

Abstract
Injury of popliteal artery during total knee arthroplasty is a relatively rare complication. We report on one case of transverse semi-dissection of the popliteal artery during the tibial cut and one case of popliteal pseudoaneurysm formation caused by Hohmann retractors. Diagnosis was made early in the first case but it was delayed in the second due to misdiagnosis of deep vein thrombosis. Both injuries were managed eventually by open surgery. Postoperative clinical examination and ultrasound imaging confirmed the successful restoration of the blood flow. This case report also describes the classification system of the type of vascular damage and describes the mechanism, the clinical presentation, diagnostic modalities and treatment options for these rare complications of total knee arthroplasty surgery.
Keywords: Total knee arthroplasty, Complications, Popliteal artery tear, Pseudoaneurysm
Introduction
Vascular complications during total knee arthroplasty (TKA) are rare. Their incidence ranges from 0.003% to 0.23% [1], [2], [3], [4], [5], [6], [7], [8]. The importance of early diagnosis and management of these devastating complications is obvious, since mortality and amputation is 7% and 42%, respectively [9]. Previous conditions related to an increased risk of vascular complications include peripheral vascular disease, especially in patients with stent deployment, weight loss, renal failure, coagulopathy and metastatic cancer [1], [10]. The majority of vascular injury during TKA involves the popliteal artery. There are few studies describing injury to the geniculate arteries during TKA [11], [12]. Based on the anatomical damage and cause, vascular injuries can be classified as follows: 1) Occlusion. The cause of occlusion may be: i) Thrombosis due to vascular wall damage. Low blood flow as a result of tourniquet application is an additional factor for thrombosis. The damage can be caused by microtears, endothelial damage and stretching of the vessels during manipulations of the knee. The application of the tourniquet or the thermal injury by the cement may also lead to thrombosis. A rare cause of arterial occlusion is compression of the popliteal artery by the knee implant [13], ii) Embolization by calcified plates from another site, usually from the area where the tourniquet has been applied; 2) Popliteal artery sharp transection during the cuts; 3) Arteriovenous (A-V) fistula formation; 4) Aneurysm or more commonly pseudoaneurysm formation. The mechanism of pseudoaneurysm formation may be direct, as a result of a partial tear on the arterial wall, or indirect due to mechanical stretching or thermal injury from the cement [14], [15], [16]. Often, pseudoaneurysm can be misdiagnosed as deep vein thrombosis [7], [17], [18].
Clinical symptoms of vascular injury include: 1) Acute ischemic disorders such as pain, pallor, pulseless, paresthesia and paralysis. The causes of these disorders are usually tear or occlusion of the popliteal artery; 2) Localized edema or pulsatile mass due to A-V fistula, pseudoaneurysm or hematoma formation from a popliteal tear; 3) Recurrent hemarthrosis or hemorrhage from a vessel tear; 4) Bruits or thrill in cases of A-V fistula or pseudoaneurysm formation. Diagnosis is based on physical examination and confirmed by imaging studies. Diagnostic modalities include pulse oximetry, Doppler ultrasound, and angiography.
Vascular complications can be managed by open or endovascular means. Endovascular methods include: 1) Thrombectomy with a Fogarty catheter; 2) Angioplasty, usually with covered stents or balloon in cases of arterial tear and occlusion; 3) Coil embolization in case of pseudoaneurysm; 4) Pharmacomechanical thrombolysis. Open methods include: 1) Open thrombectomy; 2) Direct repair of the vessel (a vein or synthetic patch can be used) or excision of the damaged part followed by end-to-end anastomosis, in case of arterial tear or pseudoaneurysm; 3) Deployment of artery bypass or interposition graft 4) Above the knee amputation. Additionally, there are percutaneous methods of treatment, such as thrombin injection into the pseudoaneurysm. Staged treatment which include as a first step endovascular management has less morbidity and good results. The only absolute indication for open repair is active hemorrhage [19]. Patients after endovascular treatment need a long-term follow-up using Doppler assessment in order to identify any recurrent stenosis of the injured artery [20]. In this study we present two rare cases of vascular complications during TKA. Two patients presenting with popliteal pseudoaneurysm and popliteal tear, respectively, are reported.
Case histories
Case 1
The first patient was a 76-year old female who underwent a TKA in another institution. Her previous medical conditions included hypertension and hyperlipidemia. She had no previous history of predisposing factors for arterial complications such as peripheral arterial disease or diabetes. Immediately after surgery the patient started to complain for increasing pain at the popliteal area. This pain expanded some hours after the surgery, involving the lower limb distal to the knee. She was complaining of paresthesia especially in the anterior area of her tibia. Because of the aggravating character of her symptoms, a Doppler study assessment was performed which demonstrated a stoppage of the arterial flow at the popliteal area. On the first postoperative day an endovascular thrombectomy through the femoral artery with a Fogarty catheter was attempted, but her symptoms were not subsided. On the same day, the patient referred to our vascular surgery department. The patient was suffering from extreme pain in her lower limb, with concomitant paresthesia and weakness. Her limb was pale but pulsatile. Nail capillary refill test was very slow, sensation of light touch was disturbed and her toes were cooler in comparison to her other leg. The ankle brachial pressure index was 0.4. The patient had an emergent CT angiography, which revealed occlusion of the popliteal artery (Figure 1, Figure 2). The patient was scheduled for surgery immediately after the angiography. In the operating room, through a posterior popliteal incision the popliteal artery was exposed. A tear involving 3/4 of the popliteal artery diameter was found with an in situ thrombus inside the vessel. A Fogarty catheter was passed through the tear inside the artery distally and proximally and restored the blood flow. After restoration of the flow, the tear was sutured with a Prolene suture. Postoperatively, the patient had no signs of ischemia and a subsequent Doppler ultrasonography confirmed the undisturbed blood flow inside the popliteal artery without any leakage.
Figure 1.

CT angiography demonstrating occlusion of the popliteal artery due to thrombus formation above the level of the injury.
Figure 2.
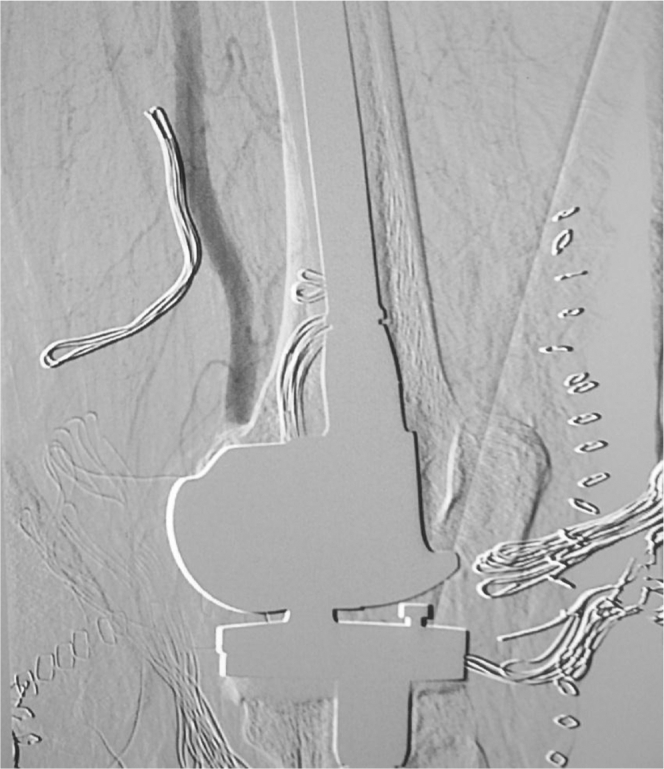
Oblique angiographic view of the thrombosed popliteal artery.
Case 2
The second case was a 76-year old female patient who underwent TKA (Fig. 3) in a nearby hospital. The patient had no previous history of atherosclerotic disease. The patient had no previous history of diabetes, ischemic heart disease or cerebrovascular problems. Also, there were no preoperative signs of peripheral vascular disease. On the third post-operative day, she felt a sharp pain at the popliteal and gastrocnemius area during her walking exercises. She also noticed a local edema and redness of the area. At that time, the patient was diagnosed with deep vein thrombosis by Doppler ultrasonography. The patient started on antithrombotic therapy with rivaroxaban. On the 40th postoperative day the local edema had partially subsided, but the pain remained at the same level. The patient presented to our emergency department and a vascular consultation was obtained. Physical examination revealed tenderness and a mass at the popliteal area, without any symptoms of ischemia. Peripheral pulses (pedal and posterior tibial) on her lower limb were palpable, there was no decrease of temperature but nail capillary refill test was slightly slower. Vascular Doppler study indicated arterial insufficiency with an ankle brachial pressure index of 0.7. Ultrasound scan demonstrated a mass of 12 × 9 cm at the popliteal area, indicative of a possible pseudoaneurysm (Fig. 4). A CT angiography confirmed the formation of popliteal artery pseudoaneurysm, which was pressing the nearby soft tissue (Fig. 5). Surgical exploration of the popliteal artery showed pseudoaneurysm measuring 9 cm. The sac of the pseudoaneurysm was opened, and fresh blood clots were removed. The neck of the pseudoaneurysm was located at the final part of the popliteal artery before its bifurcation. Three longitudinal tears were found, the longest at the anterior wall and two smaller at the posterior wall. The shape of the tears led to the conclusion that they were the result of retractor placement during anterior dislocation of the tibia. The two posterior tears were repaired with a 6-0 Prolene suture. The anterior tear was repaired with the aid of a great saphenous vein patch. Postoperatively, the patient was free of symptoms and an ultrasound scan confirmed the patency of the popliteal artery (Fig. 6).
Figure 3.

Lateral radiograph of the knee after total knee arthroplasty.
Figure 4.
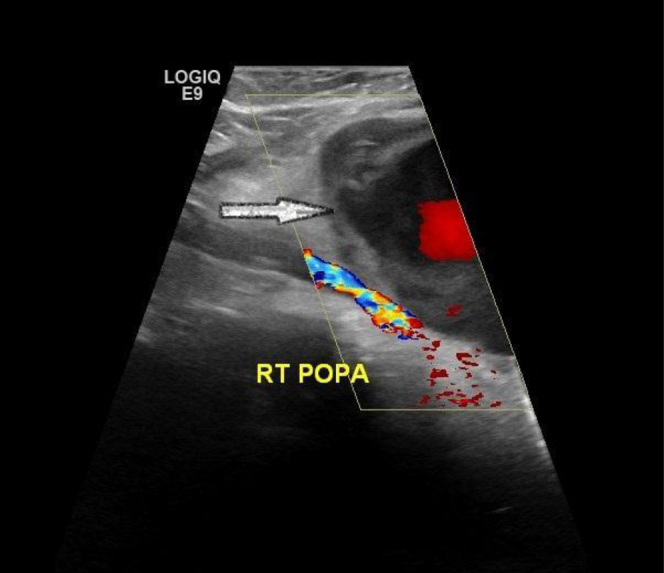
Color duplex scan image of popliteal artery. Arrow shows the pseudoaneurysm formation with arterial blood flow inside its cavity.
Figure 5.

3D CT angiography demonstrating pseudoaneurysm formation of the popliteal artery: a) lateral view, b) anteroposterior view, and c) oblique view.
Figure 6.

Postoperative color duplex scan showing restoration of arterial blood flow inside the popliteal artery.
Discussion
Most of postoperative vascular injuries are caused by tourniquet application which result in damage of calcified vessels leading to thrombosis or embolization of calcified plates [3]. Blunt trauma of the vessels is more often caused during manipulations, especially in the presence of extensive soft tissue contractures, as in posttraumatic fibrosis [21]. Although in a recent study of 32 postoperative vascular damages, 78% were the result of penetrating trauma, sharp damage to the popliteal artery is considered to be rare [22]. The incidence of above the knee amputation after vascular complications of TKA was higher in previous decades [2], [23]. The improvement of diagnostic modalities and endovascular techniques has decreased the possibility of this devastating procedure. Rubush described the danger zone for popliteal artery injury during tibial cuts or placement of the retractors. He compared the articular surface of tibia to a clock considering the 6 o'clock position as the most anterior position. The danger zone is between 11 and 3 o'clock (12 o'clock is the position of popliteal vein, 1 o'clock is the position of the popliteal artery and 2 o'clock is the position of the anterior tibial artery) [24]. The proximity of the popliteal artery to the posterior tibial surface renders it vulnerable to injury. The distance from the posterior tibial surface has been measured 0.96–3.15 mm during 0–90° of right knee flexion [25]. In another study this distance estimated to be 1 cm with the knee in extension, and 2 cm with the knee in hyperflexion [26]. Due to higher risk of vascular complications in patients with atherosclerotic disease, a complete vascular examination must be performed before surgery. In patients with concominant pathologies, vascular consultation should be done in order to be attained the best possible vascular status. Some authors recommend that in patients with ankle/brachial index <0.3 arthroplasty should be performed without the application of a tourniquet [27]. Parvizi et al. in a series of 11 vascular complications after TKA found that in 9 of them the popliteal artery was thrombosed due to an indirect mechanism. The main physical sign was absence of pulses. Almost all were diagnosed immediately postoperatively [10]. Cowell et al. published a case of popliteal pseudoaneurysm after TKA. It was managed by deployment of an angioplasty balloon across the neck pseudoaneurysm for 2 min, which resulted in thrombosis of the pseudoaneurysm [28]. In another study, Tejero-Garcia et al. presented a case of a popliteal pseudoaneurysm after unicompartmental arthroplasty which was managed by resection of the part of the popliteal artery with the pseudoaneurysm and subsequent end-to-end anastomosis with a saphenous vein graft [29]. Ibrahim et al. reported two cases of pseudoaneurysm of the popliteal and superior geniculate lateral artery. The popliteal pseudoaneurysm treated with injection of thrombin solution into its cavity. In the second case of superior geniculate lateral artery pseudoaneurysm, embolization using microcoils was performed [30].
There are 4 moments of TKA surgical procedure during which vessels, especially popliteal artery can be damaged: 1) at the tibial cut, 2) at the posterior cut of the femoral condyles, 3) during the application of retractor for anterior dislocation of the tibia, and 4) during placement of the knee in hyperextension after the cuts and before the application of the hardware [26], [31]. We presented two cases of sharp damage of popliteal artery during TKA. In the first case, popliteal artery semi-transected during tibial cut, while in the second case the artery was damaged by retractors placement during anterior dislocation of the tibia. The time of diagnosis of these complications was similar to other studies of the published literature. Popliteal semi-transection was diagnosed on the day of surgery, but pseudoaneurysm was diagnosed on the 40th postoperative day. This delay was due to misdiagnosis as deep vein thrombosis. Early diagnosis is essential since delayed diagnosis has been showed to be associated with a higher risk for amputations [32]. Prompt diagnosis depends on two things: clinical awareness of these complications and careful Doppler assessment. Clinical awareness includes assessment for signs of vascular insufficiency such as pallor, poor capillary refill and disturbed neurological status [33]. In our study, both cases were treated eventually by open surgical means, though in one case endovascular thrombectomy was initially performed without successful results.
Summary
Vascular pathology needs cautious preoperative, intraoperative and postoperative assessment. Preoperatively, clinical examination for detection of atherosclerotic disease or any other vascular problems is recommended, and patients with positive signs such as trophic changes of skin or venous guttering should be referred to a vascular surgeon [34]. Intraoperatively, great attention must be paid during the four mentioned moments of the procedure. Postoperatively, clinical awareness and careful Doppler examination are the keys to an early diagnosis of arterial injury.
Footnotes
No author associated with this paper has disclosed any potential or pertinent conflicts which may be perceived to have impending conflict with this work. For full disclosure statements refer to http://dx.doi.org/10.1016/j.artd.2015.06.001.
Appendix. Supplementary data
Conflict of Interest Statement 4.

Conflict of Interest Statement 5.

Conflict of Interest Statement 6.

References
- 1.Ko L., DeHart M., Yoo J., Huff T. Popliteal artery injury associated with total knee arthroplasty: trends, costs and risk factors. J Arthroplasty. 2014;29(6):1181. doi: 10.1016/j.arth.2014.01.007. [DOI] [PubMed] [Google Scholar]
- 2.Rand J. Vascular complications of total knee arthroplasty. J Arthroplasty. 1987;2(2):89. doi: 10.1016/s0883-5403(87)80014-1. [DOI] [PubMed] [Google Scholar]
- 3.Da Silva M., Sobel M. Popliteal vascular injury during total knee arthroplasty. J Surg Res. 2003;109(2):170. doi: 10.1016/s0022-4804(02)00088-4. [DOI] [PubMed] [Google Scholar]
- 4.Abularrage C., Weiswasser J., DeZee K. Predictors of lower extremity arterial injury after total knee or total hip arthroplasty. J Vasc Surg. 2008;47(4):803. doi: 10.1016/j.jvs.2007.11.067. [DOI] [PubMed] [Google Scholar]
- 5.Calligaro K., Dougherty M., Ryan S., Booth R. Acute arterial complications associated with total hip and knee arthroplasty. J Vasc Surg. 2003;38(6):1170. doi: 10.1016/s0741-5214(03)00918-2. [DOI] [PubMed] [Google Scholar]
- 6.DeLaurentis D., Levitsky K., Booth R. Arterial and ischemic aspects of total knee arthroplasty. Am J Surg. 1992;164(3):237. doi: 10.1016/s0002-9610(05)81078-5. [DOI] [PubMed] [Google Scholar]
- 7.Holmberg A., Milbrink J., Berqqvist D. Arterial complications after knee arthroplasty: 4 cases and a review of the literature. Acta Orthop. 1996;67(1):75. doi: 10.3109/17453679608995616. [DOI] [PubMed] [Google Scholar]
- 8.Pal A., Clarke J., Cameron A. Case series and literature review: popliteal artery injury following total knee replacement. Int J Surg. 2010;8(6):430. doi: 10.1016/j.ijsu.2010.04.008. [DOI] [PubMed] [Google Scholar]
- 9.Naresh Kumar S., Chapman J., Rawlins I. Vascular injuries in total knee arthroplasty. J Arthroplasty. 1998;13(2):211. doi: 10.1016/s0883-5403(98)90102-4. [DOI] [PubMed] [Google Scholar]
- 10.Parvizi J., Pulido L., Slenker N. Vascular injuries after total joint arthroplasty. J Arthroplasty. 2008;23(8):1115. doi: 10.1016/j.arth.2008.02.016. [DOI] [PubMed] [Google Scholar]
- 11.Julien T., Gravereaux E., Martin S. Superior medial geniculate artery pseudoaneurysm after primary total knee arthroplasty. J Arthroplasty. 2012;27(2):323.e13. doi: 10.1016/j.arth.2011.02.009. [DOI] [PubMed] [Google Scholar]
- 12.Gaheer R., Chirputkar K., Sarungi M. Spontaneous resolution of superior medial geniculate artery pseudoaneurysm following total knee arthroplasty. Knee. 2014;21(2):586. doi: 10.1016/j.knee.2012.10.021. [DOI] [PubMed] [Google Scholar]
- 13.Khan S. Popliteal artery occlusion after total knee replacement: a vascular team approach for limb salvage. Vasc Dis Manage. 2014;11(9) [Google Scholar]
- 14.Geertsema D., Defoort K., van Hellemondt G. Popliteal pseudoaneurysm after total knee arthroplasty. J Arthroplasty. 2012;27(8):1581.e1. doi: 10.1016/j.arth.2011.11.022. [DOI] [PubMed] [Google Scholar]
- 15.Saksena J., Platts A., Dowd G. Recurrent haemarthrosis following total knee replacement. Knee. 2010;17(1):7. doi: 10.1016/j.knee.2009.06.008. [DOI] [PubMed] [Google Scholar]
- 16.Sandoval E., Ortega F., García-Rayo M., Resines C. Popliteal pseudoaneurysm after total knee arthroplasty secondary to intraoperative arterial injury with a surgical pin. J Arthroplasty. 2008;23(8):1239.e7. doi: 10.1016/j.arth.2007.08.022. [DOI] [PubMed] [Google Scholar]
- 17.Choksey A., Noble J., Brown J., Marcuson R. Angiography in vascular problems with total knee replacement: a report of three cases. Knee. 1998;5(1):63. [Google Scholar]
- 18.O'Connor J., Stocks G., Crabtree J., Galasso P., Wallsh E. Popliteal pseudoaneurysm following total knee arthroplasty. J Arthroplasty. 1998;13(7):830. doi: 10.1016/s0883-5403(98)90039-0. [DOI] [PubMed] [Google Scholar]
- 19.Troutman D., Dougherty M., Spivack A., Calligaro K. Updated strategies to treat acute arterial complications associated with total knee and hip arthroplasty. J Vasc Surg. 2013;58(4):1037. doi: 10.1016/j.jvs.2013.04.035. [DOI] [PubMed] [Google Scholar]
- 20.Kovacs F., Pollock J., DeNunzio M. Endovascular stent graft repair of iatrogenic popliteal artery injuries – a report of 2 cases. Vasc Endovascular Surg. 2012;46(3):269. doi: 10.1177/1538574411434163. [DOI] [PubMed] [Google Scholar]
- 21.Kerens B., Boonen B., Schotanus M., Kort N. Popliteal lesion due to traction during unicompartmental knee revision surgery. J Orthop. 2013;10(1):38. doi: 10.1016/j.jor.2013.01.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bernhoff K., Rudstrom H., Gedeborg R., Bjorck M. Popliteal artery injury during knee replacement: a population-based nationwide study. Bone Joint J. 2013;95-B(12):1645. doi: 10.1302/0301-620X.95B12.31611. [DOI] [PubMed] [Google Scholar]
- 23.Hozack W., Cole P., Gardner R., Corces A. Popliteal aneurysm after total knee arthroplasty. J Arthroplasty. 1990;5(4):301. doi: 10.1016/s0883-5403(08)80087-3. [DOI] [PubMed] [Google Scholar]
- 24.Rubush H., Berger R., Britton C., Nettrour W., Seel M. Avoiding neurologic and vascular injuries with screw fixation of the tibial component in total knee arthroplasty. Clin Orthop Relat Res. 1993;(286):56. [PubMed] [Google Scholar]
- 25.Farrington W., Charnley G., Harries S. The position of the popliteal artery in the arthritic knee. J Arthroplasty. 1999;14(7):800. doi: 10.1016/s0883-5403(99)90028-1. [DOI] [PubMed] [Google Scholar]
- 26.Ninomiya J., Dean J., Goldberg V. Injury to the popliteal artery and its anatomic location in total knee arthroplasty. J Arthroplasty. 1999;14(7):803. doi: 10.1016/s0883-5403(99)90029-3. [DOI] [PubMed] [Google Scholar]
- 27.Langkamer V. Local vascular complications after knee replacement: a review with illustrative case reports. Knee. 2001;8(4):259. doi: 10.1016/s0968-0160(01)00103-x. [DOI] [PubMed] [Google Scholar]
- 28.Cowell G., Boom S., Ablett M. Thrombosis of popliteal artery pseudoaneurysm by deployment of angioplasty balloon after total knee arthroplasty. J Arthroplasty. 2009;24(5):825.e11. doi: 10.1016/j.arth.2008.07.018. [DOI] [PubMed] [Google Scholar]
- 29.Tejero-Garcia S., Criado J., Ast M., de Bobadilla G. Popliteal pseudoaneurysm after unicompartmental knee replacement: a case report. Knee. 2014;21(2):597. doi: 10.1016/j.knee.2013.03.003. [DOI] [PubMed] [Google Scholar]
- 30.Ibrahim M., Booth R., Clark T. Embolization of traumatic pseudoaneurysms after total knee arthroplasty. J Arthroplasty. 2004;19(1):123. doi: 10.1016/j.arth.2003.08.007. [DOI] [PubMed] [Google Scholar]
- 31.Krackow K. C.V. Mosby; St. Louis: 1990. Surgical procedure: the technique of total knee arthroplasty. [Google Scholar]
- 32.Wilson J., Miranda A., Johnson B. Vascular injuries associated with elective orthopedic procedures. Ann Vasc Surg. 2003;17(6):641. doi: 10.1007/s10016-003-0074-2. [DOI] [PubMed] [Google Scholar]
- 33.Smith D., McGraw R., Taylor D., Masri B. Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg. 2001;9(4):253. doi: 10.5435/00124635-200107000-00005. [DOI] [PubMed] [Google Scholar]
- 34.Butt U., Samuel R., Sahu A. Arterial injury in total knee arthroplasty. J Arthroplasty. 2010;25(8):1311. doi: 10.1016/j.arth.2010.05.018. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.