

Abstract
When information is exchanged across disciplinary boundaries, resources are shared, and discipline-specific approaches are altered to achieve a common scientific goal, we create a new intellectual space for transdisciplinary research. This approach, fostered heavily by multiple National Cancer Institute funded initiatives, has the potential to forge new understanding of major public health issues. By breaking down disciplinary barriers, we work toward making real, meaningful, and lasting forward motion in addressing key public health issues. One of the transdisciplinary initiatives of the National Cancer Institute is TREC: Transdisicplinary Research on Energetics and Cancer. In this article, we review the goals and scope of TREC, as well as the ways in which the initiative promotes transdisciplinary science. A particular focus is on multiple examples of the most unique aspect of the initiative: the funding of developmental projects across multiple TREC centers, toward the goal of incubating high risk science that has the potential to translate into major leaps forward in understanding energetics in cancer. As we enter an era of greater focus on investigator initiated science, new approaches may be needed to ensure that the peer review process is not solely organized along disciplinary lines. Inclusion of expertise regarding transdisciplinarity, as well as representation from multiple scientific disciplines within a panel may allow transdisciplinary research to receive an educated hearing. The body of researchers trained to work in a transdisciplinary research space is ideally suited to address these challenges.
Introduction
Transdisciplinary research gained attention in the late 1990s when the National Cancer Institute (NCI) mandated its use in funding initiatives aimed at addressing tobacco use, cancer communications, cancer disparities, and energy balance in cancer.(1–4) The last of these initiatives is a U54 cooperative agreement called Transdisciplinary Research in Energetics and Cancer (TREC). TREC was first funded in 2005 and is in its second round of funding.(3) The impetus for the development of TREC was a desire to capture the multi-levels of influence of energy balance in cancer control outcomes by including transdisciplinary scholars from the social, behavioral, and biological sciences on integrated teams. As part of this cooperative agreement, NCI scientists partner with TREC investigators to work jointly to support and stimulate activities.
The TREC initiative has two main goals, namely to enhance knowledge of the current mechanisms underlying the association between energy balance and carcinogenesis (from cellular, animal or human models to genetics and genomics and across the cancer continuum from causation and prevention to survivorship and recurrence) and to explore and integrate the etiology of obesity behavior and relevant health behavior theories, with broad population impact at the social-environmental and policy levels for prevention and control of obesity.
Rosenfield defines transdisciplinary research as research in which information is exchanged, resources are shared, and discipline-specific approaches are altered to achieve a common scientific goal.(5) It is posited that this approach will achieve the highest degree of disciplinary collaboration. In this approach, scholars begin to transcend their disciplinary boundaries to create new intellectual space. The approach has the potential to forge new understandings of major public health problems like energetics and cancer by breaking down the usual barriers to collaboration. Emmons et al. use energetics and cancer as an example of the inefficiency that occurs when boundaries between the social, behavioral, and biological are rigidly maintained in research, saying, “If the primary focus of work in obesity and energy balance is on sociocultural factors, eventually the limits of not considering both environmental and physiologic factors will be realized.”(6)
The TREC sites have leadership in a variety of disciplines, including molecular biology, genetics, oncology, psychology, nutrition, epidemiology, exercise physiology, biostatistics, social epidemiology, geography, social work, sociology, behavioral psychology, economics, cancer biology, and computer science. The TREC Steering Committee encompasses many areas of expertise, and more investigators have been brought in when additional expertise was needed. By meeting frequently, the group’s steering committee, made up of the directors and co-directors of the TREC sites, in partnership with NCI scientists and administrative program staff, has been able to establish common goals of the initiative, exemplified by its mission statement: “….to integrate diverse disciplines to find effective interventions across the lifespan to reduce the burden of obesity and cancer and to improve population health.” (7)
The NCI transdisciplinary team science initiatives, including TREC, have allowed for the creation of scientific communities that have reshaped the way problems are conceptualized and approached, based on the development of deep collaboration of individuals across the transdisciplinary continuum. In addition to the transdisciplinary research occurring within each site, new scientific communities have been fostered. Each site was required to have an education training and outreach core to provide opportunities for professional development of TREC trainees, including pre- and post-docs, as well as junior faculty. TREC trainees receive mentoring in transdisciplinary science relevant to the initiative and are invited to participate in working groups and to apply for developmental pilot funds in collaboration with a more senior faculty mentor. More detail on the TREC approach to supporting career advancement for trainees is available elsewhere (8, 9).
Working groups were defined based on the shared interests of TREC members, and bring together scientists interested in similar issues (e.g., health disparities, biomarkers) for monthly conference calls. Frequent in-person scientific meetings are used to share updates on science within and beyond TREC. A coordinating center provides a support framework, enabling teams to focus on science rather than logistics. But perhaps the most important mechanism is the funding of the cross-TREC developmental pilot projects. During years 2 through 5, funding was available for up to 2 cross-TREC developmental pilot projects of approximately $30,000 per site. Theserojects required the inclusion of at least two scientific disciplines and at least two TREC sites (but up to 5, including the coordinating center) for science that was clearly transdisciplinary in scope. The TREC steering committee prioritized cross TREC developmental pilot funds toward transdisciplinary projects that would result in future funding. Below, we review examples of how TREC has allowed participating researchers and trainees to think differently about their science and positively influence the scope and quality of scientific discovery. Although over 10 examples were available from which to choose (See Table 1), the examples presented below were chosen because we believe that they best highlight unique features of TREC. Table 1 provides a summary of the focus of all of the Cross-Center Developmental pilot projects, including involvement of TREC trainees, disciplines involved, and the common processes used by each project to foster collaboration among researchers from disparate disciplines to work toward a common goal.
Table 1.
Summary of Cross-TREC Developmental Projects
| Project Title | TREC Trainee Involvement | Disciplines Involved | Common Processes Employed |
|---|---|---|---|
| Potential for exercise to attenuate increased risk for breast cancer due to delayed parity | Principal Investigators, with mentoring, AND co-investigators | Epidemiology, molecular biology, cancer biology, exercise physiology, biostatistics |
|
| In utero exposures and offspring risk of prostate cancer | Co-investigators | Epidemiology, cancer biology, obstetrics and gynecology, developmental biology, nutrition, biostatistics | |
| Conceptual model for developing new work on the influence of obesity on racial disparities in cancer outcomes | Co-investigators | Epidemiology, health disparities, social epidemiology, social work, nutrition, economics | |
| Inflammation as a mechanism for differences in breast cancer by race and obesity | Co-investigators | Epidemiology, pathology, social sciences, health disparities, immunology, oncology | |
| Transdisciplinary intersection of geospatial and social sciences | Principal Investigators, with mentoring AND co-investigators | Environmental epidemiology, sleep medicine, exercise physiology, built environment science, geography, computer science, biostatistics | |
| Obesity, C-peptide and Lethal Prostate Cancer | Co-investigators | Epidemiology, clinical urology, statistics | |
| Lipidomic Profiling of Energetics-Associated Cancer Models in Mice | Co-investigators | Lipidomic analyses, biostatistics, systems biology mapping | |
| Obesity Profiles and Breast Cancer | Co-investigators | Biostatistics, bioinformatics, epidemiology, cancer prevention | |
| DNA Methylation Response to Diet composition in Obese Insulin Resistant Women | Co-investigators | Statistical genetics, epigenetics, nutrition, energetics | |
| Obesity and Weight Loss in Endometrial Cancer Survivors: A Randomized, Multi-site Trial (Lifestyle Beyond Cancer Study) |
Co-investigators | Clinical oncology, biostatistics, epidemiology, exercise physiology, nutrition, cancer survivorship | |
| Leveraging the Power of TREC: Study of Cancer Recurrence/Mortality Risk Factors | Co-investigators | Biomarker analyses, statistics, epidemiology, clinical oncology, cancer survivorship | |
| Field Methods for Studying Circadian Misalignment in Relation to Cancer Risk | Epidemiology, environmental health, sleep medicine, biostatistics, social work |
The potential for exercise to attenuate the increased risk for breast cancer due to delayed parity
This project was funded as one of the one year cross-TREC developmental projects in the current round of funding (2011–2016). Earlier age at menarche and later age at first pregnancy are consistently associated with higher risk of breast cancer, (10–12) and evidence from epidemiology, reproductive epidemiology, and breast oncology suggests the interval between these two reproductive events has lengthened in recent years.(13–16) An interaction of breast cancer risk levels has been observed when examining the interval between menarche and first pregnancy and alcohol intake during this time period.(17) This supports the potential modifying effect of additional lifestyle factors on breast cancer risk. Identifying lifestyle interventions to mitigate the excess risk associated with a longer interval between menarche and first pregnancy, brings together the disciplines of exercise physiology, nutritional epidemiology, and developmental biology, and nutritional epidemiology, and would have global public health implications.
Convincing epidemiologic evidence exists associating moderate-to-vigorous intensity physical activity with a 10–25% lower risk of breast cancer, compared to inactivity.(18, 19) A similar benefit is observed in well-controlled animal models of experimentally-induced mammary carcinogenesis.(20, 21) However, we do not yet know whether physical activity can offset the risk of breast cancer associated with a longer interval between menarche and first pregnancy. One of the aims of this project is to analyze existing prospective data from 63,448 women in the Nurses’ Health Study II to evaluate the interaction between length of the interval between menarche and first pregnancy and physical activity on breast cancer risk, with detailed longitudinal information on diet, lifestyle and health-related outcomes. This analysis required the expertise of biostatistics, epidemiology, exercise physiology, gynecology, and cancer biology. A second aim of this study is to investigate a rat model of exercise and delayed parity by examining changes in the gene expression levels associated with early pregnancy induced protection against mammary tumorigenesis. The collaborative team’s development began when two post-doctoral fellows (an exercise physiologist and an epidemiologist) began discussions about this project at an in-person TREC meeting. They sought the mentorship of senior TREC faculty in biostatistics, cancer biology, and gynecology to shape their application for funding. Once awarded, they employed the common processes outlined in table 1 to successfully complete this transdisciplinary project.
Developmental origins of cancer: Effect of in utero exposures on offspring risk for prostate cancer
In our next example, a cross-TREC developmental study arose out of collaborations between scientists leading within-center projects at two of the TREC sites (Washington University and Harvard University). Using a rodent model, a Washington University project led by an obstetrican/gynecologist who specializes in murine modeling aims to identify whether exposing female mice throughout pregnancy to a high fat diet (HFD), is associated with epigenetic alterations of imprinted genes in prostate tissue at 8, 16, 26, 34 and 53 weeks postnatal. The lead investigator sought advice from a molecular biologist at Washington University to pursue the investigation. Loss of imprinting (LOI) in IGF2, one of the genes under investigation, has been implicated in breast and prostate carcinogenesis. The project, which added nutritional and other epidemiologists to its research team, will generate data on whether maternal diet can influence LOI in this gene throughout the lifetime. Yet, whether this mechanism applies to other common cancers and the extent to which the findings from this rodent model are translatable to humans are unknown. Therefore, a cross-TREC developmental project was funded to examine the generalizability of this molecular mechanism to breast cancer using a rodent model. In addition, another cross-TREC team is evaluating the translatability of the findings of these two rodent models to humans using data from a prenatal cohort. Specifically, this team, which now includes cancer biologists, molecular and nutritional epidemiologists, as well as a biostatistician, is examining whether 1) effects of HFD on the methylation of IGF2 and H19 in the mouse prostate are also observed in mouse white blood cells. (WUSTL center); 2) HFD is related to methylation of IGF2 and H19 in the mouse mammary fat pad and white blood cells (UCSD center); and 3) 2nd trimester human maternal fat intake (total fat intake and intake of major types of fat) is related to methylation of IGF2 and H19 in cord blood white blood cells (Harvard center).
Inflammation as a mechanism for differences in breast cancer by race and obesity
This activity was funded as a year 3 cross-TREC developmental project. Interest has grown in understanding the association of the tumor microenvironment with breast cancer severity. Under chronic inflammation, T lymphocytes, macrophages and neutrophils contribute to increased cell proliferation and inhibition of cell death, potentially advancing cancer. The presence of these immune cells in tumor samples may indicate aggressive tumors that are likely to metastasize. Obesity is a risk factor for postmenopausal breast cancer and reduced response to endocrine therapy that has been associated with chronic inflammation.(22–26) The majority of breast cancer tumors are estrogen receptor positive (ER+). Estrogen secreted from adipose tissue promotes ER+ tumor growth, making obesity a prominent factor in ER+ tumorigenesis.(27) African-Americans face a heightened risk of obesity and poor breast cancer outcomes, but the relationship between these disparities is not fully understood and it is unclear what mechanisms drive this association.(25, 28–33) Because it is unlikely that environmental differences account for all of the disparity observed in breast cancer outcomes, biological mechanisms that place groups at high risk for aggressive disease must be considered. Higher rates of obesity increase underlying inflammation and may be a mechanism that contributes to ER+ breast cancer disparities. This cross-TREC developmental project examines the contribution of obesity to inflammation in the tumor microenvironment, given that it may explain the racial disparity in ER+ breast cancer. Inflammation biomarkers in ER+ breast cancer tumors is being examined across a range of body mass indices (BMIs) in postmenopausal African-American and White women. The study hypothesizes that higher BMI increases the presence of lymphocytes, macrophages, and neutrophils within the ER+ breast tumor microenvironment and that race modifies the association of inflammation biomarkers with BMI in ER+ breast cancer tumors. The team is linking pathologic examinations of inflammation in tumor specimens to clinical data. The team has acquired breast cancer tissue from African-American and White post-menopausal patients at four TREC sites for this study. A pathologist at the University of Pennsylvania is examining existing formalin-fixed paraffin embedded breast tissues from each TREC site, using standardized protocols, for automated scoring of tumoral lymphocytes, macrophages and neutrophils, and noting type and number of these immune cells. The significance of this study is that factors affecting race differences in the tumor microenvironment of breast cancer patients evaluated by BMI have not been described. Complementing ongoing work in cancer inflammation and disparities, these researchers will link pathologic examinations of inflammation in breast tumor specimens to clinical and questionnaire data. The quantification of changes in the tumor microenvironment by BMI and race may provide tumor signatures to improve breast cancer prognostics. The long-term objective of this work is to identify ways to improve treatments for women at high risk for poor outcomes by modifying inflammatory markers in the tumor microenvironment via dietary and/or exercise interventions. If patients can be better classified in terms of risk for metastasis, treatments can be tailored to prevent over- or undertreatment of patients via adjuvant chemotherapy.(30)
Transdisciplinary intersection of geospatial and social sciences
The TREC Spatial and Contextual Methods and Measures Working Group established a series of cross-center developmental projects around the objective measurement of health behavior and the built environment. One study added state-of-the-science accelerometers and Global Positioning System (GPS) devices to a subsample of participants drawn from the four TREC sites. This provided additional behavioral and environmental data for each site and worked to advance the science of objective contextualized (behavior and location) assessment of physical activity, sedentary behavior, and sleep—behavioral and environmental exposures related to cancer risk. The exchange of ideas and experience across sites improved the capacity of each center to measure multiple behaviors in context and to apply this to larger cohorts.
A subsequent developmental project built on these data to advance the methods in this area. The aims of the project were to identify behavior measurement error due to four spatially-related factors (e.g. missing GPS data), and to assess the effects of these errors on outcome measurement of physical activity and sedentary behavior. The researchers developed a first of its kind, shared, HIPAA-compliant secure environment for processing massive GPS data sets with complex spatial layers that can expand based on processing demands. This forms a model for future collaborations.
The cross-center collaborations and the amount of resulting measurement data provide opportunities for advancing the science of behavior and contextual measurement. A third developmental project aims to will use existing accelerometry data to derive circadian rest-activity patterns, examine how these patterns are associated with demographic characteristics, and develop novel field methods for capturing the influence of environmental cues using a mobile application.
TREC Framework and Future Directions
The NCI has supported a network of five sites (4 research centers and a coordinating center) to facilitate new collaborative endeavors and addresses knowledge gaps. This network has a common understanding that the relationships between obesity, exercise, diet, and cancer outcomes is too complex to be addressed by a single scientific discipline. As such, the challenge includes bringing together scientists with widely differing methodologic training, and assumptions, toward the goal of answering ‘big’ questions. An infrastructural framework has been developed to assist these teams in developing functional working relationships and to foster a common understanding of the shared transdisciplinary goals of the initiative (34). The infrastructural framework developed out of the lessons learned from the first round of the initiative and includes the steering committee capacity, the coordinating center infrastructure, site specific capacity, and cross-center shared activities (Figure 1).
Figure 1.
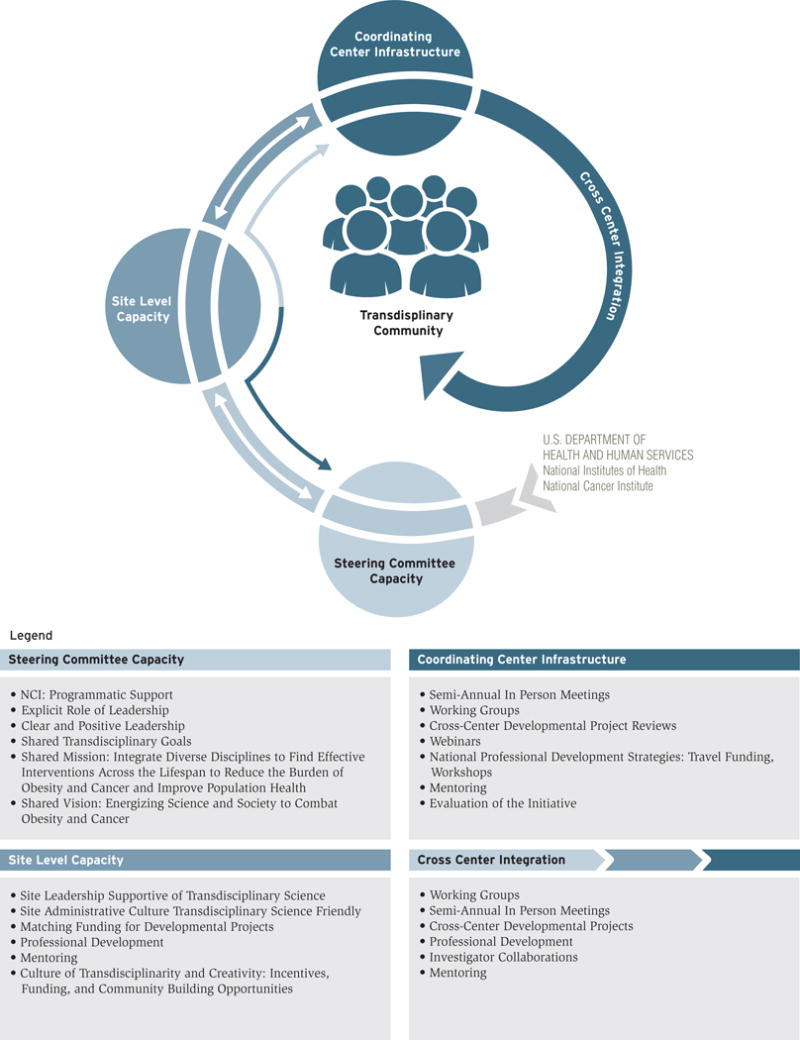
Conceptual Framework for Developing the TREC Transdisciplinary Research Community
The cross-TREC developmental projects reviewed herein demonstrate novel transdisciplinary work that integrates social, behavioral, and biological sciences to advance the pace of discovery. The formation of the TREC community has allowed participating researchers to take advantage of resources, expertise, and relevant methodologies or technologies not available at any one site and to minimize effort duplication and more efficiently use existing resources. The initiative has integrated public use assessment tools and methodologies, and to use and combine established data sets, patients/participants cohorts, and clinical centers or clinical care networks in a way that would not have been possible without the formation of the network and the developmental project funding. In addition, we have been able to extend our approach and findings to new cancer sites and to address important research questions not initially anticipated at the onset of funding, such as the intersection of obesity, cancer, and race/ethnicity.
TREC was able to include areas of TD building and management into its operations (35–39). Lessons learned in the first round of TREC have been particularly useful for this round of funding to move more quickly into transdisciplinarity (38). Building and sustaining the TD capacity in an organization is an ongoing challenge. Leadership at each site, and the individual site administrative leadership can encourage transdisciplinarity capacity. The way centers/sites/partners and steering committee organize themselves can facilitate leadership models that engage a transdisciplinary approach. The TREC Steering Committee worked together to tackle common team science/team building issues and identify common goals to be applied across the centers. We identified common transdisciplinary goals, as well as a common mission and vision. This translated into development of cross center research priorities and needs. We developed common resources to facilitate aspects of team development and education to facilitate cross-center collaborations. Finally, the Steering Committee incorporated a transdisciplinary leadership style to address issues related to decision making, problem solving, conflict resolution, information exchange, coordination, and boundary management. Essentially, the members of the TREC Steering Committee and the TREC Center’s individual leadership were able to glean from lessons learned from prior transdiciplinary center initiatives, as well as information from the science of building teams or/and transdisciplinary science literature, plus individual executive advisory groups, and incorporate aspects of leadership and management to effectively develop and maintain transdisciplinary collaborations within and across sites. TREC has had input from experts in the field of the Science of Team Science along the way, as well as the benefit of lessons learned from NCI initiatives that occurred before TREC 2. An additional consideration has been how the academic leadership within individual organizations embraced the ideas behind the TREC collaboration/centers and what type of in-kind support was offered. Based on experience, the most successful transdisciplinary centers have occurred when BOTH the initiative’s steering committee/leadership and the individual site’s academic leadership were supportive and took extra steps to facilitate the transdisciplinary approach. All of this was made possible by the U54 mechanism, and would have been difficult to capture with either a P01 or a U01 mechanism.
Conclusion
“Universities have departments, the real world has problems” (40). As illustrated by the examples given above, transdisciplinary research on energetics and cancer offers the promise of novel, wide-reaching and important discoveries. However, transcending the familiar boundaries of disciplinary silos poses considerable challenges. In transdisciplinary projects, misunderstandings and disagreement are more likely (41). Differences among scientists about the validity of each other’s conceptual frameworks, mismatches between rewards stressing disciplinary competence over innovation, and institutional disincentives can impede successful transdisciplinary endeavors (41). Success may also be elusive if transdisciplinary teams lack a common problem focus. Finally, the absence of processes for decision making, problem solving, conflict resolution, information exchange, coordination, and boundary management can be detrimental to collaboration (41).
The National Cancer Institute has been a leader in supporting transdisciplinary team science (35–39). In particular, the TREC initiative offers an efficient and effective framework to help scientists conduct transdisciplinary research on obesity and cancer and train new and established scientists to carry out this type of integrated research. The TREC initiative ensures that the research group has a common focus on using transdisciplinary science to address problems related to energetics and cancer. TREC’s governance structure provides formal and informal processes for information exchange and problem solving and ensures that critical cross-center and cross-discipline relationships are built on trust and mutual respect. Finally, as per the examples herein, the requirement to fund and conduct cross-center research projects brings together experienced and new researchers to engage in exciting, high-risk transdisciplinary projects.
In the modern era of greater focus on investigator initiated science, one challenge to extramural investigators and their NCI scientific colleagues will be to create new mechanisms that will allow transdisciplinary research to continue to flourish and grow. New approaches may be needed to ensure that the peer review process is not solely organized along disciplinary lines. Inclusion of expertise regarding transdisciplinarity, as well as representation from multiple scientific disciplines within a panel, may allow transdisciplinary research to receive an educated hearing. There are challenges ahead for transdisciplinary research, but they are welcome ones. The NCI intended to jump start a field and indeed it has: transdisciplinary research is here to stay.
Acknowledgments
Grant Support: This work was supported by the National Cancer Institute Centers for Transdisciplinary Research on Energetics and Cancer (TREC) (U01 CA116850 [Coordination Center], U54 CA155626 [Harvard University], U54 CA155435 [University of California, San Diego], U54 CA155850 [University of Pennsylvania], and U54 CA155496 [Washington University]).
Footnotes
Disclosure of Potential Conflicts of Interest: No potential conflicts of interest were disclosed.
References
- 1.Morgan GD, Kobus K, Gerlach KK, Neighbors C, Lerman C, Abrams DB, et al. Facilitating transdisciplinary research: the experience of the transdisciplinary tobacco use research centers. Nicotine Tob Res. 2003;5(Suppl 1):S11–9. doi: 10.1080/14622200310001625537. [DOI] [PubMed] [Google Scholar]
- 2.Warnecke RB, Oh A, Breen N, Gehlert S, Paskett E, Tucker KL, et al. Approaching health disparities from a population perspective: the National Institutes of Health Centers for Population Health and Health Disparities. Am J Public Health. 2008;98:1608–15. doi: 10.2105/AJPH.2006.102525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Patterson RE, Colditz GA, Hu FB, Schmitz KH, Ahima RS, Brownson RC, et al. The 2011–2016 Transdisciplinary Research on Energetics and Cancer (TREC) initiative: rationale and design. Cancer Causes Control. 2013;24:695–704. doi: 10.1007/s10552-013-0150-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hesse BW, Johnson LE, Davis KL. Extending the reach, effectiveness, and efficiency of communication: evidence from the centers of excellence in cancer communication research. Patient education and counseling. 2010;81(Suppl):S1–5. doi: 10.1016/j.pec.2010.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rosenfield PL. The potential of transdisciplinary research for sustaining and extending linkages between the health and social sciences. Soc Sci Med. 1992;35:1343–57. doi: 10.1016/0277-9536(92)90038-r. [DOI] [PubMed] [Google Scholar]
- 6.Emmons KM, Viswanath K, Colditz GA. The role of transdisciplinary collaboration in translating and disseminating health research: lessons learned and exemplars of success. Am J Prev Med. 2008;35:S204–10. doi: 10.1016/j.amepre.2008.05.009. [DOI] [PubMed] [Google Scholar]
- 7.Transdisciplinary Research on Energetics and Cancer (TREC) [homepage on the Internet] Seattle (WA): TREC Coordination Center, Fred Hutchison Cancer Research Center; [updated 2015 Nov 1; cited 2015 Oct 21]. Available from: www.trecscience.org. [Google Scholar]
- 8.Vogel AL, Feng A, Oh A, Hall KL, Stipelman BA, Stokols D, et al. Influence of a National Cancer Institute transdisciplinary research and training initiative on trainees’ transdisciplinary research competencies and scholarly productivity. Transl Behav Med. 2012;2:459–68. doi: 10.1007/s13142-012-0173-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Benesh EC, Gill J, Lamb LE, Moley KH. Maternal obesity, cage density, and age contribute to prostate hyperplasia in mice. Reprod Sci. 2015 Aug 4; doi: 10.1177/1933719115597767. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Colditz GA, Rosner B. Cumulative risk of breast cancer to age 70 years according to risk factor status: data from the Nurses’ Health Study. American journal of epidemiology. 2000;152:950–64. doi: 10.1093/aje/152.10.950. [DOI] [PubMed] [Google Scholar]
- 11.Pike MC, Krailo MD, Henderson BE, Casagrande JT, Hoel DG. ‘Hormonal’ risk factors, ‘breast tissue age’ and the age-incidence of breast cancer. Nature. 1983;303:767–70. doi: 10.1038/303767a0. [DOI] [PubMed] [Google Scholar]
- 12.Rosner B, Colditz GA. Nurses’ health study: log-incidence mathematical model of breast cancer incidence. Journal of the National Cancer Institute. 1996;88:359–64. doi: 10.1093/jnci/88.6.359. [DOI] [PubMed] [Google Scholar]
- 13.Yang XR, Sherman ME, Rimm DL, Lissowska J, Brinton LA, Peplonska B, et al. Differences in risk factors for breast cancer molecular subtypes in a population-based study. Cancer Epidemiol Biomarkers Prev. 2007;16:439–43. doi: 10.1158/1055-9965.EPI-06-0806. [DOI] [PubMed] [Google Scholar]
- 14.Ursin G, Bernstein L, Lord SJ, Karim R, Deapen D, Press MF, et al. Reproductive factors and subtypes of breast cancer defined by hormone receptor and histology. British journal of cancer. 2005;93:364–71. doi: 10.1038/sj.bjc.6602712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Colditz GA, Rosner BA, Chen WY, Holmes MD, Hankinson SE. Risk factors for breast cancer according to estrogen and progesterone receptor status. Journal of the National Cancer Institute. 2004;96:218–28. doi: 10.1093/jnci/djh025. [DOI] [PubMed] [Google Scholar]
- 16.Althuis MD, Fergenbaum JH, Garcia-Closas M, Brinton LA, Madigan MP, Sherman ME. Etiology of hormone receptor-defined breast cancer: a systematic review of the literature. Cancer Epidemiol Biomarkers Prev. 2004;13:1558–68. [PubMed] [Google Scholar]
- 17.Liu Y, Colditz GA, Rosner B, Berkey CS, Collins LC, Schnitt SJ, et al. Alcohol intake between menarche and first pregnancy: a prospective study of breast cancer risk. Journal of the National Cancer Institute. 2013;105:1571–8. doi: 10.1093/jnci/djt213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wu Y, Zhang D, Kang S. Physical activity and risk of breast cancer: a meta-analysis of prospective studies. Breast Cancer Research and Treatment. 2013;137:869–82. doi: 10.1007/s10549-012-2396-7. [DOI] [PubMed] [Google Scholar]
- 19.Neilson HK, Conroy SM, Friedenreich CM. The influence of energetic factors on biomarkers of postmenopausal breast cancer risk. Curr Nutr Rep. 2014;3:22–34. doi: 10.1007/s13668-013-0069-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Thompson HJ, Westerlind KC, Snedden J, Briggs S, Singh M. Exercise intensity dependent inhibition of 1-methyl-1-nitrosourea induced mammary carcinogenesis in female F-344 rats. Carcinogenesis. 1995;16:1783–6. doi: 10.1093/carcin/16.8.1783. [DOI] [PubMed] [Google Scholar]
- 21.Thompson HJ. Effects of physical activity and exercise on experimentally-induced mammary carcinogenesis. Breast Cancer Research and Treatment. 1997;46:135–41. doi: 10.1023/a:1005912527064. [DOI] [PubMed] [Google Scholar]
- 22.Field LA, Love B, Deyarmin B, Hooke JA, Shriver CD, Ellsworth RE. Identification of differentially expressed genes in breast tumors from African American compared with Caucasian women. Cancer. 2012;118:1334–44. doi: 10.1002/cncr.26405. [DOI] [PubMed] [Google Scholar]
- 23.Iaffaioli RV, Frasci G, Rinaldi L, Del Vecchio L, Tortoriello A, Facchini G, et al. Value of the CD25+ CD16+ cell determination in defining the prognosis of operable breast cancer patients. Eur J Gynaecol Oncol. 1993;14:412–8. [PubMed] [Google Scholar]
- 24.Martin DN, Boersma BJ, Yi M, Reimers M, Howe TM, Yfantis HG, et al. Differences in the tumor microenvironment between African-American and European-American breast cancer patients. PLoS One. 2009;4:e4531. doi: 10.1371/journal.pone.0004531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Morris GJ, Mitchell EP. Higher incidence of aggressive breast cancers in African-American women: a review. J Natl Med Assoc. 2008;100:698–702. doi: 10.1016/s0027-9684(15)31344-4. [DOI] [PubMed] [Google Scholar]
- 26.Baumgarten SC, Frasor J. Minireview: Inflammation: an instigator of more aggressive estrogen receptor (ER) positive breast cancers. Mol Endocrinol. 2012;26:360–71. doi: 10.1210/me.2011-1302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cleary MP, Grossmann ME. Minireview: Obesity and breast cancer: the estrogen connection. Endocrinology. 2009;150:2537–42. doi: 10.1210/en.2009-0070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wang Y, Beydoun MA. The obesity epidemic in the United States–gender, age, socioeconomic, racial/ethnic, and geographic characteristics: a systematic review and meta-regression analysis. Epidemiol Rev. 2007;29:6–28. doi: 10.1093/epirev/mxm007. [DOI] [PubMed] [Google Scholar]
- 29.Bruce MA, Sims M, Miller S, Elliott V, Ladipo M. One size fits all? Race, gender and body mass index among U.S. adults. J Natl Med Assoc. 2007;99:1152–8. [PMC free article] [PubMed] [Google Scholar]
- 30.Robinson WR, Gordon-Larsen P, Kaufman JS, Suchindran CM, Stevens J. The female-male disparity in obesity prevalence among black American young adults: contributions of sociodemographic characteristics of the childhood family. The American journal of clinical nutrition. 2009;89:1204–12. doi: 10.3945/ajcn.2007.25751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. JAMA. 2012;307:491–7. doi: 10.1001/jama.2012.39. [DOI] [PubMed] [Google Scholar]
- 32.Menashe I, Anderson WF, Jatoi I, Rosenberg PS. Underlying causes of the black-white racial disparity in breast cancer mortality: a population-based analysis. Journal of the National Cancer Institute. 2009;101:993–1000. doi: 10.1093/jnci/djp176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wright JL, Reis IM, Zhao W, Panoff JE, Takita C, Sujoy V, et al. Racial disparity in estrogen receptor positive breast cancer patients receiving trimodality therapy. Breast. 2012;21:276–83. doi: 10.1016/j.breast.2011.11.003. [DOI] [PubMed] [Google Scholar]
- 34.Gehlert S, Hall K, Vogel A, Hohl S, Hartman S, Nebeling L, et al. Advancing transdisciplinary research: the Transdisciplinary Research on Energetics and Cancer Initiative. J Transl Med Epidemiol. 2014;2:1032. [PMC free article] [PubMed] [Google Scholar]
- 35.Stokols D, Misra S, Moser RP, Hall KL, Taylor BK. The ecology of team science: understanding contextual influences on transdisciplinary collaboration. Am J Prev Med. 2008;35:S96–115. doi: 10.1016/j.amepre.2008.05.003. [DOI] [PubMed] [Google Scholar]
- 36.Stokols D, Hall KL, Taylor BK, Moser RP. The science of team science: overview of the field and introduction to the supplement. Am J Prev Med. 2008;35:S77–89. doi: 10.1016/j.amepre.2008.05.002. [DOI] [PubMed] [Google Scholar]
- 37.Hall KL, Feng AX, Moser RP, Stokols D, Taylor BK. Moving the science of team science forward: collaboration and creativity. Am J Prev Med. 2008;35:S243–9. doi: 10.1016/j.amepre.2008.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hall KL, Stokols D, Moser RP, Taylor BK, Thornquist MD, Nebeling LC, et al. The collaboration readiness of transdisciplinary research teams and centers findings from the National Cancer Institute’s TREC Year-One evaluation study. Am J Prev Med. 2008;35:S161–72. doi: 10.1016/j.amepre.2008.03.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Masse LC, Moser RP, Stokols D, Taylor BK, Marcus SE, Morgan GD, et al. Measuring collaboration and transdisciplinary integration in team science. Am J Prev Med. 2008;35:S151–60. doi: 10.1016/j.amepre.2008.05.020. [DOI] [PubMed] [Google Scholar]
- 40.Pohl C, Hirsch Hadorn G. Principles for designing transdisciplinary research Proposed by the Swiss Academies of Arts and Sciences. Munich: Oekom Verlag; 2007. [Google Scholar]
- 41.Gray B. Enhancing transdisciplinary research through collaborative leadership. Am J Prev Med. 2008;35:S124–32. doi: 10.1016/j.amepre.2008.03.037. [DOI] [PMC free article] [PubMed] [Google Scholar]