

Abstract
Purpose
As several years have passed since the implementation of the Korean diagnosis-related group (DRG) payment system for appendicitis, its early outcomes should be assessed to determine if further improvements are warranted.
Methods
We retrospectively analyzed clinical data from Korean patients who underwent appendectomy, dividing the sample into 2 groups of those who received services before and after implementation of the DRG system. Based on the DRG code classification, patient data were collected including the amount of DRG reimbursement and the total in-patient costs. We subsequently performed univariate and multivariate analyses to identify independent factors contributing to higher total in-patient cost.
Results
Although implementation of the DRG system for appendicitis significantly reduced postoperative length of stay (2.8 ± 1.0 days vs. 3.4 ± 1.9 days, P < 0.001), it did not reduce total in-hospital cost. The independent factors related to total inhospital cost included patient age of 70 years or more (odds ratio [OR], 3.214; 95% confidence interval [CI], 1.769–5.840; P < 0.001) and operation time longer than 100 minutes (OR, 3.690; 95% CI, 2.007–6.599, P < 0.001). In addition, older patients (≥70 years) showed a nearly 10 times greater relative risk for having a comorbid condition (95% CI, 5.141–20.214; P < 0.001) and a 3.255 times greater relative risk for having higher total in-hospital cost (95% CI, 1.731–6.119, P < 0.001).
Conclusion
It appears that older patients (>70 years) have greater comorbidities, which contribute to higher inpatient costs. Thus, our study suggests that patient age be considered as a DRG classification variable.
Keywords: Appendectomy, Diagnosis-related groups, Age groups, Length of stay, Hospital costs
INTRODUCTION
Increasing medical costs are a primary concern in modern public health. To reduce excessive medical costs and to prevent unnecessary overtreatment, many countries have adopted reimbursement systems based on diagnosis-related groups (DRGs) for selected diseases [1,2,3]. To increase hospitals' cost consciousness, the DRG system moves the financial responsibility from insurers to hospitals. This system allows hospitals to receive fixed-rate payments for inpatient services solely corresponding to the DRG group of a given patient. Accordingly, DRG-based payments encourage hospitals to reduce their costs per patient through various measures, such as reducing the length of stay (LOS), perioperative complications, or the intensity of services [4]. However, some cost-reducing efforts might incur adverse effects, including insufficient effort in diagnosing or managing patients and inappropriate early discharge [4,5,6].
To enhance the efficacy of DRG-based payments, it is essential to determine sufficiently homogenous groups of patients based on treatment cost. Thus, the most important determinants of resource consumption should be the criteria dividing patient classification for the same disease entity [3]. If the DRG classification is not divided according to the major cost-determining factors, hospitals providing greater effort would be inadequately paid for this effort [3]. Presently, DRG-implementing countries exhibit a variety of numbers of DRG classification variables for appendicitis, ranging from 2 (Poland and Sweden) to 8 (Germany) [2].
Since July 2013, South Korea has been implementing a DRG-based payment system for seven groups of specific operations/diseases, including appendicitis. It classifies appendicitis into 2 DRG groups—simple appendicitis and perforated appendicitis—based on presence of appendiceal perforation. Since several years have passed from the start, we think that it is appropriate timing to assess its initial outcomes. In this study, we intended to investigate (1) how the Korean DRG-based payment system affects surgical behavior and outcomes and (2) whether the current patient classification system of the Korean DRG is appropriate for determining patient costs.
METHODS
Study design and data collection
This study analyzed a prospectively collected database of patients who underwent appendectomy due to appendicitis between May 2012 and August 2014 at the Department of Surgery, Daejeon St. Mary's Hospital, the Catholic University of Korea, South Korea. The study was approved by the Ethics Committee at Daejeon St. Mary's Hospital, the Catholic University of Korea (approval number: DC15OISI0048). During the study period, 600 patients were screened for eligibility. The exclusion criteria were (1) patient age < 5 years, (2) combined or more extensive operation(s) beyond simple appendectomy under the same anesthesia, (3) appendectomy delayed for more than 5 days after the initial attack, and (4) a final pathologic diagnosis other than appendicitis. The DRG-based payment system was implemented in June 2013. Thus, the patient population was divided into 2 groups: patients who underwent appendectomy prior to DRG implementation (May 2012 to June 2013) and those who underwent appendectomy after DRG implementation (July 2013 to August 2014).
During the study period, all appendectomies were initially attempted via a laparoscopic approach, regardless of history of abdominal laparotomy, patient age or presence of comorbidity. Single-port laparoscopic appendectomy (SPLA) was first attempted in January 2013 and thereafter was selectively performed according to the operator's decision. In this study, uncomplicated appendicitis refers to unperforated appendicitis, and complicated appendicitis refers to appendicitis showing perforation or other consequences (i.e., periappendiceal abscess). In postoperative complications, urinary retention was defined as the need for prolonged catheterization (≥5 days) or reinsertion of a Foley catheter because of an inability to void. Intestinal obstruction was defined as the inability to tolerate a solid diet accompanied by suporting radiologic findings.
Operative technique
Throughout the study period, SPLA was the typical treatment for acute appendicitis. Our institution first performed SPLA in October 2008; since then, SPLA has largely replaced the conventional 3-port laparoscopic appendectomy. In the process of SPLA, the abdominal cavity was entered through the umbilicus using a 1.5- to 2.5-cm vertical incision. We initially used an institutionally customized single port, which was later replaced by a commercial single port, such as the OCTO port (Dalim Medical Co., Seoul, Korea) or the Glove port (Sejong Medical Co., Paju, Korea). Other operative specifics of SPLA did not vary from those of conventional laparoscopic appendectomy. Peritoneal irrigation with appropriate quantities of saline was performed under direct vision for all patients, and Jackson-Pratt drains were used as needed.
Perioperative management
We implemented a standardized perioperative protocol. For all patients with appendicitis, the initial step at the emergency department includes prompt intravenous hydration using crystalloid fluids and intravenous antibiotics (cefotetan 1.0 g). Because cefotetan has a 24-hour dosing schedule, it was typically administered only once before appendectomy (usually 1.0 g, with a maximum dose of 2.0 g). Postoperatively, cefotetan was usually administered starting on the first postoperative day for 1 to 2 days or longer as needed. All patients with complicated appendicitis were coadministered intravenous metronidazole (50 mg/kg, with a maximum dose of 2 g). Antibiotic change or dosage adjustment was considered when there were no improvements in clinical parameters, such as body temperature or leukocyte count. All patients were allowed a clear liquid diet several hours after returning to the ward, and the diet was advanced as tolerated. Patients received intravenous ketorolac (0.1 mg/kg) as needed for controlling pain. Patients were discharged when tolerating a regular diet. At discharge, oral antibiotics (cefaclor or cefcapene) were prescribed for a 3-day period only to the patients with complicated appendicitis.
Statistical analysis
Numeric data were presented as mean and standard deviation or as median and range. Continuous variables were analyzed by independent t-tests, and proportions were compared with Pearson chi-square tests or Fisher exact tests, as appropriate. For data that were not normally distributed, Wilcoxon rank-sum tests were used to examine differences in central tendencies. Logistic regression was used to assess the risk of increased total in-patient cost (≥80%) while controlling for other independent variables. Statistical analyses were performed using IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA). P-values <0.05 were considered statistically significant. All P-values are 2-tailed.
RESULTS
Baseline characteristics and preoperative variables
The patient population included patients who underwent appendectomy in the pre-DRG (n = 300) and post-DRG (n = 300) periods. The median age was 37 years (range, 6–89 years), and the median body mass index was 22.6 kg/m2 (13.6–43.7 kg/m2). The patients were comprised of 302 women (50.3%) and 298 men (49.7%). Patients were diagnosed with uncomplicated and complicated appendicitis at rates of 90.2% (n = 541) and 9.8% (n = 59), respectively. All the appendectomies were initially attempted via a laparoscopic approach, and SPLA comprised 94.5% (n = 567) of all the laparoscopic operations. The median operation time was 55 minutes (range, 20–200 minutes), and the median postoperative LOS was 3 days (1–19 days).
Table 1 shows a summary of the comparisons between demographic and preoperative clinical parameters of patients in the pre-DRG and post-DRG groups. The 2 operative groups were comparable in the most baseline variables, including age, sex, comorbidity, and (radiologically measured) appendiceal diameter. However, the WBC counts were significantly lower in the post-DRG group than in the pre-DRG group (11,247 ± 4,803/mm3 vs. 12451 ± 4295/mm3, P = 0.001).
Table 1. Patient demographics and baseline preoperative characteristics.
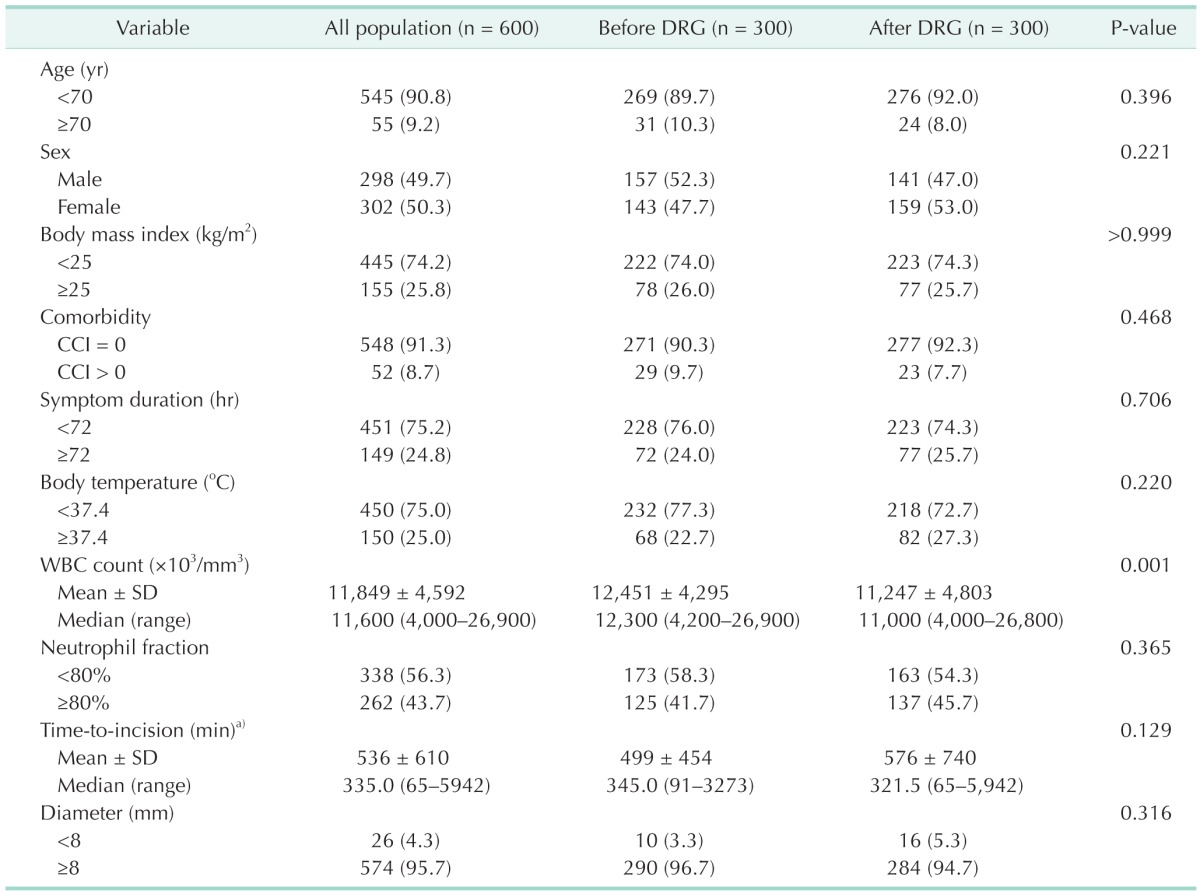
Values are presented as number (%) unless otherwise indicated.
CCI, Charlson's Comorbidity Index; SD, standard deviation.
a)Time to incision: time from arrival at the Emergency Department to incision.
Comparison of operative and postoperative variables of appendectomy before and after DRG
We next compared operative and postoperative variables between pre-DRG and post-DRG patient populations (Table 2). The 2 groups showed no significant differences in terms of operative method, conversion rate, operation time, total dose of postoperative analgesics, and incidence of postoperative complications. However, the post-DRG group showed a significantly shorter postoperative LOS than the pre-DRG group (2.8 ± 1.0 days vs. 3.4 ± 1.9 days, P < 0.001).
Table 2. Operative and postoperative characteristics of the patients who underwent appendectomies before and after DRG.
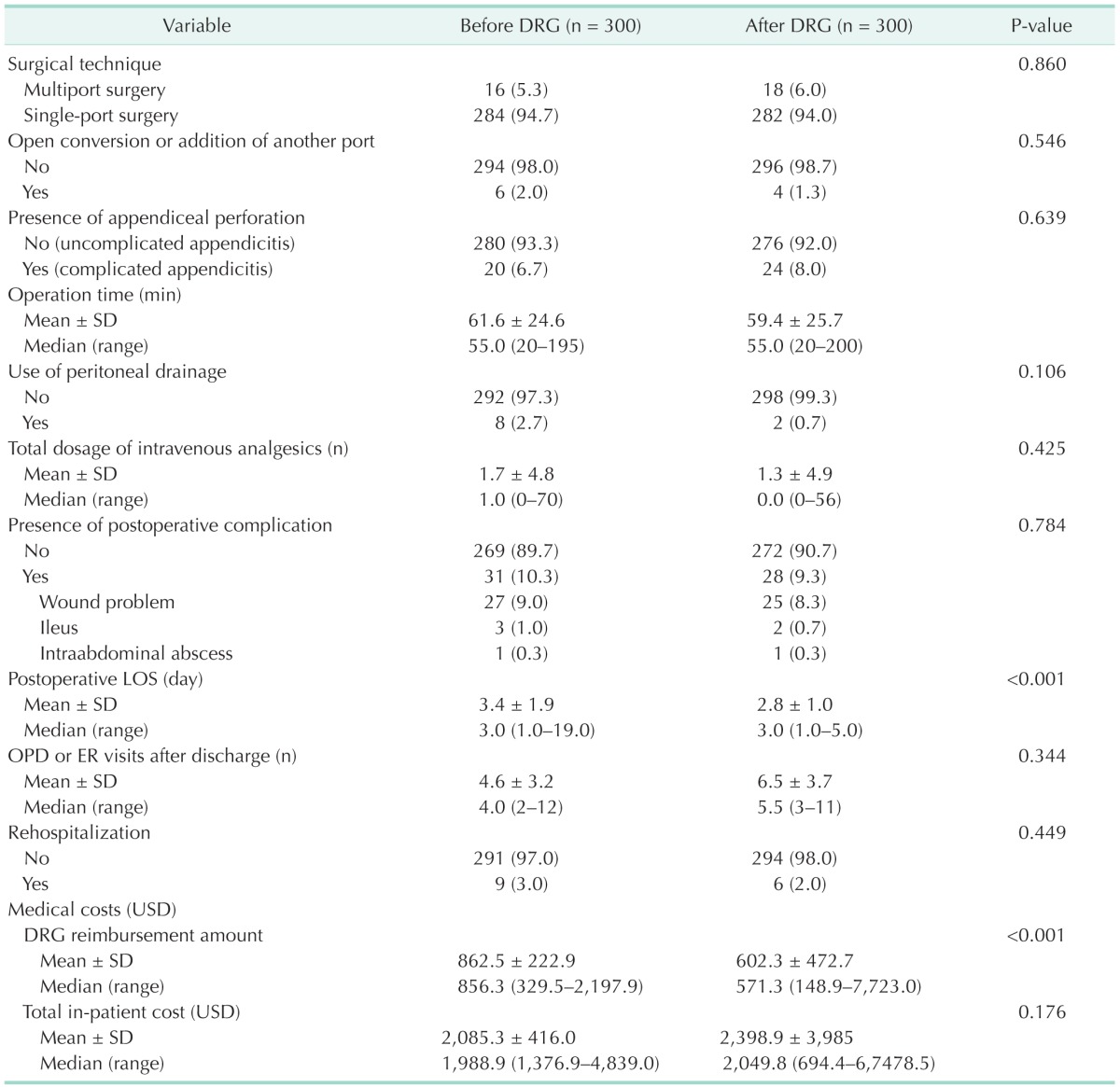
Values are presented as number (%) unless otherwise indicated.
DRG, diagnosis-related group; SD, standard deviation; LOS, length of hospital stay; OPD, outpatient clinic; ER, emergency room; USD, United States dollar.
In the comparison of medical costs, although total in-patient costs were comparable between the 2 groups, DRG reimbursement amounts were significantly lower in the post-DRG group than in the pre-DRG group (602.3 ± 472.7 United States dollar [USD] vs. 862.5 ± 222.9 USD, P < 0.001).
Identification of the factors influencing total in-patient hospital costs
We divided the patient population according to total in-patient costs (the criteria of 80%) and sought to identify the factors affecting total inpatient costs (Table 3). Univariate analyses identified patient age (<70 years vs. ≥70 years, P < 0.001), operation time (<100 minutes vs. ≥100 minutes, P < 0.001), and postoperative LOS (P = 0.025) as the factors affecting total hospital costs. However, the primary diagnosis of appendicitis (uncomplicated appendicitis vs. complicated appendicitis) was not a significant factor affecting total in-patient costs. Through multivariate analysis, we similarly identified independent factors affecting total inpatient hospital costs, including patient age of 70 years or more (OR, 3.214; 95% CI, 1.769–5.840, P < 0.001) and operation time longer than 100 minutes (OR, 3.690; 95% CI, 2.007–6.599, P < 0.001).
Table 3. Univariate and multivariate analyses of preoperative and intraoperative factors related to higher total in-hospital costs of appendectomy.
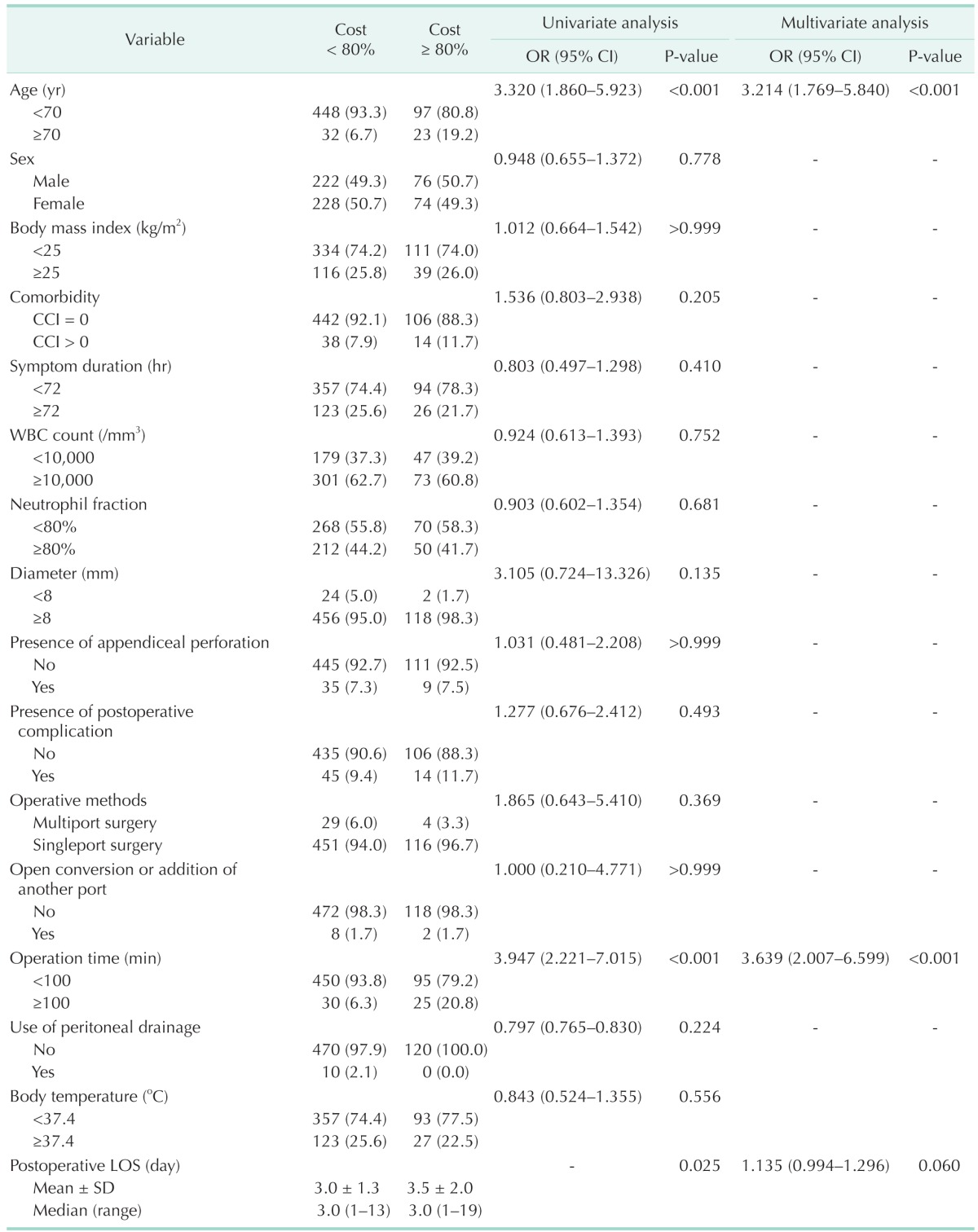
Values are presented as number (%) unless otherwise indicated
OR, odds ratio; CI, confidential interval; CCI, Charlson's Comorbidity Index; LOS, length of hospital stay; SD, standard deviation.
Effects of patient age on surgical outcomes following appendectomy
To determine the effects of patient age on surgical outcomes following appendectomy, we compared the clinical variables according to patient age (<70 years vs. ≥70 years) (Table 4). Univariate analysis identified that patient age was closely related to comorbidity (P < 0.001), incidence of postoperative complications (P = 0.052), and total in-patient costs (P < 0.001). A subsequent multivariate analysis revealed the independent factors associated with patient age to be comorbidity (CCI = 0 vs. CCI > 1) and total in-patient costs (medical cost <80% vs. ≥80%). Older patients (≥70 years) showed an almost 10 times greater relative risk for having a comorbidity (95% CI, 5.141–20.214; P < 0.001) and a 3.255 times greater relative risk for having higher total in-patient costs (95% CI, 1.731–6.119; P < 0.001).
Table 4. Univariate and multivariate analyses of preoperative and intraoperative factors related to patient age.
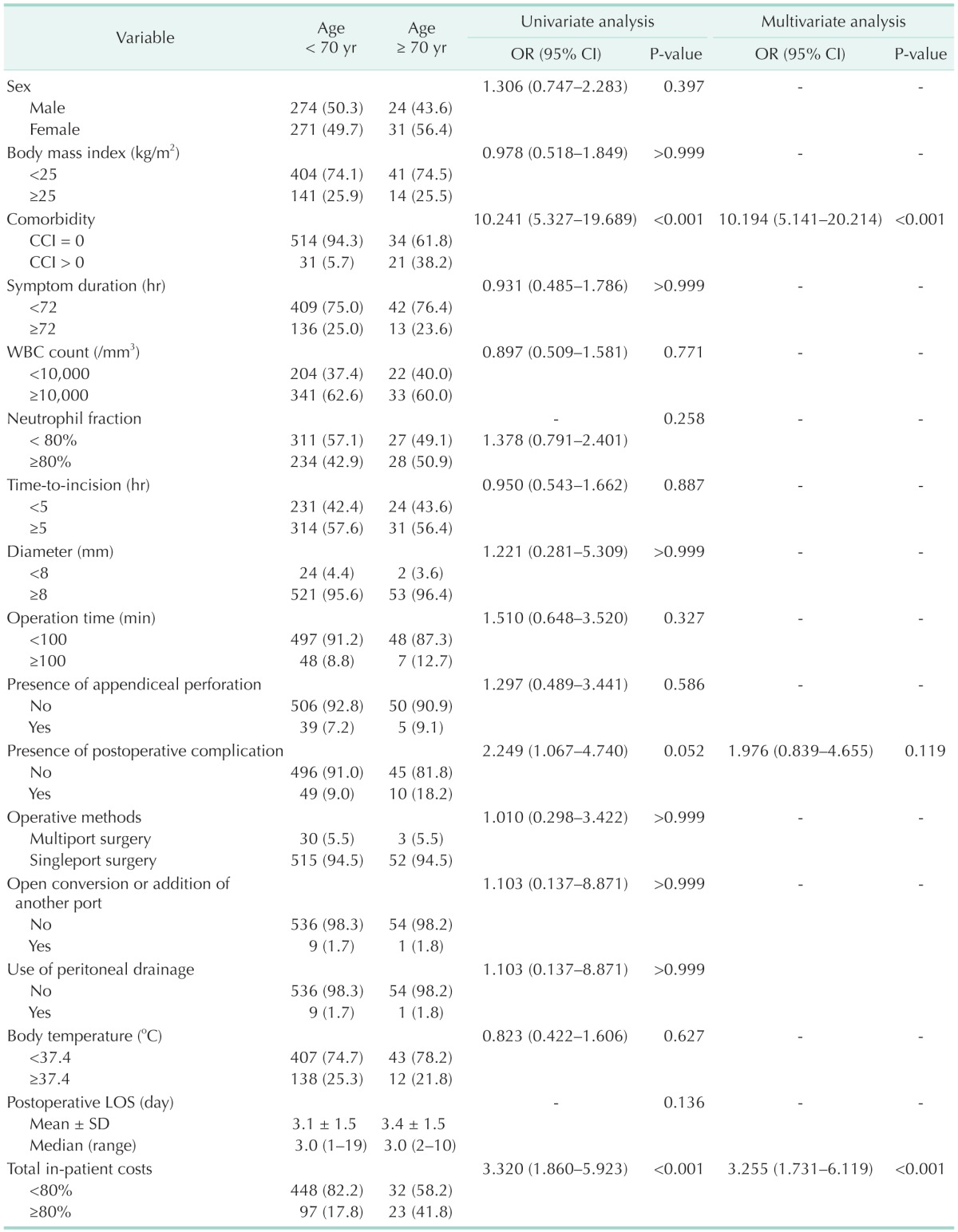
Values are presented as number (%) unless otherwise indicated.
OR, odds ratio; CI, confidential interval; CCI, Charlson's Comorbidity Index; LOS, length of hospital stay; SD, standard deviation.
DISCUSSION
This study shows the early outcomes of implementing a DRG-based payment system for appendicitis in Korea. Although implementing a DRG system for appendicitis significantly reduced postoperative LOS, it did not have an impact on the total in-hospital costs. The independent factors affecting total in-hospital costs included patient age (<70 years vs. ≥70 years), operation time (<100 minutes vs. ≥100 minutes), and postoperative LOS. In addition, older patients (≥70 years) exhibited both higher rate of comorbidity (CCI ≥ 1) and medical costs (medical cost ≥ 80%). Taken together, our results strongly suggest that patient age should be considered as a DRG classification variable, as it was found to be one of the most important determinants of medical costs.
In our study, the implementation of a DRG-based payment resulted in a significant reduction in postoperative LOS. However, we could not demonstrate other beneficial effects, (i.e., benefits in terms of operation time, incidence of postoperative complications, or total in-patient costs). The LOS-reducing effect of the DRG system could be attributed to the characteristics of DRGs that provide hospitals with incentive to reduce per patient costs. Our results are consistent with a previous report on Korean DRG-based payment for appendicitis [7]. Recently, Cheng et al. [1] conducted a study using a nationwide, population-based dataset to examine the impacts of the Taiwan DRG-based payment system for coronary artery bypass graft surgery or percutaneous transluminal coronary angioplasty. In their study, the introduction of a DRG payment system resulted in a 10% decrease in LOS, as well as a slight decrease in the intensity of care.
The Korean DRG system for appendicitis has 2 DRG classification categories (uncomplicated vs. complicated appendicitis). It is essential that a DRG category should have the patient groups which are sufficiently homogenous in terms of treatment costs. Otherwise, hospitals and surgeons who provide greater effort than others are not adequately paid for their efforts [3]. Thus, it should be investigated whether the Korean DRG system considers the most important determinants of resource consumption as its classification variables. Quentin et al. [3] provided a report of how DRG systems deal with cases of appendicitis in 11 European countries. Each country exhibited different DRG classification variables for appendicitis, ranging in number from 2 (Ireland) to 11 (Germany). In the European countries, the DRG classification variables were listed in descending order as follows: complications or comorbidities (7 countries), presence of appendiceal perforation (6 countries), patient age (3 countries), procedure (open or laparoscopic surgery) (2 countries), admission duration, inpatient or outpatient setting, extent of surgery, and mortality during admission (1 country).
Perforated appendicitis has long been considered a significant factor in medical costs due to its close relationship with (1) higher incidence of postoperative complications, (2) longer LOS, and (3) requirement for extended antibiotic coverage [8,9,10]. However, in our study, appendiceal perforation was not identified as a factor significantly affecting medical cost. We present several possible reasons for this. First, it is possible that the laparoscopic approach considerably counteracts the cost-raising effect of perforated appendicitis. Recently, as laparoscopic experience has accumulated, laparoscopy has been more frequently applied to patients with perforated appendicitis [11]. One study found that laparoscopic appendectomy had lower overall complication rates, shorter hospital LOS, lower 30-day readmission rate, and lower wound infection rate than open appendectomies for patients with perforated appendicitis, while maintaining comparable operative costs [11]. Therefore, the benefits of laparoscopic approach might counteract the cost-raising effects of perforated appendicitis. Second, we believe that this can also attributed to the recent reduction in long-standing perforated appendicitis. An improved socioeconomic status has made it possible for individuals to visit hospitals as soon as appendicitis develops. Thus, a prompt hospital visit could reduce the development of severely complicated appendicitis.
We found that older patients (≥70 years) have a 3.255 times greater relative risk for having higher total in-patient hospital costs (P < 0.001). In addition, older patients showed an almost 10 times greater relative risk for having a comorbidity (P < 0.001). Previous studies have found that older age is closely associated with preexisting comorbid conditions, higher rate of perforated appendicitis, and postoperative complications [12,13]. In an analysis of 106,929 appendectomy patients treated in the hospitals of 10 European countries, patient age and number of recorded diagnoses were identified as significant factors affecting both medical costs and LOS in all countries [2]. We also believe that older patients tend stay longer in hospitals due to concerns about their health and the absence of a fixed workplace to which a patient might return. Taken together, these results suggest that older patients undergoing appendectomy accrue significantly higher medical costs by requiring greater medical attention and having more comorbidities.
Our study has several limitations. Our study is limited by the small study population examined and also by the retrospective study design in a single institution. Retrospective nonrandomized design is, however, inevitable in the comparison of outcomes before and after implementing a system. Despite these limitations, our study is meaningful in that it provides an opportunity to reassess the Korean DRG classification variables. Our findings suggest that the current DRG classification variable, which is solely based on the presence of appendiceal perforation, needs for further refinement.
In conclusion, our study regarding the early experience of implementing a Korean DRG-based payment for appendicitis found that the DRG payment system leads to a reduction in postoperative LOS but not in total in-hospital costs. The independent factors related to higher total in-patient costs included patient age of 70 years or more, operation time longer than 100 minutes, and longer postoperative LOS. Because patient age was found to be one of the major cost-determining factors, our study suggests that patient age be considered as a DRG classification variable.
Footnotes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Cheng SH, Chen CC, Tsai SL. The impacts of DRG-based payments on health care provider behaviors under a universal coverage system: a population-based study. Health Policy. 2012;107:202–208. doi: 10.1016/j.healthpol.2012.03.021. [DOI] [PubMed] [Google Scholar]
- 2.Mason A, Or Z, Renaud T, Street A, Thuilliez J, Ward P, et al. How well do diagnosis-related groups for appendectomy explain variations in resource use? An analysis of patient-level data from 10 European countries. Health Econ. 2012;21(Suppl 2):30–40. doi: 10.1002/hec.2836. [DOI] [PubMed] [Google Scholar]
- 3.Quentin W, Scheller-Kreinsen D, Geissler A, Busse R EuroDRG group. Appendectomy and diagnosis-related groups (DRGs): patient classification and hospital reimbursement in 11 European countries. Langenbecks Arch Surg. 2012;397:317–326. doi: 10.1007/s00423-011-0877-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geissler A, Scheller-Kreinsen D, Quentin W EuroDRG group. Do diagnosis-related groups appropriately explain variations in costs and length of stay of hip replacement? A comparative assessment of DRG systems across 10 European countries. Health Econ. 2012;21(Suppl 2):103–115. doi: 10.1002/hec.2848. [DOI] [PubMed] [Google Scholar]
- 5.Ellis RP. Creaming, skimping and dumping: provider competition on the intensive and extensive margins. J Health Econ. 1998;17:537–555. doi: 10.1016/s0167-6296(97)00042-8. [DOI] [PubMed] [Google Scholar]
- 6.Martinussen PE, Hagen TP. Reimbursement systems, organisational forms and patient selection: evidence from day surgery in Norway. Health Econ Policy Law. 2009;4(Pt 2):139–158. doi: 10.1017/S1744133109004812. [DOI] [PubMed] [Google Scholar]
- 7.Kim H, Jung IM, Yun KW, Heo SC, Ahn YJ, Hwang KT, et al. Early outcome of the Korean Diagnosis-Related Groups payment system for appendectomy. Ann Surg Treat Res. 2015;88:126–132. doi: 10.4174/astr.2015.88.3.126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fukami Y, Hasegawa H, Sakamoto E, Komatsu S, Hiromatsu T. Value of laparoscopic appendectomy in perforated appendicitis. World J Surg. 2007;31:93–97. doi: 10.1007/s00268-006-0065-x. [DOI] [PubMed] [Google Scholar]
- 9.Masoomi H, Mills S, Dolich MO, Ketana N, Carmichael JC, Nguyen NT, et al. Comparison of outcomes of laparoscopic versus open appendectomy in adults: data from the Nationwide Inpatient Sample (NIS), 2006-2008. J Gastrointest Surg. 2011;15:2226–2231. doi: 10.1007/s11605-011-1613-8. [DOI] [PubMed] [Google Scholar]
- 10.Sleem R, Fisher S, Gestring M, Cheng J, Sangosanya A, Stassen N, et al. Perforated appendicitis: is early laparoscopic appendectomy appropriate? Surgery. 2009;146:731–737. doi: 10.1016/j.surg.2009.06.053. [DOI] [PubMed] [Google Scholar]
- 11.Lin HF, Lai HS, Lai IR. Laparoscopic treatment of perforated appendicitis. World J Gastroenterol. 2014;20:14338–14347. doi: 10.3748/wjg.v20.i39.14338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gürleyik G, Gürleyik E. Age-related clinical features in older patients with acute appendicitis. Eur J Emerg Med. 2003;10:200–203. doi: 10.1097/01.mej.0000088431.19737.f8. [DOI] [PubMed] [Google Scholar]
- 13.Lee JF, Leow CK, Lau WY. Appendicitis in the elderly. Aust N Z J Surg. 2000;70:593–596. doi: 10.1046/j.1440-1622.2000.01905.x. [DOI] [PubMed] [Google Scholar]