

Abstract
Awareness is growing that young adults may have distinctive experiences of adult healthcare and that their needs may differ from those of other adult users. In addition, the role of adult health teams in supporting positive transitions from paediatrics is increasingly under discussion. This paper contributes to these debates. It reports a qualitative study of the experiences of young adults – all with complex chronic health conditions — as users of adult health services. Key findings from the study are reported, including an exploration of factors that help to explain interviewees’ experiences. Study findings are discussed in the context of existing evidence from young adults in adult healthcare settings and theories of ‘young adulthood’. Implications for training and practice are considered, and priorities for future research are identified.
KEYWORDS : Adult health services, complex health conditions, emerging adulthood, transition, young adults
Introduction
Support for the notion of a distinct developmental stage bridging adolescence and adulthood is growing. Jeffrey Arnett, one of the first academics to explore and develop this idea, coined the term ‘emerging adulthood’ to describe this stage of life.1–3
In making his case, Arnett pointed to a wide range of evidence. The ages at which individuals in many societies in the developed world achieve the so-called milestones of adulthood (eg employment and leaving the family home) are significantly later than was the case in the past. Increased access to extended education and economic factors have played their role, as have societal expectations for this stage of life. Evidence also shows substantive differences between adolescent and young adult brains4,5 and that neuroprocessing associated with higher-level cognitive functions, such as regulation of emotions and rational decision making, is still developing through the twenties.6 Finally, many young adults (aged 18–25 years) do not perceive themselves as ‘adults’.7 Importantly, their perceptions of adulthood are centred in notions of self-sufficiency (self-responsibility and independent decision making) rather than the traditional adulthood milestones, such as leaving the family home or entering employment.
The notion that individuals in their late teens and twenties are relatively immature compared to older adults provides a useful lens when considering the experiences of this age group in adult healthcare. How adult health services can, or should, respond to the specific needs of young adults has begun to be discussed, driven both by evidence of poor health outcomes among young adults compared with adolescents8,9 and, for those with long-term conditions diagnosed in childhood, by evidence regarding the risks to health outcomes associated with the transfer from paediatric to adult healthcare.10 With respect to this latter population, this discussion is a welcome development. Explanations for ‘poor transitions’ have typically related to inadequacies in transition planning and preparation in paediatrics. Until recently, little consideration has been given to whether the settings into which these patients transfer are appropriate or take adequate account of their developmental stage.10,11 This is evident in the (relative) lack of attention in guidance on transition (both national policy and specific to conditions) in terms of what adult healthcare teams/settings should do to ensure a successful transfer from paediatrics.
Analysis of surveys from NHS patients suggests that young adults’ experiences of healthcare are worse than those of adolescents and older adults.12,13 This is not an issue restricted to the UK. The call for research that develops our understanding of young adults’ experiences of adult healthcare has been made widely, 12–14 as has the need to extend this work beyond more traditional areas of ‘transition research’, such as diabetes.15 This paper contributes to this evidence by providing an overview of key findings from a recently completed study of the healthcare experiences of young adults with a range of complex health conditions.
Methods
The findings reported are drawn from a larger study looking at health transitions for young people and young adults diagnosed with complex health conditions during childhood. Details of research sites recruiting young adults to the study are given in Table 1.
Table 1.
Recruitment centres and sample of young adults.
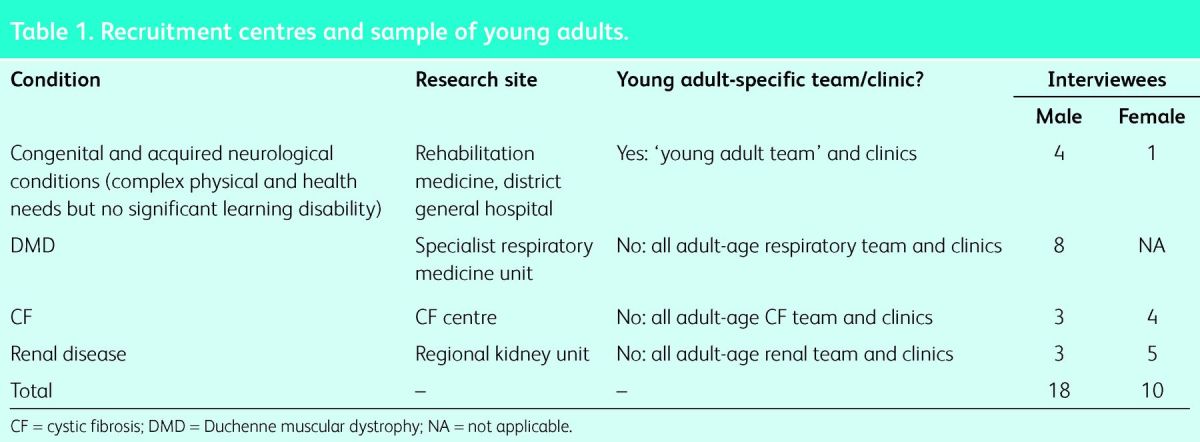
We recruited 28 young adults aged 18–25 years. Congenital and childhood-diagnosed chronic conditions were represented, all of which can be conceived as life limiting or life threatening. Participants took part in an extended, semi-structured, face-to-face (n = 17) or telephone (n = 11) interview. Recruitment rates are not available as clinics did not record the number of recruitment packs mailed out. Full details of the methods, including an account of the analytical approach, are reported elsewhere.16 The study was approved by an NHS research ethics committee.
Findings
Transfer from paediatrics
Some young adults believed that readiness to transfer to adult healthcare was grounded in their own sense of maturity and self-confidence. Work done in paediatrics, such as encouraging active involvement in consultations and ‘teenage/transition clinics’, supported this readiness. Interestingly, no patients identified self-management of their condition as an indicator of readiness. However, others challenged the notion of transition readiness. They had found that they needed to make the move to adult healthcare before they were willing, or understood the need, to assume greater responsibility for their condition and become actively involved in clinic consultations.
For a minority of patients, the transfer to adult healthcare was perceived as a minor event superseded by more significant transitions, such as moving into further/higher education and starting work. However, many recalled feeling anxious about the move.
Opinions were consistent around what had been useful during the period of transition:
visit(s) to the adult service
opportunity to meet staff, including, ideally, a named individual who would be present during the early appointments at the adult clinic
provision of information (written and verbal), particularly that which alerted them to any differences in practices/procedures and that was repeated on a number of occasions
choice over whether or not parents attended appointments
all (adult) clinic staff being aware of newly transferred patients.
Our interviews took place at least a year after patients had transferred from paediatrics. All of the young adults expressed satisfaction with their specialist adult team and none rued having to move from paediatrics. Settling in was facilitated by establishing trusted relationships with staff and observing evidence of the competence of the new team.
Parental involvement
All of our interviewees reported that their parents were – to a greater or lesser degree – actively involved in supporting them to live with and manage their condition. They believed that practice in their specialist clinics accommodated patterns of parental involvement in individual families. For example, young adults were allowed to choose whether parents attended consultations, and visiting times in specialist inpatient facilities were extended. However, our interviewees also described situations where, as inpatients, their parents had been excluded from consultations and ward rounds against their wishes. Young adults ascribed this to staff assuming that this was ‘the right thing’ to do.
A typology of parents’ presence at adult clinic appointments emerged: never attended, withdrew after settling-in period and continued to attend. All of the young adults wanted to have the final say on whether or not their parents were present during consultations. Crucially, they wanted to be able to ‘recall’ parents to appointments if they were struggling to communicate or they faced specific decisions. Some young adults were aware that their parents continued to attend in order to meet their own information and support needs; however, they were content with this. Parental presence (or not) at clinic did not seem to be associated with the young adults’ wider independence. Some of our interviewees were highly independent individuals in employment and living away from the family home yet wanted a parent to attend appointments with them.
Reasons for parents’ ongoing attendance were that the young adult did not feel that they could manage all aspects of a clinic appointment and they needed emotional support. The roles that parents assumed in appointments were the same as any ‘patient companion’:17 acting as spokesperson (or backup), ‘taking on’ information (sometimes simplifying or individualising it for the young adult) and acting as a source of emotional support. With respect to this latter point, it was clear that even routine clinic appointments could be a time of heightened anxiety for young adults with progressive conditions owing to the possibility of evidence of deterioration (eg lung function or spine curvature) being revealed through routine monitoring, and appointments also reminded them of the life-limiting nature of their condition.
It is important here to draw a distinction between ‘presence’ and ‘involvement’. All of the young adults reported that their parents knew about their appointments. Furthermore, regardless of whether they were present at consultations, parents were often involved prior to appointments (eg identifying issues to raise) and afterwards (eg ‘debriefing’). Parents sometimes proactively initiated this ‘remote’ involvement, particularly when they had concerns about their son's or daughter's health or its management.
Inpatient experiences
Inpatient stays, including unplanned admissions related to acute respiratory tract infection, were a common experience among those interviewed. These were consistently identified as the most negative aspect of the transfer from paediatric to adult healthcare. Experiences on general medical or respiratory wards were particularly problematic. A range of problems or difficulties were reported:
distress and anxiety caused by the health and/or confused state of other patients
parents excluded from consultations and decision making
unmet care needs
social isolation and lack of occupation
staff not recognising the significance of the admission in terms of indicating degeneration or worsening health.
Some interviewees recalled tours of their specialist unit's inpatient facilities, although this was perceived as limited to the physical environment rather than highlighting differences in practices and procedures between paediatric and adult settings. None recalled receiving any information about staying on general adult wards – from either their paediatric or adult team. All believed that this information would have been extremely useful.
Young adults: key issues for adult health services
We also interrogated our data for explanations for the experiences described above. The following factors may play a role in the difficulties young adults can encounter when moving into adult healthcare:
young adults being, typically, a minority group in adult healthcare
young adults perceiving themselves as health service ‘experts’
staff having assumptions or beliefs about parental involvement in young adults’ lives.
Minority group
Adult healthcare practices, skills and environments are, inevitably, organised and resourced for the majority or ‘typical’ population. Chronological age and/or diagnosis mean that young adults can be the minority group for the adult health team to which they transfer and any other settings that they use.18 This minority group status offered an explanation for some of the poor experiences described to us, particularly their experiences of health services outside the specialist clinic/department.
A lack of awareness, or recognition, by staff of the potential differences in maturity and self-sufficiency between young adults and other adult patient groups seemed to underlie some of our interviewees’ experiences. Certainly it seemed that there could be unwillingness to adjust ‘usual practice’ to accommodate the needs of this group. Alternatively, it suggests that this population is not considered or planned for. A clear example of this was practice on general wards in terms of extended visiting for parents, with reports of seemingly ad hoc policies, sometimes even differing between shifts.
Advances in the management of some conditions diagnosed in childhood have resulted in significant improvements in life expectancy. Children are now surviving into adulthood and, therefore, transferring into adult healthcare.19 However, staff in general medical wards are unlikely to have encountered these conditions, particularly if they are unusual. For some young adults, therefore, their condition and age will render them a minority in certain settings. For example, admission to adult medical/respiratory wards was something all of the young men with Duchenne muscular dystrophy had experienced owing to their increased vulnerability to respiratory tract infections. A lack of understanding of this condition among staff resulted in some very difficult experiences for these young men, many of whom had significant physical impairments. These included staff failing to assess and address the need for support with self-care (eg toileting and eating) and a lack of acknowledgement of the significance of the admission (in terms of indicating degeneration).
Health service ‘experts’
Almost all of our interviewees had years of experience of paediatric clinics and children's wards. In a sense, they, and their families, regarded themselves as health service ‘experts’. Importantly, most had not appreciated that paediatric and adult services might do things differently. Even seemingly innocuous differences (eg weighing without removing shoes) were described as unsettling and a source of anxiety. The advantage of ‘knowing the system’ in paediatrics actually became a disadvantage on moving to adult services. Interviewees described feeling anxious and disempowered when they encountered procedures and practices in clinics or on the ward that were different from those in children's services. This sense of disempowerment left them less well placed to voice their concerns and/or adapt to the new setting.
Staff attitudes or beliefs about parental involvement in young adults’ lives
A dissonance between young adults’ wishes regarding their parents’ involvement and staff attitudes or assumptions seemed to be the key, or a contributory, factor underlying some of the most difficult experiences reported by the young adults. This was most likely to be experienced in non-specialist settings (general medical/respiratory wards and accident and emergency departments in district hospitals). Here, young adults reported that staff were less likely to ascertain their wishes with respect to parental involvement or did not accede to the young adult's request that their parents were involved. Examples of situations encountered by our interviewees included refusal of request for parents to attend ward rounds and requests for young adults to make very significant decisions about the management of their condition without their parents being present.
Discussion
Our findings add to the limited body of evidence from young adults themselves about their experiences as users of adult healthcare services. The study reported here has its own limitations (for example, biases associated with a self-selecting sample), which need to be borne in mind; however, we believe it makes a useful contribution.
Some findings replicate the conclusions of earlier research: for example, the importance of providing young people preparing to transfer to adult services with information about the differences between paediatric and adult healthcare services.15 Our findings highlight the need to extend such information to all healthcare settings in which young adults may find themselves, including wards and departments in other hospitals. This is a task for paediatric and adult teams – in terms of both finding out what each other does and taking responsibility to inform and remind young adults about differences and the reasons for them. Involving young adults in developing information at a local level would help to ensure materials are meaningful and comprehensive.
Other findings add new or different insights on some issues. Working towards lone consultations with young people is regarded as a key element of preparing for the transfer to adult healthcare.20 However, current practice in the adult setting does not necessarily replicate this.21 What was important to our participants was being in control of parental presence and involvement. That all of the young adults reported that their parents were involved in their clinic appointments, albeit sometimes in a ‘remote role’, was an interesting finding. One explanation could be that the conditions represented in this study were more complex (and indeed, for some, life limiting) than the conditions represented in many previous studies. Prognosis may heighten the significance of even routine outpatient appointments for young adults and, hence, their need for support. It is also helpful to place these findings in the context of wider evidence on the potentially positive impact of ‘patient companions’ on consultations.19 We should not forget that most young adults have not replaced their parents with a ‘significant’ partner, so their choice as to who accompanies them to an appointment is necessarily limited. The apparent mismatch between young adults’ views of their parents as a key source of support and healthcare professionals’ ambivalence about ongoing parental involvement requires further exploration. It would be useful to identify what is ‘good’ parental involvement (in terms of young adults’ outcomes) and how professionals can support parents to achieve that.
The young adults’ perspectives on ‘transition readiness’, particularly the views of some that it took the move to adult healthcare to ‘make them ready’, is interesting. It may reflect individual differences in temperament or personality. Again, it merits further research and certainly highlights the importance of adult settings making adjustments in order to be appropriate and acceptable to young adult patients, who may differ considerably in terms of their maturity.
One solution to some of the difficult experiences reported in this article lies in raising awareness of, and providing training in, ‘young adulthood’ and the particular issues that young adults may face as users of adult healthcare services. This is something that the Royal College of Physicians of London is addressing (www.rcplondon.ac.uk/projects/young-adult-and-adolescent-initiative), and it is equally vital that other professional groups embrace this issue, so that practitioners across all adult healthcare services are more aware and have a better understanding of this particular patient group. At the same time, it is important to note that the evidence base to inform training and practice is still limited. The need for caution in generalising findings from research on particular conditions or settings therefore needs to be stressed.
Acknowledgements
The authors would like to acknowledge the contribution of other members of the project team: Suzanne Mukherjee, Mairi Harper, Judith Dorrell, Jane Maddison and Gemma Spiers. The research reported is drawn from a larger project on health transitions commissioned by Together for Short Lives, Help the Hospices and the National Council for Palliative Care, which was funded by the Big Lottery Fund (BLF) Research Programme. The BLF also funded the production of two resources for practitioners based on the study findings. These are freely available in electronic and print formats (www.togetherforshortlives.org.uk/professionals/resources/3683_making_a_difference_for_young_adult_patients_resources_-_free).
References
- 1.Arnett J. Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol 2000;55:469–80. 10.1037/0003-066X.55.5.469 [DOI] [PubMed] [Google Scholar]
- 2.Arnett J. Emerging adulthood: the winding road from the late teens through the twenties. New York: Oxford University Press, 2004. [Google Scholar]
- 3.Arnett J, Galambos N. Culture and conceptions of adulthood. New Dir Child Adolesc Dev 2003;100:81–98. [DOI] [PubMed] [Google Scholar]
- 4.Sowell E, Thompson P, Toga A. Mapping changes in the human cortex throughout the span of life. Neuroscientist 2004;10:372–92. 10.1177/1073858404263960 [DOI] [PubMed] [Google Scholar]
- 5.Bennett C, Baird A. Anatomical changes in the emerging adult brain: a voxel-based morphometry study. Hum Brain Mapp 2006;27:766–77. 10.1002/hbm.20218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Johnson A, Blum R, Giedd J. Adolescent maturity and the brain: the promise and pitfalls of neuroscience research in adolescent health policy. J Adolesc Health 2009;45:216–21. 10.1016/j.jadohealth.2009.05.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Arnett J. Conceptions of the transition to adulthood: -perspectives from adolescence through midlife. J Adult Dev 2001;8:133–43. 10.1023/A:1026450103225 [DOI] [Google Scholar]
- 8.Ozer E, Urquhart J, Brindis C, et al. Young adult preventive health care guidelines. Arch Paed Adolesc Med 2012;166:240–7. 10.1001/archpediatrics.2011.794 [DOI] [PubMed] [Google Scholar]
- 9.Neinstein L, Irwin C. Young adults remain worse off than -adolescents. J Adolesc Health 2013;52:559–61. 10.1016/j.jadohealth.2013.08.014 [DOI] [PubMed] [Google Scholar]
- 10.Gleeson H, McCartney S, Lidstone V. ‘Everybody's business’: -transition and the role of the adult physician. Clin Med 2012;12:561–6. 10.7861/clinmedicine.12-6-561 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McDonagh J, Robinson A. Growing up: the role of the Royal College of Physicians. Clin Med 2012;12:197–9. 10.7861/clinmedicine.12-3-197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hargreaves D, Sizmur S, Viner R. Do young and older adults have different health care priorities? Evidence from a national survey of English patients. J Adolesc Health 2012;51:528–32. 10.1016/j.jadohealth.2012.05.016 [DOI] [PubMed] [Google Scholar]
- 13.Hargreaves D, Viner R. Children's and young people's experience of the national health service in England: a review of national surveys. Arch Dis Child 2012;97:7661–6. [DOI] [PubMed] [Google Scholar]
- 14.Nguyen L, Rahman Z, Emerson R, et al. Cigarette smoking and drinking behavior of migrant adolescents and young adults in Hanoi, Vietnam. J Adolesc Health 2012;50:S61–7. 10.1016/j.jadohealth.2011.12.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Crowley R, Wolfe I, Lock K, McKee M. Improving the transition between paediatric and adult health care: a systematic review. Arch Dis Child 2011;96:548–53. 10.1136/adc.2010.202473 [DOI] [PubMed] [Google Scholar]
- 16.Beresford B, Stuttard L. Supporting health transitions for young people with life-limiting conditions: researching evidence of positive practice. York: Social Policy Research Unit, University of York, 2013. [Google Scholar]
- 17.Street R, Gordon H. Companion participation in cancer consultations. Psychooncology 2008;17:244–51. 10.1002/pon.1225 [DOI] [PubMed] [Google Scholar]
- 18.Todd C, Winitzer R, Keenan P. Transition from pediatric to adult-oriented health care: a challenge for patients with chronic disease. Curr Opin Pediatr 2001;13:310–6. 10.1097/00008480-200108000-00004 [DOI] [PubMed] [Google Scholar]
- 19.Fraser L, Miller M, Aldridge J, et al. Prevalence of life-limiting and life-threatening conditions in young adults in England 2000–2010. Palliat Med 2014;28:513–20. 10.1177/0269216314528743 [DOI] [PubMed] [Google Scholar]
- 20.Gleeson H, Turner G. Transition to adult services. Arch Dis Child Educ Pract Ed 2012;97:86–92. 10.1136/archdischild-2011-300261 [DOI] [PubMed] [Google Scholar]
- 21.Suris J, Akre C, Rutishauser C. How adult specialists deal with the principles of successful transition. J Adolesc Health 2009;45:551–5. 10.1016/j.jadohealth.2009.05.011 [DOI] [PubMed] [Google Scholar]