

Abstract
Background
The safety of surgical approaches for single- versus double-incision carpal tunnel release in association with distal radius open reduction and internal fixation remains controversial.
Purpose
The purpose of this study was to identify critical structures to determine if a single-incision extension of the standard flexor carpi radialis (FCR) approach can be performed safely.
Methods
Nine cadaveric arms with were dissected under loupe magnification, utilizing a standard FCR approach. After the distal radius exposure was complete, the distal portion of the FCR incision was extended to allow release of the carpal tunnel. Dissection of critical structures was performed, including the recurrent thenar motor branch of the median nerve, the palmar cutaneous branch of the median nerve (PCBm), the palmar carpal and superficial palmar branches of the radial artery, and proximally the median nerve proper. The anatomic relationship of these structures relative to the surgical approach was recorded.
Results
Extension of the standard FCR approach as described in this study did not damage any critical structure in the specimens dissected. The PCBm was noted to arise from the radial side of the median nerve an average of 6.01cm proximal to the proximal edge of the transverse carpal ligament. The PCBm became enveloped in the layers of the antebrachial fascia and the transverse carpal ligament at the incision site, protecting it from injury. The recurrent motor branch of the median nerve, branches of the radial artery and the median nerve proper were not at risk during extension of the FCR approach to release the carpal tunnel.
Conclusions
Extension of the standard FCR approach to include carpal tunnel release can be performed with minimal risk to the underlying structures. This exposure may offer benefits in both visualization and extent of carpal tunnel release.
Keywords: extended flexor carpi radialis approach, distal radius volar plating, acute carpal tunnel release, palmar cutaneous branch median nerve, motor recurrent
Distal radius fractures (DRF) are common injuries, comprising nearly one sixth of all fractures presenting to the emergency room, while accounting for a noteworthy proportion of health care costs.1 2 3 Operative treatment of DRF is on the rise, likely as the result of their increasing overall incidence as well as continually evolving implant technologies and fixation techniques.3 4 Unfortunately, as the incidence of these fractures increases, the risk of complications due to the injury or its treatment is expected to continue presenting challenges for surgeons.
Compression neuropathy of the median nerve is a concerning complication, particularly when presenting acutely, as is reported concomitantly in as many as 5.4 to 8.6% of DRF.5 6 7 In such cases, rapid decompression of the carpal tunnel in coordination with surgical fixation of the fracture is often necessary to minimize patient morbidity and potential for long-term sequelae. However, the occurrence of carpal tunnel syndrome (CTS) is not limited to the acute setting of DRF; altered wrist anatomy and kinematics resulting directly from the DRF or its fixation can lead to delayed secondary development of CTS in as many as 20% of the patients.8 For this reason, many surgeons advocate a prophylactic carpal tunnel release at the time of fracture fixation, although its routine practice remains controversial.9 10 11 Whether CTS is performed for therapeutic or prophylactic reasons, when performed concomitantly with distal radius fracture fixation, the optimal surgical approach is also debated. The recent popularity of fixed angle volar plating and the use of the standard flexor carpi radialis (FCR) approach to the distal radius have likely only added to this controversy.12 One theoretical advantage of a single extensile incision incorporating an FCR approach to the distal radius and carpal tunnel release is a wider surgical exposure, which may prove especially useful when treating fractures with a significantly unstable or displaced dorsal component, or complex intra-articular involvement. Thus, such an extensile approach may obviate the need for a separate dorsal incision or wrist arthroscopy.
Despite these potential advantages, the relevant anatomy of this proposed extensile approach remains inadequately understood. The purpose of this study was to identify critical structures that may be at risk during extension of the FCR approach to incorporate a standard carpal tunnel release, to determine if this extensile incision can be safely utilized to decompress the carpal tunnel following distal radius exposure.
Materials and Methods
Nine cadaveric arms from seven cadavers with no history of fracture or pathology were dissected under loupe magnification. A standard FCR approach was performed as described by Orbay et al.12 An 8 to 9 cm incision was made in line with the FCR tendon, and zigzagged across the flexor creases (Fig. 1). The incision was carried to the level of the FCR tendon sheath. The sheath was incised sharply and the FCR tendon retracted ulnarly to protect the median nerve. A 1-cm incision was then made in the floor of the tendon sheath and was extended proximally and distally with blunt Joseph scissors. The space of Parona was developed using blunt finger dissection and the pronator quadratus muscle and radial artery were identified (Fig. 2). With the radial artery retracted by a Homan retractor, an l-shaped incision was made through the pronator along the radial border. The muscle was elevated ulnarly and distally to the level of the proximal wrist capsule.
Fig. 1.

An 8 to 9 cm incision is made overlying the FCR tendon and zigzagged across the wrist crease. FCR, flexor carpi radialis.
Fig. 2.

The space of Parona is dissected. The radial artery (black arrow) and pronator quadratus (white arrow) are identified.
Following completion of the distal radius exposure, the distal aspect of the FCR incision (point A, Fig. 3) was extended to allow release of the carpal tunnel. With the fourth digit fully flexed, a mark was made along the ulnar border of its tip. (point B, Fig. 3) The metacarpophalangeal joint of the digit was then extended as to place a mark along the ulnar border of the digit tip (point C, Fig. 3) approximately 2 to 3 cm distal to the first mark. A gently curving incision was then drawn connecting the distal portion of the FCR approach (point A, Fig. 4) and the two marks (points B and C, Fig. 4). An incision through the skin was performed, and was deepened to expose the transverse carpal ligament (TCL) in the distal 2 to 3 cm only (interval between points B and C). Proximally skin flaps were raised to provide exposure of the palmar cutaneous branch of the median nerve (PCBm) as well as the proximal TCL and antebrachial fascia.
Fig. 3.

Extension of the FCR approach from its distal aspect (point A) to a standard carpal tunnel approach marked in line with the ulnar border of the ring finger (points B and C). FCR, flexor carpi radialis.
Fig. 4.

A gently curved incision connects the FCR incision to the standard carpal tunnel approach. FCR, flexor carpi radialis.
A standard carpal tunnel release was then performed by sharply incising a 1-cm portion of the TCL. A Freer elevator was placed within the tunnel to protect the nerve while blunt Joseph scissors were used to transect the TCL distally and proximally. With the TCL released and carpal tunnel decompressed, dissection of the structures of interest was then performed including: the recurrent thenar motor branch of the median nerve, the PCBm, the palmar carpal and superficial palmar branches of the radial artery, and the median nerve proper. The relationship of these structures to the incision, to the FCR tendon, and to each other was measured using a digital caliper. Measurements of the distance from the takeoff of the PCBm to the proximal extent of the TCL were also taken, as were measurements of the distance between the ulnar border of the FCR tendon and the median and palmar cutaneous nerves.
Results
The recurrent motor branch of the median nerve was identified and noted to be extraligamentous in all nine specimens (Fig. 5). Evaluation of the radial artery and its palmar branches revealed that in all specimens, the palmar carpal branch of the radial artery could be identified within 1 cm of the distal edge of the pronator quadratus muscle (Table 1 and Fig. 6). From its branch point, the radial palmar carpal artery coursed ulnarly and passed immediately dorsal to the floor of the FCR tendon sheath. However, with regards to the extension of the FCR incision performed here, neither the superficial palmar nor the palmar carpal branch of the radial artery was noted to be in proximity to this incision.
Fig. 5.

The recurrent thenar motor branch of median nerve (arrow A) and PCBm (arrow B) becoming enveloped by layers of antebrachial fascia and transverse carpal ligament. PCBm, palmar cutaneous branch of the median nerve.
Table 1. Measured distances and relationships between structures of interest and important anatomic landmarks.
| Structure | Relation to | Anatomic landmark | Mean distance |
|---|---|---|---|
| PCBm takeoff | Arises radially from | Median nerve | – |
| Proximal to | Proximal edge of transverse carpal ligament | 59.8 mma | |
| Dorsal FCR sheath (via standard approach incision) | Radial to | Median nerve | 3.7 mm |
| Motor recurrent of median nerve takeoff | Distal and extraligamentous to | Transverse carpal ligament | – |
| Palmar carpal branch of radial artery | Distal to | Distal edge of PQ | 8.8 mm |
Abbreviations: FCR, flexor carpi radialis; PCBm, palmar cutaneous branch of the median nerve; PQ, pronator quadratus.
One specimen had a second PCBm with takeoff measured 25.2 mm proximal to transverse carpal ligament (Fig. 6).
Fig. 6.
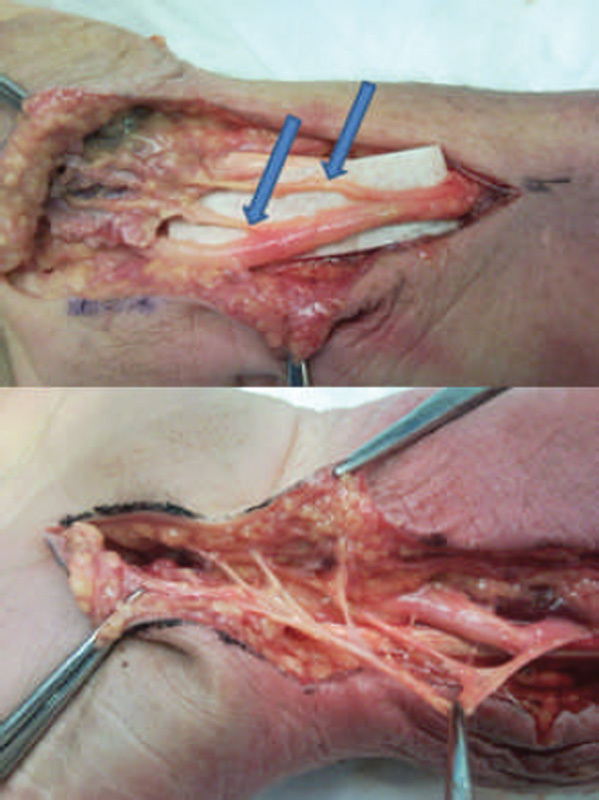
(Top) Distal course demonstrating dual PCBm, depicted by arrows. (Bottom) PCBm splits giving rise to two major branches. PCBm, palmar cutaneous branch of the median nerve.
The relationship of the median nerve proper to its surrounding tendons and to the plane of surgical dissection was then evaluated. In its course through the forearm, the median nerve was noted to be adherent to the FCR sheath at its ulnar edge (Table 1). In all specimens, the median nerve lay ulnar to the FCR tendon, ulnar and dorsal to the flexor pollicus longus tendon, and radial to the superficial flexor tendons. This relationship remained constant from the proximal extent of the incision to the level of the TCL.
During initial skin incision at the extended portion of this surgical approach, the PCBm could not be identified in any of the cadavers. However, after proximal dissection of the median nerve (interval between points A and B on Figs. 3 and 4), the PCBm was found in all specimens. This branch was dissected distally and noted to have several key anatomic relationships (see Tables 1 and 2). The PCBm ran alongside the median nerve and became adherent to the FCR tendon sheath for the majority of its proximal course. At the level of the proximal wrist crease the nerve turned ulnarly to run in line with the third digit as it became enveloped in the layers of the antebrachial fascia and the TCL. The PCBm remained encased in the flexor retinaculum at the level of the A to B portion of the incision and emerged from the retinaculum radial to the B to C portion of the incision. Upon emergence, the nerve divided into two or three main trunks. A consistent thenar trunk was noted in eight of nine specimens which provided cutaneous branches to the thenar palm. The ulnar branch pattern was more varied in its division and in one specimen a branch of the PCBm was noted to cross the distal portion of the incision at the level of the superficial palmar fascia and was at risk during the standard carpal tunnel portion of the approach. In all specimens, the recurrent motor branch was not at risk for injury during extension of the FCR approach (Fig. 5).
Table 2. Distance from proximal transverse carpal ligament to takeoff of PCBm.
| Specimen | Most proximal (mm) | Most distal (mm) |
|---|---|---|
| 1 R | 61.3 | |
| 2 L | 60.8 | |
| 3 L | 55.7 | |
| 4 R | 69.2 | |
| 4 L | 46.8 | |
| 5 R | 76.7 | |
| 5 L | 70.8 | |
| 6 L | 44.9 | |
| 7 R | 51.9 | 25.2 |
Abbreviations: L, left; PCBm, palmar cutaneous branch of the median nerve; R, right.
Discussion
CTS is a concerning complication following DRF CTS, occurring in as many as 8.6 and 20% of acute and delayed cases, respectively.5 6 7 8 In the acute setting, rapid decompression of the carpal tunnel within 8 hours of onset is indicated to prevent permanent nerve injury.13 While early diagnosis and decompression are key to satisfactory outcomes in the acute setting, the indications for prophylactic release for prevention of chronic cases of CTS are debated.9 10 11
Regardless of the indications, if distal radius fixation and carpal tunnel release are performed in conjunction, there is additional debate regarding the optimal surgical approach for each procedure, and the utility of one versus two incisions. Orbay et al suggested the use of a two-incision technique due to concerns that an ulnarly directed incision would place the PCBm at risk for injury; a concern that has again been echoed more recently.12 14 Lattmann et al reported on distal radius fixation and carpal tunnel release via a single-incision midline volar approach, which was abandoned due to an unacceptably high rate of persistent median nerve symptoms.15 More recently, Pensy et al reported their findings using a “hybrid” FCR approach and found no evidence of danger to the PCBm in cadavers.16 The authors described their approach to include exposure for volar plate fixation of distal radius in combination with the FCR approach to the carpal tunnel as originally described by Weber and Sanders.16 17 Further clinical study demonstrated that in the authors' hands, this hybrid approach was clinically safe with no iatrogenic injury noted to any critical structures.9 18 However, the degree of visualization of the distal TCL is somewhat unclear from the authors' description. In addition, Weber and Sanders themselves acknowledged that the recurrent motor branch of the median nerve is not well visualized in the FCR approach to the carpal tunnel.
In light of these theoretical shortcomings, we elected to study an alternative extensile approach that would also incorporate a carpal tunnel release. The extension of the standard FCR approach described in this study did not damage any critical structure in the nine specimens dissected. This approach has allowed for the identification of the palmar cutaneous branch of the median nerve before performing the carpal tunnel release. After identification the PCBm and its branches can be protected during the remainder of the case. Also, better visualization of the proximal TCL and antebrachial fascia may allow for a more complete release of the proximal structures.
This proposed technique, and this study as a whole are not without limitations. A notable drawback of this exposure is the significantly longer incision and greater degree of soft-tissue dissection that is required compared with other techniques. However, our intention was not necessarily to demonstrate its superiority, but rather to provide information as to a potential alternative exposure that may be warranted in particular fracture types, or when the clinical scenario imposes time constraints against a second, dorsal incision. As with any cadaveric study, there is an inherent potential that the specimens may not fully represent normal human anatomy as the result of embalming and other stages of processing. Thus, our findings would need to be verified clinically before use in a wider population of patients. Additionally, our relatively small sample size may further limit its generalizability to the clinical setting. Despite these limitations, we feel these findings may prove useful for surgeons tasked with performing concomitant carpal tunnel release following distal radius fracture, where wide exposure is desired without the cost iatrogenic injury to nearby structures. With meticulous dissection, extension of the standard FCR approach to include carpal tunnel release can be performed with minimal risk to the underlying structures, which may potentially offer benefits in both visualization and extent of carpal tunnel release.
Conflict of Interest None.
Note
This study was performed at the Department of Orthopaedic Surgery, Louisiana State University Health Sciences Center, New Orleans, LA.
References
- 1.Owen R A, Melton L J III, Johnson K A, Ilstrup D M, Riggs B L. Incidence of Colles' fracture in a North American community. Am J Public Health. 1982;72(6):605–607. doi: 10.2105/ajph.72.6.605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shauver M J, Yin H, Banerjee M, Chung K C. Current and future national costs to medicare for the treatment of distal radius fracture in the elderly. J Hand Surg Am. 2011;36(8):1282–1287. doi: 10.1016/j.jhsa.2011.05.017. [DOI] [PubMed] [Google Scholar]
- 3.Farner S, Malkani A, Lau E, Day J, Ochoa J, Ong K. Outcomes and cost of care for patients with distal radius fractures. Orthopedics. 2014;37(10):e866–e878. doi: 10.3928/01477447-20140924-52. [DOI] [PubMed] [Google Scholar]
- 4.Koval K J, Harrast J J, Anglen J O, Weinstein J N. Fractures of the distal part of the radius. The evolution of practice over time. Where's the evidence? J Bone Joint Surg Am. 2008;90(9):1855–1861. doi: 10.2106/JBJS.G.01569. [DOI] [PubMed] [Google Scholar]
- 5.Cooney W P III, Dobyns J H, Linscheid R L. Complications of Colles' fractures. J Bone Joint Surg Am. 1980;62(4):613–619. [PubMed] [Google Scholar]
- 6.Brüske J, Niedźwiedź Z, Bednarski M, Zyluk A. Acute carpal tunnel syndrome after distal radius fractures—long term results of surgical treatment with decompression and external fixator application [in Polish] Chir Narzadow Ruchu Ortop Pol. 2002;67(1):47–53. [PubMed] [Google Scholar]
- 7.Dyer G, Lozano-Calderon S, Gannon C, Baratz M, Ring D. Predictors of acute carpal tunnel syndrome associated with fracture of the distal radius. J Hand Surg Am. 2008;33(8):1309–1313. doi: 10.1016/j.jhsa.2008.04.012. [DOI] [PubMed] [Google Scholar]
- 8.Bienek T, Kusz D, Cielinski L. Peripheral nerve compression neuropathy after fractures of the distal radius. J Hand Surg [Br] 2006;31(3):256–260. doi: 10.1016/j.jhsb.2005.09.021. [DOI] [PubMed] [Google Scholar]
- 9.Tannan S C, Pappou I P, Gwathmey F W, Freilich A M, Chhabra A B. The extended flexor carpi radialis approach for concurrent carpal tunnel release and volar plate osteosynthesis for distal radius fracture. J Hand Surg Am. 2015;40(10):2026–20310. doi: 10.1016/j.jhsa.2015.07.001. [DOI] [PubMed] [Google Scholar]
- 10.Fuller D A, Barrett M, Marburger R K, Hirsch R. Carpal canal pressures after volar plating of distal radius fractures. J Hand Surg [Br] 2006;31(2):236–239. doi: 10.1016/j.jhsb.2005.10.013. [DOI] [PubMed] [Google Scholar]
- 11.Odumala O, Ayekoloye C, Packer G. Prophylactic carpal tunnel decompression during buttress plating of the distal radius—is it justified? Injury. 2001;32(7):577–579. doi: 10.1016/s0020-1383(00)00198-4. [DOI] [PubMed] [Google Scholar]
- 12.Orbay J L, Badia A, Indriago I R. et al. The extended flexor carpi radialis approach: a new perspective for the distal radius fracture. Tech Hand Up Extrem Surg. 2001;5(4):204–211. doi: 10.1097/00130911-200112000-00004. [DOI] [PubMed] [Google Scholar]
- 13.Mack G R, McPherson S A, Lutz R B. Acute median neuropathy after wrist trauma. The role of emergent carpal tunnel release. Clin Orthop Relat Res. 1994;(300):141–146. [PubMed] [Google Scholar]
- 14.Ilyas A M. Surgical approaches to the distal radius. Hand (NY) 2011;6(1):8–17. doi: 10.1007/s11552-010-9281-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lattmann T, Dietrich M, Meier C, Kilgus M, Platz A. Comparison of 2 surgical approaches for volar locking plate osteosynthesis of the distal radius. J Hand Surg Am. 2008;33(7):1135–1143. doi: 10.1016/j.jhsa.2008.03.016. [DOI] [PubMed] [Google Scholar]
- 16.Pensy R A, Brunton L M, Parks B G, Higgins J P, Chhabra A B. Single-incision extensile volar approach to the distal radius and concurrent carpal tunnel release: cadaveric study. J Hand Surg Am. 2010;35(2):217–222. doi: 10.1016/j.jhsa.2009.11.011. [DOI] [PubMed] [Google Scholar]
- 17.Weber R A, Sanders W E. Flexor carpi radialis approach for carpal tunnel release. J Hand Surg Am. 1997;22(1):120–126. doi: 10.1016/S0363-5023(05)80191-1. [DOI] [PubMed] [Google Scholar]
- 18.Gwathmey F W Jr, Brunton L M, Pensy R A, Chhabra A B. Volar plate osteosynthesis of distal radius fractures with concurrent prophylactic carpal tunnel release using a hybrid flexor carpi radialis approach. J Hand Surg Am. 2010;35(7):1082–1.088E7. doi: 10.1016/j.jhsa.2010.03.043. [DOI] [PubMed] [Google Scholar]