

Abstract
This study investigated patients’ attitudes to doctors in different attires in a hospital setting. A cross-sectional descriptive survey asked 586 adult patients to rate and rank photographs of a doctor in each of the following attires: scrubs, professional informal, professional formal, smart casual, casual and white coat. They were also asked to choose the single most important feature of a doctor's appearance out of six predetermined choices. Patients had most confidence in doctors wearing the white coat, followed by professional informal. Casual attire was the least confidence inspiring. No two attires were deemed to be equally rated or ranked. Varying demographic groups within the hospital rated and ranked some attire differently. Daily laundered clothing was considered to be the most important feature. With patients’ clear preference for white coats, its reintroduction should be given consideration and education regarding the cleanliness of scrubs may increase patient confidence.
Key Words: attire, dress, patient preference, physician, doctor, white coat
Introduction
A doctor's attire has always been considered an important means of establishing a good first impression in any doctor–patient interaction.1,2 It is a symbol of recognition and trust and is believed to be essential in developing a successful professional relationship.3,4 For these reasons, the white coat established itself as the fundamental image of the medical profession during the 20th century. The familiar, recognisable white coat has provided patients with the impression of cleanliness, high expectations of care and professionalism. However, in the UK, there has been a move away from the white coat for fear of the spread of infection.5 A recent study found that 56% of patients preferred doctors to wear white coats,6 a preference supported by other studies.1,7–11 Most found that the white coat improved many aspects of doctor–patient interaction and that the doctor was seen to be more professional, scientific, hygienic and easily identifiable.7,8 But do patients care or even notice?
The move away from the white coat has inspired much debate on the appropriate attire for a consulting physician. For manydoctors there is a need to ascertain an acceptable and appropriate dress code for practice. The aim of this study is to assess whether patients believe that the doctor's attire is an important aspect of the doctor–patient relationship and, if so, which they consider to be the most confidence-inspiring attire.
Methods
A cross-sectional descriptive survey was conducted on 586 adult patients at Airedale General Hospital in June 2008. Participants were invited to take part in an anonymous, self-completion, patient opinion survey to gauge patients’ degree of confidence in photographs of doctors in differing attire (Fig 1). Outpatients attending clinics, inpatients on the wards and accident and emergency (A&E) patients were approached for their participation. The survey encompassed a wide range of medical, surgical and emergency specialties. Patients of 18 years or older were invited to take part unless it was deemed clinically inappropriate by a member of the medical or nursing staff. Verbal consent was obtained prior to distribution of the questionnaire and there was a tick-box opt-out option for their responses not to be included in analysis.
Fig 1.

Description of attires and their corresponding photographs for male and female doctors.
Patients were asked to complete a questionnaire comprising of four parts (available from the authors on request). Part one requested demographic information including gender, age and location within the hospital (inpatient, outpatient or A&E patient). Part two was completed after patients had reviewed a set of six photographs of a male doctor in different attire (Fig 1a). They were asked to rate each photograph on how confident they would feel about the ability of each doctor. A five-point Likert scale was adopted for this purpose, ranging from ‘not at all’ to ‘very’. The patient was then asked to rank the six photographs in order from ‘most confident in their ability’ to ‘least confident in their ability’. The purpose of this was to make participants specify a preference if two or more attires were equally rated on the Likert scale. Part three asked patients to repeat this with a set of six photographs of a female doctor dressed in equivalent clothing (Fig 1b). Part four asked patients to choose the single most important feature of a doctor's appearance out of six predetermined choices. There was also a seventh choice, where the patient could specify their own important feature if they felt that the single most important feature had been omitted.
The photographs were presented to the patients randomly and labelled only by a number as opposed to the attire descriptors so as not to influence their choices. The same male and female subjects were used for each photograph with the clothing being the only variable. In each photograph the doctors had a stethoscope placed around their neck, an identification badge on display and a neutral facial expression. The stance, hairstyle and background were kept constant in each photograph. Photographs, as opposed to live physicians, were deemed to be the most appropriate way of isolating the variable of attire from other variables such as manner, demeanour and tone of voice.
Responses from the survey were compared across demographic groups (gender, age and location of patient within hospital). Statistical analysis comprised student's t-tests and analysis of variance (ANOVA) of the parametric ranking data, while Mann-Whitney U testing and Kruskall-Wallis analysis of variance were performed on the non-parametric Likert rating data. A Bonferroni correction was made to give sufficient protection against a type I error occurring due to multiple comparisons, such that α = 0.0036.
Results
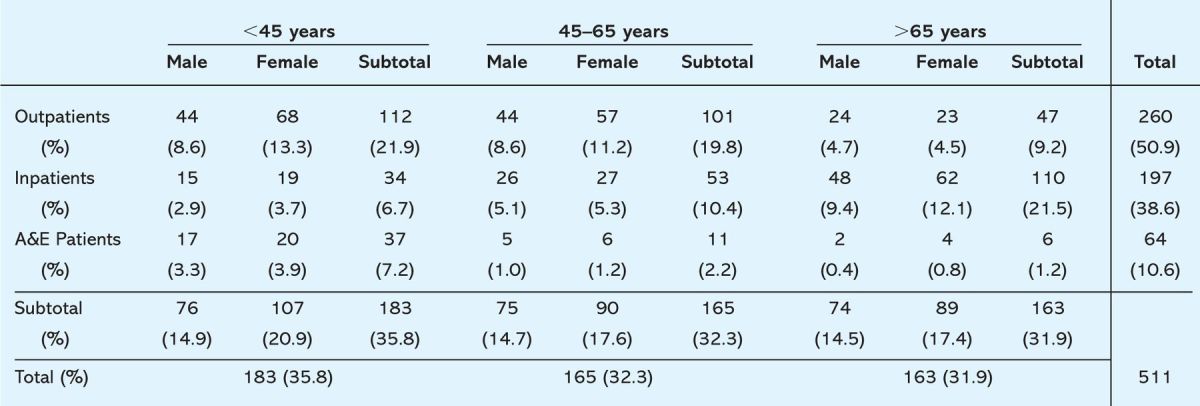
The population surveyed consisted of 586 patients (Table 1). Respondents returned 511 (87.2%) completed surveys. There were 75 partially or uncompleted surveys. Of the 511 questionnaires, there were 225 (44.0%) male and 286 (56.0%) female respondents. The number of patients aged less than 45 was 183 (35.8%); 165 patients (32.3%) were aged between 45 and 65; and 163 patients (31.9%) were aged more than 65. Of the 511 patients, 197 (38.6%) were inpatients, 260 (50.9%) were outpatients and 54 (10.5%) patients completed the questionnaire in A&E.
Table 1.
Number and proportion of patients surveyed in each demographic category (sex, age group, location).
For analysis of the Likert ratings the degree of patient confidence in a doctor's attire was given a numerical value. The value ‘1’ equated to ‘not at all confident’ through to the value ‘5’ which equated to ‘very confident’. For analysis of the photograph rankings the descriptor ‘most confident’ was given a score of 1, while ‘least confident’ was given a score of 6.
Figure 2a demonstrates that white coats were rated the most confidence-inspiring attire (mean Likert rating 4.17 (95% CI 4.12 to 4.23)). Patients similarly ranked white coats above other attires. Overall, all dress styles were rated by the patients as having a degree of confidence above neutral (Likert rating >3) except for the casual attire which gained a mean Likert rating score of 2.09 (95% CI 2.02 to 2.15).
Fig 2a–d.
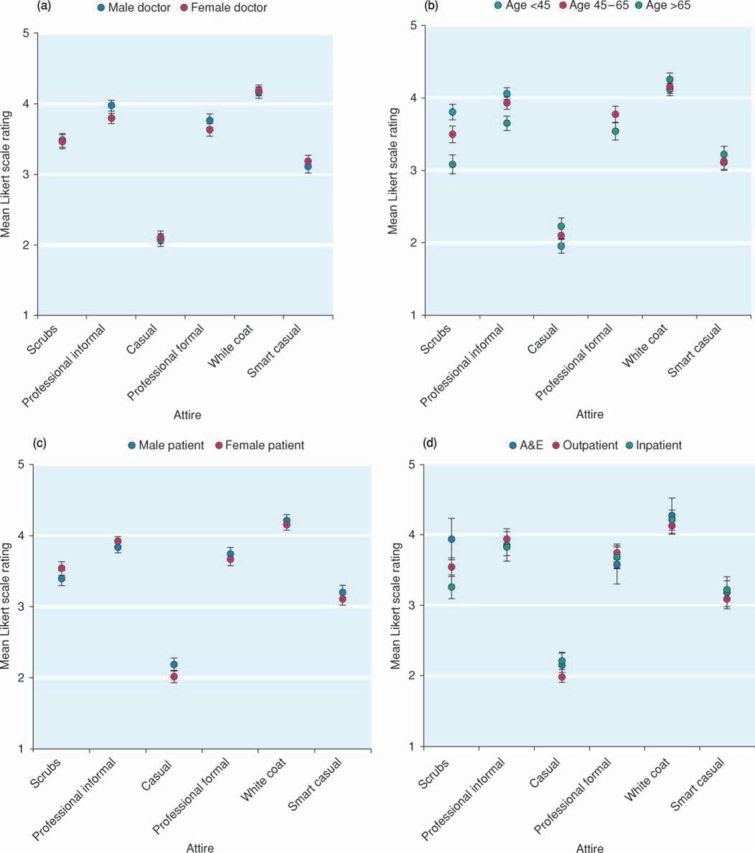
Patient mean Likert ratings (95% confidence intervals) for each attire.
There was no significant difference between the Likert rating data for female and male doctors for each attire, except for those wearing professional informal attire (p = 0.0001). Patients gave more positive ratings for the male doctor wearing professional informal attire compared to the female doctor in corresponding attire (Fig 2a).
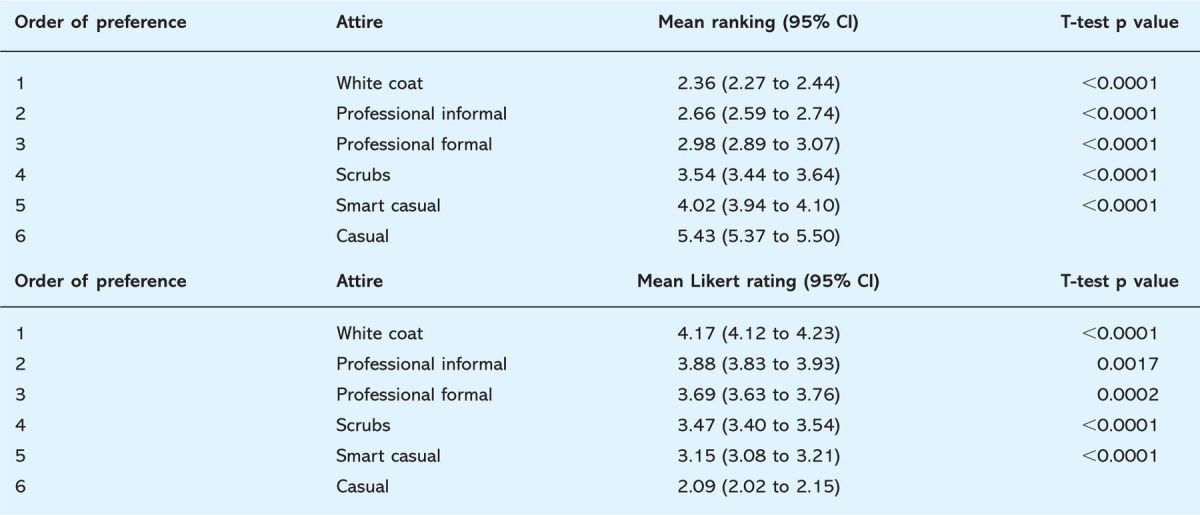
Table 2 shows a comparison of each attire with the next most confidence inspiring outfit. Statistical testing showed there to be a significant heterogeneity in patients’ rating of each attire. Overall, trends that were observed in patient's ratings were replicated in the ranking of each attire.
Table 2.
Comparison of mean ranking and Likert rating for each attire.
Patient age
The Likert rating data showed a significant difference between age groups with regards to scrubs (p<0.0001) as shown in Fig 2b. Patients less than 45 years old gave scrubs a mean Likert rating of 3.80 (95% CI 3.69 to 3.91) as opposed to a mean rating of 3.49 (95% CI 3.38 to 3.61) in patients aged 45 to 65 years and 3.08 (95% CI 2.95 to 3.21) in patients aged over 65 years. Furthermore, significant difference in opinion was also revealed between the under 45s and the over 65s with regard to professional informal (p<0.0001), and casual (p=0.002) attire. Similar results were obtained on analysis of the ranking data.
Patient sex
The only significant differences that were noted between male and female participants were their Likert ratings of casual attire (p=0.001). Male participants (mean rating 2.18 (95% CI 2.09 to 2.27)) had greater confidence in doctors wearing casual attire compared to female participants (mean rating 2.01 (95% CI 1.93 to 2.10)) as shown in Fig 2c. Again, patients ranked each attire similarly.
Patient location
Figure 2d reveals that participants had the most confidence in doctors wearing scrubs in the A&E setting (mean Likert rating 3.94 (95% CI 3.78 to 4.09)). Participants had significantly less confidence in scrubs worn in inpatient (p<0.0001) and outpatient (p=0.0032) departments. A significant difference was also found with regards to casual attire (p=0.002) worn in different locations. It was preferred in an inpatient setting (mean Likert rating 1.97 (95% CI 1.90 to 2.06)) compared to the outpatient setting (mean Likert rating 2.21 (95% CI 2.10 to 2.32)). Similar results were reflected in analysis of the ranking data. However, smart casual attire received significantly different rankings when worn in inpatients compared to outpatients (p=0.0003) and A&E (p=0.004).
Most important feature of a doctor's appearance
Part 4 of the questionnaire returned the results that a majority (46%) of patients responding to the questionnaire regarded ‘daily laundered clothing’ as the single most important feature of a doctor's appearance. ‘A white coat worn at all times’ was the second most common preference (18%). Other noteworthy comments were that an identity badge should be in clear view and that the doctor should look smart and have a smile.
Discussion
Patients were found to be more confident in doctors wearing white coats across all demographic groups. This was concordant with other similar studies, which also found that white coats were the preferred patient choice.1,6–11 However, our findings contradict the findings of Lill and Wilkinson which found patients prefer doctors to dress in a semiformal style.5 Many patients commented that there was a need for a means by which to identify a doctor, besides an identification badge. It could be argued that the white coat fulfils this valuable requirement. The British government changed the traditional use of white coats at the beginning of 2008 as part of their plans to tackle hospital infection and advised doctors to ‘avoid using white coats when providing patient care’.12 However, patients had most confidence in doctors wearing a white coat, perhaps because they are unaware of its suspected infection implications. It is important to remember that trust and confidence in the patient-doctor partnership should not be undermined in this current climate of heightened concern over infection risk.
Professional informal attire was the second most popular choice. The reason for this is probably due to patients’ exposure to this dress type in clinical settings, as well as patients’ perceptions of this attire being smart and professional. Many commented on the fact that they found professional formal attire too intimidating and that even though it conveyed authority, some regarded it as being slightly pretentious. Casual attire was found to be least confidence-inspiring as the unkempt appearance of the doctor was believed, by many patients, to be associated with a lack of ability. Casual attire was found to be the only dress style that had a mean Likert rating less than neutral, suggesting casual dress has a negative effect on the confidence inspired by the doctor.
Concerning patients’ responses in relation to their age, it is interesting to note that the three age groups were closely united in their ranking and rating of doctors in white coats. This may be due to the familiarity with white coats that all age groups share, as a traditional symbol for the medical profession. However, there was a much greater spread in responses regarding scrubs. Older participants found scrubs much less appealing than younger people did. The reasons for this are speculative: it might be suggested that younger generations are more familiar with the attire and its association with cleanliness, through its frequent portrayal in popular culture and the media. Similarly it may be suggested that older people's views are more traditional, and that scrubs (as a relatively new outfit in hospitals) do not impart the degree of professionalism and confidence that a white coat or a suit does. When debating any possible alterations in national dress codes for doctors, it is important to consider the variation in the opinions of different age groups. One must take into account the current and ever increasing ageing population utilising the health service, as well as the younger demographic of patients who will be occupying services in the future.
Patients’ sex had little bearing on their ranking and Likert rating of the doctors. As a result, suggestions cannot be made for future changes in attire on single-sex wards or clinics. Surprisingly, inpatients were most tolerant of casual attire. However, it was not surprising to discover that patients in A&E favoured scrubs compared to patients in other locations. It is suspected that this is due to patient perception that A&E is an area where trauma and open wounds are encountered frequently, and as a result requires a cleaner environment. Furthermore, participants may be more familiar with scrubs in the A&E setting through their depiction in popular medical television programmes.
While patients chose daily laundered clothing as the most important feature of a doctor's attire it is not possible to ensure that all doctors launder their clothing. At present, it may be feasible to provide doctors with clean scrubs each day. There is no denying that this would aid in the ongoing struggles with infection control but it does not adhere to patients’ preference in dress styles and, as previously mentioned, it raises the issue of identification and the confidence that the attire imparts. It could be inferred that the results obtained from this survey support the idea of hospital laundered white coats.
Certain limitations of this study have been identified. It only surveyed one hospital over a brief period and as a result secular changes and varying demographics may not have been accounted for. The survey made no reference to the specific type of doctor shown in the photographs (although some patients associated professional formal attire with a consultant, scrubs with a surgeon and the casual attire with a general practitioner). In future studies it may be appropriate to investigate particular dress types of doctors associated with their corresponding specialty and to seek the opinion of doctors and other healthcare professionals.
Conclusion
A physician's attire has long been known to play a central role in the patient's first impressions, especially in inspiring confidence in the doctor. In this study, patients showed a significant preference for white coats in all hospital settings. Its reintroduction could be considered if daily laundering and short sleeves were implemented to reduce the infection risk which is believed to be associated with this particular dress type. An education campaign, informing patients of the reasons that scrubs are adopted in certain hospital settings would serve to increase patients’ confidence in this attire. These changes may increase confidence in the doctor–patient relationship, which in turn will lead to beneficial health outcomes for more patients.
Acknowledgements
The authors would like to extend their thanks to Dr Graham Law, epidemiological statistician at the University of Leeds, for his help and advice in this study.
References
- 1.McKinstry B, Wang J. Putting on the style: what patients think of the way their doctor dresses. Br J Gen Pract 1991;41:275–8. [PMC free article] [PubMed] [Google Scholar]
- 2.Hochberg MS. The doctor's white coat – an historical perspective. Am Med Assoc 2007;9:310–4. [DOI] [PubMed] [Google Scholar]
- 3.Short D. First impressions. Br J Hosp Med 1993;50:270–1. [PubMed] [Google Scholar]
- 4.Mckenna G, Lillywhite GRR, Maini N. Patient preferences for dental clinical attire: a cross-sectional survey in a dental hospital. Br Dent J 2007;203:681–5 10.1038/bdj.2007.1109 [DOI] [PubMed] [Google Scholar]
- 5.Lill MM, Wilkinson TJ. Judging a book by its cover: descriptive survey of patients’ preferences for doctors’ appearance and mode of address. BMJ 2005;331:24–31. 10.1136/bmj.331.7531.1524 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Douse J, Derrett-Smith E, Dheda K, Dilworth JP. Should doctors wear white coats? Postgrad Med J 2004;80:284–6. 10.1136/pgmj.2003.017483 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gooden BR, Smith MJ, Tattersall SJ, Stockler MR. Hospitalised patients’ views on doctors and white coats. Med J Aust 2001;175:219–22. [DOI] [PubMed] [Google Scholar]
- 8.Harnett PR. Should doctors wear white coats? Med J Aust 2001;174:343–4. [DOI] [PubMed] [Google Scholar]
- 9.Rehman SU, Nietert PJ, Cope DW, Kilpatrick AO. What to wear today? Effect of doctor's attire on the trust and confidence of patients. Am J Med 2005;118:1279–86. 10.1016/j.amjmed.2005.04.026 [DOI] [PubMed] [Google Scholar]
- 10.Manahem S, Shvartzman P. Is our appearance important to our patients? Fam Pract 1998;15:391–7. 10.1093/fampra/15.5.391 [DOI] [PubMed] [Google Scholar]
- 11.Ikusaka M, Kamegai M, Sunaga T. et al Patients’ attitudes towards consultations by a physician without a white coat in Japan. Intern Med 1999;38:533–6. 10.2169/internalmedicine.38.533 [DOI] [PubMed] [Google Scholar]
- 12.Department of Health. Uniforms and workwear: an evidence base for developing local policy. London: DH, 2007. www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_078433 [Google Scholar]