

Abstract
Background:
The knowledge about Ebola virus disease (EVD) is very crucial in the response to the recent outbreak and in order to control its spread. This study was conducted to assess the effectiveness of self-instructional module (SIM) in enhancing knowledge of EVD among Nigerian students in Bengaluru, India.
Materials and Methods:
A pre-experimental study design was employed, and a simple random sampling technique was used to select 60 participants. A pretest was conducted with the tool to assess the baseline knowledge of participants after which SIM was administered to all the participants in two episodes. The posttest was conducted after 7 days using the same tool to assess any gain in knowledge among the participants. Data were analyzed using SPSS at an alpha level of 0.001 and Descriptive analysis (such as percentage, frequency, mean and standard deviation [SD]) as well as independent t-test was conducted.
Results:
Findings showed that the majority of the participants (53%) were males, studying for the undergraduate degree (85%), 36 participants (60%) were in arts/social courses. More than average of the participants (67%) had spent only 1-year in India. Majority (53.3%) had average knowledge but after the administration of the SIM, majority had very good knowledge about EVD. The mean pretest knowledge score was 16.03 with an SD of 2.951 while the mean posttest knowledge score was 28.22 with SD of 3.273. The calculated t value was 21.432 (P < 0.001).
Conclusion:
SIM was observed to be very effective in this study and therefore should be adopted by health personnel in order to convey health-related information to the public.
Keywords: Ebola virus disease, effectiveness, Nigerian students, self-instructional module
INTRODUCTION
Ebola virus disease (EVD), formerly known as Ebola hemorrhagic fever is a very severe and often fatal illness in humans caused by Ebola virus.[1] The virus is usually transmitted to people from wild animals and spread across the human population through human-to-human transmission. There is currently an overwhelming concern in West Africa about the spread of EVD and the consequent health challenges and burden in the affected regions. EVD has a high fatality rate, and there is currently no treatment or vaccine with proven safety and efficacy for the disease.[2] This makes EVD a dreadful disease indeed.
Ebola virus disease is considered as a very dangerous disease majorly because it presents with sudden and diverse symptoms that could easily be mistaken with symptoms of other viral diseases. This has mounted serious challenge with early diagnosis.[3] EVD is characterized by febrile severe illness, with gastrointestinal manifestations of very high magnitude and is complicated by intravascular volume depletion, shock, electrolyte imbalance, and finally, organ failure.[4] The most unfortunate thing about EVD symptoms is that they are also easily mistaken for malaria, typhoid fever, dysentery, influenza, and various bacterial infections, all of which are prevalent in the Ebola stricken regions.[3] Ebola virus represent an illness that should warrant a substantial paradigm shift in the health care delivery and the public health personnel should be instrumental in making this happen by providing adequate information to the people about the causes, symptoms, mode of transmission, prevention and treatment of EVD.
Ebola virus is only transmitted by patients who are already presenting symptoms of the disease and by direct contact with blood or body fluid of an Ebola patient.[2] It is therefore very crucial to equip the masses with relevant information concerning this dangerous disease.
Improving the knowledge about EVD is very important in order to curtail its further transmission across borders. Researchers have identified a lack of knowledge among other issues as a serious challenge in the response to EVD outbreak.[5] Therefore, understanding the unending risk of transmission resurgence is essential in implementing rapid and effective response.
A Harvard School of Public Health/SSRS poll found that people with less knowledge and education about EVD are more concerned about an outbreak and are also more concerned that they or their families will get sick. The same study also reported that those with less knowledge and education are less likely to be following the news about Ebola outbreak in West Africa closely.[6] Nigerians in Diaspora have particularly been concerned with measures to eradicate EVD from their beloved nation. Many Nigerians are currently in India for educational or business purposes. Nigeria has a broad bilateral tie and favorable diplomatic relationship with India. Till date, there has been no published study on the level of knowledge about EVD among Nigerians in Diaspora. There have been instances where few Nigerians were subjected to quarantine in India because they presented EVD-like symptoms. Till recent times, there has not been any confirmed case of EVD in India. As a result, the knowledge of EVD may not have been well-established among Nigerians currently residing in India.
Various teaching and educational methods have been adopted and found effective by researchers in disseminating health related information to improve peoples’ knowledge about certain health issues. A study conducted in Delhi, India reported that information, education and communication programme was effective in enhancing the knowledge of mothers on prevention and management of warning signs during pregnancy.[7]
Structured teaching program was also adopted in another study conducted in India and was reported to be highly effective in improving knowledge and opinions of Nursing students toward prevention of mental retardation.[8] Several health education programs, including health coaching programs,[9] are effective in motivating and assisting people to change unfavorable health behaviors.
Ebola disease is the current health concern among Africans and Nigerians specifically. Adequate awareness has been advocated to curb and control the outbreak. International federation of the red cross and red crescent societies recently published that knowledge of EVD and mode of transmission is limited within the affected population and there are rumors and misconceptions regarding the mode of transmission as well as denial that it exists.[10] It is therefore advocated that there is a need to scale up social mobilization and awareness raising with different strategies employed to reach everybody. The self-instructional module (SIM) represents a distinct advance over traditional methods of enhancing peoples’ knowledge on health related issues. It makes learning a process of active seeking rather than passive absorbing. This present study, therefore, sets out to assess the effectiveness of SIM in enhancing knowledge about EVD among Nigerian students in Bengaluru, India.
MATERIALS AND METHODS
A pre-experimental design (one group pretest posttest design) was employed to explore the effectiveness of SIM in improving knowledge about EVD among Nigerian students in Bengaluru, India. The study population included all Nigerian students studying in different colleges in Bengaluru. The exclusive criterion was unwillingness to participate in the study. A simple random sampling technique (Ballot method) was used to select 60 participants during a congregation held by the Community of Nigerian and Nigerian students in Bengaluru in preparation for the activities of the forthcoming Nigerian Independence celebration on October 1, 2014. The research instruments were SIM and a structured questionnaire which were developed based on the literature review, conceptual framework and experts’ opinions. The SIM used for this study was a 28 page printed material which consisted of detailed information on EVD with some colorful pictorial illustrations. This material, which is sequentially arranged units of instructions, is self-paced to allow the participants to be independent in the learning process. A proposal of the study was submitted to the organizing committee who granted the permission to conduct this study. Participants were given a full explanation regarding the objectives of the study and measures of confidentiality. Participants willingly gave their consents. The SIM took a period of 7 days and was conducted in two episodes. The first episode consisted of causes, risk factors, and signs and symptoms of EVD while the second episode consisted of diagnosis, treatment, prevention, and control of the disease on the 1st day, a pretest was conducted with the tool to assess the baseline knowledge of participants after which the first episode of the SIM was administered to all the participants. The participants were allowed to study the material and understand the content after which the SIM was retrieved. The second episode was administered on the 2nd day. Participants were asked to study the whole materials until the 7th day. On the 7th day, a posttest was conducted using the same tool to assess any gain in knowledge among the participants. The structured questionnaire consisted of two parts. Part A was on socio-demographic information of participants which included their gender, educational level, area of study, duration of stay in India, previous knowledge of EVD and source of information. Part B consisted of knowledge question regarding Ebola disease. Part B was subdivided into five sections which consisted of 33 structured knowledge questions. Eight questions on causes and risk factors, seven questions on signs and symptoms, five questions on diagnosis and diagnostic tests, five questions on treatment, and eight questions on prevention and control. Each of the questions had four options comprising of one correct option and three distracters. A score of 1 was assigned to each correct option, and 0 was assigned to incorrect options selected by the participants. The overall score was used to judged participants knowledge level as very good (80–100%), good (60–79%), average (50–59%) poor (30–49%), and very poor (below 30%) A pilot study was conducted with six people who were not included in the main study. Reliability of the tool was ascertained by conducting a split half test using Spearman–Brown's prophecy formula which yielded 0.96.
Data were analyzed using SPSS [17.0 IL, Chicago, USA] at an alpha level of 0.001. Descriptive analysis (such as percentage, frequency, mean and standard deviation [SD]) as well as independent t-test was conducted.
RESULTS
There was a 100% response rate in this study. As shown in Table 1, majority of the participants (53%) were males studying for the undergraduate degree (85%). 36 participants (60%) were in arts/social courses. More than average of the participants (67%) have spent only 1-year in India. All participants (100%) had previous knowledge of EVD while majority of the participants (73.4%) got the information through media/social networks. Medical professionals are not the only ones providing health and medical information to the population. A study reported that use of print media and interpersonal sources of health information are most consistently associated with self-reported health behaviors.[11]
Table 1.
Frequency distribution table of demographic data of participants (n=60)
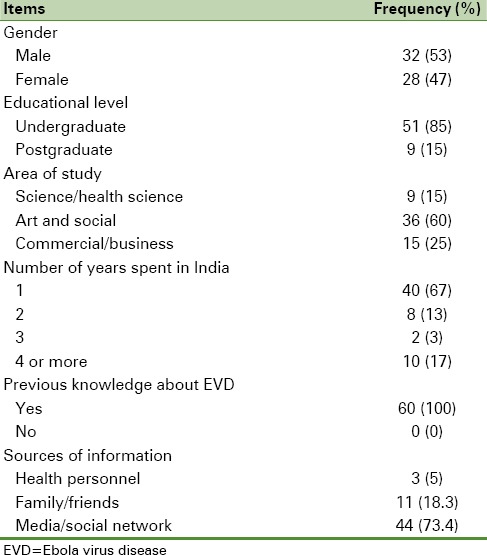
Before the intervention was conducted, 32 participants (53.3%) had average knowledge, 26 participants (43.3%) had good knowledge, and only two participants (3.3%) had poor knowledge but after the administration of the SIM, 43 (71.7%) had very good knowledge and 17 participants (28.3%) had good knowledge about EVD.
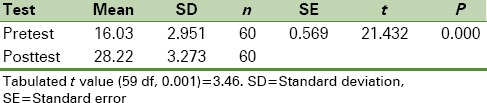
As shown in Table 2, the mean pretest knowledge score was 16.03 with an SD of 2.951 while the mean posttest knowledge score was 28.22 with SD of 3.273. The calculated t value was 21.432 with a standard error of 0.569 (P < 0.001).
Table 2.
Difference in pretest and posttest knowledge scores
DISCUSSION
Findings from this study revealed that all the participants indicated that they had a previous knowledge of EVD. Notably, majority (73.4%) got the information through social media while only very few (5%) got the information from health personnel. This is in line with several studies that reported that social network is very influential in disseminating health information.[10,12] This implies that online social networking sites offer a novel setting for the delivery of health promotion interventions due to their potential to reach a large population and the possibility for two-way engagement.
It was observed from the findings of this study that participants had relatively low levels of baseline knowledge of EVD compared to what is expected since Nigeria is currently facing the outbreak. This is also similar to the report of International Federation of Red cross and Red Crescent Societies stating that Liberian citizens have limited knowledge regarding the mode of transmission of the Ebola virus.[13] After the administration of the SIM, majority of the participants gain very good knowledge about EVD. Similarly, findings from the study revealed that the mean pretest knowledge of participants was 16.03 (±2.951), and the mean posttest knowledge score was 28.22 (±3.273). The calculated t value was 21.432 as against the tabulated t value of 3.46 (P < 0.001). This shows that there is a significant difference between the pretest and posttest knowledge scores. Therefore, we conclude that SIM is effective in enhancing the knowledge of Nigerian students in Bengaluru about EVD. This method was also reported effective in a study conducted to assess the effect of a SIM on the child-rearing knowledge and child rearing practice of women with epilepsy and developmental outcome of their babies.[14] Various educational modules are been adopted by public health professional to improve the knowledge and health-related behaviors among the population. Even in psychiatry, an educational module have been reported to be effective in improving the knowledge of primary school teachers regarding early symptoms of childhood psychiatric disorders.[15] In a study conducted to evaluate the effect of an instructional module on patient self-management for undergraduate pharmacy students in an Australian university, it was reported that completion of a comprehensive module on patient self-management increased undergraduate pharmacy students’ understanding and knowledge of patients experiencing chronic pain and it was recommended that the module could be implemented across other healthcare disciplines.[16] SIM are not only useful to nonhealth personnel, it can also be adopted in improving the knowledge and understanding of health workers about some health related concerns. It has been reported that SIM is very effective in increasing the skills of general practitioners in diagnosing melanocytic lesions and skin cancer.[17] Patients understanding about the procedures, they are been scheduled to undergo is very essential. It is the duty of the nurse or primary health provider to ensure adequate understanding among patients. A study reported that SIM was effective in improving the knowledge of cardiac angiography among patients undergoing cardiac angiography in a selected hospital in India.[11] The findings of this study corroborate with findings from a number of other studies which have reported a significant increase in participants’ knowledge after the administration of the SIM.[18] The findings of this study revealed a significance increase in the posttest knowledge scores after the administration of SIM. Therefore, it is confirmed that SIM is an effective teaching strategy.
Limitations
This study was limited by the small sample size selected which is a small group of all Nigerian students currently studying in Bengaluru. Moreover, conducting a study on small sample size reduces the generalizability of the findings. It is therefore suggested that similar studies should be conducted among larger sample size and in other settings.
CONCLUSION AND RECOMMENDATION
This study has revealed that despite poor baseline knowledge about EVD in relation to its causes, risk factors, mode of transmission, diagnostic procedures, treatment, prevention, and control, Nigerian students in Bengaluru gained adequate knowledge and understanding after the administration of SIM. This is a proven method that can be adopted by different public health workers in order to enhance their health education activities. SIM is easy to administer if the content has been well-drafted based on the desired information. It is therefore recommended that this method should be emphasized in educational institutions where health workers are trained and to incorporate this in their training so that the student would gain proficiency in administering this teaching method during their carriers. This study should be replicated across different groups of people to really ascertain its effectiveness among different groups. Nurses and doctors could effectively teach their patient regarding different medical procedures and treatments with the use of SIM. It should be designed to suit the educational level of clients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
My sincere gratitude goes to all the participants who willingly devoted their time and energy. I would also like to thank Mrs. P.E Ahuchuba for her love and support. I will not fail to acknowledge all the experts who validated the content of the tool.
REFERENCES
- 1.World Health Organization. Fact Sheet No. 103. 2014. [Last accessed on 2014 Sep 04]. Available from: http://www.who.int/mediacentre/factsheets/fs103/en .
- 2.Ki M. What do we really fear.The epidemiological characteristics of Ebola and our preparedness? Epidemiol Health. 2014;36:e2014014. doi: 10.4178/epih/e2014014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.CDC Special Pathogens Branch. Ebola Hemorrhagic Fever Case and Location List. Ebola Hemorrhagic Fever Information Packet. 2010 [Google Scholar]
- 4.Fowler RA, Fletcher T, Fischer WA, nd, Lamontagne F, Jacob S, Brett-Major D, et al. Caring for critically ill patients with Ebola virus disease. Perspectives from West Africa. Am J Respir Crit Care Med. 2014;190:733–7. doi: 10.1164/rccm.201408-1514CP. [DOI] [PubMed] [Google Scholar]
- 5.Tambo E, Ugwu EC, Ngogang JY. Need of surveillance response systems to combat Ebola outbreaks and other emerging infectious diseases in African countries. Infect Dis Poverty. 2014;3:29. doi: 10.1186/2049-9957-3-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Harvard School of Public Health. “Many in US Lack Knowledge About Ebola, Its Transmission, Poll Finds” ScienceDaily ScienceDaily; 22 August, 2014. [Last accessed on 2014 Sep 02]. Available from: http://www.sciencedaily.com/releases/2014/08/140822094238.htm .
- 7.Takoo S, Chhugani M, Sharma V. Effect of information education and communication (IEC) programme on knowledge of pregnant mothers regarding prevention and management of warning signs during pregnancy. Nurs J India. 2013;104:284–8. [PubMed] [Google Scholar]
- 8.Moharana K. Effect of structured teaching programme on the knowledge and opinion of nursing students towards prevention of mental retardation. Nurs J India. 2013;104:134–7. [PubMed] [Google Scholar]
- 9.Neuner-Jehle S, Schmid M, Grüninger U. The “Health Coaching” programme: A new patient-centred and visually supported approach for health behaviour change in primary care. BMC Fam Pract. 2013;14:100. doi: 10.1186/1471-2296-14-100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hamm MP, Shulhan J, Williams G, Milne A, Scott SD, Hartling L. A systematic review of the use and effectiveness of social media in child health. BMC Pediatr. 2014;14:138. doi: 10.1186/1471-2431-14-138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Catherine T. Self instructional module and cardiac angiography. Effectiveness of self instructional module on cardiac angiography for patients undergoing cardiac angiography in a selected hospital. Nurs J India. 2005;96:132–3. [PubMed] [Google Scholar]
- 12.Korda H, Itani Z. Harnessing social media for health promotion and behavior change. Health Promot Pract. 2013;14:15–23. doi: 10.1177/1524839911405850. [DOI] [PubMed] [Google Scholar]
- 13.International Federation of Red Cross and Red Crescent Societies. Emergency Plan of Action (EPoA) Liberia: Ebola Virus Disease; April, 2014 [Google Scholar]
- 14.Saramma PP, Sarma PS, Thomas SV. Effect of a self-instructional module on the child rearing knowledge and practice of women with epilepsy. Seizure. 2014;23:424–8. doi: 10.1016/j.seizure.2014.02.006. [DOI] [PubMed] [Google Scholar]
- 15.Daniel LT, Gupta S, Sagar R. Effect of educational module on knowledge of primary school teachers regarding early symptoms of childhood psychiatric disorders. Indian J Psychol Med. 2013;35:368–72. doi: 10.4103/0253-7176.122228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Smith L, Brown L, Bundy A, Ronaldson S, McKenzie H, Lewis P, et al. A learning and teaching resource on patient self-management of chronic pain. Am J Pharm Educ. 2013;77:35. doi: 10.5688/ajpe77235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Youl PH, Raasch BA, Janda M, Aitken JF. The effect of an educational programme to improve the skills of general practitioners in diagnosing melanocytic/pigmented lesions. Clin Exp Dermatol. 2007;32:365–70. doi: 10.1111/j.1365-2230.2007.02414.x. [DOI] [PubMed] [Google Scholar]
- 18.Verma P. Impact of self-instructional module for the nurses on nursing-management of the patients having chest tube drainage. Nurs J India. 2003;94:33–4. [PubMed] [Google Scholar]