

Summary:
Diced cartilage graft wrapped in Surgicel or fascia has been widely reported in the literature. Pure diced cartilage graft without the use of a “sleeve,” on the contrary, is not as commonly reported. This could be due to concerns of graft dispersion, palpability, or visibility. In this case report, histologic findings of a pure diced cartilage graft placed 4½ years ago are reported. In addition, advantages and disadvantages of this technique are discussed in detail. Two pieces of the diced cartilage graft placed 4½ years prior were excised and sent for histologic analysis during a revision procedure. The microscopic examination reveals several small blocks of mature hyaline cartilage embedded in dense fibrous connective tissue with widely scattered small vascular channels. The cartilage is vital with scattered chondrocytes within their lacunae. Histology of the diced cartilage graft demonstrated viability and stability of the graft 4½ years after insertion. This case report also suggests that pure diced cartilage graft can provide reliable volume augmentation of nasal dorsum in cleft rhinoplasty.
Pure diced cartilage graft without the use of a tissue wrap has been widely used at our center for revision rhinoplasty to augment the nasal dorsum in cleft patients since 2003. In this case report, we present the histologic findings of a pure diced cartilage graft inserted 4½ years before biopsy. Advantages and disadvantages of this technique are also discussed.
CASE REPORT
This is a 36-year-old Asian woman with a history of complete cleft lip deformity on the left. This patient provided written consent for all photographs presented in this case report. She underwent revision rhinoplasty and diced cartilage graft for nasal dorsum augmentation and cheiloplasty in April 2010. In November 2014, she presented with a chief complaint of alar base asymmetry and uneven nostril height. Comparing her intraoperative photographs taken 4½ years apart, the diced cartilage graft along the nasal dorsum seems to maintain its shape and volume with minimal resorption. The patient, however, desired further augmentation around the radix, nasal dorsum, and increased tip projection in addition to a more symmetric alar base.
Procedures
We harvested the costal cartilage from the right eighth rib to replace the existing columellar strut and alar rim graft. The remaining harvested cartilage was then diced into 0.5- to 1-mm cubes to be used in radix and nasal dorsum augmentation. During elevation of the midline subcutaneous pocket, excess diced cartilage graft was encountered around the caudal portion of the nasal dorsum. The previously inserted diced cartilage graft is a conglomerate of diced cartilages surrounded by fibrous connective tissue, and it can be easily distinguished from the newly prepared diced cartilage or the underlying nasal cartilages based on its appearance and consistency. Two pieces of excess cartilage graft were excised to create space for insertion of the tuberculin syringe carrying the newly prepared diced cartilage to the radix. The excised cartilage graft was sent for histologic analysis (Fig. 1). A symmetric alar base with increased projection at the radix, nasal dorsum, and nasal tip was achieved.
Fig. 1.
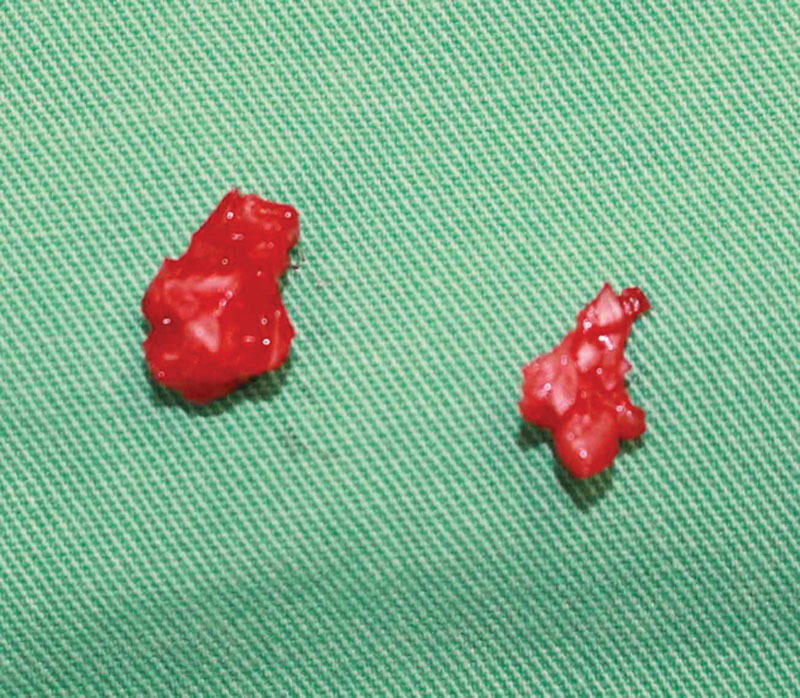
Gross specimens sent for histologic analysis. Clusters of diced cartilages were surrounded by connective tissue.
Histology
Two pieces of diced cartilage graft measuring 1.0 × 0.6 × 0.3 cm and 1.0 × 0.6 × 0.5 cm are submitted for histologic analysis. Hematoxylin and eosin staining of the submitted specimens is demonstrated in Figure 2. The microscopic examination reveals a mass of dense fibrous connective tissue with widely scattered small vascular channels. Embedded within the stroma are several small blocks of mature hyaline cartilage. The stroma is mature and demonstrates a very mild patchy lymphocytic infiltrate. The cartilage is vital as evidenced by the scattered chondrocytes within their lacunae (Fig. 2C).
Fig. 2.
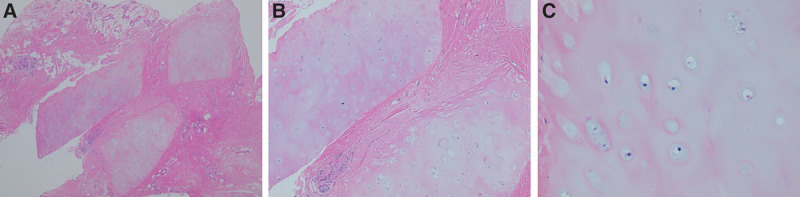
A, Blocks of mature hyaline cartilage embedded in dense fibrous connective tissue (hematoxylin and eosin stain; original magnification, 4×). B, Mature fibrous stroma with intermixed cartilage and a mild patchy lymphocytic infiltrate (hematoxylin and eosin stain; original magnification, 10×). C, Vital hyaline cartilage with scattered chondrocytes within their lacunae (hematoxylin and eosin stain; original magnification, 20×).
DISCUSSION
Histology of the diced cartilage graft demonstrated viability and stability of the graft 4½ years after insertion. Ingrowth of vascularized tissue with collagen deposition later occurred around the diced cartilage and helped achieve a solid fusion of the diced cartilage graft with connective tissue filling in the interstices. The viability of diced cartilage was compared with crushed or morselized cartilage graft in several animal studies. Diced cartilage has shown superior results with more viable chondrocytes compared with the other 2 methods of graft preparation.1–3 In our center, dicing the costal cartilage into 0.5- to 1-mm cubes while avoiding crush injury to the graft has been our standard protocol.
Some authors advocated the use of Surgicel (Ethicon, USA) to wrap the diced cartilage to prevent graft dispersion,4,5 whereas others have found extensive graft resorption with increased fibrosis due to foreign body reaction induced by Surgicel.6–8 Histologic findings of grossly reduced viability of the cartilage graft with decreased regeneration potential of the chondrocytes when Surgicel was used have been reported in several studies.2,6,8
Various types of autologous fascia such as rectus abdominis fascia,9 fascia lata from the lateral thigh,10 or temporal fascia7,11 have been used to wrap the diced cartilage for nasal dorsum augmentation. This, however, requires a separate incision and a longer operation time. It can also be associated with donor site morbidity. Daniel and Calvert12 advocate the use of temporal fascia sleeve filled with diced cartilage and insert the graft as a whole for nasal dorsum augmentation. Depending on the size of the fascia sleeve and the amount of diced cartilage it contains, insertion of the graft while maintaining the desired shape within the recipient pocket can be difficult. Very often, the lateral extent of the graft does not blend in with the nasal dorsum and resulted in a visible depression along the sides of the graft. Wrapping the diced cartilage with fascia also makes molding the diced cartilage graft to fill in small defect more difficult.
Some authors also advocate the use of esterified hyaluronic acid,8 amniotic membrane,13 autologous fibrin glue,14 or a combination of platelet-rich plasma (platelet gel) and platelet-poor plasma (fibrin glue)15 to prevent dispersion and enhance the viability of the graft. Although the results are promising, there are increased medical expenses and operation time associated with the use of these materials. The histologic findings of the pure diced cartilage graft without the use of wrapping material or tissue glue demonstrate the maintenance of structural integrity and viability of the graft over the long term.
This technique has its potential drawbacks including dorsal irregularity, migration of the diced cartilage, and visibility of the graft. In a retrospective study including 246 cleft patients who received diced cartilage graft at our center, the rate of dorsal irregularity and visibility of the graft was 8.5% and 1.2%, respectively.16 Intraoperatively, precise dissection of the subcutaneous pocket is performed to minimize graft migration. A thermoplastic stent is used to protect the graft for 7 days during the initial healing period. After stent removal, patients are instructed to apply manual massage to maintain the desired nasal shape. Dorsal irregularity or visibility of the graft can improve with manual massage up to 3 weeks postoperatively.
In conclusion, histologic findings from this case report confirmed viability of the graft with long-term stability. They also suggest that reproducible and aesthetic outcome of nasal dorsum augmentation can be achieved with this method.
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Kayabasoglu G, Ozbek E, Sahin F, et al. The comparison of the viability of crushed, morselized and diced cartilage grafts: a confocal microscopic study. Eur Arch Otorhinolaryngol. 2015;272:1135–1142. doi: 10.1007/s00405-014-3192-2. [DOI] [PubMed] [Google Scholar]
- 2.Yilmaz S, Erçöçen AR, Can Z, et al. Viability of diced, crushed cartilage grafts and the effects of Surgicel (oxidized regenerated cellulose) on cartilage grafts. Plast Reconstr Surg. 2001;108:1054–1060. doi: 10.1097/00006534-200109150-00040. discussion 1061. [DOI] [PubMed] [Google Scholar]
- 3.Cakmak O, Bircan S, Buyuklu F, et al. Viability of crushed and diced cartilage grafts: a study in rabbits. Arch Facial Plast Surg. 2005;7:21–26. doi: 10.1001/archfaci.7.1.21. [DOI] [PubMed] [Google Scholar]
- 4.Erol OO. The Turkish delight: a pliable graft for rhinoplasty. Plast Reconstr Surg. 2000;105:2229–2241. doi: 10.1097/00006534-200005000-00051. discussion 2242. [DOI] [PubMed] [Google Scholar]
- 5.Elahi MM, Jackson IT, Moreira-Gonzalez A, et al. Nasal augmentation with Surgicel-wrapped diced cartilage: a review of 67 consecutive cases. Plast Reconstr Surg. 2003;111:1309–1318. doi: 10.1097/01.PRS.0000047442.41691.C8. discussion 1319. [DOI] [PubMed] [Google Scholar]
- 6.Calvert JW, Brenner K, DaCosta-Iyer M, et al. Histological analysis of human diced cartilage grafts. Plast Reconstr Surg. 2006;118:230–236. doi: 10.1097/01.prs.0000220463.73865.78. [DOI] [PubMed] [Google Scholar]
- 7.Daniel RK. Diced cartilage grafts in rhinoplasty surgery: current techniques and applications. Plast Reconstr Surg. 2008;122:1883–1891. doi: 10.1097/PRS.0b013e31818d2104. [DOI] [PubMed] [Google Scholar]
- 8.Kazikdas KC, Ergur B, Tugyan K, et al. Viability of crushed and diced cartilage grafts wrapped in oxidized regenerated cellulose and esterified hyaluronic acid: an experimental study. Laryngoscope. 2007;117:1728–1734. doi: 10.1097/MLG.0b013e3180f62b36. [DOI] [PubMed] [Google Scholar]
- 9.Cerkes N, Basaran K. Diced cartilage grafts wrapped in rectus abdominis fascia for nasal dorsum augmentation. Plast Reconstr Surg. 2016;137:43–51. doi: 10.1097/PRS.0000000000001876. [DOI] [PubMed] [Google Scholar]
- 10.Baser B, Kothari S, Thakur M. Diced cartilage: an effective graft for post-traumatic and revision rhinoplasty. Indian J Otolaryngol Head Neck Surg. 2013;65(Suppl 2):356–359. doi: 10.1007/s12070-012-0525-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Calvert J, Brenner K. Autogenous dorsal reconstruction: maximizing the utility of diced cartilage and fascia. Semin Plast Surg. 2008;22:110–119. doi: 10.1055/s-2008-1063570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Daniel RK, Calvert JW. Diced cartilage grafts in rhinoplasty surgery. Plast Reconstr Surg. 2004;113:2156–2171. doi: 10.1097/01.prs.0000122544.87086.b9. [DOI] [PubMed] [Google Scholar]
- 13.Ozturk M, Aydin O. Use of diced cartilage grafts wrapped with amniotic membrane in soft tissue augmentation: experimental study. Ann Otol Rhinol Laryngol. 2013;122:66–70. doi: 10.1177/000348941312200112. [DOI] [PubMed] [Google Scholar]
- 14.Tasman AJ. Advances in nasal dorsal augmentation with diced cartilage. Curr Opin Otolaryngol Head Neck Surg. 2013;21:365–371. doi: 10.1097/MOO.0b013e3283627600. [DOI] [PubMed] [Google Scholar]
- 15.Bullocks JM, Echo A, Guerra G, et al. A novel autologous scaffold for diced-cartilage grafts in dorsal augmentation rhinoplasty. Aesthetic Plast Surg. 2011;35:569–579. doi: 10.1007/s00266-011-9725-9. [DOI] [PubMed] [Google Scholar]
- 16.Chang CS, Bergeron L, Chen PK. Diced cartilage rhinoplasty technique for cleft lip patients. Cleft Palate Craniofac J. 2011;48:663–669. doi: 10.1597/09-169. [DOI] [PubMed] [Google Scholar]