

Abstract
The objective of this study was to offer HIV testing to all patients attending the acute medical admissions unit (AMU) in Newcastle upon Tyne to assess feasibility, acceptability and point prevalence in accordance with the 2008 UK National HIV testing guidelines. A prospective audit was performed offering HIV testing to all patients with the capacity to give verbal consent who attended the AMU. In total, 3,753 eligible patients were admitted during the audit period and 586 (15.6%) were considered for testing. Of those approached, 108 (18.4%) were clinically ineligible to test and 478 were offered a test. In the 396 patients who consented (82.8%), there were two new HIV diagnoses (point prevalence 0.5%). Offering HIV testing in an AMU setting is feasible and acceptable to patients. The high uptake rate but low proportion of admissions tested suggests a lack of confidence of medical staff in offering a test. Misconceptions regarding HIV testing remain and greater education is required for healthcare workers.
Key Words: diagnosis, HIV, testing
Introduction
The number of people living with HIV in the UK continues to rise, with an estimated 86,500 infected at the end of 2009, of whom over a quarter (26%) were unaware of their infection.1 Late diagnosis (CD4 cell count <350 cells/ml, or AIDS defining illness at diagnosis) remains a problem and is associated with increased mortality and morbidity, impaired response to highly active antiretroviral treatment (HAART) and increased cost to healthcare services.1–3 It has previously been reported that in Newcastle, 63% of new diagnoses in 2007 and 59% in 2008 were very late presenters (CD4 < 200 cells/ul)4 as compared to 30% nationally.1 Approximately 50% of these very late presenters have been seen with indicator diseases (diagnoses that should prompt the offering of an HIV test) in the recent past by healthcare professionals without the diagnosis of HIV having been made.
In 2008, the UK National guidelines for HIV testing were produced with the intention of facilitating an increase in HIV testing in all healthcare settings as recommended by the UK's chief medical officer and chief nursing officer in order to reduce the proportion of individuals with undiagnosed HIV infection.5 At present, the majority of testing occurs in specified settings such as genitourinary medicine (GUM) clinics and antenatally where an ‘opt out’ system is in place. The 2008 guidelines recommend that HIV testing should be offered to all general medical admissions where the reported prevalence of HIV is >2/1,000. Newcastle upon Tyne Primary Care Trust had a community prevalence of HIV of three per 1,000 in 2007 (with local authority diagnosed prevalence for Newcastle upon Tyne of 1.62 per 1,000 in 2010). This article describes a prospective audit that was undertaken offering HIV testing to all patients attending the acute medical admissions unit (AMU) in Newcastle upon Tyne to assess feasibility, acceptability and point prevalence.
Methods
The audit was based in the AMU at the Royal Victoria Infirmary, Newcastle upon Tyne, a large 700-bed tertiary receiving centre. The AMU is the main admissions unit and receives approximately 20,000 admissions annually from both accident and emergency (A&E) and general practice. The aim was to offer HIV testing to all patients aged over 18 attending the AMU with capacity for verbal consent during two block periods of six and 11 weeks in 2009 (14 September to 26 October) and 2010 (4 January and 19 March). The first period was physician led, the second predominantly physician assistant led (band 4 associate practitioners previously appointed in the unit to provide physician support with phlebotomy and other tasks).
Training was undertaken and led by the infectious diseases team in the form of a presentation at a medical meeting and small group tutorials. This training covered issues relating to how to obtain consent for a test and what the test involved. An information leaflet regarding HIV testing and highlighting the reasons for testing was given to patients who were assessed to have mental capacity to consent on admission. The staff member approaching a patient for testing was asked to complete a standardised one-page proforma documenting patients' demographic, whether or not consent had been obtained, and reasons for non-consent or refusal. This was filed in the patient's notes at the end of the audit. Once consent was obtained, a clotted blood sample was taken and a fourth generation (Enzygnost HIV Integral II) antigen/antibody test was used at a cost of £3.88 per test with the aim of providing the result within 36 hours.
A patient was informed of a non-reactive (negative) result if they remained an inpatient. Those patients who had subsequently been discharged were advised that unless they were contacted, they could assume that their test was negative (contact details including home address, home and mobile telephone numbers, and general practitioner's address were collected on each patient on admission in case a discharged patient's test proved to be reactive). Informing all patients with a negative result was considered in this audit but restricted resources, unfortunately, did not permit this. Not informing patients of negative results is routinely practised in genitourinary and antenatal clinics where the offer of HIV testing is widely undertaken.6 Reactive (positive) results were directed to the on-call infectious diseases team who arranged further testing and counselling. Statistical analysis on the results was performed using Microsoft Excel 2003 in the form of Student's t test and chi-squared analysis.
Results
In total, 3,753 eligible patients were admitted during the audit period and 586 (15.6%) were considered for testing (Table 1). Of those approached, 108 (18.4%) were clinically ineligible to test due to lack of capacity to consent. Of the 478 patients offered a test, 396 consented (uptake rate 82.8%). Uptake rates were significantly lower in the over 65 age group (69.3%) compared with the under 65s (80.3%) (p=0.012).
Table 1.
Characteristics of those tested/not tested.
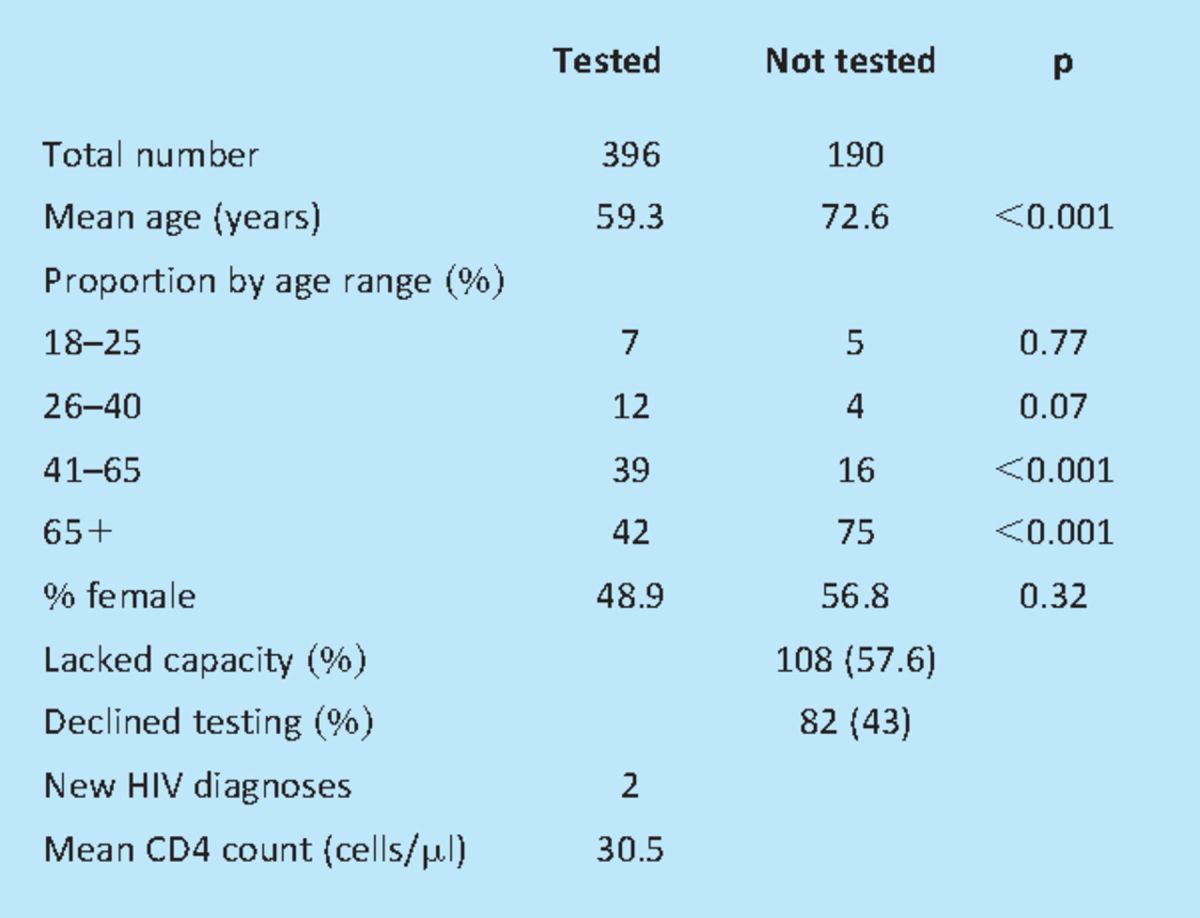
There were two new HIV diagnoses (point prevalence 0.5%). In each case the presenting complaint was breathlessness with a final diagnosis of Pneumocystis jirovecii pneumonia (PJP). The first case was a 36-year-old man from Zambia with a CD4 cell count of 15 cells/ml (HIV viral load 433,736 copies/ml). The second was a 46-year-old MSM (man who has sex with men) with a CD4 cell count of 46 cells/ml (HIV viral load 451,316 copies/ml).
In the first testing period, the majority of the tests (55.1%) were performed by foundation year 1 and 2 (FY1/2) doctors with 36% performed by core medical trainees (CMT) and 8.5% by specialty registrars (Fig 1). In the second audit period, 78.9% were performed by the physician assistants.
Fig 1.

Proportion of tests performed by healthcare worker grade. Physician assistants (PAS) did not take part in audit period 1. CMT = core medical trainee; FY = foundation year doctor; PA = physician assistant; SpR = specialist registrar.
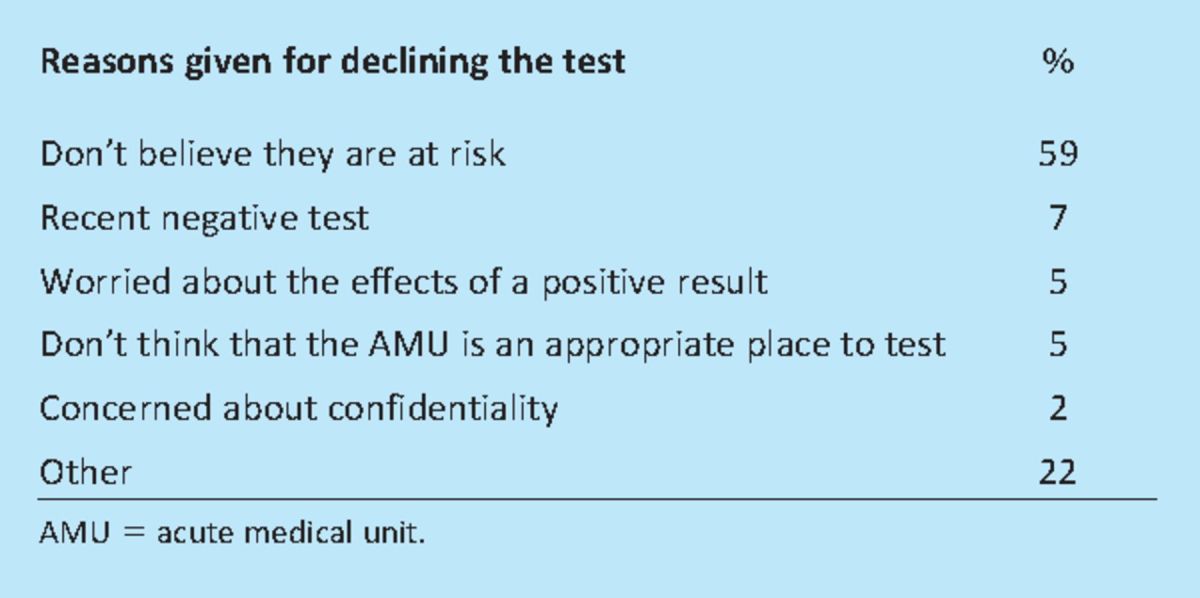
Eighty-two patients (43%) with capacity refused testing with 59% believing that they were not at risk and 5% believing that the AMU was an inappropriate place to be tested (Table 2). Patients approached but not tested were on average 13.3 years older than those who consented (p<0.001). In total, 95% of results were available within 36 hours with 100% within 48 hours.
Table 2.
Patient barriers to testing.
Conclusions
This audit demonstrates that HIV testing in an acute medical admissions setting is feasible and acceptable to the majority of patients with a high uptake rate of 82.8%. This is consistent with studies in similar clinical areas that reported uptake rates of 88.2%7 but higher than that reported in A&E settings (61%).8
It was disappointing that a larger proportion of admissions were not offered testing. The high acceptability rates seen in this study suggest that the main barrier to testing is not with the patients but more with the healthcare workers not offering a test. Physician barriers to testing, although not formally assessed, were ascertained by interviews with medical staff during the project. Those identified are similar to those in other studies9 including restrictions on time (large volume of patients admitted daily) and not wanting to repeat phlebotomy when admission blood had been taken in A&E. It is also worth noting that despite publication of the HIV testing guidelines and a general drive to increase testing, there remain many misperceptions about what an HIV test entails. Many believed extensive pre-test counselling was required and concerns regarding having to declare an HIV test on insurance or mortgage applications persist. It is clear that increased awareness of HIV and testing is required for all grades of medical staff.
The two new HIV diagnoses were both classified as late diagnoses, presenting with an AIDS-defining diagnosis and low CD4 cell counts. Both were from groups considered high risk for HIV infection and an offer of an HIV test in this setting should be a standard of care. Of note, each patient had been in contact with the healthcare profession on at least two occasions within the last 12 months without the diagnosis of HIV having been considered or an HIV test being offered. These represent missed opportunities for testing and is a feature frequently seen in those diagnosed late.3,4
There is a recognised need to reduce the proportion of patients living with undiagnosed infection both for their own health and also from a public health perspective to reduce the onward transmission of infection. Increasing testing in all hospital settings, in particular in patients with indicator diseases, has the potential to impact greatly on the proportion of late presenters. Acute services such as an A&E or medical admissions unit are often the first contact that patients will have had with secondary healthcare services.
However, there are a number of reasons why universal opt-out testing in an AMU setting may not be a realistic objective. Firstly, the patient population attending an AMU is generally an elderly one with 57% of admissions in the studied unit aged over 65 and therefore in a low risk group for HIV infection. Secondly, although a relatively small proportion of admissions were tested in this study, there were no ‘unexpected’ diagnoses as both new diagnoses were late presenters with PJP, the most common AIDS-defining condition in the UK. Thirdly, many AMUs, including the Newcastle AMU, are already under a great deal of pressure with increasing admission rates and reduced staffing levels and therefore the introduction of opt-out universal testing in an AMU or A&E setting would require additional resources and dedicated staff to offer the tests. Other testing studies have utilised additional staff to successfully increase testing rates with up to 74% of admissions approached for testing.8,10 This study was reliant on the staff already available in the unit and included trained associate practitioners to offer testing at the point of initial phlebotomy. This was successful with almost 80% of tests in the second study period being performed by the practitioners. These are band 4 healthcare workers who have no previous formal nursing training highlighting that, as stipulated in the HIV testing guidelines, all levels of healthcare worker should be able to offer HIV testing after appropriate training.
The above reasons, combined with the current workload and financial pressures make universal opt-out testing in AMUs difficult to implement in areas of low prevalence, but it is important that cost:benefit studies are undertaken. Until such data are available, the main emphasis should be on educating healthcare workers about HIV and how to perform a test and also which indicator diseases, such as those listed in the guidelines, should prompt an HIV test. This may result in an increase in testing in a more focused manner and reduce the rate of undiagnosed HIV infection and late presenters.
Acknowledgements
We would like to thank the patients and staff on the medical admissions unit, Dr Sheila Waugh, consultant virologist, and Jayne Harwood, biomedical scientist, for assistance in this audit project. We would also like to thank Gilead Sciences for providing funding for the project.
Conflict of interests
Dr ELC Ong co-chaired the UK national HIV testing guidelines 2008.
Funding
An unrestricted grant was provided by Gilead Sciences as part of their fellowship programme.
References
- 1.Health Protection Agency. HIV in the United Kingdom 2010 report 2010London: HPA; 4–47 [Google Scholar]
- 2.Moreno S, Mocroft A, Monforte A. Medical and societal consequences of late presentation. Antiviral Therapy 2010; 15Suppl 19–15 10.3851/IMP1523 [DOI] [PubMed] [Google Scholar]
- 3.Burns FM, Johnson AM, Nazroo J, et al. SONHIA Collaboration Group. Missed opportunities for earlier HIV diagnosis within primary and secondary healthcare settings in the UK. AIDS 2008; 1: 115–22 [DOI] [PubMed] [Google Scholar]
- 4.Premchand N, Golds K, Tan PY, Sankar N, Ong E. The burden of late presentation: characteristics of patients newly diagnosed with HIV in the North East of England in 2007 and 2008. HIV Med 2009; 10(Suppl 2): PE18.11/1 [Google Scholar]
- 5.Palfreeman A, Fisher M, Ong E. Testing for HIV: concise guidance. Clin Med 2009; 9: 471–6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Department of Health. Guidelines for offering voluntary HIV antibody testing to women receiving ante-natal care 1994London: DH [Google Scholar]
- 7.Perry N, Heald L, Cassell J, et al. HIV testing in acute general medical admissions must be universally offered to reduce undiagnosed HIV. HIV Med 2010; 11Suppl 1O19 [Google Scholar]
- 8.Rayment M, Thornton A, Gidwani S, et al. HIV testing in the emergency department–reporting one arm of the HIV testing in non-traditional settings (HINTS) study. HIV Med 2010; 11Suppl 1O20 [Google Scholar]
- 9.Deblonde J, De Koker P, Hamers FF, et al. Barriers to HIV testing in Europe: a systematic review. Eur J Public Health 2010; 4: 422–32 10.1093/eurpub/ckp231 [DOI] [PubMed] [Google Scholar]
- 10.Cridford R, Thornton A, Rayment M, et al. HIV testing in non-traditional settings: feasibility and acceptability in an acute admissions unit. J Int AIDS Soc 2010; 13Suppl 4P219. 10.1186/1758-2652-13-S4-P219 [DOI] [Google Scholar]