

Abstract
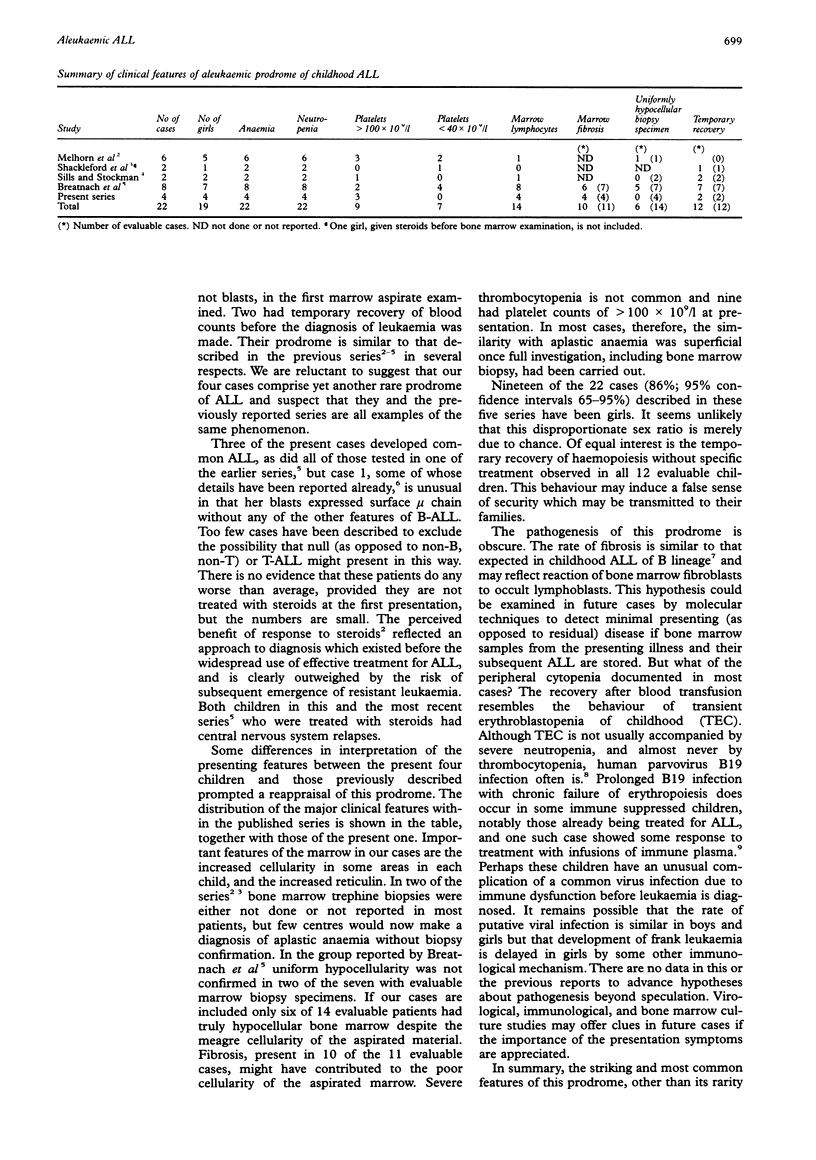
AIMS: To document the features of the so-called aplastic presentation of childhood acute lymphoblastic leukaemia (ALL) and to determine whether this prodrome can be distinguished from aplasia. METHODS: The peripheral blood and bone marrow appearances of all cases of childhood ALL presenting in one health region of England in 13 years and eight months were reviewed. All cases presenting with cytopenia without circulating blasts and marrow aspirates with no infiltrate of blasts were studied in detail. RESULTS: Four of 305 (1.3%) children presented in this way. All four had reticulin fibrosis and increased cellularity in all or part of the marrow biopsy specimen. All were girls. Three had common and one surface membrane immunoglobulin positive ALL. Reassessment of this prodrome, by combining the features of four previously reported series of similar cases with the present one, highlighted the female preponderance (19 of 22 cases), bone marrow fibrosis (10 of 11 evaluable cases), prominent bone marrow lymphocytes (14 of 22 cases) and temporary recovery (all 12 evaluable cases). Six of 14 evaluable cases had bone marrow biopsy specimen appearances of apparently uniform hypocellularity, but only one of these did not have fibrosis. CONCLUSIONS: If, in addition to an aspirate, a bone marrow trephine biopsy is carried out the prodrome can be distinguished from aplasia in most cases. The similarity of this prodrome to aplastic anaemia is merely superficial. Clinicians and morphologists may fail to appreciate the implications of this mode of presentation if the term "aplastic" continues to be used to describe this aleukaemic prodrome of ALL.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Melhorn D. K., Gross S., Newman A. J. Acute childhood leukemia presenting as aplastic anemia: the response to corticosteroids. J Pediatr. 1970 Oct;77(4):647–652. doi: 10.1016/s0022-3476(70)80207-4. [DOI] [PubMed] [Google Scholar]
- Pak C. Y., Eun H. M., McArthur R. G., Yoon J. W. Association of cytomegalovirus infection with autoimmune type 1 diabetes. Lancet. 1988 Jul 2;2(8601):1–4. doi: 10.1016/s0140-6736(88)92941-8. [DOI] [PubMed] [Google Scholar]
- Reid M. M. B-ALL without Burkitt characteristics in children. Br J Haematol. 1988 Aug;69(4):574–574. doi: 10.1111/j.1365-2141.1988.tb02419.x. [DOI] [PubMed] [Google Scholar]
- Shackelford G. D., Bloomberg G., McAlister W. H. The value of roentgenography in differentiating aplastic anemia from leukemia masquerading as aplastic anemia. Am J Roentgenol Radium Ther Nucl Med. 1972 Nov;116(3):651–654. doi: 10.2214/ajr.116.3.651. [DOI] [PubMed] [Google Scholar]
- Sills R. H., Stockman J. A., 3rd Preleukemic states in children with acute lymphoblastic leukemia. Cancer. 1981 Jul 1;48(1):110–112. doi: 10.1002/1097-0142(19810701)48:1<110::aid-cncr2820480121>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- Young N. Hematologic and hematopoietic consequences of B19 parvovirus infection. Semin Hematol. 1988 Apr;25(2):159–172. [PubMed] [Google Scholar]