

Abstract
The impact of ranolazine, an anti-ishemic agent with antiarrhythmic properties, on paroxysmal atrial fibrillation (PAF) in patients with coronary artery disease (CAD) remains unclear. Pacing devices can be useful tools for disclosing even asymptomatic PAF. Purpose of this study is to assess the effect of ranolazine on atrial fibrillation (AF), in patients with CAD, PAF and a dual-chamber pacemaker.
We studied 74 patients with CAD, PAF, and sick sinus syndrome or atrio-ventricular block, treated with pacemakers capable to detect PAF episodes. The total time in AF, AF burden, and the number of PAF episodes within the last 6 months before enrolment in the study, mean AF duration per episode, and the QTc interval were initially assessed. Subsequently, patients were randomized into additional treatment with ranolazine (375 mg twice daily) or placebo. Following six months of treatment, all parameters were reassessed and compared to those before treatment.
Ranolazine was associated with shorter total AF duration (81.56±45.24 hours versus 68.71±34.84 hours, p=0.002), decreased AF burden (1.89±1.05% versus 1.59±0.81%, p=0.002), and shortened mean AF duration (1.15±0.41 hours versus 0.92±0.35 hours, p=0.01). In the placebo group no such differences were observed. In both groups, no significant differences in the number of PAF episodes and QTc duration were observed.
We conclude that in patients with CAD and PAF, ranolazine reduces the total time in AF, AF burden, and mean AF duration. These findings may imply additional antiarrhythmic properties of ranolazine on atrial myocardium and might indicate the necessity of its use in ischemic patients with PAF.
Introduction
Ranolazine is an antianginal and anti-ischemic drug with antiarrhythmic properties, as shown in experimental and clinical studies.[1-8] In atrial myocytes, ranolazine exerts its antiarrhythmic effect mainly by inhibiting IKr, early INa, and late INa currents in a selective, use-dependent way.[9,10] There are reports suggesting that ranolazine prevents the induction of atrial fibrillation (AF) and terminates the episodes of the arrhythmia.[6, 11-13] However, in clinical practice, a considerable proportion of AF episodes are asymptomatic and this poses difficulties in the detection of the arrhythmic events and the evaluation of antiarrhythmic medications.[14,15]
The efficacy of ranolazine in patients with ischemic heart disease and paroxysmal AF (PAF) has not been completely studied. Since implantable pacemakers can store significant information about high atrial rate episodes and rhythm control in patients with AF, they can be useful tools in evaluating the antiarrhythmic potency of ranolazine on both symptomatic and asymptomatic episodes of AF.[16-21] Therefore, in a prospective, placebo-controlled, randomized study, we used diagnostic data derived from the interrogation of pacing devices in order to assess the antiarrhythmic effect of ranolazine in patients with coronary artery disease (CAD) and PAF, who had been treated with a permanent dual-chamber pacemaker, due to sick sinus syndrome (SSS) or atrio-ventricular conduction block (AVB).
Material and Methods
Patients
Among patients routinely followed in the Pacemaker Clinic within an 18-month period, 460 individuals were initially assessed, and patients eligible for enrollment in the study were those with known CAD and myocardial ischemia, who had been implanted a dual-chamber pacemaker due to SSS or AVB. The pacemakers should be implanted at least six months before recruitment in the study and should be able to store and recall atrial high-rate episodes.
The diagnosis of CAD was based on patients’ history, documented in the past by typical symptoms, electrocardiographic recordings, markers of myocardial necrosis, coronary angiography and interventions for cardiac revascularization, when indicated. Exercise stress test or myocardial scintigraphy revealed myocardial ischemia. SSS and atrio-ventricular conduction abnormalities were diagnosed by symptoms (syncope, presyncope or inappropriate fatigue) combined with 12-lead electrocardiogram, 24-hour Holter recordings and electrophysiologic study, if necessary. PAF was defined according to the Task Force for management of Atrial Fibrillation of the European Society of Cardiology, and documented by Holter recordings and the interrogation of the pacing devices.[22]
Exclusion criteria were recent myocardial infarction, unstable angina, candidacy for revascularization, congestive heart failure, renal failure (creatinine clearance < 30 ml/min), hepatic impairment, and age above eighty-five years. Additionally, patients under antiarrhythmic medication were not included in the study, in order to avoid drug interactions that would make the evaluation of the effect of ranolazine difficult.
Patients received the optimal hemodynamically tolerated treatment, and were randomly assigned to adjunctive treatment with ranolazine or placebo (control group), in an 1:1 order. Each patient was given a unique 3-digit numeric code upon enrollment, and the “Random Allocation Software” for parallel group randomized trial was used to produce a simple 1:1 randomization of the predefined candidacy code numbers.
The following pacemaker models had been implanted in the studied population: 1) Adapta DR, Medtronic, Minneapolis, USA, 2) Symphony DR, Sorin, Milan, Italy, 3) Insignia Ultra DR, Boston Scientific, Phoenix, Arizona, USA, 4) T60 DR and C70 DR, Vitatron, Maastricht, Netherlands, and 5) Victory XL DR and Identity XL DR, St. Jude Medical, St. Paul, Minneapolis, USA. The devices had automatic mode switch features and could provide information concerning the number of AF episodes (mode switches), the duration of each episode, and the total time in AF (AF burden) between two sequential interrogations. Additionally, AF burden was automatically calculated and expressed as percentage (%).
Initial Evaluation and Assessed Parameter
Clinical examination, twelve-lead electrocardiogram along with assessment of the corrected Q-T interval (QTc), evaluation of renal function, and transthoracic echocardiographic study were performed at baseline. Left ventricular end-diastolic and end-systolic diameter (LVEDD and LVESD, respectively) were measured, and left ventricular ejection fraction (EF) was estimated according to the modified Simpson’s method. The anteroposterior diameter of the left atrium (LA) was measured at the parasternal short axis. Demographics, clinical characteristics and medication of the studied population are presented in the Table. The total time in AF, AF burden, and the number of AF episodes during the last six months before enrolment in the study were recalled during the interrogation of the pacemakers at the time of recruitment (baseline). Furthermore, AF duration per episode (mean AF duration) was calculated.
QTc was the Q-T interval corrected for heart rate and expressed in msec. It was calculated by the duration of the QT interval divided by the square root of the R-R interval, according to the Bazett’s formula.
AF burden was presented as percentage (%), and defined as the total time in AF (time in mode-switch) during follow-up, divided by the time of follow-up (six months) and multiplied by 100.
AF duration per episode (mean AF duration) was calculated by dividing the total time in AF by the number of AF episodes.
Randomized Treatment and Follow-Up
In the ranolazine group, ranolazine was administered at a dose of 375 mg twice daily, as an adjunctive therapy on top of conventional medication for CAD, according to current indications and the rules of the Hellenic National drug Organization.[23] This dose scheme was decided in order to avoid interactions with other drugs and serious side effects that could cause premature discontinuation of the treatment. In the control group, placebo was administered twice daily. During a six-month follow-up period, all patients were prospectively reevaluated with programmed visits in the pacemaker clinic. Interrogation of the devices and clinical evaluation was taking place every second month and when symptoms were reported, and performed by specialized physicians. The total time in AF, AF burden, the number of AF episodes during follow-up, mean AF duration per episode, and QTc were reassessed after six months of treatment and compared to that before randomization. Renal function was also evaluated at each programmed visit.
During follow-up, pacemaker settings and medication remained unaltered. If changes in treatment were necessary or clinical instability was observed, the patients were excluded from the study. Other exclusion criteria secondary to enrolment were: serious deterioration of renal function, serious adverse events associated with ranolazine and requiring temporary interruption or permanent cessation of treatment, consent withdrawal or loss of contact during follow-up. The study protocol was approved by the institutional ethics committee and all patients gave their informed consent before enrolment.
The investigators of the study were assigned into two groups. The first one was responsible for the enrollment in the study, randomization, and clinical follow-up, until the end of the study. The second group was blinded to treatment, and performed the interrogation of the pacing devices, data extraction, processing and analysis. All episodes were evaluated by the interval plots and electrocardiographic tracings saved by the devices and confirmed by experienced electrophysiologists.
Statistics
Statistical analysis was carried out by SPSS for Windows, version 17.0 (SPSS Inc. Chicago, IL, USA). Data are expressed as mean ± standard deviation (SD) for continuous variables and as frequency (percentage) for categorical parameters. Normality of distribution of continuous variables was assessed by the Kolmogorov-Smirnov test corrected by Lilliefors, and moreover confirmed graphically by Q-Q plots. Whenever the normality hypothesis was rejected, non-parametric significance tests were used.
Comparisons of continuous variables between groups were performed using Student’s t-test for independent samples, preceded by Levene’s test for equality of variances, or Mann–Whitney U non-parametric test, as appropriate. Comparisons of continuous variables within the same group prior to and following six months of treatment were performed using paired Student’s t-test or Wilcoxon signed-rank test for related samples, as appropriate. Categorical data were summarized in contingency tables and between groups comparisons were performed using the Fisher’s exact test.
All statistical significance tests were two-sided and the null hypothesis was the presumption of equality of means. Differences between and within groups were considered to be statistically significant if the null hypothesis could be rejected with >95% level of confidence (p-value <0.05).
Results
Baseline Characteristics
Out of the 460 patients’ pool, 77 met the eligibility criteria for the study. Seventy four of them provided written informed and were initially enrolled. Two patients were excluded from the study: one from the ranolazine group developed unstable angina and another from the control group had to change his treatment due to unsatisfactory control of his blood pressure (Figure 1). Demographics, clinical characteristics, history, medication of the remaining 72 studied patients and comparison between groups are presented in the Table. During the initial evaluation, patients treated with ranolazine and controls were comparable regarding the aforementioned parameters (Table 1).
Figure 1. The flow diagram of the study shows the initial assessment of eligibility, and the randomization of enrolled patients into adjunctive treatment with ranolazine or placebo.
Table 1. Demographics, clinical characteristics, history of revascularization and medication of the studied population,presented in groups, according to randomization.
yrs: years, SSS: sick sinus syndrome, AVB: atrio-ventricular conduction block, CABG: coronary artery bypass grafting, PCI: percutaneous coronary intervention, EF:ejection fraction, LVEDD: left ventricular end-diastolic diameter, LVESD: left ventricular end-systolic diameter, LA: left atrium, QTc: corrected Q-T interval, AF: atrial fibrillation, hrs: hours, ACE: angiotensin converting enzyme, ARB: angiotensin receptor blockers
| Ranolazine group(n=36) | Control group(n=36) | p value | |
|---|---|---|---|
| Age (yrs) | 73.8 ± 6.8 | 73.9 ± 4.5 | 0.726 |
| Male gender (%) | 25 (69.4%) | 22 (61.1%) | 0.621 |
| SSS | 21 (58.3%) | 23 (63.9%) | 0.809 |
| AVB | 15 (41.7%) | 13 (36.1%) | 0.809 |
| Prior revascularization | 18 (50.0%) | 15 (41.7%) | 0.637 |
| CABG | 5 (13.9%) | 4 (11.1%) | 1.000 |
| PCI | 13 (36.1%) | 11 (30.6%) | 0.803 |
| Angina | 21 (58.9%) | 23 (63.9%) | 0.809 |
| Positive stress test/scintigraphy | 36 (100%) | 36 (100%) | 1.000 |
| Echocardiography | |||
| No | 57 (62) | 182 (63.6) | 245 (66.6) |
| EF (%) | 54.6 ± 6.3 | 54.3 ± 7.6 | 0.943 |
| LVEDD (mm) | 51.4 ± 2.7 | 50.7 ± 2.8 | 0.233 |
| LVESD (mm) | 32.4 ± 2.2 | 32.1 ± 2.2 | 0.446 |
| LA diameter (mm) | 42.9 ± 2.7 | 42.6 ± 3.1 | 0.687 |
| QTc (msec) | 436 ± 10 | 437 ± 9 | 0.857 |
| AF statistics at baseline | |||
| total time in AF (hrs) | 81.56 ± 45.24 | 80.28 ± 43.198 | 0.903 |
| AF burden (%) | 1.89 ± 1.05 | 1.86 ± 1.00 | 0.903 |
| number of AF episodes | 77.3 ± 36.1 | 71.56 ± 30.92 | 0.468 |
| mean duration (hrs) | 1.05 ± 0.41 | 1.12 ± 0.43 | 0.486 |
| Comorbidities | |||
| hypertension | 28 (77.8%) | 29 (80.6%) | 1.000 |
| dyslipidemia | 24 (66.7%) | 26 (72.2%) | 0.798 |
| diabetes mellitus | 8 (22.2%) | 3 (8.3%) | 0.189 |
| thyroid disease | 2 (5.6%) | 3 (8.3%) | 1.000 |
| Medication | |||
| nitrates | 30 (83.3%) | 33 (91.6%) | 0.631 |
| β-blocker | 36 (100.0%) | 35 (97.2%) | 1.000 |
| ACE inhibitor/ARB | 29 (80.6%) | 25 (69.4%) | 0.415 |
| calcium channel blocker | 12 (33.3%) | 14 (38.9%) | 0.806 |
| dihydropyridine | 9 (25.0%) | 12 (33.3%) | 0.605 |
| non-dihydropyridine | 3 (8.3%) | 2 (5.6%) | 1.000 |
| statin | 34 (94.4%) | 36 (100%) | 0.798 |
| diuretics | 13 (36.1%) | 16 (44.4%) | 0.631 |
Treatment and Follow-Up
Ranolazine was overall well tolerated and no serious side effects were reported. Initially, five patients complained about constipation, abdominal discomfort or dizziness within the first two weeks of ranolazine administration. However, these symptoms were attenuated later on and patients continued treatment for the entire follow-up period.
Within group comparisons showed a statistically significant decrease of the total time of AF with ranolazine, from 81.56 ± 45.24 hours before treatment to 68.71 ± 34.84 hours during therapy (p=0.002), as presented in Figure 2. AF burden decreased too (Figure 3), from 1.89 ± 1.05 % to 1.59 ± 0.81 % (p=0.002). The number of AF episodes under treatment with ranolazine was not significantly lower compared to that before treatment (75.53 ± 33.13 episodes versus 77.33 ± 36.12 episodes, respectively, p=0.61), as depicted in Figure 4. However, the mean AF duration decreased from 1.05 ± 0.41 hours before treatment to 0.92 ± 0.35 hours (p=0.01) with ranolazine (Figure 5). The duration of QTc interval following ranolazine administration was comparable with that before treatment (436 ± 10 msec and 438 ± 10 msec, respectively, p=0.25).
Figure 2. Total time in AF during the last six months before treatment (white bars) and during the 6-month period of treatment (dark bars) is shown in the two groups. Statistical significance of difference within each group (p-values) is also presented.
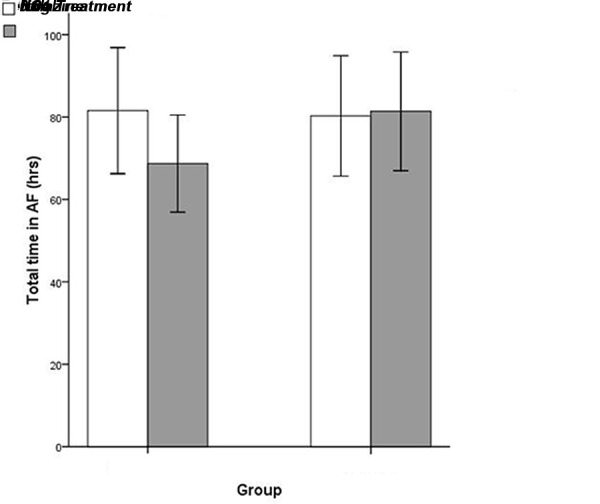
AF: atrial fibrillation, hrs: hours, NS: statistically not significant (p>0.05)
Figure 3. AF burden (%) during the six months before (white bars) and under treatment (dark bars) is compared within each group. For each comparison, p-value is presented.
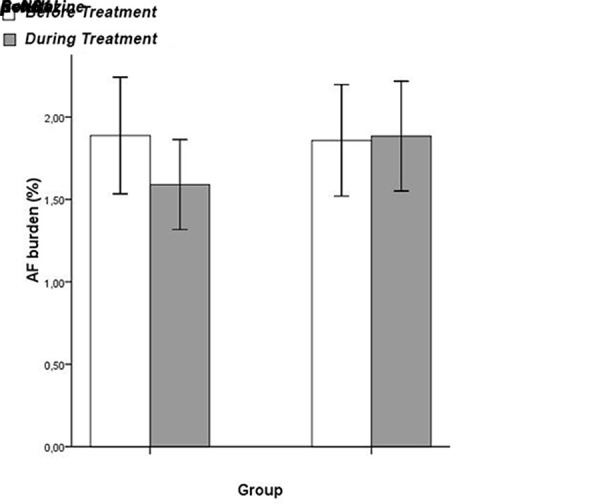
AF: atrial fibrillation, NS: statistically not significant (p>0.05)
Figure 4. In both groups, the number of AF episodes before (white bars) and during treatment (dark bars) are not significantly different.
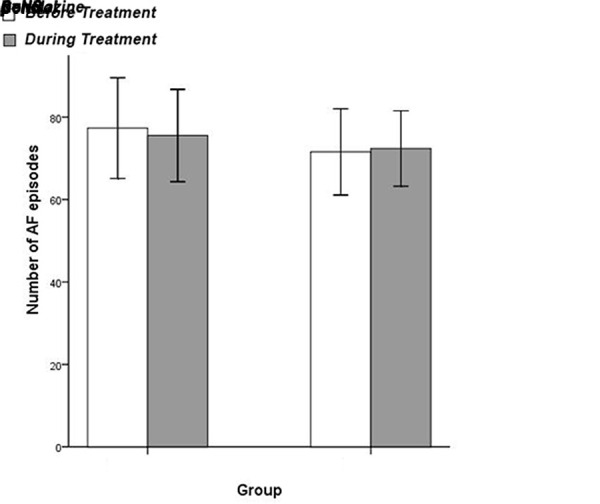
AF: atrial fibrillation, NS: p-value not statistically significant (p>0.05)
Figure 5. Mean AF duration before treatment (white bars) and during treatment (dark bars) is shown by groups. Statistical significance of comparisons within each group (p-values) is also presented.
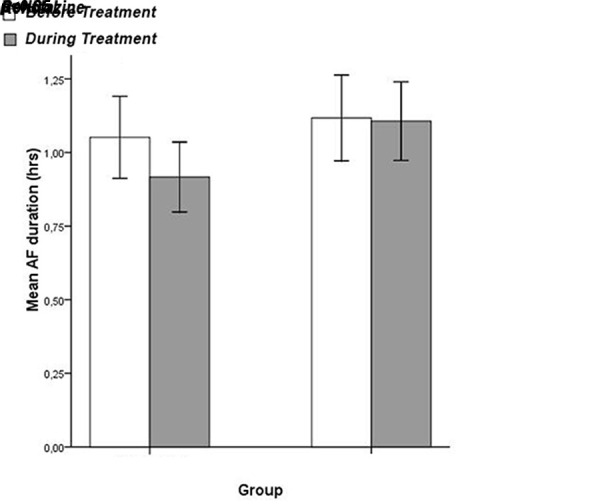
AF: atrial fibrillation, hrs: hours, NS: statistically not significant (p>0.05)
In the control group, no significant changes were observed between the six-month period before enrolment in the study and during follow-up regarding the total time in AF (80.28 ± 43.20 hours versus 81.40 ± 42.54 hours, p=0.57), AF burden (1.86 ± 1.00 % versus 1.88 ± 0.99 %, p=0.57), mean time in AF per episode (1.12 ± 0.43 hours versus 1.11 ± 0.40 hours, p=0.53), the number of AF episodes (71.56 ± 30.92 episodes versus 72.39 ± 26.99 episodes, p=0.66), and QTc duration (437 ± 9 msec versus 437 ± 10 msec, p=0.60).
The comparison between groups confirmed the significant difference in the mean duration of AF episodes (p=0.034). Furthermore, when the changes in all the aforementioned parameters were compared between groups, a statistically significant difference favoring ranolazine was found (Table 2).
Table 2. The differences in total time in AF, AF burden, number of AF episodes, and mean duration of each episode between baseline and during follow-up are compared between the two groups.
hrs: hours
| Ranolazine group(n=36) | Control group(n=36) | p value | |
|---|---|---|---|
| Difference in total time in AF (hrs) | - 12.85 ± 22.94 | 1.13 ± 11.77 | 0.002 |
| Difference in AF burden (%) | - 0.30 ± 0.53 | 0.03 ± 0.27 | 0.002 |
| Difference in the number of AF episodes | - 1.81 ± 12.55 | 0.83 ± 11.28 | 0.528 |
| Difference in mean duration (hrs) | - 0.13 ± 0.30 | - 0.01 ± 0.19 | 0.041 |
Discussion
In the present study, the effect of adjunctive treatment with ranolazine on AF burden was evaluated in patients with ischemic heart disease and PAF. Implanted dual-chamber pacing devices were used for heart rhythm monitoring, detection of asymptomatic PAF, and providing information regarding the number and duration of AF episodes. At the selected dose-scheme, ranolazine was associated with a statistically significant decrease in the total time in AF, AF burden, and the duration of each AF episode.
The studied patients were clinically stable during follow-up, so that the progression of ischemia would not be involved in the results. Patients with highly symptomatic AF necessitating antiarrhythmic medication were excluded, in order i) to avoid interactions between the antiarrhythmic agents and ranolazine, and ii) to evaluate the pure antiarrhythmic effect of ranolazine. These restrictions resulted in a highly selected sample, and give advantages to the study.
Total AF Burden
Experimental and clinical studies suggest an antifibrillatory impact of ranolazine on atrial myocardium. It has been reported that ranolazine is more effective than lidocaine in terminating AF in perfused canine right atrial preparations, mainly through the development of a rate-dependent postrepolarization refractoriness.[11] In canine isolated atrial preparations, ranolazine was comparable to propafenone in terminating acetylcholine-mediated persistent AF.[24] Besides, ranolazine suppressed triggers of AF originating from the sleeves of pulmonary veins.[25] Additionally, it has been proposed that ranolazine may prevent AF by suppressing cellular calcium overload and delayed afterdepolarizations that can trigger atrial arrhythmias.[26] The role of the late phase 3 EAD-induced trigger activity has been shown to be involved in the reinduction immediately after an episode of atrial fibrillation and the prolongation of the total duration of the arrhythmia.[27]
In human right atrial appendages obtained from patients undergoing heart surgery, ranolazine was found to suppress calcium- or isoprenaline-induced premature atrial contractions that might initiate or perpetuate AF.[28] Furthermore, there are clinical observations suggesting that oral ranolazine could be used in a “pill in the pocket” approach to convert PAF, and that it could facilitate electrical cardioversion in cardioversion-resistant cases. [12,29]
In accordance with these studies, we found that treatment with ranolazine at the aforementioned dose-scheme was associated with decreased AF burden during follow-up and shorter AF duration per episode. These observations indicate the earlier termination of AF episodes and could be attributed to the use-dependent properties of ranolazine, the increase of atrial refractoriness and the suppression of premature contractions in the atrium or pulmonary veins that can not only induce but also perpetuate AF. The reduction of AF burden and AF duration per episode may have an even greater clinical importance in patients with higher AF burden and more frequent AF relapse.[30] Finally, an additional anti-ischemic effect and the improvement in diastolic dysfunction might also be involved in this beneficial effect, since ischemia has been implicated in the pathophysiology of AF.[31-35]
Dual-chamber pacemakers have been used as tools for the evaluation of the efficacy of antiarrhythmic agents before. In a recent study, budiodarone, a novel chemical analogue of amiodarone, administered at a dose of 200 mg daily in patients with PAF and a dual-chamber pacemaker, decrease in AF burden by 14% approximately.[36] Our results are comparable with those of budiodarone, since ranolazine was associated with a decrease in total time in AF and AF burden by 16%. The antiarrhythmic effect of ranolazine was observed despite the relatively low initial load of AF in the studied population. Although this effect may have a small impact on the quality of life among asymptomatic patients or those with short AF duration, it is important in terms of pathophysiology and deserves further clinical investigation.
Number of AF Episodes
Treatment with ranolazine was not associated with a significant decrease in the number of AF episodes. This can be explained if the following aspects are taken under consideration: i) Some episodes of AF might have been aborted by the beneficial effect of atrial pacing. In patients with SSS, atrial pacing reduces the incidence of AF, especially when ventricular pacing is minimized.[37,38] Besides, it has been reported that atrial pacing diminishes the arrhythmogenic dispersion of atrial refractoriness associated with bradycardia.[39] Furthermore, atrial pacing may prevent the induction of AF by suppressing premature atrial contractions.[40,41] ii) Ranolazine exhibits rate-dependent antiarrhythmic properties.[9,11,42] This may result in an increased effect of the drug during each PAF episode compared to that in sinus rhythm. iii) Higher doses of ranolazine, if well tolerated, may be more effective in reducing AF recurrence. iv) The studied population was mainly characterized by short and sporadic episodes of PAF. This might be an additional reason for not observing any significant difference in the number of AF episodes with ranolazine. The confirmation of this antiarrhythmic effect in patients with high AF burden is a challenge for the future and it could introduce new indications for the use of ranolazine.
QTc Duration and Side Effects
Ranolazine was not associated with a significant prolongation in the QTc segment. In accordance with our observation, in the MERLIN-TIMI 36 trial, ranolazine did not have a major impact on the QT interval, although, during chronic treatment, the oral dose was 1000 mg twice daily for the majority of the patients (83%).[43] In that study, in only 0.9% of the studied patients the dose of ranolazine was reduced due to persistent QTc prolongation.
Ranolazine can be associated with minor side effects, such as dizziness, nausea, constipation and headache.[44] The MERLIN-TIMI 36 trial reported discontinuation of the drug due to adverse events in 8.8% of the patients who received ranolazine.[43] In our study, a lower dose of ranolazine was associated with minor symptoms that were diminished following the first days of treatment. No significant interactions with other drugs were observed. These observations suggest that treatment with ranolazine at the dose of 375 mg twice daily is an effective and safe option as an adjunctive therapy in patients with coronary artery disease, relatively preserved LV function and paroxysmal AF.
Limitations of the Study
Data concerning AF recurrence and duration derived from the pacing devices, based on algorithms of high atrial rate detection and also on the statistics collected and saved by the pacemakers. Therefore, more specific details regarding the characteristics of AF, and the pathophysiologic mechanisms of induction and perpetuation of the arrhythmia are limited and beyond the main purpose of the study.
Enrollment in the study was based on the presence of ischemic heart disease and not on the severity of AF symptoms, the frequency of recurrences, or the duration of the arrhythmia. Therefore, total time in AF, AF burden and mean AF duration were relatively small, and their decrease with ranolazine was proportionately limited. Despite this, our findings are statistically significant, and imply that ranolazine warrants further evaluation among non-paced patients, and individuals with higher AF burden, more frequent and longer AF episodes.
The potential antiarrhythmic effect of pacing cannot be ruled out. However, this beneficial impact was equally distributed in the controls and the ranolazine-group.
The number of patients enrolled in the study is relatively small, due to the specific inclusion criteria and the indications for ranolazine administration. Therefore, they were not separately studied in different groups according to a predominantly atrial pacing (sinus node dysfunction) versus ventricular pacing (impaired atrioventricular conduction). A potential correlation between the ischemic burden and the effect of ranolazine was not assessed in the study. However, in the within-group statistical analysis, each patient was the control of himself and the antiarrhythmic effect was evaluated on the same ischemic substrate, and with the same pacing mode before and following treatment.
Conclusions
In a selected population of patients with CAD, PAF, and a dual-chamber pacemaker, ranolazine may have an antiarhythmic effect, indicated by a shorter total time in AF, a reduced AF burden, and decreased mean AF duration, as documented by the pacing devices. These observations may imply a beneficial effect of ranolazine administration in patients with CAD and PAF, necessitating further clinical confirmation.
Disclosures
None.
References
- 1.Antzelevitch Charles, Belardinelli Luiz, Zygmunt Andrew C, Burashnikov Alexander, Di Diego José M, Fish Jeffrey M, Cordeiro Jonathan M, Thomas George. Electrophysiological effects of ranolazine, a novel antianginal agent with antiarrhythmic properties. Circulation. 2004 Aug 24;110 (8):904–10. doi: 10.1161/01.CIR.0000139333.83620.5D. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kumar Kapil, Nearing Bruce D, Carvas Marcelo, Nascimento Bruno C G, Acar Mariana, Belardinelli Luiz, Verrier Richard L. Ranolazine exerts potent effects on atrial electrical properties and abbreviates atrial fibrillation duration in the intact porcine heart. J. Cardiovasc. Electrophysiol. 2009 Jul;20 (7):796–802. doi: 10.1111/j.1540-8167.2009.01437.x. [DOI] [PubMed] [Google Scholar]
- 3.Carvas Marcelo, Nascimento Bruno C G, Acar Mariana, Nearing Bruce D, Belardinelli Luiz, Verrier Richard L. Intrapericardial ranolazine prolongs atrial refractory period and markedly reduces atrial fibrillation inducibility in the intact porcine heart. J. Cardiovasc. Pharmacol. 2010 Mar;55 (3):286–91. doi: 10.1097/FJC.0b013e3181d26416. [DOI] [PubMed] [Google Scholar]
- 4.Sicouri Serge, Burashnikov Alexander, Belardinelli Luiz, Antzelevitch Charles. Synergistic electrophysiologic and antiarrhythmic effects of the combination of ranolazine and chronic amiodarone in canine atria. Circ Arrhythm Electrophysiol. 2010 Feb;3 (1):88–95. doi: 10.1161/CIRCEP.109.886275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Miles Ronald H, Passman Rod, Murdock David K. Comparison of effectiveness and safety of ranolazine versus amiodarone for preventing atrial fibrillation after coronary artery bypass grafting. Am. J. Cardiol. 2011 Sep 1;108 (5):673–6. doi: 10.1016/j.amjcard.2011.04.017. [DOI] [PubMed] [Google Scholar]
- 6.Murdock David K, Kersten Mary, Kaliebe Jeff, Larrain German. The use of oral ranolazine to convert new or paroxysmal atrial fibrillation: a review of experience with implications for possible "pill in the pocket" approach to atrial fibrillation. Indian Pacing Electrophysiol J. 2009 Sep 01;9 (5):260–7. [PMC free article] [PubMed] [Google Scholar]
- 7.Scirica Benjamin M, Morrow David A, Hod Hanoch, Murphy Sabina A, Belardinelli Luiz, Hedgepeth Chester M, Molhoek Peter, Verheugt Freek W A, Gersh Bernard J, McCabe Carolyn H, Braunwald Eugene. Effect of ranolazine, an antianginal agent with novel electrophysiological properties, on the incidence of arrhythmias in patients with non ST-segment elevation acute coronary syndrome: results from the Metabolic Efficiency With Ranolazine for Less Ischemia in Non ST-Elevation Acute Coronary Syndrome Thrombolysis in Myocardial Infarction 36 (MERLIN-TIMI 36) randomized controlled trial. Circulation. 2007 Oct 9;116 (15):1647–52. doi: 10.1161/CIRCULATIONAHA.107.724880. [DOI] [PubMed] [Google Scholar]
- 8.Aidonidis Isaac, Doulas Konstantinos, Hatziefthimiou Apostolia, Tagarakis Georgios, Simopoulos Vassilios, Rizos Ioannis, Tsilimingas Nikolaos, Molyvdas Paschalis-Adam. Ranolazine-induced postrepolarization refractoriness suppresses induction of atrial flutter and fibrillation in anesthetized rabbits. J. Cardiovasc. Pharmacol. Ther. 2013 Jan;18 (1):94–101. doi: 10.1177/1074248412453874. [DOI] [PubMed] [Google Scholar]
- 9.Rajamani Sridharan, El-Bizri Nesrine, Shryock John C, Makielski Jonathan C, Belardinelli Luiz. Use-dependent block of cardiac late Na(+) current by ranolazine. Heart Rhythm. 2009 Nov;6 (11):1625–31. doi: 10.1016/j.hrthm.2009.07.042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Antzelevitch Charles, Burashnikov Alexander, Sicouri Serge, Belardinelli Luiz. Electrophysiologic basis for the antiarrhythmic actions of ranolazine. Heart Rhythm. 2011 Aug;8 (8):1281–90. doi: 10.1016/j.hrthm.2011.03.045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Burashnikov Alexander, Di Diego José M, Zygmunt Andrew C, Belardinelli Luiz, Antzelevitch Charles. Atrium-selective sodium channel block as a strategy for suppression of atrial fibrillation: differences in sodium channel inactivation between atria and ventricles and the role of ranolazine. Circulation. 2007 Sep 25;116 (13):1449–57. doi: 10.1161/CIRCULATIONAHA.107.704890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Murdock DK, Reiffel JA, Kaliebe JW, Larrain G. The conversion of paroxysmal or initial onset of atrial fibrillation with oral ranolazine: implications for “pill in the pocket” approach in structural heart diseas. J Am Coll Cardiol. 2010;55:A6–E58. [Google Scholar]
- 13.Miles Ronald H, Passman Rod, Murdock David K. Comparison of effectiveness and safety of ranolazine versus amiodarone for preventing atrial fibrillation after coronary artery bypass grafting. Am. J. Cardiol. 2011 Sep 1;108 (5):673–6. doi: 10.1016/j.amjcard.2011.04.017. [DOI] [PubMed] [Google Scholar]
- 14.Page R L, Wilkinson W E, Clair W K, McCarthy E A, Pritchett E L. Asymptomatic arrhythmias in patients with symptomatic paroxysmal atrial fibrillation and paroxysmal supraventricular tachycardia. Circulation. 1994 Jan;89 (1):224–7. doi: 10.1161/01.cir.89.1.224. [DOI] [PubMed] [Google Scholar]
- 15.Strickberger S Adam, Ip John, Saksena Sanjeev, Curry Ken, Bahnson Tristram D, Ziegler Paul D. Relationship between atrial tachyarrhythmias and symptoms. Heart Rhythm. 2005 Feb;2 (2):125–31. doi: 10.1016/j.hrthm.2004.10.042. [DOI] [PubMed] [Google Scholar]
- 16.Israel C W, Barold S S. Pacemaker systems as implantable cardiac rhythm monitors. Am. J. Cardiol. 2001 Aug 15;88 (4):442–5. doi: 10.1016/s0002-9149(01)01700-3. [DOI] [PubMed] [Google Scholar]
- 17.Mehra Rahul, Ziegler Paul, Koehler Jodi. Diagnostic information in implantable devices that pertain to endpoints in atrial fibrillation studies. Heart Rhythm. 2004 Jul;1 (2 Suppl):B64–9, discussion B69. doi: 10.1016/j.hrthm.2004.04.010. [DOI] [PubMed] [Google Scholar]
- 18.Glotzer Taya V, Hellkamp Anne S, Zimmerman John, Sweeney Michael O, Yee Raymond, Marinchak Roger, Cook James, Paraschos Alexander, Love John, Radoslovich Glauco, Lee Kerry L, Lamas Gervasio A. Atrial high rate episodes detected by pacemaker diagnostics predict death and stroke: report of the Atrial Diagnostics Ancillary Study of the MOde Selection Trial (MOST). Circulation. 2003 Apr 1;107 (12):1614–9. doi: 10.1161/01.CIR.0000057981.70380.45. [DOI] [PubMed] [Google Scholar]
- 19.Cheung Jim W, Keating Richard J, Stein Kenneth M, Markowitz Steven M, Iwai Sei, Shah Bindi K, Lerman Bruce B, Mittal Suneet. Newly detected atrial fibrillation following dual chamber pacemaker implantation. J. Cardiovasc. Electrophysiol. 2006 Dec;17 (12):1323–8. doi: 10.1111/j.1540-8167.2006.00648.x. [DOI] [PubMed] [Google Scholar]
- 20.Orlov Michael V, Ghali Jalal K, Araghi-Niknam Mohsen, Sherfesee Lou, Sahr Diane, Hettrick Douglas A. Asymptomatic atrial fibrillation in pacemaker recipients: incidence, progression, and determinants based on the atrial high rate trial. Pacing Clin Electrophysiol. 2007 Mar;30 (3):404–11. doi: 10.1111/j.1540-8159.2007.00682.x. [DOI] [PubMed] [Google Scholar]
- 21.Willems Rik, Morck Margaret L, Exner Derek V, Rose Sarah M, Gillis Anne M. Ventricular high-rate episodes in pacemaker diagnostics identify a high-risk subgroup of patients with tachy-brady syndrome. Heart Rhythm. 2004 Oct;1 (4):414–21. doi: 10.1016/j.hrthm.2004.06.004. [DOI] [PubMed] [Google Scholar]
- 22.Camm A John, Kirchhof Paulus, Lip Gregory Y H, Schotten Ulrich, Savelieva Irene, Ernst Sabine, Van Gelder Isabelle C, Al-Attar Nawwar, Hindricks Gerhard, Prendergast Bernard, Heidbuchel Hein, Alfieri Ottavio, Angelini Annalisa, Atar Dan, Colonna Paolo, De Caterina Raffaele, De Sutter Johan, Goette Andreas, Gorenek Bulent, Heldal Magnus, Hohloser Stefan H, Kolh Philippe, Le Heuzey Jean-Yves, Ponikowski Piotr, Rutten Frans H. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Europace. 2010 Oct;12 (10):1360–420. doi: 10.1093/europace/euq350. [DOI] [PubMed] [Google Scholar]
- 23.Henderson Robert A, O'Flynn Norma. Management of stable angina: summary of NICE guidance. Heart. 2012 Mar;98 (6):500–7. doi: 10.1136/heartjnl-2011-301436. [DOI] [PubMed] [Google Scholar]
- 24.Burashnikov Alexander, Belardinelli Luiz, Antzelevitch Charles. Atrial-selective sodium channel block strategy to suppress atrial fibrillation: ranolazine versus propafenone. J. Pharmacol. Exp. Ther. 2012 Jan;340 (1):161–8. doi: 10.1124/jpet.111.186395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sicouri Serge, Glass Aaron, Belardinelli Luiz, Antzelevitch Charles. Antiarrhythmic effects of ranolazine in canine pulmonary vein sleeve preparations. Heart Rhythm. 2008 Jul;5 (7):1019–26. doi: 10.1016/j.hrthm.2008.03.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Song Yejia, Shryock John C, Belardinelli Luiz. An increase of late sodium current induces delayed afterdepolarizations and sustained triggered activity in atrial myocytes. Am. J. Physiol. Heart Circ. Physiol. 2008 May;294 (5):H2031–9. doi: 10.1152/ajpheart.01357.2007. [DOI] [PubMed] [Google Scholar]
- 27.Burashnikov Alexander, Antzelevitch Charles. Reinduction of atrial fibrillation immediately after termination of the arrhythmia is mediated by late phase 3 early afterdepolarization-induced triggered activity. Circulation. 2003 May 13;107 (18):2355–60. doi: 10.1161/01.CIR.0000065578.00869.7C. [DOI] [PubMed] [Google Scholar]
- 28.Sossalla Samuel, Kallmeyer Birte, Wagner Stefan, Mazur Marek, Maurer Ulrike, Toischer Karl, Schmitto Jan D, Seipelt Ralf, Schöndube Friedrich A, Hasenfuss Gerd, Belardinelli Luiz, Maier Lars S. Altered Na(+) currents in atrial fibrillation effects of ranolazine on arrhythmias and contractility in human atrial myocardium. J. Am. Coll. Cardiol. 2010 May 25;55 (21):2330–42. doi: 10.1016/j.jacc.2009.12.055. [DOI] [PubMed] [Google Scholar]
- 29.Murdock David K, Kaliebe Jeff, Larrain German. The use of ranolazine to facilitate electrical cardioversion in cardioversion-resistant patients: a case series. Pacing Clin Electrophysiol. 2012 Mar;35 (3):302–7. doi: 10.1111/j.1540-8159.2011.03298.x. [DOI] [PubMed] [Google Scholar]
- 30.Wijffels M C, Kirchhof C J, Dorland R, Allessie M A. Atrial fibrillation begets atrial fibrillation. A study in awake chronically instrumented goats. Circulation. 1995 Oct 1;92 (7):1954–68. doi: 10.1161/01.cir.92.7.1954. [DOI] [PubMed] [Google Scholar]
- 31.Eldar M, Canetti M, Rotstein Z, Boyko V, Gottlieb S, Kaplinsky E, Behar S. Significance of paroxysmal atrial fibrillation complicating acute myocardial infarction in the thrombolytic era. SPRINT and Thrombolytic Survey Groups. Circulation. 1998 Mar 17;97 (10):965–70. doi: 10.1161/01.cir.97.10.965. [DOI] [PubMed] [Google Scholar]
- 32.Goto Shinya, Bhatt Deepak L, Röther Joachim, Alberts Mark, Hill Michael D, Ikeda Yasuo, Uchiyama Shinichiro, D'Agostino Ralph, Ohman E Magnus, Liau Chiau-Suong, Hirsch Alan T, Mas Jean-Louis, Wilson Peter W F, Corbalán Ramón, Aichner Franz, Steg P Gabriel. Prevalence, clinical profile, and cardiovascular outcomes of atrial fibrillation patients with atherothrombosis. Am. Heart J. 2008 Nov;156 (5):855–63, 863.e2. doi: 10.1016/j.ahj.2008.06.029. [DOI] [PubMed] [Google Scholar]
- 33.Depta Jeremiah P, Bhatt Deepak L. Atherothrombosis and atrial fibrillation: Important and often overlapping clinical syndromes. Thromb. Haemost. 2010 Oct;104 (4):657–63. doi: 10.1160/TH10-05-0332. [DOI] [PubMed] [Google Scholar]
- 34.Weijs Bob, Pisters Ron, Haest Rutger J, Kragten Johannes A, Joosen Ivo A, Versteylen Mathijs, Timmermans Carl C, Pison Laurent, Blaauw Yuri, Hofstra Leonard, Nieuwlaat Robby, Wildberger Joachim, Crijns Harry J. Patients originally diagnosed with idiopathic atrial fibrillation more often suffer from insidious coronary artery disease compared to healthy sinus rhythm controls. Heart Rhythm. 2012 Dec;9 (12):1923–9. doi: 10.1016/j.hrthm.2012.08.013. [DOI] [PubMed] [Google Scholar]
- 35.Tagarakis Georgios I, Aidonidis Isaac, Daskalopoulou Stella S, Simopoulos Vassilios, Liouras Vassilios, Daskalopoulos Marios E, Parisis Charalampos, Papageorgiou Kiriaki, Skoularingis Ioannis, Triposkiadis Filippos, Molyvdas Paschalis-Adam, Tsilimingas Nikolaos B. Effect of ranolazine in preventing postoperative atrial fibrillation in patients undergoing coronary revascularization surgery. Curr Vasc Pharmacol. 2013 Nov;11 (6):988–91. doi: 10.2174/157016111106140128123506. [DOI] [PubMed] [Google Scholar]
- 36.Ezekowitz Michael D, Nagarakanti Rangadham, Lubinski Andrzej, Bandman Olga, Canafax Daniel, Ellis David J, Milner Peter G, Ziola Margaret, Thibault Bernard, Hohnloser Stefan H. A randomized trial of budiodarone in paroxysmal atrial fibrillation. J Interv Card Electrophysiol. 2012 Jun;34 (1):1–9. doi: 10.1007/s10840-011-9636-3. [DOI] [PubMed] [Google Scholar]
- 37.Inoue Noriko, Ishikawa Toshiyuki, Sumita Shinichi, Kobayashi Tsukasa, Matsushita Kohei, Matsumoto Katsumi, Taima Minoru, Shimura Miei, Uchino Kazuaki, Kimura Kazuo, Umemura Satoshi. Suppression of atrial fibrillation by atrial pacing. Circ. J. 2006 Nov;70 (11):1398–401. doi: 10.1253/circj.70.1398. [DOI] [PubMed] [Google Scholar]
- 38.Sweeney Michael O, Bank Alan J, Nsah Emmanuel, Koullick Maria, Zeng Qian Cathy, Hettrick Douglas, Sheldon Todd, Lamas Gervasio A. Minimizing ventricular pacing to reduce atrial fibrillation in sinus-node disease. N. Engl. J. Med. 2007 Sep 6;357 (10):1000–8. doi: 10.1056/NEJMoa071880. [DOI] [PubMed] [Google Scholar]
- 39.Han J, Millet D, Chizzonitti B, Moe G K. Temporal dispersion of recovery of excitability in atrium and ventricle as a function of heart rate. Am. Heart J. 1966 Apr;71 (4):481–7. doi: 10.1016/0002-8703(66)90213-4. [DOI] [PubMed] [Google Scholar]
- 40.Dimmer C, Szili-Torok T, Tavernier R, Verstraten T, Jordaens L J. Initiating mechanisms of paroxysmal atrial fibrillation. Europace. 2003 Jan;5 (1):1–9. doi: 10.1053/eupc.2002.0273. [DOI] [PubMed] [Google Scholar]
- 41.Miki Yuko, Ishikawa Toshiyuki, Inoue Noriko, Yamakawa Youhei, Kobayashi Tsukasa, Matsushita Kohei, Matsumoto Katsumi, Taima Minoru, Kosuge Masami, Sumita Shinichi, Uchino Kazuaki, Kimura Kazuo, Umemura Satoshi. Efficacy of consistent atrial pacing algorithm for suppression of atrial arrhythmias in patients with sick sinus syndrome and atrial fibrillation. Int Heart J. 2008 May;49 (3):273–80. doi: 10.1536/ihj.49.273. [DOI] [PubMed] [Google Scholar]
- 42.Zygmunt Andrew C, Nesterenko Vladislav V, Rajamani Sridharan, Hu Dan, Barajas-Martinez Hector, Belardinelli Luiz, Antzelevitch Charles. Mechanisms of atrial-selective block of Na⁺ channels by ranolazine: I. Experimental analysis of the use-dependent block. Am. J. Physiol. Heart Circ. Physiol. 2011 Oct;301 (4):H1606–14. doi: 10.1152/ajpheart.00242.2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Morrow David A, Scirica Benjamin M, Karwatowska-Prokopczuk Ewa, Murphy Sabina A, Budaj Andrzej, Varshavsky Sergei, Wolff Andrew A, Skene Allan, McCabe Carolyn H, Braunwald Eugene. Effects of ranolazine on recurrent cardiovascular events in patients with non-ST-elevation acute coronary syndromes: the MERLIN-TIMI 36 randomized trial. JAMA. 2007 Apr 25;297 (16):1775–83. doi: 10.1001/jama.297.16.1775. [DOI] [PubMed] [Google Scholar]
- 44.Stone Peter H, Gratsiansky Nikolay A, Blokhin Alexey, Huang I-Zu, Meng Lixin. Antianginal efficacy of ranolazine when added to treatment with amlodipine: the ERICA (Efficacy of Ranolazine in Chronic Angina) trial. J. Am. Coll. Cardiol. 2006 Aug 1;48 (3):566–75. doi: 10.1016/j.jacc.2006.05.044. [DOI] [PubMed] [Google Scholar]