partial mediation between nursing work environment (including nurse-physician relations) and adverse events via burnout. Three studies (60 %) covered teamwork, clinician occupational well-being and patient safety amongst other aspects of the (nursing) work environment, but did not analyze the variables simultaneously, and reported mixed results [118, 121, 122]. Altogether, the five studies reported 33 associations between teamwork, clinician occupational well-being and patient safety, 21 (63 %) of which were significant and in line with authors’ assumptions. These 21 associations included five (23 %) negative associations between teamwork and a negative indicator of patient safety, teamwork and a negative indicator of clinician occupational well-being, and clinician occupational well-being and a negative indicator of patient safety. The 16 positive associations (76 %) included relationships between teamwork and patient safety, clinician occupational well-being and patient safety, and between negative indicators of clinician occupational well-being and negative indicators of patient safety.
Effect sizes ranged from small (r = 0.13) to medium (r = 0.39).
Integrative framework
Our aim was to develop a framework applicable to many different healthcare teams in hospital settings. We combined psychological models of team performance and work strain with the findings and theoretical assumptions of this review to formulate specific hypotheses regarding the relationships between teamwork, clinician occupational well-being and patient safety (Fig. 2).
Drawing from the job demands-resources model, we propose that teamwork can be a demand or a resource [29]. This model proposes two parallel processes that influence positive and negative aspects of occupational well-being, such as work engagement and burnout. Job demands deplete the individual’s energy and eventually decrease occupational well-being. Job resources, on the other hand, help employees attain goals, increase occupational well-being or reduce the strain caused by job demands [29].
A team in which actions are not well-coordinated (action team processes), goals are not communicated (transition team processes) and employee’s input to the team is not welcomed by fellow team members (interpersonal team processes) may be demanding for its members and thus directly decrease the team’s ability to provide safe patient care (Fig. 2, arrow C) [10, 11, 25, 120, 123–126]. Simultaneously, ineffective teamwork may lead to decreased clinician occupational well-being: according to the conservation of resources theory, decreased well-being can develop if there is an imbalance between resource investment and resource gain [22, 55, 107, 127]. Ineffective teamwork, as a lack of resource, can lead to a higher individual workload or emotional distress, thereby decreasing well-being [55, 56].
Poor well-being, in turn, may decrease clinicians’ ability to provide safe care (arrow D), because clinicians’ physical and mental resources are depleted [128], cognitive functioning may suffer and they may not be able to exhibit safe working behaviors [129, 130]. The effects of decreased clinician well-being might also be reflected in the team, because distressed team members may not be able to execute relevant team behaviors as effectively (arrow B) [54].
In contrast, if teamwork quality is high, teamwork may act as a resource supporting clinicians to provide safe patient care (e.g., developing shared team mental models, backup behaviors, high psychological safety encouraging clinicians to speak up; or transition, action, and interpersonal team processes; arrow C) [10, 65, 120, 123, 124, 131]. Effective teamwork helps to balance workload, prevent errors, and provide social support in a demanding work environment [126, 132], and may also lead to lower strain levels (arrow A), thereby indirectly supplying clinicians with resources needed for safe patient care (arrow D) [42, 55].
From the reviewed studies, it is not clear whether patient safety influences clinician occupational well-being or vice versa. Clinicians with reduced well-being may not be able to care for patients as safely and effectively due to depletion of resources [23]. Conversely, being involved in an adverse event may lead to guilt and emotional stress potentially compromising psychological well-being in the short- or long-term. [24] Given the existing evidence, we hypothesize that clinician occupational well-being and patient safety are tightly coupled: Tangible patient safety incidents are likely to cause short-term emotional distress [103] and chronic strain in clinicians [24]. Several authors have recognized that, after the patient, the clinician may become the second victim following an adverse event. They may be blamed for errors and have their clinical competence questioned. Sufficient support systems or policies to deal with the effects of error on second victims, such as feelings of anxiety, guilt or shame, do not always exist. [133–135] Chronic strain may also develop due to demanding working conditions which may decrease clinicians’ motivation and efficiency, which could lead to reduced patient safety in the long run (arrows D and E) [23].
Gaps and trends in current research
One aim of this study was to point out current gaps and recommendations to inform future studies addressing the relationships between teamwork, clinician occupational well-being and patient safety. These gaps and recommendations based on the reviewed studies are summarized in Fig. 2. We found that a holistic approach taking account of the complexity of teams in terms of team structure and different teamwork processes in healthcare organizations was missing, especially in survey studies: for instance, in addition to focusing on the individual professions within the team, the entire multi-professional team should be included (e.g., box A/B). Potential multiple team memberships, measures covering transition, action, and interpersonal teamwork processes, and adoption of a temporal rather than static perspective to account for the temporal instability of healthcare teams should be considered (boxes 1 and C in Fig. 2) [136–138]. For example, future studies might employ the team classification developed by Andreatta, which distinguishes between four different team types by classifying team membership and team roles as stable versus variable [139]. Moreover, correlating teamwork behaviors and patient safety indicators over an entire shift is not sufficient to gain an understanding of how they are linked. Instead, changes during the course of a shift or a specific task together with other influencing factors such as disturbances or interruptions need to be taken into account [74, 140].
Future approaches should consider reciprocal relationships between clinician occupational well-being and patient safety, and broaden the assessment of well-being to acute strain, physiological stress indicators or positive outcomes such as work engagement (box 2 in Fig. 2) [141].
With respect to patient safety, there is a clear need to consider how teamwork and well-being interact and impact upon objective safety indicators (boxes D/E and 3 in Fig. 2). This also includes ensuring independence of the objective indicators from other variables. For instance, measuring patient safety via subjective ratings or incident reports may not shed light on a unit’s safety, but rather measure clinicians’ willingness to report errors, which will be higher for clinicians working in a positive team climate [93, 142]. Yet, there seems to be a gap between the need for safety indicators that are feasible and a lack of theoretical discussion of what these indicators actually entail.
We identified several conceptual and methodological issues overarching all three concepts, which could be addressed through more focused study designs (bottom box in Fig. 2). These issues included missing or unclear theoretical foundations, definitions of key concepts, research goals and hypotheses, use of instruments with low validity (despite availability of valid instruments), incomplete description of analyses and reporting of results, mismatch of analyses and research question, and overgeneralization of results.
However, none of the studies suffered from all these drawbacks and many studies investigated the larger work environment so that the comprehensive measurement of teamwork, clinician occupational well-being and patient safety was not within the scope of these studies. Despite the gaps we identified, a large proportion of the reviewed studies were of high methodological quality, using triangulated data, validated instruments and statistical analyses of adequate complexity. Still, validity of results could be greatly improved by supporting pragmatic reasoning with sound theory to define key concepts and formulate clear, measurable research goals and hypotheses. In addition, it will be easier to perform analyses accounting for complexity of both the setting and data (i.e., structural equation or multilevel modeling, longitudinal studies, non-dichotomization of continuous variables).
Altogether, we found the most recent studies seem to address the issues mentioned above, i.e., by employing longitudinal research designs, sampling multi-professional teams or including objective measures of patient safety.
Discussion
This review provides an overview of the current state of research by scrutinizing relationships between teamwork, clinician occupational well-being and patient safety in hospital settings. Overall, ample evidence on associations between combinations of either two of these concepts exists. The volume and diversity of studies highlight the relevance of these concepts and provide a rich source of information for the design of future studies and interventions. Furthermore, the findings of the review in combination with psychological theories served as the foundation for the framework to explain interrelations between the concepts. The framework is intended to aid interpretation of findings, inconsistencies, and gaps in current research, to serve as a blueprint to designing future studies aiming to improve teamwork, clinician psychological well-being and patient safety.
Need to explore mechanisms behind relationships
Based on this review, the fact that some studies found no or only partial support for their hypotheses and reported small effect sizes is mainly due to the aforementioned conceptual and methodological issues, rather than non-existent relationships between concepts. These issues could be addressed by utilizing more stringent study designs. For instance, one may not find a relationship between general perceptions of teamwork and objective patient safety indicators. However, a targeted approach that draws from theory on aspects of teamwork and error types and uses validated measures may show that distorted shared mental models are related to inadequate nursing care.
Five of the 98 studies investigated relationships between all three concepts. These five, rather recent and very diverse studies did not provide a sufficient basis for drawing conclusive conclusions regarding the causal mechanisms between the concepts (e.g., because the entire team was not sampled, contradictory results were found across the studies), but demonstrate that the need for an integrative approach has been recognized.
The next step would be to design coherent studies based on strong theoretical foundations to uncover the mechanisms underlying the well-established relationships between teamwork, clinician occupational well-being and patient safety. Knowledge of these mechanisms may serve as a basis for designing interventions that integrate all three concepts.
Adopting an integrative approach
Teamwork is the predominant form of work organization in healthcare. Clinician occupational well-being and patient safety develop in a teamwork context and are dependent on each other. Consequently, clinician occupational well-being and patient safety should not be viewed as outcomes to be managed separately. They may even seem contradictory - additional policies to ensure patient safety may increase clinician workload and decrease well-being. Our findings suggest that they can be integrated into a comprehensive approach: Teamwork may serve as a means to improve both these central organizational outcomes. Also, team-based interventions may be utilized to benefit from the synergies between teamwork, clinician well-being and patient safety. To achieve this, it is essential to focus on multi-professional teamwork and include nurses, physicians and other healthcare professionals. For example, differences in perceptions of teamwork quality by different professions [143, 144] and different approaches to team tasks may result in interpersonal friction [145] and decreased team effectiveness [5, 12]. Aside from proposing general mechanisms between teamwork, clinician well-being and patient safety, the review and framework provide an overview of the specific aspects (i.e., chronic and acute strain, interpersonal, action and transition team processes) that may help target particular problems.
Outlook
The findings of this review have implications for researchers, and the proposed framework can help to address them in an integrative manner (Fig. 2).
-
Comprehensive approach to teamwork, well-being and patient safety
There is a clear need to investigate teamwork, clinician occupational well-being and patient safety simultaneously in order to evaluate the complex interrelations between these constructs. Interdisciplinary exchange (e.g., medical, nursing, psychological) during study design would help harvest the full potential of studying these associations. Understanding these relationships may help develop interventions aimed at improving all three concepts.
-
Exploration of causal relationships
Little is known about the causal associations between teamwork, clinician occupational well-being and patient safety, and their changes over time. Theoretically informed longitudinal studies and practical interventions will shed more light on this issue. Designing and implementing team-based interventions may investigate the simultaneous effect of improved teamwork on clinician occupational well-being and patient safety.
-
Considering the entire healthcare team
Inter-professional tasks are inherent in healthcare. Thus, only considering nurses and physicians (and other healthcare professionals as appropriate) will provide a comprehensive picture of the complex associations between teamwork, clinician occupational well-being and patient safety. In addition, the complexity of teams in healthcare (i.e., temporal instability) needs to be taken in to account [136–139]. In practice, consideration of the entire healthcare team is likely to increase the impact of team-based interventions on clinician and patient outcomes [146].
Limitations
Although we employed a rigorous search strategy, we may have missed relevant studies. For instance, the lack of consensus between different research approaches concerning terminology for key concepts may have resulted in ambiguous database indexing. However, we compensated for this limitation by including a thorough search of reviews and reference lists. Second, qualitative and interventional studies might have provided additional insights, but – with one exception [88] – were excluded because they did not examine statistical relationships between the concepts that were the focus of this review. Third, study selection, data extraction and rating of study quality were naturally influenced by authors’ reporting style. Nevertheless, the detailed review procedure including structured quality rating proved useful in exploring strengths and weaknesses of the selected studies and thus provided a solid foundation for framework development. Fourth, since disagreements between raters regarding study quality were resolved by consensus discussion, interrater reliability was not calculated. Fifth, we limited this review to acute care hospital contexts, thus, we cannot be sure that our findings are applicable to other (healthcare) settings. However, while other healthcare settings, such as primary care, may differ in terms of team structure or risks to patient safety, we are nevertheless convinced that the overarching issues of this review mentioned in the section above are worth addressing in other contexts. Lastly, as with all reviews, there is always a possibility of publication bias, because non-significant results are often not published.
Conclusion
We identified substantial relationships between combinations of two of the three concepts teamwork, well-being and patient safety, indicating that all three might influence each other. The proposed framework is based on solid research and provides a foundation for overcoming current research gaps and inconsistencies by hypothesizing causal mechanisms between the concepts and investigating relationships between all three concepts simultaneously. In the most recent studies, we identified a trend to address these gaps. Following the three main recommendations (i.e., comprehensive approach to teamwork, clinician well-being and patient safety; consideration of the entire healthcare team and exploration of causal relationships) will generate research that substantially explores and supports the hypothesized links between teamwork, clinician occupational well-being and patient safety. An integrative perspective of the synergies between teamwork, well-being and patient safety will inform future research, and aims to benefit clinicians and patients alike.
Abbreviations
AHRQ, agency for healthcare research and quality; AIC, akaike information criterion; ANOVA, analysis of variance; ANTS, anesthetist’s non-technical skills; ATLS, advanced trauma life support; ATOM, anti-air teamwork observation measure; AW, annalena welp; BIC, bayesian information criterion; CBI, Copenhagen burnout inventory; CD-RISC, Connor-Davidson resilience scale; CFI, comparative fit index; CI, confidence interval; CLABSI, central line associated bloodstream infections; CoMeT–E, coordination system for medical teams - emergency; CPR, Cardio-pulmonary resuscitation; CQS, chirurgisches qualitätssiegel survey; GEE, generalized estimating equations; GHQ-12, general health questionnaire; GLM, generalized linear mixed model; icu, intensive care unit; JV, Johanna Vogt (see Acknowledgments); LQWQ-N, Leiden quality of work questionnaire for nurses; M, mean; MBI, Maslach burnout inventory; MD, Mariel Dardel; MeSH, Medical subject heading; MISSCARE, missed nursing care; NNFI, non-normed fit index; NOTECHS, surgical non-technical skills system (observational instrument); NOTSS, non-technical skills for surgeons; NRP, neonatal resuscitation program; NS, not significant; NWI, nursing work index; NWI-R, nursing work index revised; OCHRA, observation clinical human reliability assessment; OLBI, Oldenburg burnout inventory; OR, odds ratio; OTAS, observational teamwork assessment for surgery; RMSEA, root mean square error of approximation; RR, risk ratio; SAQ, safety attitudes questionnaire; SD, standard deviation; SEM, structural equation modeling; SF-36, short form health survey; SOS, safety organizing scale; SS, Sven Schmutz (see Acknowledgments); SSI, standard shiftwork index; STAI, state-trait anxiety inventory; TCI, team climate inventory; TCT, team check-up tool; TEAM, team emergency assessment measure; TeamSTEPPS, team strategies and tools to enhance performance and patient safety; TLI, Tucker Lewis index; TM, Tanja Manser; TPQ, teamwork perceptions questionnaire; UBOS, Utrecht burnout scale; UWES, Utrecht work engagement scale
Acknowledgements
We are grateful to Mariel Dardel (MD), Nicola Rudolph, Sven Schmutz (SS), and Johanna Vogt (JV) for their assistance in screening of literature, selection of relevant articles, data extraction and rating study quality.
Funding
This work was supported by the Swiss National Science Foundation (grant number PP00P1_128616).
Availability of data and materials
This systematic review used published studies as raw data. The publications included in this review are listed in Tables 2, 3, 4 and 5 and the reference list. In addition, search strategies for all six databases, the complete number of studies retrieved, search strategies for all six databases, and the detailed quality rating of all studies may be obtained from the corresponding author.
Author’s contributions
AW designed the study, conducted the literature search, analyzed and interpreted the data and wrote the manuscript. TM substantially contributed to the design of the study, aided in data interpretation and substantially contributed to the writing of the manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
This systematic review did not use human subjects, thus, no consent to publish was needed.
Ethics approval and consent to participate
This systematic review was based on already published studies. It did not use human subjects, human material, or original human data, thus, not ethics approval was needed. This systematic review did not use human subjects, thus, no consent to participate was needed.
Registration of systematic reviews
This systematic review has not been registered.
Additional files
Exemplary Search Strategies. (PDF 281 kb)
Quality rating questions. (PDF 196 kb)
Contributor Information
Annalena Welp, Email: annalena.welp@unifr.ch.
Tanja Manser, Email: tanja.manser@ukb.uni-bonn.de.
References
- 1.de Vries EN, Ramrattan MA, Smorenburg SM, Gouma DJ, Boermeester MA. The incidence and nature of in-hospital adverse events: a systematic review. Qual Saf Health Care. 2008;17:216–23. doi: 10.1136/qshc.2007.023622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vincent C. Patient safety. 2. Oxford: Wiley Blackwell; 2010. [Google Scholar]
- 3.Kozlowski SWJ, Ilgen DR. Enhancing the effectiveness of work groups and teams. Psychol Sci Public Interest. 2006;7:77–124. doi: 10.1111/j.1529-1006.2006.00030.x. [DOI] [PubMed] [Google Scholar]
- 4.Manser T. Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesth Scand. 2009;53:143–51. doi: 10.1111/j.1399-6576.2008.01717.x. [DOI] [PubMed] [Google Scholar]
- 5.Burtscher MJ, Kolbe M, Wacker J, Manser T. Interactions of team mental models and monitoring behaviors predict team performance in simulated anesthesia inductions. J Exp Psychol-Appl. 2011;17:257–69. doi: 10.1037/a0025148. [DOI] [PubMed] [Google Scholar]
- 6.McCulloch P, Mishra A, Handa A, Dale T, Hirst G, Catchpole K. The effects of aviation-style non-technical skills training on technical performance and outcome in the operating theatre. Qual Saf Health Care. 2009;18:109–15. doi: 10.1136/qshc.2008.032045. [DOI] [PubMed] [Google Scholar]
- 7.Schmutz J, Manser T. Do team processes really have an effect on clinical performance? A systematic literature review. Brit J Anaesth. 2013;110:529–44. doi: 10.1093/bja/aes513. [DOI] [PubMed] [Google Scholar]
- 8.Leroy H, Dierynck B, Anseel F, Simons T, Halbesleben JR, McCaughey D, et al. Behavioral integrity for safety, priority of safety, psychological safety, and patient safety: a team-level study. J Appl Psychol. 2012;97:1273–81. doi: 10.1037/a0030076. [DOI] [PubMed] [Google Scholar]
- 9.Hoffer Gittell J, Fairfield KM, Bierbaum B, Head W, Jackson R, Kelly M, et al. Impact of relational coordination on quality of care, postoperative pain and functioning, and length of stay: a nine-hospital study of surgical patients. Med Care. 2000;38:807–19. doi: 10.1097/00005650-200008000-00005. [DOI] [PubMed] [Google Scholar]
- 10.Edmondson AC. Learning from mistakes is easier said than done: group and organizational influences on the detection and correction of human error. J Appl Behav Sci. 2004;40:66–90. doi: 10.1177/0021886304263849. [DOI] [Google Scholar]
- 11.Manser T, Harrison TK, Gaba DM, Howard SK. Coordination patterns related to high clinical performance in a simulated anesthetic crisis. Anesth Anal. 2009;108:1606–15. doi: 10.1213/ane.0b013e3181981d36. [DOI] [PubMed] [Google Scholar]
- 12.Burtscher MJ, Manser T, Kolbe M, Grote G, Grande B, Spahn DR, et al. Adaptation in anaesthesia team coordination in response to a simulated critical event and its relationship to clinical performance. Br J Anaesth. 2011;106:801–6. doi: 10.1093/bja/aer039. [DOI] [PubMed] [Google Scholar]
- 13.Merlani P, Verdon M, Businger A, Domenighetti G, Pargger H, Ricou B. Burnout in ICU caregivers: a multicenter study of factors associated to centers. Am J Respir Crit Care Med. 2011;184:1140–6. doi: 10.1164/rccm.201101-0068OC. [DOI] [PubMed] [Google Scholar]
- 14.Teng C-I, Shyu Y-IL, Chiou W-K, Fan H-C, Lam SM. Interactive effects of nurse-experienced time pressure and burnout on patient safety: a cross-sectional survey. Int J Nurs Stud. 2010;47:1442–50. doi: 10.1016/j.ijnurstu.2010.04.005. [DOI] [PubMed] [Google Scholar]
- 15.Lazarus RS, Folkman S. Stress, appraisal, and coping. New York: Springer; 1984. [Google Scholar]
- 16.Aiken LH, Sermeus W, Van den Heede K, Sloane DM, Busse R, McKee M, et al. Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ. 2012;344:e1717. doi: 10.1136/bmj.e1717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Estryn-Behar M, Doppia MA, Guetarni K, Fry C, Machet G, Pelloux P, et al. Emergency physicians accumulate more stress factors than other physicians - results from the French SESMAT study. Emerg Med J. 2011;28:397–410. doi: 10.1136/emj.2009.082594. [DOI] [PubMed] [Google Scholar]
- 18.Gabriel AS, Diefendorff JM, Erickson RJ. The relations of daily task accomplishment satisfaction with changes in affect: a multilevel study in nurses. J Appl Psychol. 2011;96:1095–104. doi: 10.1037/a0023937. [DOI] [PubMed] [Google Scholar]
- 19.Van Bogaert P, Clarke S, Roelant E, Meulemans H, Van de Heyning P. Impacts of unit-level nurse practice environment and burnout on nurse-reported outcomes: a multilevel modelling approach. J Clin Nurs. 2010;19:1664–74. doi: 10.1111/j.1365-2702.2009.03128.x. [DOI] [PubMed] [Google Scholar]
- 20.Budge C, Carryer J, Wood S. Health correlates of autonomy, control and professional relationships in the nursing work environment. J Adv Nurs. 2003;42:260–8. doi: 10.1046/j.1365-2648.2003.02615.x. [DOI] [PubMed] [Google Scholar]
- 21.Sutinen R, Kivimaki M, Elovainio M, Forma P. Associations between stress at work and attitudes towards retirement in hospital physicians. Work Stress. 2005;19:177–85. doi: 10.1080/02678370500151760. [DOI] [Google Scholar]
- 22.Halbesleben JRB, Wakefield BJ, Wakefield DS, Cooper LB. Nurse burnout and patient safety outcomes - nurse safety perception versus reporting behavior. West J Nurs Res. 2008;30:560–77. doi: 10.1177/0193945907311322. [DOI] [PubMed] [Google Scholar]
- 23.West CP, Tan AD, Habermann TM, Sloan JA, Shanafelt TD. Association of resident fatigue and distress with perceived medical errors. JAMA. 2009;302:1294–300. doi: 10.1001/jama.2009.1389. [DOI] [PubMed] [Google Scholar]
- 24.Rassin M, Kanti T, Silner D. Chronology of medication errors by nurses: accumulation of stresses and PTSD symptoms. Issues Ment Health Nurs. 2005;26:873–86. doi: 10.1080/01612840500184566. [DOI] [PubMed] [Google Scholar]
- 25.Marks MA, Mathieu JE, Zaccaro SJ. A temporally based framework and taxonomy of team processes. Acad Manage Rev. 2001;26:356–76. [Google Scholar]
- 26.Zapf D. Emotion work and psychological well-being: a review of the literature and some conceptual considerations. Hum Resourc Manage R. 2002;12:237–68. doi: 10.1016/S1053-4822(02)00048-7. [DOI] [Google Scholar]
- 27.Nikolova I, Van Ruysseveldt J, De Witte H, Syroit J. Well-being in times of task restructuring: the buffering potential of workplace learning. Work Stress. 2014;28:217–35. doi: 10.1080/02678373.2014.929601. [DOI] [Google Scholar]
- 28.Winefield H, Gill T, Taylor A, Pilkington R. Psychological well-being and psychological distress: is it necessary to measure both? Psychol Well Being. 2012;2:3. doi: 10.1186/2211-1522-2-3. [DOI] [Google Scholar]
- 29.Demerouti E, Bakker AB, Nachreiner F, Schaufeli WB. The job demands-resources model of burnout. J Appl Psychol. 2001;86:499–512. doi: 10.1037/0021-9010.86.3.499. [DOI] [PubMed] [Google Scholar]
- 30.Bohle P, Tilley AJ. Early experience of shiftwork: influences on attitudes. J Occup Organ Psychol. 1998;71:61–79. doi: 10.1111/j.2044-8325.1998.tb00663.x. [DOI] [Google Scholar]
- 31.Vincent C. The essentials of patient safety. http://www.chfg.org/wp-content/uploads/2012/03/Vincent-Essentials-of-Patient-Safety-2012.pdf . 2012. Accessed 30 March 2016.
- 32.Buckley S, Coleman J, Davison I, Khan KS, Zamora J, Malick S, et al. The educational effects of portfolios on undergraduate student learning: a Best Evidence Medical Education (BEME) systematic review. BEME Guide No. 11. Med Teach. 2009;31:282–98. doi: 10.1080/01421590902889897. [DOI] [PubMed] [Google Scholar]
- 33.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377–84. doi: 10.1136/jech.52.6.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Mahwah: Lawrence Erlbaum Associates; 1988.
- 35.Chen H, Cohen P, Chen S. How big is a big odds ratio? Interpreting the magnitudes of odds ratios in epidemiological studies. Commun Stat Simul Comput. 2010;39:860–4. doi: 10.1080/03610911003650383. [DOI] [Google Scholar]
- 36.Kirk RE. Promoting good statistical practices: some suggestions. Educ Psychol Meas. 2001;61:213–8. doi: 10.1177/00131640121971185. [DOI] [Google Scholar]
- 37.Pisarski A, Barbour JP. What roles do team climate, roster control, and work life conflict play in shiftworkers’ fatigue longitudinally? Appl Ergon. 2014;45:773–9. doi: 10.1016/j.apergo.2013.10.010. [DOI] [PubMed] [Google Scholar]
- 38.Bobbio A, Bellan M, Manganelli AM. Empowering leadership, perceived organizational support, trust, and job burnout for nurses: A study in an Italian general hospital. Health Care Manage Rev. 2012;37:77–87. doi: 10.1097/HMR.0b013e31822242b2. [DOI] [PubMed] [Google Scholar]
- 39.Bratt MM, Broome M, Kelber S, Lostocco L. Influence of stress and nursing leadership on job satisfaction of pediatric intensive care unit nurses. Am J Crit Care. 2000;9:307–17. [PubMed] [Google Scholar]
- 40.Brunetto Y, Farr-Wharton R, Shacklock K. Supervisor-nurse relationships, teamwork, role ambiguity and well-being: public versus private sector nurses. Asia Pac J Hum Resour. 2011;49:143–64. doi: 10.1177/1038411111400161. [DOI] [Google Scholar]
- 41.Bruyneel L, Van den Heede K, Diya L, Aiken L, Sermeus W. Predictive validity of the International Hospital Outcomes Study Questionnaire: an RN4CAST pilot study. J Nurs Scholarsh. 2009;41:202–10. doi: 10.1111/j.1547-5069.2009.01272.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Gunnarsdottir S, Clarke SP, Rafferty AM, Nutbeam D. Front-line management, staffing and nurse-doctor relationships as predictors of nurse and patient outcomes. A survey of Icelandic hospital nurses. Int J Nurs Stud. 2009;46:920–7. doi: 10.1016/j.ijnurstu.2006.11.007. [DOI] [PubMed] [Google Scholar]
- 43.Kanai-Pak M, Aiken LH, Sloane DM, Poghosyan L. Poor work environments and nurse inexperience are associated with burnout, job dissatisfaction and quality deficits in Japanese hospitals. J Clin Nurs. 2008;17:3324–9. doi: 10.1111/j.1365-2702.2008.02639.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Klopper HC, Coetzee SK, Pretorius R, Bester P. Practice environment, job satisfaction and burnout of critical care nurses in South Africa. J Nurs Manage. 2012;20:685–95. doi: 10.1111/j.1365-2834.2011.01350.x. [DOI] [PubMed] [Google Scholar]
- 45.Lehmann-Willenbrock N, Lei ZK, Kauffeld S. Appreciating age diversity and German nurse well-being and commitment: co-worker trust as the mediator. Nurs Health Sci. 2012;14:213–20. doi: 10.1111/j.1442-2018.2012.00681.x. [DOI] [PubMed] [Google Scholar]
- 46.Rafferty AM, Ball J, Aiken LH. Are teamwork and professional autonomy compatible, and do they result in improved hospital care? Qual Health Care. 2001;10:32–7. doi: 10.1136/qhc.0100032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Van Bogaert P, Meulemans H, Clarke S, Vermeyen K, Van de Heyning P. Hospital nurse practice environment, burnout, job outcomes and quality of care: test of a structural equation model. J Adv Nurs. 2009;65:2175–85. doi: 10.1111/j.1365-2648.2009.05082.x. [DOI] [PubMed] [Google Scholar]
- 48.Brunetto Y, Xerri M, Shriberg A, Farr-Wharton R, Shacklock K, Newman S, et al. The impact of workplace relationships on engagement, well-being, commitment and turnover for nurses in Australia and the USA. J Adv Nurs. 2013;69:2786–99. doi: 10.1111/jan.12165. [DOI] [PubMed] [Google Scholar]
- 49.Cheng C, Bartram T, Karimi L, Leggat SG. The role of team climate in the management of emotional labour: implications for nurse retention. J Adv Nurs. 2013;69:2812–25. doi: 10.1111/jan.12202. [DOI] [PubMed] [Google Scholar]
- 50.Li BY, Bruyneel L, Sermeus W, Van den Heede K, Matawie K, Aiken L, et al. Group-level impact of work environment dimensions on burnout experiences among nurses: a multivariate multilevel probit model. I J Nurs Stud. 2013;50:281–91. doi: 10.1016/j.ijnurstu.2012.07.001. [DOI] [PubMed] [Google Scholar]
- 51.Van Bogaert P, Adriaenssens J, Dilles T, Martens D, Van Rompaey B, Timmermans O. Impact of role-, job-and organizational characteristics on nursing unit managers’ work related stress and well-being. J Adv Nurs. 2014;70:2622–33. doi: 10.1111/jan.12449. [DOI] [PubMed] [Google Scholar]
- 52.Van Bogaert P, Kowalski C, Weeks SM, Van Heusden D, Clarke SP. The relationship between nurse practice environment, nurse work characteristics, burnout and job outcome and quality of nursing care: a cross-sectional survey. Int J Nurs Stud. 2013;50:1667–77. doi: 10.1016/j.ijnurstu.2013.05.010. [DOI] [PubMed] [Google Scholar]
- 53.Raftopoulos V, Savva N, Papadopoulou M. Safety culture in the maternity units: a census survey using the Safety Attitudes Questionnaire. BMC Health Serv Res. 2011;11:238. doi: 10.1186/1472-6963-11-238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Gevers J, van Erven P, de Jonge J, Maas M, de Jong J. Effect of acute and chronic job demands on effective individual teamwork behaviour in medical emergencies. J Adv Nurs. 2010;66:1573–83. doi: 10.1111/j.1365-2648.2010.05314.x. [DOI] [PubMed] [Google Scholar]
- 55.Rathert C, Williams ES, Lawrence ER, Halbesleben JRB. Emotional exhaustion and workarounds in acute care: cross sectional tests of a theoretical framework. Int J Nurrs Stud. 2012;49:969–77. doi: 10.1016/j.ijnurstu.2012.02.011. [DOI] [PubMed] [Google Scholar]
- 56.So TT, West MA, Dawson JF. Team-based working and employee well-being: a cross-cultural comparison of United Kingdom and Hong Kong health services. Eur J Work Organ Psy. 2011;20:305–25. doi: 10.1080/13594320903384821. [DOI] [Google Scholar]
- 57.Profit J, Sharek PJ, Amspoker AB, Kowalkowski MA, Nisbet CC, Thomas EJ, et al. Burnout in the NICU setting and its relation to safety culture. BMJ Qual Saf. 2014;23:806–13. doi: 10.1136/bmjqs-2014-002831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Lake ET. Development of the practice environment scale of the nursing work index. Res Nurs Health. 2002;25:176–88. doi: 10.1002/nur.10032. [DOI] [PubMed] [Google Scholar]
- 59.Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory manual. 3. Palo Alto: Consulting Psychologists Press; 1996. [Google Scholar]
- 60.Kalisch BJ, Lee KH. The impact of teamwork on missed nursing care. Nurs Outlook. 2010;58:233–41. doi: 10.1016/j.outlook.2010.06.004. [DOI] [PubMed] [Google Scholar]
- 61.Burtscher MJ, Wacker J, Grote G, Manser T. Managing nonroutine events in anesthesia: the role of adaptive coordination. Hum Factors. 2010;52:282–94. doi: 10.1177/0018720809359178. [DOI] [PubMed] [Google Scholar]
- 62.Catchpole K, Giddings A, Hirst G, Dale T, Peek G, de Leval M. A method for measuring threats and errors in surgery. Cogn Technol Work. 2008;10:295–304. doi: 10.1007/s10111-007-0093-9. [DOI] [Google Scholar]
- 63.Catchpole K, Mishra A, Handa A, McCulloch P. Teamwork and error in the operating room - analysis of skills and roles. Ann Surg. 2008;247:699–706. doi: 10.1097/SLA.0b013e3181642ec8. [DOI] [PubMed] [Google Scholar]
- 64.Catchpole K, Giddings AEB, Wilkinson M, Hirst G, Dale T, de Leval MR. Improving patient safety by identifying latent failures in successful operations. Surgery. 2007;142:102–10. doi: 10.1016/j.surg.2007.01.033. [DOI] [PubMed] [Google Scholar]
- 65.Kolbe M, Burtscher MJ, Wacker J, Grande B, Nohynkova R, Manser T, et al. Speaking up is related to better team performance in simulated anesthesia inductions: an observational study. Anesth Analg. 2012;115:1099–108. doi: 10.1213/ANE.0b013e318269cd32. [DOI] [PubMed] [Google Scholar]
- 66.Künzle B, Zala-Mezö E, Wacker J, Kolbe M, Spahn DR, Grote G. Leadership in anaesthesia teams: the most effective leadership is shared. Qual Saf Health Care. 2010;19:1–6. doi: 10.1097/QMH.0b013e3181d1391c. [DOI] [PubMed] [Google Scholar]
- 67.Künzle B, Zala-Mezö E, Kolbe M, Wacker J, Grote G. Substitutes for leadership in anaesthesia teams and their impact on leadership effectiveness. Eur J Work Organ Psy. 2010;19:505–31. doi: 10.1080/13594320902986170. [DOI] [Google Scholar]
- 68.Lubbert PHW, Kaasschieter EG, Hoorntje LE, Leenen LPH. Video registration of trauma team performance in the emergency department: the results of a 2-year analysis in a level 1 trauma center. J Trauma Inj Infect Crit Care. 2009;67:1412–20. doi: 10.1097/TA.0b013e31818d0e43. [DOI] [PubMed] [Google Scholar]
- 69.Mishra A, Catchpole K, Dale T, McCulloch P. The influence of non-technical performance on technical outcome in laparoscopic cholecystectomy. Surg Endosc. 2008;22:68–73. doi: 10.1007/s00464-007-9346-1. [DOI] [PubMed] [Google Scholar]
- 70.Ottestad E, Boulet JR, Lighthall GK. Evaluating the management of septic shock using patient simulation. Crit Care Med. 2007;35:769–75. doi: 10.1097/01.CCM.0000256849.75799.20. [DOI] [PubMed] [Google Scholar]
- 71.Siassakos D, Fox R, Crofts JF, Hunt LP, Winter C, Draycott TJ. The management of a simulated emergency: better teamwork, better performance. Resuscitation. 2011;82:203–6. doi: 10.1016/j.resuscitation.2010.10.029. [DOI] [PubMed] [Google Scholar]
- 72.Siassakos D, Bristowe K, Draycott TJ, Angouri J, Hambly H, Winter C, et al. Clinical efficiency in a simulated emergency and relationship to team behaviours: a multisite cross-sectional study. BJOG. 2011;118:596–607. doi: 10.1111/j.1471-0528.2010.02843.x. [DOI] [PubMed] [Google Scholar]
- 73.Thomas E, Sexton J, Lasky R, Helmreich R, Crandell D, Tyson J. Teamwork and quality during neonatal care in the delivery room. J Perinatol. 2006;26:163–9. doi: 10.1038/sj.jp.7211451. [DOI] [PubMed] [Google Scholar]
- 74.Tschan F, Semmer NK, Gautschi D, Hunziker P, Spychiger M, Marsch SU. Leading to recovery: group performance and coordinative activities in medical emergency driven Groups. Hum Perform. 2006;19:277–304. doi: 10.1207/s15327043hup1903_5. [DOI] [Google Scholar]
- 75.Tschan F, Semmer NK, Gurtner A, Bizzari L, Spychiger M, Breuer M, et al. Explicit reasoning, confirmation bias, and illusory transactive aemory: a simulation study of group medical decision making. Small Group Res. 2009;40:271–300. doi: 10.1177/1046496409332928. [DOI] [Google Scholar]
- 76.Westli HJB, Eid J, Rasten I, Brattebø G. Teamwork skills, shared mental models, and performance in simulated trauma teams: an independent group design. Scand J Trauma Resusc Emerg Med. 2010;18:47. doi: 10.1186/1757-7241-18-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Wiegmann DA, Elbardissi AW, Dearani JA, Daly RC, Sundt Iii TM. Disruptions in surgical flow and their relationship to surgical errors: an exploratory investigation. Surgery. 2007;142:658–65. doi: 10.1016/j.surg.2007.07.034. [DOI] [PubMed] [Google Scholar]
- 78.Williams AL, Lasky RE, Dannemiller JL, Andrei AM, Thomas EJ. Teamwork behaviours and errors during neonatal resuscitation. Qual Saf Health Care. 2010;19:60–4. doi: 10.1136/qshc.2007.025320. [DOI] [PubMed] [Google Scholar]
- 79.Schmutz J, Hoffmann F, Heimberg E, Manser T. Effective coordination in medical emergency teams: the moderating role of task type. Eur J Work Organ Psy. 2015;24:761–76. doi: 10.1080/1359432X.2015.1018184. [DOI] [Google Scholar]
- 80.Siassakos D, Draycott TJ, Crofts JF, Hunt LP, Winter C, Fox R. More to teamwork than knowledge, skill and attitude. BJOG. 2010;117:1262–9. doi: 10.1111/j.1471-0528.2010.02654.x. [DOI] [PubMed] [Google Scholar]
- 81.Endacott R, Bogossian FF, Cooper SJ, Forbes H, Kain VJ, Young SC, et al. Leadership and teamwork in medical emergencies: performance of nursing students and registered nurses in simulated patient scenarios. J Clin Nurs. 2015;24:90–100. doi: 10.1111/jocn.12611. [DOI] [PubMed] [Google Scholar]
- 82.Manojlovich M, Decicco B. Healthy work environments, nurse-physician communication, and patients’ outcomes. Am J Crit Care. 2007;16:536–43. [PubMed] [Google Scholar]
- 83.Hwang J, Ahn J. Teamwork and clinical error reporting among nurses in Korean hospitals. Asian Nurs Res. 2015;9:14–20. doi: 10.1016/j.anr.2014.09.002. [DOI] [PubMed] [Google Scholar]
- 84.Ogbolu Y, Johangten M, Zhu S, Johnson JV. Nurse reported patient safety in low-resource settings: a cross-sectional study of MNCH nurses in Nigeria. Appl Nurs Res. 2015;28:341–6. doi: 10.1016/j.apnr.2015.02.006. [DOI] [PubMed] [Google Scholar]
- 85.Schraagen JM. Dealing with unforeseen complexity in the OR: the role of heedful interrelating in medical teams. TIES. 2011;12:256–72. [Google Scholar]
- 86.Schraagen JM, Schouten T, Smit M, Haas F, van der Beek D, van de Ven J, et al. A prospective study of paediatric cardiac surgical microsystems: assessing the relationships between non-routine events, teamwork and patient outcomes. BMJ Qual Saf. 2011;20:599–603. doi: 10.1136/bmjqs.2010.048983. [DOI] [PubMed] [Google Scholar]
- 87.Brewer BB. Relationships among teams, culture, safety, and cost outcomes. West J Nurs Res. 2006;28:641–53. doi: 10.1177/0193945905282303. [DOI] [PubMed] [Google Scholar]
- 88.Chan KS, Hsu YJ, Lubomski LH, Marsteller JA. Validity and usefulness of members reports of implementation progress in a quality improvement initiative: findings from the Team Check-up Tool (TCT). Implement Sci. 2011;6. [DOI] [PMC free article] [PubMed]
- 89.Chang YK, Mark BA. Antecedents of severe and nonsevere medication errors. J Nurs Scholarsh. 2009;41:70–8. doi: 10.1111/j.1547-5069.2009.01253.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Fasolino T, Snyder R. Linking nurse characteristics, team member effectiveness, practice environment, and medication error incidence. J Nurs Care Qual. 2012;27:E9–16. doi: 10.1097/NCQ.0b013e318241da17. [DOI] [PubMed] [Google Scholar]
- 91.Manojlovich M, Antonakos CL, Ronis DL. Intensive care units, communication between nurses and physicians, and patients’ outcomes. Am J Crit Care. 2009;18:21–30. doi: 10.4037/ajcc2009353. [DOI] [PubMed] [Google Scholar]
- 92.Taylor JA, Dominici F, Agnew J, Gerwin D, Morlock L, Miller MR. Do nurse and patient injuries share common antecedents? An analysis of associations with safety climate and working conditions. BMJ Qual Saf. 2012;21:101–11. doi: 10.1136/bmjqs-2011-000082. [DOI] [PubMed] [Google Scholar]
- 93.Vogus TJ, Sutcliffe KM. The impact of safety organizing, trusted leadership, and care pathways on reported medication errors in hospital nursing units. Med Care. 2007;45:997–1002. doi: 10.1097/MLR.0b013e318053674f. [DOI] [PubMed] [Google Scholar]
- 94.Wheelan SA, Burchill CN, Tilin F. The link between teamwork and patients’ outcomes in intensive care units. Am J Crit Care. 2003;12:527–34. [PubMed] [Google Scholar]
- 95.Yun S, Faraj S, Sims HP., Jr Contingent leadership and effectiveness of trauma resuscitation teams. J Appl Psychol. 2005;90:1288–96. doi: 10.1037/0021-9010.90.6.1288. [DOI] [PubMed] [Google Scholar]
- 96.Flin RH, Lynne M, Goeters KM, Hörmann HJ, Amalberti R, Valot C, et al. Development of the NOTECHS (non-technical skills) system for assessing pilots’ CRM skills. Hum Factors Aero Saf. 2003;3:95–117. [Google Scholar]
- 97.Prins JT, van der Heijden FMMA, Hoekstra-Weebers JEHM, Bakker AB, van de Wiel HBM, Jacobs B, et al. Burnout, engagement and resident physicians’ self-reported errors. Psychol Health Med. 2009;14:654–66. doi: 10.1080/13548500903311554. [DOI] [PubMed] [Google Scholar]
- 98.Arakawa C, Kanoya Y, Sato C. Factors contributing to medical errors and incidents among hospital nurses - nurses’ health, quality of life, and workplace predict medical errors and incidents. Ind Health. 2011;49:381–8. doi: 10.2486/indhealth.MS968. [DOI] [PubMed] [Google Scholar]
- 99.Arimura M, Imai M, Okawa M, Fujimura T, Yamada N. Sleep, mental health status, and medical errors among hospital nurses in Japan. Ind Health. 2010;48:811–7. doi: 10.2486/indhealth.MS1093. [DOI] [PubMed] [Google Scholar]
- 100.Jones MC, Johnston DW. Does clinical incident seriousness and receipt of work-based support influence mood experienced by nurses at work? A behavioural diary study. Int J Nurs Stud. 2012;49:978–87. doi: 10.1016/j.ijnurstu.2012.02.014. [DOI] [PubMed] [Google Scholar]
- 101.Maiden J, Georges JM, Connelly CD. Moral distress, compassion fatigue, and perceptions about medication errors in certified critical care nurses. DCCN. 2011;30:339–45. doi: 10.1097/DCC.0b013e31822fab2a. [DOI] [PubMed] [Google Scholar]
- 102.Ramanujam R, Abrahamson K, Anderson JG. Influence of workplace demands on nurses’ perception of patient safety. Nurs Health Sci. 2008;10:144–50. doi: 10.1111/j.1442-2018.2008.00382.x. [DOI] [PubMed] [Google Scholar]
- 103.Squires M, Tourangeau A, Laschinger HK, Doran D. The link between leadership and safety outcomes in hospitals. J Nurs Manag. 2010;18:914–25. doi: 10.1111/j.1365-2834.2010.01181.x. [DOI] [PubMed] [Google Scholar]
- 104.Cimiotti JP, Aiken LH, Sloane DM, Wu ES. Nurse staffing, burnout, and health care-associated infection. Am J Infect Control. 2012;40:486–90. doi: 10.1016/j.ajic.2012.02.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Kirwan M, Matthews A, Scott P. The impact of the work environment of nurses on patient safety outcomes: a multi-level modelling approach. Int J Nurs Stud. 2013;50:253–63. doi: 10.1016/j.ijnurstu.2012.08.020. [DOI] [PubMed] [Google Scholar]
- 106.Fahrenkopf AM, Sectish TC, Barger LK, Sharek PJ, Lewin D, Chiang VW, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336:488–91. doi: 10.1136/bmj.39469.763218.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Halbesleben JRB, Rathert C. Linking physician burnout and patient outcomes: exploring the dyadic relationship between physicians and patients. Health Care Manage Rev. 2008;33:29–39. doi: 10.1097/01.HMR.0000304493.87898.72. [DOI] [PubMed] [Google Scholar]
- 108.Hayashino Y, Utsugi-Ozaki M, Feldman MD, Fukuhara S. Hope modified the association between distress and incidence of self-perceived medical errors among practicing physicians: prospective cohort study. PLoS ONE. 2012;7:e35585. doi: 10.1371/journal.pone.0035585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Hunziker S, Semmer NK, Tschan F, Schuetz P, Mueller B, Marsch S. Dynamics and association of different acute stress markers with performance during a simulated resuscitation. Resuscitation. 2012;83:572–8. doi: 10.1016/j.resuscitation.2011.11.013. [DOI] [PubMed] [Google Scholar]
- 110.Klein J, Frie KG, Blum K, von dem Knesebeck O. Burnout and perceived quality of care among German clinicians in surgery. Int J Qual Health Care. 2010;22:525–30. doi: 10.1093/intqhc/mzq056. [DOI] [PubMed] [Google Scholar]
- 111.Shanafelt TD, Balch CM, Bechamps G, Russell T, Dyrbye L, Satele D, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251:995–1000. doi: 10.1097/SLA.0b013e3181bfdab3. [DOI] [PubMed] [Google Scholar]
- 112.Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136:358–67. doi: 10.7326/0003-4819-136-5-200203050-00008. [DOI] [PubMed] [Google Scholar]
- 113.West CP, Huschka MM, Novotny PJ, Sloan JA, Kolars JC, Habermann TM, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA. 2006;296:1071–8. doi: 10.1001/jama.296.9.1071. [DOI] [PubMed] [Google Scholar]
- 114.Chen KY, Yang CM, Lien CH, Chiou HY, Lin MR, Chang HR, et al. Burnout, job satisfaction, and medical malpractice among physicians. Int J Med Sci. 2013;10:1471–8. doi: 10.7150/ijms.6743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Wetzel CM, Black SA, Hanna GB, Athanasiou T, Kneebone RL, Nestel D, et al. The effects of stress and coping on surgical performance during simulations. Ann Surg. 2010;251:171–6. doi: 10.1097/SLA.0b013e3181b3b2be. [DOI] [PubMed] [Google Scholar]
- 116.Garrouste-Orgeas M, Perrin M, Soufir L, Vesin A, Blot F, Maxime V, et al. The Iatroref study: medical errors are associated with symptoms of depression in ICU staff but not burnout or safety culture. Intensive Care Med. 2015;41:273–84. doi: 10.1007/s00134-014-3601-4. [DOI] [PubMed] [Google Scholar]
- 117.Welp A, Meier LL, Manser T. Emotional exhaustion and workload predict clinician-rated and objective patient safety. Front Psychol. 2015;5:1573. doi: 10.3389/fpsyg.2014.01573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Davenport DL, Henderson WG, Mosca CL, Khuri SF, Mentzer RM., Jr Risk-adjusted morbidity in teaching hospitals correlates with reported levels of communication and collaboration on surgical teams but not with scale measures of teamwork climate, safety climate, or working conditions. J Am Coll Surg. 2007;205:778–84. doi: 10.1016/j.jamcollsurg.2007.07.039. [DOI] [PubMed] [Google Scholar]
- 119.Laschinger HKS, Leiter MP. The impact of nursing work environments on patient safety outcomes - the mediating role of burnout/engagement. J Nurs Adm. 2006;36:259–67. doi: 10.1097/00005110-200605000-00019. [DOI] [PubMed] [Google Scholar]
- 120.Rathert C, Ishqaidef G, May DR. Improving work environments in health care: test of a theoretical framework. Health Care Manage Rev. 2009;34:334–43. doi: 10.1097/HMR.0b013e3181abce2b. [DOI] [PubMed] [Google Scholar]
- 121.Wilkins K, Shields M. Correlates of medication error in hospitals. Health Rep. 2008;19:7–18. [PubMed] [Google Scholar]
- 122.Van Bogaert P, Timmermans O, Weeks SM, van Heusden D, Wouters K, Franck E. Nursing unit teams matter: impact of unit-level nurse practice environment, nurse work characteristics, and burnout on nurse reported job outcomes, and quality of care, and patient adverse events - a cross-sectional survey. Int J Nurs Stud. 2014;51:1123–34. doi: 10.1016/j.ijnurstu.2013.12.009. [DOI] [PubMed] [Google Scholar]
- 123.Edmondson A. Psychological safety and learning behavior in work teams. Admin Sci Q. 1999;44:350–83. doi: 10.2307/2666999. [DOI] [Google Scholar]
- 124.Edmondson A. Speaking up in the operating room: how team leaders promote learning interdisciplinary action teams. J Manage Stud. 2003;40:1419–52. doi: 10.1111/1467-6486.00386. [DOI] [Google Scholar]
- 125.Nagpal K, Vats A, Lamb B, Ashrafian H, Sevdalis N, Vincent C, et al. Information transfer and communication in surgery: a systematic review. Ann Surg. 2010;252:225–39. doi: 10.1097/SLA.0b013e3181e495c2. [DOI] [PubMed] [Google Scholar]
- 126.Reader T, Flin R, Lauche K, Cuthbertson BH. Non-technical skills in the intensive care unit. Brit J Anaesth. 2006;96:551–9. doi: 10.1093/bja/ael067. [DOI] [PubMed] [Google Scholar]
- 127.Hobfoll SE. Conservation of resources: a new attempt at conceptualizing stress. Am Psychol. 1989;44:513–24. doi: 10.1037/0003-066X.44.3.513. [DOI] [PubMed] [Google Scholar]
- 128.Arora S, Sevdalis N, Nestel D, Woloshynowych M, Darzi A, Kneebone R. The impact of stress on surgical performance: a systematic review of the literature. Surgery. 2010;147:318–30.e6. doi: 10.1016/j.surg.2009.10.007. [DOI] [PubMed] [Google Scholar]
- 129.Nahrgang JD, Morgeson FP, Hofmann DA. Safety at work: a meta-analytic investigation of the link between job demands, job resources, burnout, engagement, and safety outcomes. J Appl Psychol. 2011;96:71–94. doi: 10.1037/a0021484. [DOI] [PubMed] [Google Scholar]
- 130.Deligkaris P, Panagopoulou E, Montgomery AJ, Masoura E. Job burnout and cognitive functioning: a systematic review. Work Stress. 2014;28:107–23. [Google Scholar]
- 131.Mathieu JE, Heffner TS, Goodwin GF, Salas E, Cannon-Bowers JA. The influence of shared mental models on team process and performance. J Appl Psychol. 2000;85:273–83. doi: 10.1037/0021-9010.85.2.273. [DOI] [PubMed] [Google Scholar]
- 132.Berland A, Natvig GK, Gundersen D. Patient safety and job-related stress: a focus group study. Intensive Crit Care Nurs. 2008;24:90–7. doi: 10.1016/j.iccn.2007.11.001. [DOI] [PubMed] [Google Scholar]
- 133.Mira JJ, Lorenzo S, Navarro I. Hospital reputation and perceptions of patient safety. Med Princ Pract. 2014;23. [DOI] [PMC free article] [PubMed]
- 134.Wu AW. Medical error: the second victim. BMJ. 2000;320. [DOI] [PMC free article] [PubMed]
- 135.Wu AW, Steckelberg RC. Medical error, incident investigation and the second victim: doing better but feeling worse? BMJ Qual Saf. 2012;21. [DOI] [PubMed]
- 136.Roe RA. Time in applied psychology: The study of “what happens” rather than “what is”. Eur Psychol. 2008;13:37–52. doi: 10.1027/1016-9040.13.1.37. [DOI] [Google Scholar]
- 137.Roe RA, Gockel C, Meyer B. Time and change in teams: where we are and where we are moving. Eur J Work Organ Psy. 2012;21:629–56. doi: 10.1080/1359432X.2012.729821. [DOI] [Google Scholar]
- 138.Schmutz J, Welp A, Kolbe M. Teamwork in healthcare organizations. In: Örtenblad A, Abrahamson Löfström C, Sheaff R, editors. Management strategies for health care organizations: adopt, abandon, or adapt? London: Routledge; 2016. pp. 359–77. [Google Scholar]
- 139.Andreatta PB. A typology for health care teams. Health Care Manage Rev. 2010;35:345–54. doi: 10.1097/HMR.0b013e3181e9fceb. [DOI] [PubMed] [Google Scholar]
- 140.Manser T, Howard SK, Gaba DM. Adaptive coordination in cardiac anaesthesia: a study of situational changes in coordination patterns using a new observation system. Ergonomics. 2008;51:1153–78. doi: 10.1080/00140130801961919. [DOI] [PubMed] [Google Scholar]
- 141.Schaufeli W, Salanova M, González-Romá V, Bakker A. The Measurement of engagement and burnout: a two sample confirmatory factor analytic approach. J Happiness Stud. 2002;3:71–92. doi: 10.1023/A:1015630930326. [DOI] [Google Scholar]
- 142.Naveh E, Katz-Navon T, Stern Z. Readiness to report medical treatment errors: the effects of safety procedures, safety information, and priority of safety. Med Care. 2006;44:117–23. doi: 10.1097/01.mlr.0000197035.12311.88. [DOI] [PubMed] [Google Scholar]
- 143.Reader TW, Flin R, Cuthbertson BH. Communication skills and error in the intensive care unit. Curr Opin Crit Care. 2007;13:732–6. doi: 10.1097/MCC.0b013e3282f1bb0e. [DOI] [PubMed] [Google Scholar]
- 144.Fleming M, Smith S, Slaunwhite J, Sullivan J. Investigating interpersonal competencies of cardiac surgery teams. Can J Surg. 2006;49:22–30. [PMC free article] [PubMed] [Google Scholar]
- 145.Rosenstein AH, O'Daniel M. Disruptive behavior & clinical outcomes: perceptions of nurses & physicians. Am J Nurs. 2005;105:54–64. doi: 10.1097/00000446-200501000-00025. [DOI] [PubMed] [Google Scholar]
- 146.Le Blanc PM, Hox JJ, Schaufeli WB, Taris TW, Peeters MCW. Take Care!! The evaluation of a team-based burnout intervention program for oncology care providers. J Appl Psychol. 2007;92:213–27. doi: 10.1037/0021-9010.92.1.213. [DOI] [PubMed] [Google Scholar]
- 147.Kotrlik JW, Williams HA. The incorporation of effect size in information technology, learning, and performance research. ITLPJ. 2003;21:1–7. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
This systematic review used published studies as raw data. The publications included in this review are listed in Tables 2, 3, 4 and 5 and the reference list. In addition, search strategies for all six databases, the complete number of studies retrieved, search strategies for all six databases, and the detailed quality rating of all studies may be obtained from the corresponding author.