

Abstract
Background and Objectives:
Congestive heart failure is one of the most common cardiovascular diseases that have a progressive and chronic trend and influences individuals’ and their families’ various dimensions. Social support is one of the psychosocial factors that can have a positive effect on individuals’ physical, mental and social status. Despite the existence of evidences, revealing the importance of family's support on patients’ condition, family centered supportive interventions with goal of clinical outcomes improvement have been less conducted among these patients. Therefore, the present study aimed to investigate the effect of family supportive intervention on the level of the support, received among heart failure patients.
Materials and Methods:
This is a two-group two-stage clinical trial, conducted on 64 patients with cardiac failure, referring to selected educational centers and meeting the inclusion criteria, who were selected through convenient sampling. They were assigned to study (n = 32) and control (n = 32) groups through random allocation. Data were collected by questioning through a two-section medical records questionnaire and were analyzed by SPSS.
Results:
Results of the study showed that mean scores of received support score were 13.7 (3.8) in the study and 0.8 (2.4) in the control group. Independent t-test showed a significant difference in mean changes of perceived support scores after the intervention between study and control groups (P < 0.001).
Conclusions:
Based on familial dimension in social support have a positive effect on patients’ perceived support. Nurses, as professional members of health care team, and with an important role in education and care of cardiac failure patients, can support, educate and guide these patients through designing appropriate care plans and educating their family members.
Keywords: Congestive heart failure, family oriented program, Iran, social support
INTRODUCTION
Congestive Heart failure (CHF) is one of the most common cardiovascular diseases, which have a progressive and chronic trend.[1] This disease is very disabling and costly in such a way that 70% of the involved patients are re-hospitalized within the first 3 months after their discharge.[2] In this way, a high amount of health care system resources are wasted on this disease. The patients’ hospitalization annual burden is estimated 130 million dollars in Iran.[3] Treatment of CHF is very sophisticated, and in most of the cases, it is administrated with goal of survival increase, reduction of hospitalizations and improvement of quality of life (QOL).[4] Therefore, the patients should be encouraged to have self-care behavior such as obedience from a strict medication order and diet, and generally, a diet therapy, to achieve this goal.[5] Despite this, the research results showed that at least 50% of the patients do not follow treatment program that leads to their re-hospitalization.[6] Therefore, different interventions and educational programs have been suggested to modify and change patients’ health behavior. Meanwhile, researches showed that various social factors in patients’ life have a high influence on their level of obedience from the recommendations in long-term treatment programs, especially when long-term changes in patients’ life style and behavior are needed.[7] Social support is one of the psycho-social factors, known as a facilitator for health behavior modification,[8] which refers to the care, attention and help, given to the patients by other individuals or groups.[7] Social support is counted as an important factor in patients’ recovery[8] since it can prevent incidence of unwanted physiological complications in the patients, increase their self-confidence and have a positive effect on their physical, psychological and social conditions.[9] Cassel is among the first theoreticians who introduced the concept of social support and stated that social support can improve human's health.[10] Numerous studies showed a direct association between perceived social support and high level of patients’ obedience from treatment and diet therapy.[8,11,12,13] Some scholars believe that social support is beneficial for human's health and vice-versa. Based on this theory, the more the social support is, the healthier the individuals will be. Therefore, being healthy is influenced by the level of social support.[14] Family is considered as one of the most important sources for social support, especially for the patients.[15] Family often plays a pivotal role in helping the patients in controlling and treating a disease. Familial support leads to health improvement and is counted as a major factor in fighting against a disease.[16] Beliefs and attitudes about physical, emotional and psychological health, and the behaviors affecting health such as nutrition, sport and stress management are learned and empowered in the atmosphere of the family. In fact, the family is the main health care provider for its members. On the other hand, paying attention to the family and its members’ participation in taking care of the other members has increased through care plans and other budget management programs. It is in such a way that consideration of cost efficacy of care has driven hospital care to home care. In this regard, family, and especially home caregivers, play a vital role in patients’ health and well-being, and, in fact, are considered as the hidden health care providers.[17] Studies on CHF patients have reported a positive association between family support and these patients’ obedience from self-care behaviors. Gallagher et al. showed that the patients with higher perceived support had better obedience from self-care behaviors such as limitation in fluid intake, regular medication, having physical exercises and referring to a physician in case of being overweight.[18] Sayers et al. reported a notable and positive association between perceived support and obedience from medication and food diets, as well as other aspects of self-care in heart failure patients.[19] Although the conducted research showed a positive association between types of social support, given from the side of the family, and components of health including improvement of self-care behavior, most of them do not know what care is beneficial for their patients or how their patients should be encouraged and supported to have self-care behavior.[20] Families can take appropriate supportive actions and seek positive and constructive coping mechanisms as well as some techniques such as increasing the right of selection, self-control domination, personal selection, expression of sympathy, participation and feel of belonging and a companionship toward the individuals to improve their patients’ support.[21] Unfortunately, despite the existence of evidences on the importance of family support in clinical outcomes and self-care in heart failure patients, fewer family centered studies have been conducted on these patients to improve such clinical outcomes. Meanwhile, as nursing is a profession in the field of health, and with regard to its crucial role in support, education and care of these patients and their caregivers,[22] it is potential to design appropriate care plans through educating the family members concerning supporting, educating and guiding these patients, and taking effective steps in improvement of their self-care behavior. Designing administration, evaluation and application of such programs and educational and supportive interventions can reveal the important role of the nurses in promotion of patients’, their families’ and consequently, society's health behaviors and self-care. Therefore, the present study aimed to investigate the effect of family supportive intervention on the level of the support, perceived among heart failure patients.
MATERIALS AND METHODS
This is a two-group two-stage clinical trial, conducted in Isfahan, Iran in 2011 (No. 390458). The effect of the independent variable of family centered support on the dependent variable of perceived support was investigated in CHF patients. Subjects were selected from the CHF patients who are referring to four selected educational hospitals university. The inclusion criteria were being in heart failure classes 2, 3 or 4, based on classification of American Heart Association, being involved in CHF at least for 1-year, being conscious and able to make communication, age over 21 years and absence of any other additional chronic and progressive diseases, the diseases acting as a risk factor for cardiac diseases (hypertension, diabetes, hyperlipidemia), having a family, and not living alone. The caregivers were a member of patients’ family who had the highest participation in patients’ care and were aged over 18 years, had reading and writing literacy, and were interested in attending the study. Through Dunbar et al.[23] and Piette et al.[24] and with consideration of confidence level of 95% and power of 80%, 64 heart failure patients referring to university clinics and meeting the inclusion criteria were selected through convenient sampling. Then, by random numbers table, they were assigned to two groups of study and control (n = 32, n = 32). After subjects’ random allocation to study and control groups, their caregivers were also assigned to the same groups. Sampling lasted for 4 months to reach the target sample size (January 2012 to May 2012).
Data were collected by questioning and with the help of a two-section questionnaire and patients’ medical documents. Section one included two parts. The first part contained patients’ demographic data (age, sex, level of education, marital status, history of heart failure disease and other diseases as well as the number of hospitalizations). The second section included patients’ medical evidences including cardiac ejection fraction, disease class, and consumed medications.
The second part of the questionnaire was a researcher made perceived support questionnaire, which was prepared by various related tools such as multi-dimensional perceived social support,[25] social support,[26] questionnaire of care atmosphere in the family[27] and experts’ indications. This questionnaire contained 15 items to evaluate making the patients to participate in decision making, patients’ encouragement, giving appropriate feedback to the patients, expression of empathy and love, practical support and help to the patient, and generally, overall family support to the patients concerning having self-care behavior and disease control. The items were answered in a five-point Likert's scale from never (Score 0) to always (Score 4). There were four negative items in this tool, which were scored inversely. The scores of the questions ranged 0–60 points. To establish and calculate the face and content validity of perceived support questionnaire, it was distributed among 10 academic members from various departments in Isfahan University of Medical Sciences, and necessary modifications were made based on their indications. To establish reliability, the questionnaires were distributed among 10 qualified subjects in a pilot study and Cronbach's alpha was calculated (alpha = 0.74). These 10 subjects were left out of the study. Researcher, after presenting his letter of introduction and explanation of research goals to the authorities of selected clinics and obtaining their agreement and cooperation, administrated sampling and collected the data. The selected main caregiver had active cooperation in all care aspects such as making an appointment with the physician and accompanying the patient to visit the physician, prepare medication, control diet obedience, and generally, cooperate with the patient in all decisions related to the disease and its treatment. After the allocation of the subjects in study group, group sessions including three educational sessions were conducted for two 10-member and one 12-member groups of caregivers. These 1–1.5 h sessions were held once a week in one of the educational classes of above-mentioned centers based on the following schedule.
In the first session, the subjects were familiarized with the definition and process of heart failure, causes and treatments, importance and methods of self-care skills and behaviors administration and importance of family centered care and the role of family members in patients’ support. At the end of the sessions, a guideline booklet of CHF patients self-care was given to each caregiver not only to read but also to review the important points with other members of the family and to answer the questions concerning the disease and self-care behavior at the end of the booklet with cooperation of the patient. There were also asked to write down their questions and deliver them to the researcher in the following session.
In the second session, patients’ and their caregivers’ responses to the questions in the booklet were picked up, the related issues were educated, and the administration of education was measured. Then, necessary guidance was given to the caregivers. Next, the importance and role of the family in disease control and patients’ care were explained. Caregivers conducted group discussion about living with a CHF patient and the ways to support him/her, and in order to increase patients’ emotional support, they explained about effective communication skills. Case scenarios, role play of presented strategies, group discussion, and supportive dialogues were conducted to reinforce and practice the already learned skills. At the end of session, each caregiver was given a booklet about the importance and methods of practical and emotional support of the patients’ families, and they were asked to pass it out to other members of the family to study.
In the third session, caregivers gave examples about application of the strategies and communicational methods, which could support the patient as well as the prohibiting and facilitating factors during the past week. Then, other scenarios were used to modify and reinforce the skills. In the end, some points about the way of self-care were explained to the caregivers, and some indications were made to finalize the discussed issues during the sessions and reach a conclusion.
Finally, contact phone numbers were given to the caregivers to answer their questions concerning the disease and self-care behaviors. Two weeks after the end of group sessions, necessary guidance was given, in addition to the evaluation of transfer of information and skills concerning patients’ care and family support to the caregivers through follow-up phone calls.
The questionnaires of perceived support were completed by the subjects in both groups 1-month after. In this study, for the control group, simultaneously underwent two educational sessions about the needed care of CHF patients and were given an educational booklet with regard to the importance and role of family support.
Collected data were analyzed by descriptive and analytical (independent t-test, paired t-test) statistical tests through SPSS 20 (SPSS Inc: Chicago), and significance level was considered P < 0.05.
RESULTS
In the present study, firstly 276 CHF patients referring to university clinics of the research environment who met inclusion criteria were primarily investigated during 3 months. Among them, 81 patients met the needed qualifications of whom 17 did not attend the study either due to irregular attendance in the sessions, progression of their diseases or not attending the study from the very beginning. Finally, the data of 64 family caregivers were analyzed. As presented in Table 1, comparison of the subjects characteristics showed no significant difference between two groups concerning patients’ age, sex, marital status, level of education, class of the disease, history of hospitalization as well as caregivers’ sex, age and level of education, their relationship with the patient and the length of caring the patients.
Table 1.
Demographic characteristics of samples in control and interventional groups
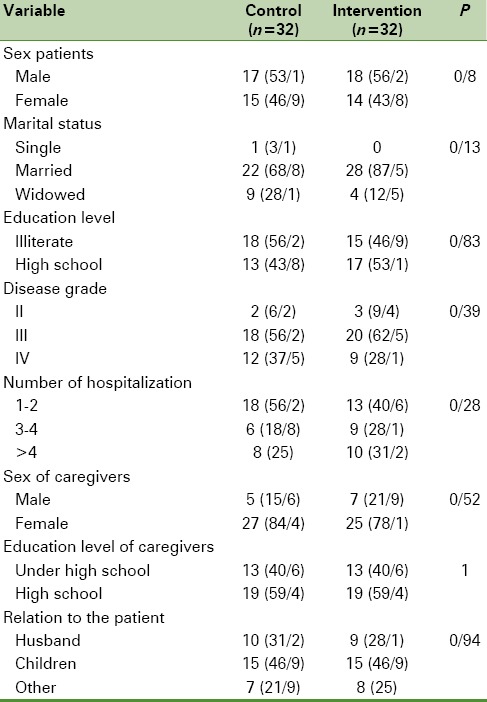
Most of the subjects in both groups were male, married and in class 3 of the disease with 1–2 times history of hospitalization due to CHF. Most of the subjects in study group were illiterate while, in the control group, they had an education lower than high school diploma. Most of the caregivers in both groups were women with education levels of high school diploma and under. With regard to family relationship, the caregivers were mostly patients’ children.
As presented in Table 2, mean scores of perceived support before intervention in study and control groups were 37.4 (3.9) and 37.8 (4.2), respectively. Independent t-test showed no significant difference in mean scores of perceived support between study and control groups before the intervention (P = 0.74). Mean scores of perceived support 1-month after intervention were 51.2 (4.9) and 38.6 (3.9) in study and control groups respectively.
Table 2.
The comparison between perceived support mean scores of the subjects in the intervention and control groups before and after the intervention
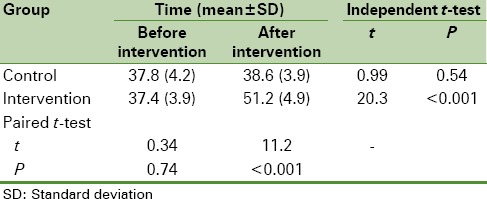
Independent t-test showed a significant difference in mean scores of perceived support between study and control groups after the intervention (P < 0.0001). The obtained results showed that mean scores of perceived support were 13.7 (3.8) and 0.8 (2.4) in study and control groups after the intervention, respectively. Independent t-test showed a significant difference in mean score changes of perceived support between study and control groups after the intervention (P < 0.001).
DISCUSSION
Although the present study focused on the familial dimension of social support, it revealed the effect of all dimensions of social support on patients’ perceived support, consistent with other studies focusing on emotional or informational dimensions of social support. As our obtained results showed, supportive interventions could lead to improvement of perceived support in patients, especially when the family members administrated the support. Davari, in a study on the effect of social support on QOL in patients with heart failure, showed a significant difference in mean scores of perceived social support between study and control groups after intervention.[28] Duhamel reported that spouses’ behavior changed toward encouragement of the patients for diet therapy obedience. They also reported an increase in the support given to the patients after administration of a family centered nursing intervention, counseling and the follow-up phone calls made with the patients and their spouses concerning the interactions between the patients and their family members.[29] Their results are in line with those of the present study as in the present study; interventions to improve interactions between the caregivers and the patients were designed and administrated in form of group sessions, which resulted in an increase in patients’ support. Piette et al., in a study on improving heart failure self-management support by actively engaging out-of-home caregivers, showed that even the support, given by nonrelatives and out-of-home caregivers, could lead to satisfaction with administration of intervention in 98% of the patients receiving support from their caregivers.[24] Sayers et al. concluded that the administration of supportive and educational programs for CHF patients and their family members improved self-care behaviors.[19] Although numerous studies reported the effect of interventions based on patients’ caregivers participation on perceived social support, there are few studies reporting controversial results. Riegel et al. reported no significant difference in mean scores of perceived support between study and control groups after the intervention.[11] In their study, the support was given by the peers, but not by the patients’ family members. In addition, the patients’ diseases were not restricted to CHF, and there were patients with diabetes and hypertension. They indicated that poor intervention, high mean age of the subjects, subjects’ numerous physical problems and living alone were the causes for inefficacy of the conducted intervention on perceived support. Their results are not consistent with the present study. The difference may have been resulted from their different adopted interventions, higher age of their subjects and the higher number of the subjects living alone in the above-mentioned study. Agren et al., in a study on investigation and assessment of the effects of administration of heart failure patients and their partners, reported no significant difference in mean scores of self-care behaviors between study and control groups after intervention. Their care program included cognitive, psychosocial and behavior treatments for the patients and their caregivers. In their study, conducted on 155 subjects and their caregivers in Sweden, several tools were adopted to evaluate the depression (Beck), self-care behaviors, QOL, attitude control criterion and care giving burden. The effects of the interventional program were evaluated 3 and 12 months after patients’ discharge, and no effect of the intervention on self-care and QOL was observed.[30] Their study was different from the present study with regard to the sample size, interventional program, longer posttest time and filling different questionnaires. Dunbar et al.,[23] in a study on 61 patients with heart failure in USA, conducted two methods of patients mere education, and education in addition to family participative intervention, administrated by the nurses, physicians and a nutritionists and reported no change in mean scores of perceived support 3 months after intervention in mere education group. Meanwhile, although there was a difference in mean scores of perceived support in family participation group, it was not significant. One of the interesting findings of the present study that is originated from Iranian culture is that most of the caregivers were patients’ children in the first rank and their spouses in the second rank. On the contrary, the studies, conducted in other countries such as the study of Gallagher et al.[18] in Netherland and Dunbar et al.[23] in USA reported that most of the caregivers were patients’ partners.
CONCLUSION
The results of the present study showed the pivotal role of social support, especially the support given by the family members, in CHF patients’ perception from their received support.
Therefore, the nurses, as the professional members of health domain and with regard to their important role in support, education and care of CHF patients and their caregivers can support, educate and guide CHF patients by designing appropriate care plans through educating the patients’ family members. They can take efficient steps toward improvement of patients’ perceived social support, especially family support, and promotion of their self-care behaviors. Designing, administration and application of such educational and supportive programs, based on patients’ families participation, can reveal the role of the nurses in involvement of the families in improvement of the patients’ and the society's health behaviors. As family-participation-based interventions can lead to feeling more support among the patients by making a change in the atmosphere of the family, it is suggested to design and administrate such interventions and conduct more studies to improve self-care and change health behaviors in other chronic diseases patients.
Financial support and sponsorship
School of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors acknowledge the Nursing and Midwifery Faculty, Isfahan University of Medical Sciences, for supporting this work. They would also like to thank all the people who made this study possible.
REFERENCES
- 1.Ghahramani A, Kamrani F, Mohamadzadeh SH. Effect of self-care education on knowledge, performance and readmission in patient with heart failure. J Health Care. 2010;12:11–20. [Google Scholar]
- 2.Woods SL, Froelicher ES, Motzer SU, Bridges EJ. 5th ed. New York: Lippincott Williams & Wilkins; 2010. Cardiac Nursing; p. 555. [Google Scholar]
- 3.Hekmatpou D, Mohamadi E, Ahmadi F, Arefi SH, Rafie M. The effectiveness of applying “Making Sensivity to Readmission Caring Model” on controlling congestive heart failure complications among hospitalized patients in Tehran cardiovascular centers. Med J Iran Univ. 2009;17:33–49. [Google Scholar]
- 4.Luttik ML, Jaarsma T, Veeger N, Tijssen J, Sanderman R, van Veldhuisen DJ. Caregiver burden in partners of Heart Failure patients; limited influence of disease severity. Eur J Heart Fail. 2007;9:695–701. doi: 10.1016/j.ejheart.2007.01.006. [DOI] [PubMed] [Google Scholar]
- 5.Baker DW, Rown J, Chan K, Dracub K, Keeler EA. Telephone survey to measure communication, education, self-management and health status for patients with heart failure: The improving chronic illness care evaluation (ICICE) J Card Fail. 2005;11:36–42. doi: 10.1016/j.cardfail.2004.05.003. [DOI] [PubMed] [Google Scholar]
- 6.Rafiei F, Rambod M, Hosseini F. Perceived social support for patients treated with Hemodialysis. Hayat J. 2009;15:5–12. [Google Scholar]
- 7.Sarrafino A. Tehran: Roushd Publication; 2004. Psychology of Health, translation by Mirzaei E. [Google Scholar]
- 8.DiMatteo MR. Social support and patient adherence to medical treatment: A meta-analysis. Health Psychol. 2004;23:207–18. doi: 10.1037/0278-6133.23.2.207. [DOI] [PubMed] [Google Scholar]
- 9.Yu DS, Lee DT, Woo J. Psychometric testing of the Chinese version of the medical outcomes study social support survey (MOS-SSS-C) Res Nurse Health. 2004;27:135–43. doi: 10.1002/nur.20008. [DOI] [PubMed] [Google Scholar]
- 10.Schaffer MA. Social support. In: Peterson SJ, Bredow TS, editors. Application to Nursing Research. Philadelphia: Wolters Kluwer Health; 2009. [Google Scholar]
- 11.Riegel B, Moser DK, Anker SD, Appel LJ, Dunbar SB, Grady KL, et al. State of the science: Promoting self-care in persons with heart failure: A scientific statement from the American Heart Association. Circulation. 2009;120:1141–63. doi: 10.1161/CIRCULATIONAHA.109.192628. [DOI] [PubMed] [Google Scholar]
- 12.Heidari A, Mazloom SR, Ildarabadi E. Nursing's position in health care delivery system in Iran. Iran J Nurs Res. 2012;7:37–44. [Google Scholar]
- 13.Rosland AN, Kieffer E, Israel B. When is social support important?. The association of family support and professional support with specific diabetes self-management behaviors. J Gen Intern Med. 2008;23:1992–9. doi: 10.1007/s11606-008-0814-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Keyvanara M. Evaluation of Economic and Social Factors Affecting the Control of Diabetes in Patients Admitted to Hospital Dr. Gharazi in Isfahan, Master Thesis, Isfahan Medical Sciences. 2011 [Google Scholar]
- 15.Hogana BE, Linden W, Najarian B. Social support interventions: Do they work? Clin Psychol Rev. 2002;22:381–440. doi: 10.1016/s0272-7358(01)00102-7. [DOI] [PubMed] [Google Scholar]
- 16.Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. 12th ed. New York: Lippincott Williams & Wilkins; 2010. Brunner & Suddarth's Text Book of Medical-surgical Nursing. [Google Scholar]
- 17.Brostrom A, Stromberg A, Dahlstrom U, Fridlund B. Congestive heart failure, spouses’ support and the couple's sleep situation: A critical incident technique analysis. J Clin Nurs. 2003;12:223–33. doi: 10.1046/j.1365-2702.2003.00692.x. [DOI] [PubMed] [Google Scholar]
- 18.Gallagher R, Luttik ML, Jaarsma T. Social support and self-care in heart failure. J Cardiovasc Nurs. 2011;26:439–45. doi: 10.1097/JCN.0b013e31820984e1. [DOI] [PubMed] [Google Scholar]
- 19.Sayers SL, Riegel B, Pawlowski S, Coyne JC, Samaha FF. Social support and self-care of patients with heart failure. Ann Behav Med. 2008;35:70–9. doi: 10.1007/s12160-007-9003-x. [DOI] [PubMed] [Google Scholar]
- 20.Clark AM, Margaret ER, Caroline EM, Simon C, Murdoch DL, John J. The complex nature of informal care in home based heart failure management. J Adv Nurs. 2007;61:373–83. doi: 10.1111/j.1365-2648.2007.04527.x. [DOI] [PubMed] [Google Scholar]
- 21.Campbell TL. Improving Health through Family Interventions, Handbook of Families and Health. 2006. [Last accessed on 2014 Jul 04]. Available from: http://www.books.google.com14 .
- 22.Kang X, Li Z, Nolan MT. Informal caregivers’ experiences of caring for patients with chronic heart failure: Systematic review and meta synthesis of qualitative studies. J Cardiovasc Nurs. 2011;26:386–94. doi: 10.1097/JCN.0b013e3182076a69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dunbar SB, Clark PC, Deaton C, Smith AL, De AK, O’Brien MC. Family education and support interventions in heart failure: A pilot study. Nurs Res. 2005;54:158–66. doi: 10.1097/00006199-200505000-00003. [DOI] [PubMed] [Google Scholar]
- 24.Piette JD, Gregor MA, Share D, Heisler M, Bernstein SJ, Koelling T, et al. Improving heart failure self-management support by actively engaging out-of-home caregivers: Results of a feasibility study. Congest Heart Fail. 2008;14:12–8. doi: 10.1111/j.1751-7133.2008.07474.x. [DOI] [PubMed] [Google Scholar]
- 25.Zimet GD, Powell SS, Farley GK, Werkman S, Berkoff KA. Psychometric characteristics of the Multidimensional Scale of Perceived Social Support. J Pers Assess. 1990;55:610–7. doi: 10.1080/00223891.1990.9674095. [DOI] [PubMed] [Google Scholar]
- 26.Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med. 1991;32:705–14. doi: 10.1016/0277-9536(91)90150-b. [DOI] [PubMed] [Google Scholar]
- 27.Clark PC, Dunbar SB. Preliminary reliability and validity of a Family Care Climate Questionnaire for heart failure. Fam Syst Health. 2003;21:283–93. [Google Scholar]
- 28.Davari A. The Effect of Social Support on Quality of Life in Patients with Heart Failure Referring to Specialized Center of Cardiology, Hamadan University of Medical Sciences, Master Thesis. 2011 [Google Scholar]
- 29.Duhamel F, Dupuis F, Reidy M, Nadon N. A qualitative evaluation of a family nursing intervention. Clin Nurse Spec. 2007;21:43–9. doi: 10.1097/00002800-200701000-00009. [DOI] [PubMed] [Google Scholar]
- 30.Agren S, Evangelista LS, Hjelm C, Stromberg A. Dyads affected by chronic heart failure: A Randomized study evaluating effects of education and psychosocial support to patients with heart failure and their partners. J Card Fail. 2012;18(5):359–366. doi: 10.1016/j.cardfail.2012.01.014. [DOI] [PMC free article] [PubMed] [Google Scholar]