

Abstract
Intussusception is a very rare cause of intestinal obstruction in neonates. It is of extremely rare occurrence among premature neonates. We present a case of 11-day-old premature neonate who presented with abdominal distension, intolerance to feeds, vomiting, significant bilious aspirate and bleeding per rectum. The initial diagnosis of necrotizing enterocolitis (NEC) led to a delay in the diagnosis. On exploratory laparotomy, it turned out to be a case of ileo-colic intussusception with Meckel's diverticulum as a lead point. This site of intussusception (ileo-colic) and presence of a lead point among premature neonate is of exceedingly rare occurrence and very few such cases have been reported.
In this article, the published work about clinical features and management on intussusceptions in premature neonates has been reviewed. The authors intend to highlight the difficulty in distinguishing the NEC and intussusception. Subtle clinical and radiological features which can help in differentiating the two conditions have been emphasized. This can avoid the delay in diagnosis and management which can prove critical. High index of suspicion with timely intervention is the key for optimizing outcome. A diagnosis of intussusception should always be considered in any preterm infant with suspected NEC.
Keywords: Intussusception, Meckel's diverticulum, necrotizing enterocolitis, neonate, premature, preterm
INTRODUCTION
Less than 1.3% of all cases of intussusceptions occur in term neonates.[1] Intussusception in the premature neonate is an exceedingly rare clinical entity. The rarity of the condition and the lack of specific clinical features often lead to diagnostic confusion with necrotizing enterocolitis (NEC) which is a much more common disorder in this age group. This further leads to delay in the diagnosis and surgical treatment resulting in increased morbidity and mortality. The exact aetiology remains unclear in majority of cases. We present a case of intussusception in an 11-day-old premature neonate who was born at gestational age of 32 weeks. The etiopathogenesis, diagnostic and treatment protocols of this rare clinical entity are discussed herewith along with subtle clues to avoid the diagnostic dilemma.
CASE REPORT
A 1.3 kg male neonate who was delivered at 32 weeks of gestation presented at 11th day of life with vomiting, failure to pass meconium and abdominal distension. The child was admitted to neonatal intensive care unit with the provisional diagnosis of NEC and was treated as per standard protocols for a couple of days. Subsequently there was bilious vomiting with progressive abdominal distention and an episode of bleeding per rectum. Hematological tests showed the leucocytosis, thrombocytopenia and dyselectrolemia which were corrected. Abdominal radiograph showed multiple air and fluid-filled bowel loops [Figure 1]. Ultrasonography (USG) revealed fixed small bowel loops with suspicion of intussusception. Exploratory laparotomy was planned for suspected intestinal obstruction. Child was started on ionotropic support for hypotension pre-operatively. Intra-operatively, ileo-colic intussusception with meckel's diverticulum acting as the lead point with adjoining bowel ischemia was detected [Figure 2]. Intussusception was reduced, and resection of the gangrenous bowel with ileo-ileal anastomosis was performed. The post-operative period was stormy with features of septicaemia, disseminated intravascular coagulation and pneumonitis. Unfortunately, the child succumbed on third post-operative day to septicaemia, persistent hypotension and multiple organ dysfunction syndrome.
Figure 1.
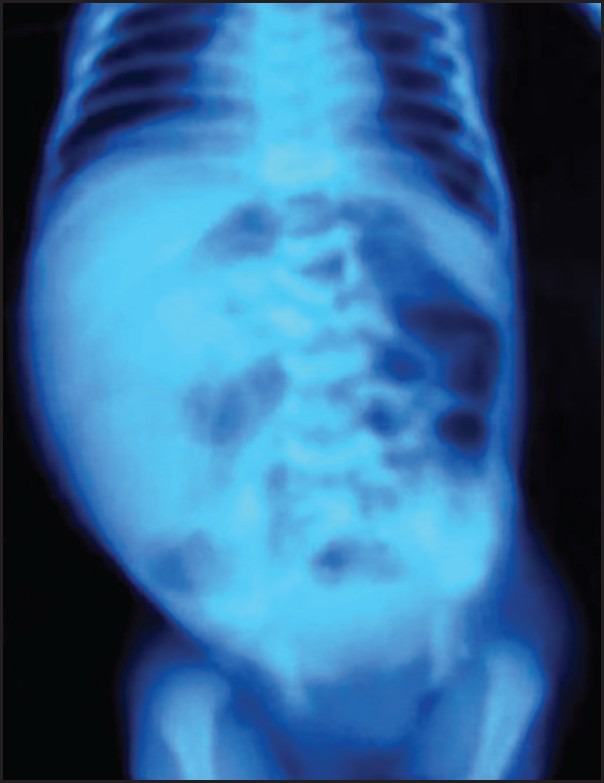
X-ray abdomen showing dilated bowel loops in the centre with paucity of gas in pelvis
Figure 2.

Intraoperative photograph showing ileo-colic intussusception
DISCUSSION
Intussusception is the most common cause of intestinal obstruction at ages between 6 and 18 months but is an extremely rare clinical entity in neonates, especially among premature neonates. It accounts for only 3% of intestinal obstruction in neonates and only 0.3% (0-2.7%) of all cases of intussusceptions.[2] Intussusception occurring in premature infants shows numerous differences from that in the typical age group of patients, or even that in full-term neonate.[2,3,4]
Intussusception in infancy, childhood and full-term neonates occurs most commonly at the level of the ileo-colic junction (80%). The small bowel intussusceptions are found in <10% cases among all age groups. In premature neonates, however, the involvement of small bowel is very common and is mostly observed in ileum and jejunum (91.6%).[2,3,5] In this case, it was ileo-colic intussusceptions which is very uncommon among premature neonates.
The etiology of neonatal intussusceptions in premature infants remains unclear. In full-term infants, it is associated with identifiable lead point.[6] In the majority of premature infants, usually no lead point is found, and the exact etiopathology is still unclear.[7] In these patients, recognizable anatomical leading points, such as diverticulum, polyps, or cysts are not common and may be found in only about 8% of cases.[8] In our case, Meckel's diverticulum was present as the lead point, and this again is quite rare amongst premature neonates.
It is suggested that common perinatal risk factors resulting in intestinal hypo perfusion, hypoxia, dysmotility and stricture formation may act as a lead point for intussusceptions.[6] Moreover, intestinal hypo perfusion or ischemia results in dysmotility and stasis, but accelerated peristalsis occurs in the early or recovering phases of the event, potentially acting as a functional leading point.[1,6,9] Ueki et al., in a recent study of 14 neonates concluded that hypoxic events may play a crucial role in the pathogenesis of late-onset neonatal intussusceptions.[10]
In many of these patients, common perinatal risk factors such as respiratory distress syndrome, patent ductus arteriosus, hypoxia, hypotension and umbilical catheterization are often present and add substantially to morbidity.[3]
Onset of symptoms in premature infants with intussusceptions usually occurs at around 10 days of age, when hypoxic and ischaemic events due to delayed cardiopulmonary adaption are most likely to occur.[11]
Intussusceptions occurring in premature neonates are difficult to assess. Typical clinical features are absent and the symptoms viz. abdominal distension, feeding intolerance, vomiting and bloody stools are almost identical to NEC. A palpable abdominal mass is present less commonly. Owing to its high prevalence in this age group, NEC is the first diagnosis in most cases thus resulting in an average delay on the correct diagnosis of approximately 7 days. This average period gets longer in cases not complicated with perforation.[1,2,5,6,8,10]
Bilious emesis or nasogastric secretions are present in most patients, as is marked abdominal distension without pneumatosis intestinalis. This along with the passage of blood per rectum, without systemic signs of toxicity, makes NEC less likely.[12]
Mooney et al., in their series observed that more than half of the cases were misdiagnosed as NEC, and only 10% cases was diagnosed pre-operatively.[12]
There has been no previous report of any specific radiological features of intussusceptions in preterm infants. The most common imaging finding in patients with intussusceptions in premature neonates is dilated bowel loops. Pneumatosis intestinalis or portal venous gas are neither common nor do they relate appropriately to the clinical course of the disease.[1]
One of the major criteria for diagnosing intussusceptions is absent cecal shadow. In neonates, the sigmoid colon comes to lie superficially on the right side (43%) along with distended small bowel loops overlapping the intussuscepted bowel and obscuring it which results in diagnostic dilemma.[7]
Recent studies concluded that ultrasound scan is capable to establish an early diagnosis of intussusceptions in neonates, but a high index of suspicion is warranted. Indeed, USG is a very reliable imaging tool for rapid and accurate diagnosis. Advantages of USG include the ability to document ileo-ileal intussusception, the absence of ionizing radiation to the neonate and identification of lead points.[1,3,8] USG shows a characteristic multi concentric ring on axial and sandwich-like appearance on longitudinal scans in the lower right quadrant of abdomen confirming intussusception.[11]
Contrast enemas may be both diagnostic and therapeutic for older children. In premature neonates, however, the ileo-ileal location of the intussusceptions and a higher rate of complications like intestinal perforation and metabolic disturbances make contrast enema less useful.[12] The use of enemas should, therefore, be limited to positive and equivocal cases as well as to detect unsuspected disease in selected cases.[8]
Subtle clinical and radiographic differences are important and helpful in differentiating NEC from intussusception. Various clues to exclude the diagnosis of NEC are non-deterioration of the general condition, the presence of negative inflammation indicators especially C-reactive protein and platelet count, the absence of both bloody stools and microscopically conditions that frequently occur in NEC, and finally, the radiograph findings.[8] Indeed, intussusceptions must be highly suspected in a neonate who is diagnosed with NEC but who has a more stable course than would be expected.[2]
It is important to distinguish the condition from NEC as the management changes drastically. The conservative management for NEC will jeopardize the viability of the bowel resulting in high morbidity and mortality if the infant has intussusception.
Premature infants with intussusceptions require surgical correction. Prompt laparotomy following diagnosis is crucial for achieving better outcomes. Primary anastomosis can be performed successfully, and stomas can be created in the critically ill patients or those with late detection and septicaemia. No recurrences have been reported, and anastomotic stricture is the only post-operative intestinal problem reported till date is.[12]
Hydrostatic reduction should not be attempted as the primary management in view of its reported higher morbidity and mortality.
Despite improved outcomes in surgical neonates, the overall prognosis for premature infants with intussusceptions depends on the co-morbidities and once a critical condition develops, as in this case, the mortality rate is likely to rise.[11]
CONCLUSION
Intussusception is a rare clinical entity among premature infants. It is difficult to diagnose and is frequently confused with NEC. The unusual constellation of symptoms may adjourn the diagnosis and increase the mortality and morbidity. Subtle clinical and radiographic difference may help to differentiate it from NEC and avoid the delay in therapy. A high degree of suspicion is of paramount importance. It is, therefore, imperative for neonatologists, paediatricians and paediatric surgeons to be aware of the possibility of intussusception in association with NEC or as an alternative diagnosis, particularly when there is a poor response to medical treatment. Timely diagnosis and prompt and appropriate management can significantly improve the otherwise poor outcome.
Footnotes
Source of Support: Nil.
Conflict of Interest: None Conflict of Interest.
REFERENCES
- 1.Avansino JR, Bjerke S, Hendrickson M, Stelzner M, Sawin R. Clinical features and treatment outcome of intussusception in premature neonates. J Pediatr Surg. 2003;38:1818–21. doi: 10.1016/j.jpedsurg.2003.08.048. [DOI] [PubMed] [Google Scholar]
- 2.Wang NL, Yeh ML, Chang PY, Sheu JC, Chen CC, Lee HC, et al. Prenatal and neonatal intussusception. Pediatr Surg Int. 1998;13:232–6. doi: 10.1007/s003830050305. [DOI] [PubMed] [Google Scholar]
- 3.Martínez Biarge M, García-Alix A, Luisa del Hoyo M, Alarcón A, Sáenz de Pipaón M, Hernández F, et al. Intussusception in a preterm neonate; A very rare, major intestinal problem – systematic review of cases. J Perinat Med. 2004;32:190–4. doi: 10.1515/JPM.2004.036. [DOI] [PubMed] [Google Scholar]
- 4.Nock ML, Wilson-Costello D. Intussusception in a premature neonate. Clin Pediatr (Phila) 2002;41:721–4. doi: 10.1177/000992280204100913. [DOI] [PubMed] [Google Scholar]
- 5.Al-Salem AH, Habash BM. Ileoileal intussusception: A report of four cases. Ann Saudi Med. 2000;20:310–2. doi: 10.5144/0256-4947.2000.310. [DOI] [PubMed] [Google Scholar]
- 6.Slam KD, Teitelbaum DH. Multiple sequential intussusceptions causing bowel obstruction in a preterm neonate. J Pediatr Surg. 2007;42:1279–81. doi: 10.1016/j.jpedsurg.2007.02.028. [DOI] [PubMed] [Google Scholar]
- 7.Shad J, Biswas R. Ileo-colic intussusception in premature neonate. BMJ Case Rep 2011. 2011 doi: 10.1136/bcr.11.2011.5109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Loukas I, Baltogiannis N, Plataras C, Skiathitou AV, Siahanidou S, Geroulanos G. Intussusception in a premature neonate: A rare often misdiagnosed cause of intestinal obstruction. Case Rep Med 2009. 2009:607989. doi: 10.1155/2009/607989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hirokawa S, Uotani H, Yoshida T, Tsukada K. Ileoileal intussusception and ileal stricture associated with necrotizing enterocolitis in a premature infant: Report of a case. Surg Today. 2001;31:1097–9. doi: 10.1007/s595-001-8066-6. [DOI] [PubMed] [Google Scholar]
- 10.Ueki I, Nakashima E, Kumagai M, Tananari Y, Kimura A, Fukuda S, et al. Intussusception in neonates: Analysis of 14 Japanese patients. J Paediatr Child Health. 2004;40:388–91. doi: 10.1111/j.1440-1754.2004.00408.x. [DOI] [PubMed] [Google Scholar]
- 11.Shima Y, Kumasaka S, Yashiro K, Nakajima M, Migita M. Intussusception in an extremely premature infant following bacterial sepsis. Eur J Pediatr. 2012;171:725–7. doi: 10.1007/s00431-011-1635-y. [DOI] [PubMed] [Google Scholar]
- 12.Mooney DP, Steinthorsson G, Shorter NA. Perinatal intussusception in premature infants. J Pediatr Surg. 1996;31:695–7. doi: 10.1016/s0022-3468(96)90676-4. [DOI] [PubMed] [Google Scholar]