

Abstract
Painful bone metastases are common in prostate cancer, with current treatments including non-steroidal analgesics and opiates, surgery, external beam radiotherapy and bone-targeting β-emitting radiopharmaceuticals. The α-emitting isotope 223Ra-dichloride (Ra-223) has been associated with improved overall survival and increased time to first skeletal-related events in patients with castration-resistant prostate cancer (CRPC) presenting with symptomatic bone metastases. The current study reports the case of a 70-year-old male patient, who was diagnosed with prostate cancer in 1999 upon presentation with increased prostate-specific antigen (PSA) levels and painful bone metastases in the context of CRPC. In November 2010, subsequent to undergoing hormonal blockage, the patient was treated with ketoconazole (200 mg/8 h) followed by 10 cycles of docetaxel (75 mg/m2 every 3 weeks). Following disease progression, the patient received 6 doses of Ra-223 (50 kBq/kg; 1 dose/4 weeks). During this treatment period, an improvement in the patient's symptoms, and levels of bone alkaline phosphatase (BAP) and PSA were noted. Furthermore, Ra-223 was well-tolerated without any relevant bone marrow toxicity. However, 2 months after the administration of the final dose of Ra-223, PSA and BAP levels increased again, and bone pain deteriorated. A bone scan showed stable disease in the previously observed metastatic lesions; however, new lesions simultaneously appeared in different locations, indicating progressive disease.
Keywords: 223Ra-dichloride, castration-resistant prostate cancer, bone metastases, Prostate Cancer Working Group
Introduction
Bone metastasis is common in prostate cancer, and the majority of patients with castration-resistant prostate cancer (CRPC) present with radiographic evidence of bone disease and associated symptoms. Up to 80% of patients develop associated symptoms of bone disease, including bone pain, bone fractures or even spinal cord compression. As prostate cancer has a particular propensity to spread to the bone, common symptoms include skeletal-related events (SREs), such as pain, fractures, hypercalcemia and medullar compression, which result in significant morbidity, worsen patient quality of life and comprise the most frequent cause of mortality in these patients. Palliative treatment for bone pain associated with metastasis includes non-steroidal analgesics and opiates, surgery, bone-targeted therapies (bisphosphonates and denosumab) and external beam radiotherapy. The effect of the aforementioned treatments are limited to delaying the onset of SREs (1,2).
Bone-targeting radiopharmaceuticals have also been added to the treatment options available, as they have been shown to be efficient in relieving metastatic bone pain, particularly in patients with widespread bone disease (3). The radiopharmaceuticals most frequently used for bone pain relief are β-emitting isotopes, such as 89Sr-chloride, 153Sm-ethylenediaminetetramethylene phosphonic acid and 186Re-etidronate.
Recently, an α-emitting isotope, 223Radium-dichloride (Ra-223), has been approved for the treatment of patients with CRPC that develop painful bone metastasis without evidence of visceral metastases. In general, α-emitters are associated with a shorter range (<0.1 mm) and a higher energetic radiation compared with β-particles and γ-rays, which have a low Linear Energy Transfer (LET) radiation. In addition, α-emitters exhibit a tissue penetration diameter of 2–10 cells, minimizing the damage to healthy hematopoietic tissue. Furthermore, due to their high LET radiation, α-particles are considered more lethal, inducing non-repairable double-stranded DNA breaks in adjacent tumor cells (4).
Ra-223 is the only radiopharmaceutical that has been demonstrated to increase overall survival (OS) in patients with CRPC with bone metastasis in a phase III study. The aforementioned study, the ALSYMPCA trial, is an international, randomized, double-blinded, placebo-controlled study that was conducted in men with symptomatic metastatic CRPC (5). The inclusion criteria were symptomatic CRPC, no known visceral metastasis, ≥2 bone metastases, and either docetaxel-pretreated patients, patients that were unfit for docetaxel treatment or patients that refused to receive chemotherapy. Patients were randomized in a 2:1 ratio to receive Ra-223 injections at 50 kBq/kg plus best standard of care or placebo plus best standard of care. Best standard of care included secondary hormonal therapies (second- or third-line hormonal maneuvers, including, but not limited to, high-dose bicalutamide, prednisone and estrogens) or external beam radiotherapy, but not cytotoxic chemotherapy or radioisotopes. Patients were divided into groups according to total bone alkaline phosphatase (BAP) levels, bisphosphonate use and prior docetaxel treatment. The primary endpoint was OS, while the secondary endpoints were: Time to i) first SRE, ii) total BAP progression, iii) total BAP response, iv) total BAP normalization and v) prostate-specific antigen (PSA) progression; vi) adverse events; and vii) affected quality of life. The trial included 921 male patients (Ra-223, n=614; placebo, n=307). All patients enrolled in the study received up to 6 intravenous injections of Ra-223 or placebo, administered at 4-week intervals (5).
The trial was terminated following the recommendation of an independent committee, due to early evidence of Ra-223 benefit in OS. Ra-223 was shown to significantly improve OS in patients with CRPC and bone metastases, as compared with the placebo group [hazard ratio (HR), 0.70; 95% confidence interval (CI), 0.58–0.83; median OS, 14.9 vs. 11.3 months; P<0.001]. A significant beneficial effect was also observed in all patients except for patients with an Eastern Cooperative Oncology Group Performance Status of ≥2, possibly due to the limited number of patients included in the study. Time to first SRE was also found to be significantly prolonged in the in the Ra-223 group compared with the placebo group (HR, 0.66; 95% CI, 0.52–0.83; median time to first SRE, 15.6 vs. 9.8 months; P<0.001) (6). In addition, the quality of life of the patients was markedly improved following treatment with Ra-223 (5–7), with no differences in severe side-effects (grades 3–4) observed between the Ra-223 and placebo groups (8).
The findings on the aforementioned studies indicate that Ra-223 should not merely be used to visualize bones, but also as a systemic treatment strategy for patients with CRPC developing bone metastasis, either as first-line or salvage therapy. Ra-223 had a significant benefit on survival, delaying the onset of SREs with an acceptable safety profile. This effect had not been previously recorded for other available radiopharmaceuticals (4). The use of Ra-223 has been approved for CRPC patients exhibiting symptomatic bone metastasis without visceral disease, regardless of previous treatment with docetaxel. In fact, the ALSYMPCA study demonstrated a benefit of Ra-223 on OS compared with the placebo, regardless of prior docetaxel treatment (hazard ratio, 0.71 vs. 0.74) (8–10).
The present study reports the case of a patient with CRPC who met the inclusion criteria of the ALPSYMCA trial and was treated with Ra-223.
Case report
A 70-year-old male patient, with no history of concomitant diseases, was diagnosed with T3 Gleason 7 (11) prostate cancer by echography and transrectal biopsy in November 1999 at Hospital Santa Creu I Sant Pau (Barcelona, Spain). At that time, the patient had PSA levels of 12.5 ng/ml (normal range, <4 ng/ml) and a diagnosis of clinical stage cT2aNx disease (12). Therefore, a successful radical prostatectomy was performed in January 2000. The histopathology report of formalin-fixed sections revealed Gleason grade 7 left lobe adenocarcinoma with extraprostatic invasion, non-affected surgical margins and negative lymphatic nodes (pT3pN0).
Following definitive pathological staging, a bone scan was performed in March 2001, which showed a total of 2 osteoblastic bone metastases in both ischiopubic branches. Subsequent to the diagnosis of metastatic prostate cancer, treatment with luteinizing hormone-releasing hormone (LH-RH) analogues was initiated in March 2001. The patient achieved a complete biochemical response (PSA level, 1.03 ng/ml). Hormonal therapy was terminated in May 2004 due to stable disease, according to Prostate Cancer Working Group (PCWG)-2 criteria (13), with undetectable PSA levels and a lack of symptoms, within an intermittent therapy strategy.
In May 2005, the patient presented with a biochemical relapse (PSA level, 77.0 ng/ml) and underwent complete androgen blockade (CAB) with bicalutamide (50 mg) plus LH-RH analogues, such as gosrelin acetate, until November 2006, when treatment was terminated due to undetectable PSA levels.
In December 2007, PSA levels increased again (PSA level, 105 ng/ml). As a result, CAB was re-initiated and continued until October 2010, as the patient developed progressive disease (PD), according to the PCWG-2 criteria. The patient presented with bone pain, therefore, a bone scan was performed. The scan showed an increase in the number and extension of pelvic metastases compared with the bone scan performed in March 2001.
Between September and October 2010, PSA levels increased from 66.8 to 75.6 ng/ml, and BAP levels reached 594 U/l (normal range, 44–147 U/l). In November 2010, treatment with ketoconazole (200 mg/8 h) was administered until July 2011, when PSA increased to 408 ng/ml. A new bone scan showed PD with painful pelvic lesions.
In July 2011, following the recurrence of PD, 10 cycles of docetaxel (75 mg/m2 every 3 weeks) were administered between August 2011 and April 2012, with a good clinical and biochemical response (PSA and BAP decreased to 4.01 ng/ml and 75 U/l, respectively). However, 3 months later, PSA and BAP increased to 29.1 ng/ml and 203 U/l, respectively, and a bone scan observed progression of bone metastasis (new PD). Docetaxel rechallenge (75 mg/m2 every 3 weeks) was initiated in July 2012; although a clinical response initially occurred, the patient developed bone pain with radiological progression following the fourth cycle. The patient also exhibited biochemical progression (PSA, 317 ng/ml; BAP, 402 U/l). As the patient had painful PD without visceral metastases, treatment with Ra-223 was scheduled. A bone scan performed in February 2013 showed widespread bone metastases on the bilateral ribs, dorsolumbar vertebrae, pelvis, sacrum and proximal femurs (Fig. 1).
Figure 1.
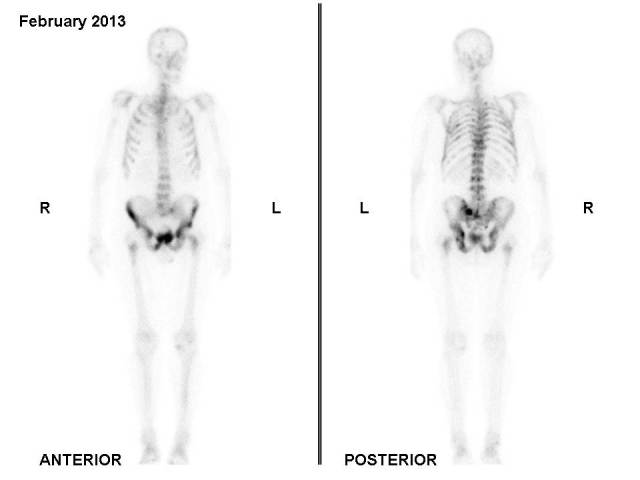
Bone scan performed in February 2013 (prior to 223Ra-dichloride treatment) showing widespread bone metastases on the bilateral ribs, dorsolumbar vertebrae, pelvis, sacrum and proximal femurs.
Between March and August 2013, the patient was treated with 6 doses of Ra-223 (50 kBq/kg; 1 dose/4 weeks). The administered doses were: 2.92 MBq (March 12), 3.64 MBq (April 8), 3.4 MBq (May 8), 3.3 MBq (June 6), 3.4 MBq (July 8) and 3.4 MBq (August 5). During this period, PSA and BAP decreased from 317 to 80.1 ng/ml and from 402 to 81 U/l, respectively, and bone pain was controlled. Furthermore, Ra-223 was well-tolerated without associated bone marrow toxicity. However, 2 months after administration of the final dose of Ra-223, PSA and BAP increased to 314.8 ng/ml and 159 U/l, respectively, and bone pain worsened. A bone scan performed in October 2013 did not show any tracer uptake in the previously observed metastatic lesions; however, PD was evident due to the detection of tracer uptake by new lesions in the backbone and head (Fig. 2).
Figure 2.
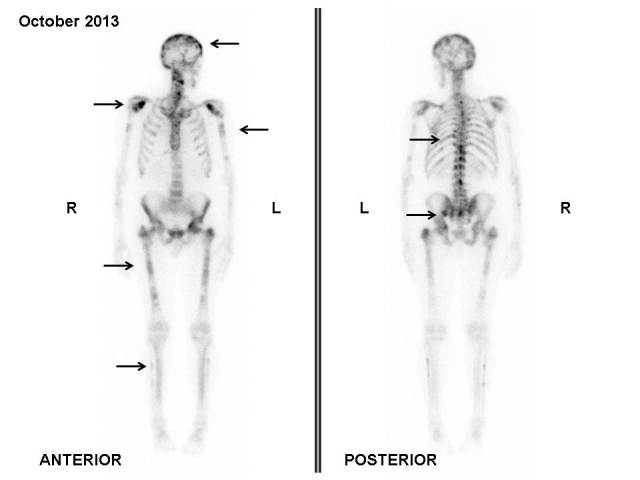
Bone scan performed in October 2013 (2 months after 223Ra-dichloride treatment) showing new lesions in sites with no previous uptake (arrows).
In November 2013, 4 cycles of cabazitaxel (20 mg/m2 every 3 weeks) were administered. A bone scan performed in March 2014 revealed metastatic disease progression (Fig. 3). Changes in the patient's PSA and BAP levels over time are shown in Fig. 4, indicating that the patient is currently in clinical and biochemical progression. The patient was re-evaluated every 9 weeks with measurement of PSA levels. The final follow-up was performed in March 2015, and due to symptomatic deterioration, the patient was treated only for palliative relief subsequent to that date. Written informed consent was obtained from the patient and their family for publication of the present study.
Figure 3.
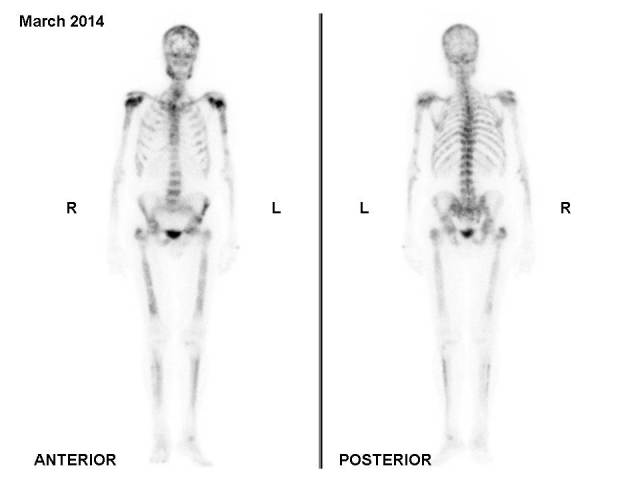
Bone scan performed in March 2014 showing metastatic disease progression, with new bone metastases in the backbone and head.
Figure 4.
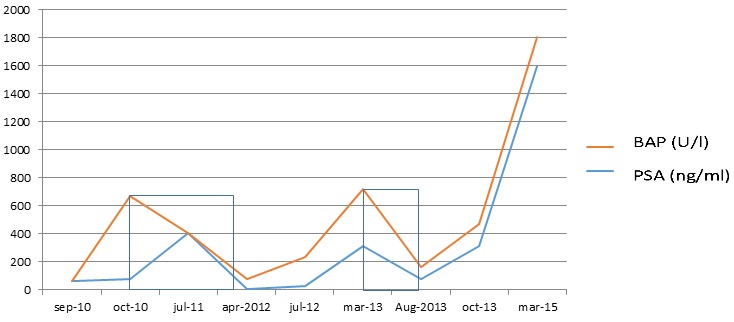
Changes in BAP and PSA levels over time. The two squares indicate the time and response when the patient was treated with docetaxel and 223Ra-dichloride, respectively. BAP, bone alkaline phosphatase; PSA, prostate-specific antigen.
Discussion
Ra-223 is a bone-targeting calcium mimetic α-emitter known to accumulate in areas of increased bone turnover (4–6). It has been reported that α radiation has high LET that generates double-stranded DNA breaks, resulting in elevated cytotoxicity and greater biological effectiveness compared with β radiation (7). At present, clinical experience of Ra-223 is limited compared with β-emitting radiopharmaceuticals, with knowledge of Ra-223 limited to findings from two phase I, three phase II and one phase III clinical studies (4). Furthermore, in contrast to previous studies based on β-emitter radiopharmaceuticals, clinical studies assessing the effectiveness of Ra-223 in relieving bone pain used primary endpoints of OS and secondary endpoints of time to the first symptomatic skeletal-related event (9).
The dosage of Ra-223 depends on body weight and, due to its higher biological effectiveness; administered doses are smaller than those applicable to β-emitting radiopharmaceuticals. A large multicentric double-blinded randomized phase III clinical study showed that 6 doses of 50 kBq/kg administered once every 4 weeks resulted in a significant decrease in bone marker levels and a significant delay in the onset of SREs, resulting in improved OS and pain relief (6). Additional clinical studies compared different dosages of Ra-223 or compared Ra-223 with a placebo and achieved similar results (4–6,14–18).
In the present case, a patient with CRPC treated with 6 intravenous doses of Ra-223 (50 kBq/kg) achieved bone pain relief, and a significant decrease in PSA and BAP levels. In addition, 2 months after the administration of the final dose, a bone scan showed improvement of the widespread bone metastases, with tracer uptake normalization in the metastatic lesions of the ribs and pelvis. PSA response is unusual under Ra-223 treatment, whereas BAP response is common. Therefore, it has been recommended that changes in BAP should be considered as a biomarker of response to Ra-223 treatment; however, this only applies to patients with elevated BAP levels at baseline. In the present patient, PD was indicated by the appearance of new metastatic lesions located in sites where no Ra-223 uptake had previously been reported. Notably, a response to β-emitting isotopes is not commonly observed upon imaging, however, partial responses may be observed with Ra-223. In the present patient, pain relief was achieved, with normalization of tracer uptake in the bone metastases that were previously present, and a decrease in BAP and PSA levels during Ra-223 treatment.
Evaluating drugs for the treatment of prostate cancer poses certain challenges. For example, measurable disease occurs infrequently. As a result, the PCWG addressed this and various other challenges in their consensus recommendations for the conduct of clinical trials. Although the Response Evaluation Criteria in Solid Tumors (RECIST) are considerably well-established recommendations, they do not consider certain key characteristics of prostate cancer; for example, post-therapeutic changes in PSA levels were not addressed by RECIST (19).
Despite the developments made in imaging modalities, interpreting the clinical significance of changes in the size or intensity of bone metastases observed on bone scans is challenging. In cases where a bone scan is the sole indicator of progression, PCWG defines bone disease progression as the appearance of ≥2 new lesions on a bone scan compared with a prior scan for trial entry. When scan findings are suggestive of the appearance of new lesions or a flare reaction, possibly due to trauma, it may prove useful to confirm these results using other imaging modalities (13).
In addition, it should be taken into consideration that the findings of scans can potentially appear worse before they improve, resulting in the erroneous conclusion that the treatment has failed when, in fact, it was too early to assess the effect of the drug (20).
In conclusion, in the present study a patient with CRPC was treated with Ra-223 without major toxicities. Following the development of PD, the patient was treated with cabazitaxel. The results of ongoing randomized trials are required to determine whether Ra-223 or docetaxel rechallenge can be part of a long-term treatment regime.
Acknowledgements
The authors thank Dr Sonia Maciá (Pivotal S.L., Madrid, Spain) for providing advice on how to handle and submit the paper.
References
- 1.World Health Organization: Cancer Pain Relief: With a Guide to Opioid Availability. 2nd. WHO; Geneva, Switzerland: 1996. pp. 36–37. [Google Scholar]
- 2.http://www.nccn.org/professionals/physician_gls/pdf/pain.pdf. [Jan;2016 ];National Comprehensive Cancer Network (NCCN): NCCN Guidelines for Supportive Care: Adult cancer pain. 2013 Version 2. Accessed. [Google Scholar]
- 3.Hamdy NA, Papapoulos SE. The palliative management of skeletal metastases in prostate cancer: Use of bone-seeking radionuclides and bisphosphonates. Semin Nucl Med. 2001;31:62–68. doi: 10.1053/snuc.2001.18767. [DOI] [PubMed] [Google Scholar]
- 4.Herranz Anido U, Fernández Calvo O, Afonso Afonso FJ, de Rodríguez Martínez Llano S, Lázaro Quintela M, León Mateos L, Vázquez Estévez S, Antón Aparicio LM. Radium-223 dichloride: A new paradigm in the treatment of prostate cancer. Expert Rev Anticancer Ther. 2015;15:339–348. doi: 10.1586/14737140.2015.999045. [DOI] [PubMed] [Google Scholar]
- 5.Parker C, Nilsson S, Heinrich D, Helle SI, O'Sullivan JM, Fosså SD, Chodacki A, Wiechno P, Logue J, Seke M, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med. 2013;369:213–223. doi: 10.1056/NEJMoa1213755. [DOI] [PubMed] [Google Scholar]
- 6.Sartor O, Coleman R, Nilsson S, Heinrich D, Helle SI, O'Sullivan JM, Fosså SD, Chodacki A, Wiechno P, Logue J, et al. Effect of radium-223 dichloride on symptomatic skeletal events in patients with castration-resistant prostate cancer and bone metastases: Results from a phase 3, double-blind, randomised trial. Lancet Oncol. 2014;15:738–746. doi: 10.1016/S1470-2045(14)70183-4. [DOI] [PubMed] [Google Scholar]
- 7.Nilsson S, Franzén L, Parker C, Tyrrell C, Blom R, Tennvall J, Lennernäs B, Petersson U, Johannessen DC, Sokal M, et al. Two-year survival follow-up of the randomized, double-blind, placebo-controlled phase II study of radium-223 chloride in patients with castration-resistant prostate cancer and bone metastases. Clin Genitourin Cancer. 2013;11:20–26. doi: 10.1016/j.clgc.2012.07.002. [DOI] [PubMed] [Google Scholar]
- 8.Nilsson S, Strang P, Aksnes AK, Franzèn L, Olivier P, Pecking A, Staffurth J, Vasanthan S, Andersson C, Bruland ØS. A randomized, dose-response, multicenter phase II study of radium-223 chloride for the palliation of painful bone metastases in patients with castration-resistant prostate cancer. Eur J Cancer. 2012;48:678–686. doi: 10.1016/j.ejca.2011.12.023. [DOI] [PubMed] [Google Scholar]
- 9.Nilsson S, Larsen RH, Fosså SD, Balteskard L, Borch KW, Westlin JE, Salberg G, Bruland OS. First clinical experience with alpha-emitting radium-223 in the treatment of skeletal metastases. Clin Cancer Res. 2005;11:4451–4459. doi: 10.1158/1078-0432.CCR-04-2244. [DOI] [PubMed] [Google Scholar]
- 10.Nilsson S, Franzén L, Parker C, Tyrrell C, Blom R, Tennvall J, Lennernäs B, Petersson U, Johannessen DC, Sokal M, et al. Bone-targeted radium-223 in symptomatic, hormone-refractory prostate cancer: A randomised, multicentre, placebo-controlled phase II study. Lancet Oncol. 2007;8:587–594. doi: 10.1016/S1470-2045(07)70147-X. [DOI] [PubMed] [Google Scholar]
- 11.Humphrey PA. Gleason grading and prognostic factors in carcinoma of the prostate. Mod Pathol. 2004;17:292–306. doi: 10.1038/modpathol.3800054. [DOI] [PubMed] [Google Scholar]
- 12.Prostate Cancer: Diagnosis and Treatment. National Collaborating Centre for Cancer (UK); Cardiff: 2008. National Collaborating Centre for Cancer (UK): TNM staging for prostate cancer. Appendix 2. [Google Scholar]
- 13.Sonpavde G, Pond GR, Armstrong AJ, Galsky MD, Leopold L, Wood BA, Wang SL, Paolini J, Chen I, Chow-Maneval E, et al. Radiographic progression by Prostate Cancer Working Group (PCWG)-2 criteria as an intermediate endpoint for drug development in metastatic castration-resistant prostate cancer. BJU Int. 2014;114:E25–E31. doi: 10.1111/bju.12589. [DOI] [PubMed] [Google Scholar]
- 14.Sgouros G, Roeske JC, McDevitt MR, Palm S, Allen BJ, Fisher DR, Brill AB, Song H, Howell RW, Akabani G, et al. MIRD pamphlet no. 22 (abridged): Radiobiology and dosimetry of alpha-particle emitters for targeted radionuclide therapy. J Nucl Med. 2010;51:311–328. doi: 10.2967/jnumed.108.058651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lassmann M, Nosske D. Dosimetry of Ra-223-chloride: Dose to normal organs and tissues. Eur J Nucl Med Mol Imaging. 2013;40:207–212. doi: 10.1007/s00259-012-2265-y. [DOI] [PubMed] [Google Scholar]
- 16.Pandit-Taskar N, Larson SM, Carrasquillo JA. Bone-seeking radiopharmaceuticals for treatment of osseous metastases, part 1: α therapy with 223Ra-dichloride. J Nucl Med. 2014;55:268–274. doi: 10.2967/jnumed.112.112482. [DOI] [PubMed] [Google Scholar]
- 17.Parker CC, Pascoe S, Chodacki A, O'Sullivan JM, Germá JR, O'Bryan-Tear CG, Haider T, Hoskin P. A randomized, double-blind, dose finding, multicenter, phase 2 study of radium chloride (Ra 223) in patients with bone metastases and castration-resistant prostate cancer. Eur Urol. 2013;63:189–197. doi: 10.1016/j.eururo.2012.09.008. [DOI] [PubMed] [Google Scholar]
- 18.Carrasquillo JA, O'Donoghue JA, Pandit-Taskar N, Humm JL, Rathkopf DE, Slovin SF, Williamson MJ, Lacuna K, Aksnes AK, Larson SM, et al. Phase I pharmacokinetic and biodistribution study with escalating doses of 223Ra-dichloride in men with castration-resistant metastatic prostate cancer. Eur J Nucl Med Mol Imaging. 2013;40:1384–1393. doi: 10.1007/s00259-013-2427-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, Eisenberger MA, Higano C, Bubley GJ, Dreicer R, et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: Recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol. 2008;26:1148–1159. doi: 10.1200/JCO.2007.12.4487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Carducci MA, Padley RJ, Breul J, Vogelzang NJ, Zonnenberg BA, Daliani DD, Schulman CC, Nabulsi AA, Humerickhouse RA, Weinberg MA, et al. Effect of endothelin-A receptor blockade with atrasentan on tumor progression in men with hormone-refractory prostate cancer: A randomized, phase II, placebo-controlled trial. J Clin Oncol. 2003;21:679–689. doi: 10.1200/JCO.2003.04.176. [DOI] [PubMed] [Google Scholar]