

Introduction
Atrial fibrillation (AF) is a frequently encountered tachyarrhythmia that can substantially impair quality of life through symptom production, adverse consequences (such as stroke, systemic embolization, heart failure, hospitalization, death), economic impact, and more.[1,2] In many patients AF is progressive and reaches a pattern (frequency, duration, and/or severity of symptoms) for which the patient seeks therapy. Such therapy often includes an antiarrhythmic strategy.[3]
When antiarrhythmic drug therapy is chosen, the agent may be selected from among those drugs approved by regulatory agencies (such as the federal Food and Drug Administration [FDA] in the U.S.) that have an indication for use in AF (such as, alphabetically: dofetilide, dronedarone, flecainide, propafenone, quinidine, sotalol), or the agent may be selected “off-label” from other available drugs for which the medical literature offers support for AF management -- amiodarone being, perhaps, the major representative of this latter approach.
Recently, the drug ranolazine, an agent approved in the U.S. for the management of angina pectoris, has attracted attention as a potential antiarrhythmic agent for AF (off-label) as ranolazine has been demonstrated to have antiarrhythmic actions, including effects on the “late sodium current” and potassium flux, among others.[4-13] Recent reports have been published indicating that ranolazine has been effective as “pill-in-the-pocket” therapy for pharmacologic conversion of recent onset AF,[13] for AF occurring acutely after cardiac surgery, and in selected other circumstances of limited duration. The following case, in which the patient compulsively tracked his episodes of AF in a detailed log, clearly demonstrates the potential of ranolazine for the chronic management of progressive, drug-resistant, paroxysmal AF.
Case Report
The patient was a 45 year old male at our first encounter in 1993, at which time he gave a history of 5 episodes of documented symptomatic paroxysmal AF (PAF) between 1990 and 1993. Rate control was attained with digoxin, which reduced the severity of his symptoms but did not abolish their occurrence. [Figure 1] demonstrates the course of his AF from 1990 to the present time. A thorough investigation into the possible etiology of his PAF was unrevealing aside from a familial link on the male side of his family and a personal and familial tendency towards sinus bradycardia [his father had AF and a permanent pacemaker]. All hematological studies (including thyroid function) were normal, as was chest X ray, ECG (aside from his PAF), echocardiography, and stress testing with nuclear and echocardiographic images on different occasions. When PAF occurred, it was associated with irregular palpitations, mild dyspnea, vague weakness, and mild chest discomfort (prior to rate control with digoxin but not after it). Episode duration varied from 1 hr to 24 hrs as judged from his episode log, which he kept in detail. Commonly their onset was nocturnal.
Figure 1. A time plot of the frequency of paroxysmal AF events and simultaneous drug therapy. The top, middle, and bottom time bars are continuous.
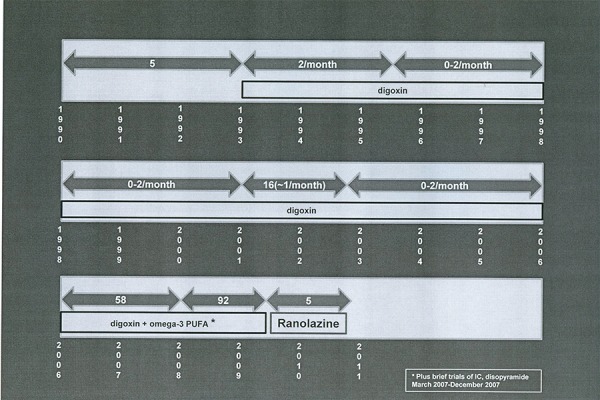
In 2006, because of an increase in the frequency and average duration of his episodes, a trial of omega-3 fish oil was begun, without effect, and, in addition, he was given flecainide, 300 mg single dose, to use as “pill-in-the-pocket” therapy to atReporttain pharmacologic abbreviation of the episodes, which worked well. Nonetheless, his episodes increased in frequency [see [Figure 1]], such that he then underwent trials of twice daily administration of flecainide, then propafenone, then disopyramide. Each of these had minimal effect on his episode frequency; each was associated with bothersome side effects; and each, in turn was discontinued. He declined to be hospitalized for a trial of dofetilide, and declined trials of sotalol or amiodarone out of concern that they would provoke the need for pacemaker insertion. Between 2006 and mid 2009, the patient documented in his log 156 episodes -- despite the periods of antiarrhythmic drug use as noted above. In mid 2009, a trial of ranolazine was begun, in addition to his digoxin. Initially he was given 1000 mg twice daily, but this was soon reduced to 500 mg twice daily because of constipation. Since being on ranolazine, he has noted only 5 episodes, all brief, with none at all over the past 5 months.
Discussion
PAF is a very common dysrhythmia that: is often associated with significant impairment on quality of life; usually requires therapy; can remain stable in its pattern, can progress in frequency, and/or can presage the development of persistent episodes requiring cardioversion and/or the development of permanent AF.[1,2]
Antiarrhythmic drug therapy may be effective in managing PAF, as defined by a reduction in frequency, duration, and severity of episodes to the point of being acceptable to the patient (but rarely, if ever, to the point of permanent elimination).[2,3] Antiarrhythmic therapy may also reduce hospitalization for AF, heart failure from AF, and, perhaps in some circumstances, mortality associated with AF.[14] Antiarrhythmic therapy, however, may also be associated with fatal or debilitating adverse consequences, including (for drugs) organ toxicity, ventricular proarrhythmia, bradyarrhythmias and conduction disturbances, hemodynamic deterioration/heart failure, and death, and (for non-pharmacologic therapy) procedural complications, including death, perforation, embolization, and others.[1,2] Accordingly, there is a pressing need for additional effective and safer therapies.
Some new therapies will come through well designed industry development programs. Others may come from careful clinical observations of “off-label” experience. That is the purpose of reporting the case herein. Ranolazine is an already marketed antianginal compound which in its development program has been found to be free from organ toxicity; ventricular proarrhythmia; the provocation of bradyarrhythmias, conduction defects, or hypo/hypertension; or hemodynamic impairment. It has also been found to possess electrophysiological actions that may provide antiarrhythmic benefit for AF (among other arrhythmias) as well as protection against the generation of torsades de pointes that can accompany the use of several of our currently available antiarrhythmic drugs.[4-13]
In the current case, with episodes more closely tracked than in any previously published, ranolazine provided now long-term beneficial management of AF in a patient with a progressive pattern that failed to improve with class IC and IA antiarrhythmics, and has done so without the provocation of any worsening of his sinus bradycardia or the production of any other serious adverse effect.
This case adds strength to the growing body of literature indicating the potential role of ranolazine for the management of AF. Importantly, regardless of whether any subsequent investigations demonstrate a high degree of efficacy or only a modest one for ranolazine, cases such as this do reveal the importance of individual observations (“the power of one”) in conjunction with clinical trials in advancing our knowledge base concerning therapeutic options and advancement.
Disclosures
None.
References
- 1.Pratt CM, Epstein AE, Kowey PR, Naccarelli GV, Pritchett ELC, Reiffel JA. Cardiol Review. 2004. Management of atrial fibrillation: From clinical trials to clinical practice. pp. 1–8. [Google Scholar]
- 2.Fuster Valentin, Rydén Lars E, Cannom David S, Crijns Harry J, Curtis Anne B, Ellenbogen Kenneth A, Halperin Jonathan L, Le Heuzey Jean-Yves, Kay G Neal, Lowe James E, Olsson S Bertil, Prystowsky Eric N, Tamargo Juan Luis, Wann Samuel. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation-executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients with Atrial Fibrillation). Eur. Heart J. 2006 Aug;27 (16):1979–2030. doi: 10.1093/eurheartj/ehl176. [DOI] [PubMed] [Google Scholar]
- 3.Reiffel JA. Rate versus rhythm control pharmacotherapy for atrial fibrillation: where are we in 2008? JAFIB. 2008;1:31–47. doi: 10.4022/jafib.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Belardinelli L, Shryock JC, Fraser H. The mechanism of ranolazine action to reduce ischemia-induced diastolic dysfunction. Eur Heart J. 2006 [Google Scholar]
- 5.Song Yejia, Shryock John C, Wu Lin, Belardinelli Luiz. Antagonism by ranolazine of the pro-arrhythmic effects of increasing late INa in guinea pig ventricular myocytes. J. Cardiovasc. Pharmacol. 2004 Aug;44 (2):192–9. doi: 10.1097/00005344-200408000-00008. [DOI] [PubMed] [Google Scholar]
- 6.Burashnikov Alexander, Di Diego José M, Zygmunt Andrew C, Belardinelli Luiz, Antzelevitch Charles. Atrium-selective sodium channel block as a strategy for suppression of atrial fibrillation: differences in sodium channel inactivation between atria and ventricles and the role of ranolazine. Circulation. 2007 Sep 25;116 (13):1449–57. doi: 10.1161/CIRCULATIONAHA.107.704890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Antzelevitch Charles, Belardinelli Luiz, Zygmunt Andrew C, Burashnikov Alexander, Di Diego José M, Fish Jeffrey M, Cordeiro Jonathan M, Thomas George. Electrophysiological effects of ranolazine, a novel antianginal agent with antiarrhythmic properties. Circulation. 2004 Aug 24;110 (8):904–10. doi: 10.1161/01.CIR.0000139333.83620.5D. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Undrovinas Albertas I, Belardinelli Luiz, Undrovinas Nidas A, Sabbah Hani N. Ranolazine improves abnormal repolarization and contraction in left ventricular myocytes of dogs with heart failure by inhibiting late sodium current. J. Cardiovasc. Electrophysiol. 2006 May;17 Suppl 1:S169–S177. doi: 10.1111/j.1540-8167.2006.00401.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Morrow David A, Scirica Benjamin M, Karwatowska-Prokopczuk Ewa, Murphy Sabina A, Budaj Andrzej, Varshavsky Sergei, Wolff Andrew A, Skene Allan, McCabe Carolyn H, Braunwald Eugene. Effects of ranolazine on recurrent cardiovascular events in patients with non-ST-elevation acute coronary syndromes: the MERLIN-TIMI 36 randomized trial. JAMA. 2007 Apr 25;297 (16):1775–83. doi: 10.1001/jama.297.16.1775. [DOI] [PubMed] [Google Scholar]
- 10.Scirica Benjamin M, Morrow David A, Hod Hanoch, Murphy Sabina A, Belardinelli Luiz, Hedgepeth Chester M, Molhoek Peter, Verheugt Freek W A, Gersh Bernard J, McCabe Carolyn H, Braunwald Eugene. Effect of ranolazine, an antianginal agent with novel electrophysiological properties, on the incidence of arrhythmias in patients with non ST-segment elevation acute coronary syndrome: results from the Metabolic Efficiency With Ranolazine for Less Ischemia in Non ST-Elevation Acute Coronary Syndrome Thrombolysis in Myocardial Infarction 36 (MERLIN-TIMI 36) randomized controlled trial. Circulation. 2007 Oct 09;116 (15):1647–52. doi: 10.1161/CIRCULATIONAHA.107.724880. [DOI] [PubMed] [Google Scholar]
- 11.Murdock David K, Overton Naomi, Kersten Mary, Kaliebe Jeff, Devecchi Fausto. The effect of ranolazine on maintaining sinus rhythm in patients with resistant atrial fibrillation. Indian Pacing Electrophysiol J. 2008 Aug 01;8 (3):175–81. [PMC free article] [PubMed] [Google Scholar]
- 12.Murdock David K, Kersten Mary, Kaliebe Jeff, Larrain German. The use of oral ranolazine to convert new or paroxysmal atrial fibrillation: a review of experience with implications for possible "pill in the pocket" approach to atrial fibrillation. Indian Pacing Electrophysiol J. 2009 Sep 01;9 (5):260–7. [PMC free article] [PubMed] [Google Scholar]
- 13.Murdock, MD David K., Reiffel , MD James A, Kaliebe, MT, CCRC Jeff, Larrain, MD Germa. The conversion of paroxysmal or initial onset persistent atrial fibrillation with oral ranolazine: Implications for a new “pill in the pocket” approach in structural heart disease. JAFIB. 2010;2:705–710. [Google Scholar]
- 14.Hohnloser Stefan H, Crijns Harry J G M, van Eickels Martin, Gaudin Christophe, Page Richard L, Torp-Pedersen Christian, Connolly Stuart J. Effect of dronedarone on cardiovascular events in atrial fibrillation. N. Engl. J. Med. 2009 Feb 12;360 (7):668–78. doi: 10.1056/NEJMoa0803778. [DOI] [PubMed] [Google Scholar]