

Abstract
The evidence supporting the practice of dysplasia surveillance in inflammatory bowel disease (IBD) has remained sparse, and optimal detection strategies are still lacking. These issues, added to the declining incidence of dysplasia in IBD, have led to much debate over the diagnosis and management of dysplasia. White-light endoscopy with targeted and random biopsies remains the technique of choice for most practicing gastroenterologists. However, during the past decade, a surge of literature has questioned the efficacy of this strategy. Simultaneously, chromoendoscopy has emerged as an alternative, and perhaps superior, technique that has been included in some society guidelines. Nevertheless, many issues remain unclear, such as the best way to implement chromoendoscopy into everyday practice, whether there are any outcome benefits that can be attributed to the use of chromoendoscopy, and, perhaps most importantly, how to manage dysplasia uncovered by this and other advanced techniques. In this article, we discuss the various techniques currently available for dysplasia surveillance in IBD, with a focus on chromoendoscopy. Additionally, we highlight the overarching issues of setting appropriate endpoints and individualizing the care of patients with long-standing colitis.
Keywords: Chromoendoscopy, dysplasia, inflammatory bowel disease, Crohn’s disease, ulcerative colitis
Inflammatory bowel disease (IBD), which includes ulcerative colitis (UC) and Crohn’s disease, is associated with an increased risk of colorectal cancer (CRC).1,2 CRC in IBD likely stems from chronic inflammation of the colonic mucosa, which leads to carcinogenesis through a stepwise progression from inflammation to dysplasia to carcinoma.3 This concept of carcinogenesis, however, appears to be the only near certainty that decades of research have yielded with regard to CRC in IBD. The degree to which cancer risk is increased, the efficacy of various preventative strategies, and the appropriate management of colitis-associated dysplasia and cancer all remain topics of interest. In this article, we focus on current dysplasia surveillance practices in IBD.
Colorectal Cancer in Inflammatory Bowel Disease: Risk and Prevention
Reexamining the Colorectal Cancer Risk in Inflammatory Bowel Disease
In 2001, Eaden and colleagues published a pivotal meta-analysis in which the cumulative risk of CRC in patients with UC was estimated to be 2% at 10 years, 8% at 20 years, and 18% at 30 years of disease duration.1 In recent years, population-based studies of unselected cohorts have shown that these early estimates of CRC risk in UC were likely exaggerated.4-8 A recent meta-analysis of population-based studies by Jess and colleagues showed that CRC was diagnosed in an average of 1.6% of patients with UC during 14 years of follow-up, corresponding to a 2.4-fold (95% CI, 2.1-2.7) increased risk compared with risk in the general population.9 In this analysis, the absolute cumulative risk of CRC in UC was 1.15% after 15 years, 1.69% after 20 years, and 2.61% after 25 years of disease duration, significantly lower than the risk stated in the report of Eaden and colleagues from the previous decade.1 An association between CRC and colonic Crohn’s disease has also been established. A meta-analysis by Canavan and colleagues showed an increased risk of CRC in patients with Crohn’s colitis (relative risk [RR], 4.5; 95% CI, 1.3-14.9) but not in patients with ileal disease (RR, 1.1; 95% CI, 0.8-1.5).2
Recent data not only have mitigated the fear of CRC in patients with IBD but also have provided a better understanding of the strata of patients at highest risk. The influence of disease extent on CRC risk in IBD has been demonstrated by several investigators.6,10,11 A meta-analysis by Lutgens and colleagues found that the overall risk of CRC in IBD appears to be driven largely by patients with extensive colitis (standardized incidence ratio [SIR], 6.4; 95% CI, 2.4-17.5), whereas the overall risk in all patients with UC is significantly lower (SIR, 1.7; 95% CI, 1.2-2.2).12 The effect of disease duration on CRC risk was demonstrated in a large population-based study showing that the risk of CRC is markedly greater in patients with a UC diagnosis in childhood or adolescence (RR, 43.8; 95% CI, 27.2-70.7) than in those with a diagnosis in late adulthood (RR, 0.76; 95% CI, 0.62-0.92).13 These findings indicate that a longer duration of inflammation promotes carcinogenesis, a concept supported by studies demonstrating that the severity of both macroscopic and histologic inflammation is strongly associated with dysplasia and CRC in patients with UC.14,15 Concomitant primary sclerosing cholangitis (PSC) has also proved to be a significant risk factor, as demonstrated by a meta-analysis in which patients with UC and PSC had a 4.8-fold (95% CI, 3.6-6.4) increased risk of CRC in comparison with UC patients without PSC.16 Other significant risk factors include a family history of CRC,17 extensive pseudopolyposis, and colonic strictures.18
However, even after all of the known risk factors have been taken into account, a history of prior dysplasia is the most reliable clinical predictor of future CRC risk in patients with IBD.19 It has been demonstrated that dysplasia is present in the colon in more than 90% of patients with UC undergoing colectomy for carcinoma and that dysplasia can occur at the site of the cancer as well as in areas of the colon distant from the cancer.20,21 Thus, a history of dysplasia has the greatest weight in decisions regarding surveillance and management in patients with IBD.
Rationale and Evidence for Dysplasia Surveillance in Inflammatory Bowel Disease
The backbone of CRC prevention in IBD has been and remains colonoscopic screening and surveillance, a practice that aims to identify neoplasia at an early stage, prevent progression to advanced dysplasia and cancer, and decrease CRC-related morbidity and mortality. These goals are accomplished through lesion removal at the time of colonoscopy or through colectomy if lesion removal is not feasible. Thus, periodic dysplasia surveillance via colonoscopy is considered the standard of care for all patients with long-standing UC or Crohn’s colitis.22-24 However, it should be noted that retrospective observational data, rather than randomized controlled trials, provide only indirect and quite limited evidence supporting the practice of dysplasia surveillance. In a retrospective case-control study, Karlén and colleagues found that having undergone a surveillance colonoscopy was associated with a decreased risk of death from CRC in patients with longstanding UC, although the difference was not statistically significant.25 Two other retrospective studies assessing various risk factors for CRC in IBD also found that having undergone colonoscopic surveillance decreased the risk of CRC.26,27 A retrospective analysis of a large pathology database found that 5-year CRC-related survival rates were better in patients with IBD and a diagnosis of CRC who had undergone surveillance than in similar patients in a nonsurveillance group (100% vs 74%; P=.042). The mortality benefit was derived mostly from the finding that the tumors of patients who underwent surveillance were discovered at significantly earlier stages.28
Dysplasia Surveillance Strategies in Inflammatory Bowel Disease: Past and Present
Based on the preceding data suggesting that surveillance detects CRC at earlier stages and leads to a mortality benefit, and in the absence of a superior tool for distinguishing high-risk from lower-risk subpopulations, patients who have IBD with long-standing, extensive colitis are enrolled in colonoscopic surveillance programs. However, although the practice of colonoscopic surveillance is widely accepted, its specific implementation has been a controversial issue. This is perhaps because a comparison of the survival of patients with cancers detected by surveillance and the survival of patients with symptomatic cancers or cancers detected through other, nonsurveillance-based means is a flawed comparison; it is not a true comparison of all patients undergoing surveillance and those at equal risk but who are not undergoing surveillance.
White-Light Endoscopy and Random Biopsies: Tried and True?
Traditionally, surveillance protocols have involved annual or biennial colonoscopy beginning 8 to 10 years after diagnosis among patients with left-sided or more extensive disease. The examination consists of a thorough white-light inspection of the mucosa, resection or biopsy of any suspicious lesions, and nontargeted 4-quadrant biopsies in every 10-cm segment of the colon.21 The rationale for nontargeted biopsies is based on the observation that dysplastic lesions in IBD may be flat and thus difficult, or impossible, to detect. It has been estimated that taking between 33 and 64 random biopsy specimens at colonoscopy can achieve 90% to 95% sensitivity for dysplasia detection in the mucosa of a patient with UC.29 This practice is endorsed in most current society guidelines.21,22,24
Although nontargeted biopsies are recommended to uncover “invisible” dysplasia, it is now accepted that most dysplasia in IBD is in fact detectable with the use of modern white-light endoscopy (WLE) equipment.30,31 Several studies have shown that, in addition to detecting clinically important dysplastic foci, endoscopy provides safe and effective management of lesions with good long-term outcomes, provided that aggressive surveillance is continued.32-35 The advent of high-definition (HD), or high-resolution, colonoscopy has further improved the quality of white-light examinations. This was demonstrated in a retrospective cohort of patients with UC or Crohn’s colitis in which HD-WLE was found to significantly improve dysplasia detection compared with standard WLE (adjusted prevalence ratio, 2.99; 95% CI, 1.16-7.79).36
Although it has been difficult to gauge the efficacy of traditional surveillance practices in terms of a mortality benefit, it appears that the incidence of CRC in patients with IBD is declining, although the mechanism responsible for this decline remains uncertain. In 2 large population-based studies, the incidence of CRC in patients with IBD was found to have declined over the past 40 years.10,13 Notably, the risk of death from CRC also declined during the same time period.10,37 Although the reasons for these trends may not be clear, a leading hypothesis is that the broad implementation of surveillance programs with improved optics may be responsible for the decline. Based on available data, WLE remains a cornerstone of dysplasia surveillance in IBD.
Limitations of the Random Biopsy Protocol: Time to Put Away the Biopsy Forceps?
Current surveillance practices are imperfect, in part because of the ineffectiveness and inefficiency of the random biopsy protocol. Obtaining upward of 30 biopsy specimens per colonoscopy is time-consuming and expensive. In fact, surveys of large numbers of gastroen-terologists as well as observational data in surveillance systems without protocols have demonstrated poor rates of adherence to these guidelines.20,38 Even if the requisite number of biopsy specimens were obtained in practice, the amount of colonic tissue sampled would constitute only a very small fraction of the available colonic mucosa—making this practice similar to finding a needle in a haystack.
The yield and clinical significance of random biopsies were illustrated in an analysis by van den Broek and col-leagues.39 The investigators reviewed data from 475 patients with UC who underwent 1010 colonoscopies and a total of 11,772 random biopsies (median, 29 per colonoscopy) over a 10-year period. Dysplasia was detected in random biopsy specimens alone in 5 colonoscopies (0.5%) in 4 patients (0.8%). Of these 4 patients, 2 had had visible dysplasia in previous colonoscopies, 1 had unifocal low-grade dysplasia that was not confirmed in 3 subsequent colonoscopies, and 1 had multifocal low-grade dysplasia and suspicious-appearing ulcerations and underwent proctocolectomy, which confirmed the presence of neoplasia. Thus, dysplasia uncovered via random biopsy changed the management of only 1 of 475 patients (0.2%). In comparison, targeted biopsy specimens were positive for neoplasia in 83 colonoscopies (8.2%), and major therapeutic decisions (endo-scopic resection or colectomy) were made in 61 of these cases (73%). Whether random biopsies should be abandoned as a surveillance tool in patients with IBD remains debated. However, these data, as well as similar findings from other studies, suggest that “invisible” dysplasia is rare in IBD and has limited clinically relevant consequences. It is also assumed that the yield of dysplasia is the outcome of interest. Physicians should always remember that reducing CRC morbidity and mortality is the goal of surveillance.
Chromoendoscopy: The Holy Grail of Surveillance in Inflammatory Bowel Disease?
A major advance in IBD dysplasia surveillance over the past decade has been the introduction of chromoen-doscopy into clinical practice and society guidelines. In chromoendoscopy, the topical application of dye to the colonic mucosa enhances the detection and delineation of surface abnormalities. The 2 dye agents most commonly used are methylene blue and indigo carmine. Because the dyes are taken up differently by normal colonocytes and inflamed or neoplastic colonic mucosa, the pit patterns of the colonic surface are highlighted and the borders of mucosal lesions demarcated (Figure 1). These agents are applied to the entire colonic mucosa with a spray catheter or the water jet channel of a standard colonoscope, and inspection is possible within minutes of application.
Figure 1.
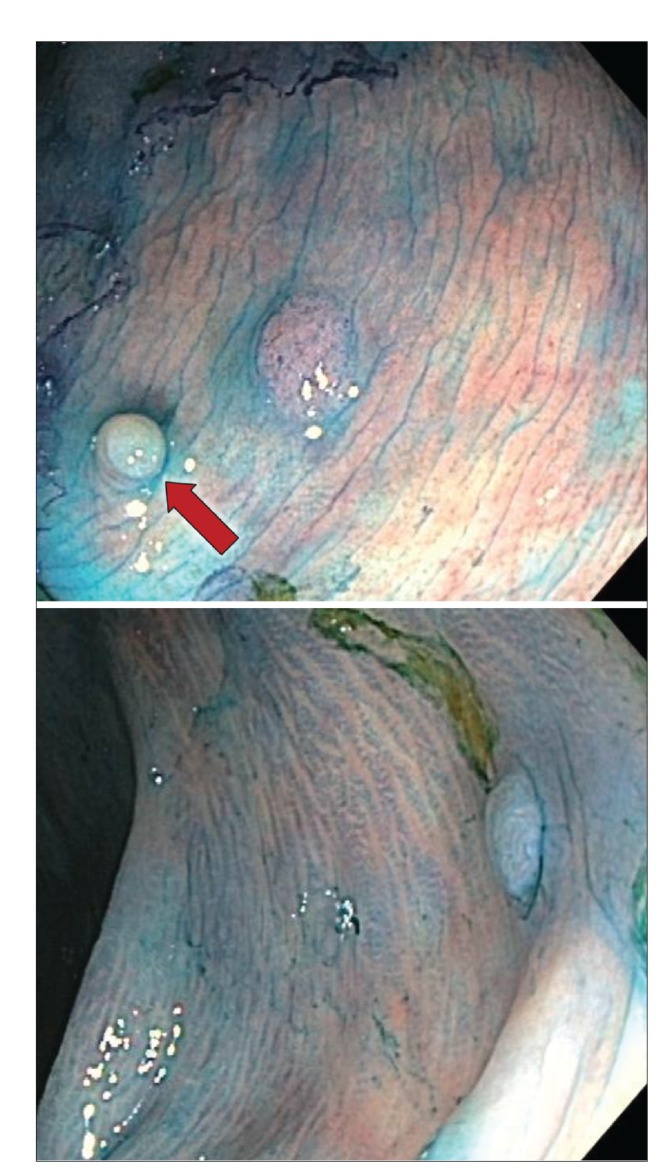
Chromoendoscopic images of a patient with longstanding, extensive ulcerative colitis, in whom methylene blue was applied to detect small sessile polyps with a cerebriform pit pattern, which were treated via complete endoscopic resection. Histologic examination of the polyps revealed low-grade dysplasia. A small pseudopolyp with a normal-appearing surface pattern was also noted (arrow).
To date, 6 prospective cross-sectional trials have assessed chromoendoscopy as a “red flag” technology for the detection of dysplasia in IBD.40-45 The results of all of the studies have favored chromoendoscopy in comparison with WLE, with an approximately 2- to 3-fold increase in dysplasia detection per patient and a 4- to 5-fold increase per lesion. A meta-analysis of the results of the chromoendoscopy trials yielded an overall difference in dysplasia detection between chromoendoscopy and WLE of 7% (95% CI, 3.2-11.3) on a per-patient basis, with a number needed to treat of 14.3. Of note, the increase in the diagnosis of flat dysplastic lesions (as defined by the Paris classification46) using chromoendoscopy over WLE with nontargeted biopsies was 27% (95% CI, 11.2-41.9).47 The overwhelmingly positive chromoendoscopy data have caused a shift in dysplasia surveillance recommendations. The latest British Society of Gastroenterology practice guidelines endorse chromoendoscopy as the preferred dysplasia surveillance modality, and the American Gastroenterological Association guidelines consider chromoendoscopy an acceptable alternative to random biopsies in expert centers.21,22
In addition to increasing the dysplasia yield, chromoendoscopy may also lower costs and decrease procedure time by obviating the need for nontargeted biopsies. Although the implementation of chromoendoscopy requires special training, there are published data suggesting that even among inexperienced endoscopists, chromoendoscopy results in high rates of interobserver agreement for polyp detection, acceptable withdrawal times, and enhanced dysplasia detection.48 With respect to safety, some investigators have suggested that methylene blue may cause DNA damage in colonocytes, although this remains a hypothetical risk with unclear clinical relevance.49,50
Should the Enthusiasm for Chromoendoscopy Be Restrained?
Although the chromoendoscopy literature is certainly enticing, several issues should give pause to gastroenterologists who are considering whether to adopt this technique as their first choice for dysplasia surveillance. First, all 6 of the previously referenced trials were carried out in expert centers. Although general gastroenterologists can learn chromoendoscopy techniques, it is unlikely that every endoscopist can obtain the experience and expertise necessary to achieve results akin to those reported in the literature. Second, although chromoendoscopy certainly detects more lesions, it is unclear if this increase in detection will result in a CRC morbidity or mortality benefit. There are no longitudinal data showing that chromoendoscopy reduces cancer-related morbidity or mortality. Simply finding more dysplastic lesions may not be the best measure of the quality or clinical impact of a method of surveillance. Finally, the nature of the dysplasia detected with chromoendoscopy is unknown. Detecting lesions whose clinical consequences are uncertain may lead to an increase in unwarranted colectomies and anxiety among both patients and gastroenterologists. This may also cause the phenomenon of stage migration, in which the finding of lower-stage lesions of little or no clinical consequence leads to treatment and perceived improvement in survival in a group of patients in the absence of a true benefit.51
There is no debate that chromoendoscopy finds as many lesions as its predecessor, or more, while requiring fewer biopsies, incurring less expense, and lowering the workload of endoscopists. However, it is unclear whether these are ideal outcome measures. The lack of longitudinal data and evidence of a cancer-related mortality benefit should prompt further study of the true value of chromoendoscopy.
Virtual Chromoendoscopy Systems
Our understanding of the epidemiology and biology of neoplasia in IBD has evolved parallel to the growing sophistication of our endoscopic skill and equipment. Not surprisingly, the success of chromoendoscopy has led investigators to search for new technologies with similar efficacy but without the need for dye spray, which entails expense and is a nuisance to both endoscopy team members and the laundry services that support them. Several platforms have been investigated for this purpose.
Narrow-band imaging (NBI) is a technology that uses specialized light filters to modulate the intensity of the constituents of the white-light spectrum, allowing it to highlight vascular and mucosal architecture.52 NBI has been studied as a tool for dysplasia detection in IBD, but the results have been disappointing. In 3 prospective, randomized studies, no significant difference was found between the dysplasia yield of NBI and that of WLE.52-54 In one comparison study with chromoendoscopy, a higher rate of missed lesions was found when NBI was used.55
The 2 other virtual chromoendoscopy systems that are currently available are Fuji Intelligent Chromoendoscopy (FICE; Fujinon) and i-scan (Pentax). These systems differ from NBI in that they use a postprocessing computer algorithm that modifies a white-light image after it is captured.56 Although no clinical trials have assessed the utility of FICE or i-scan for dysplasia detection in IBD, these modalities have been investigated as tools for polyp detection in average-risk populations. In 3 studies comparing FICE with WLE, HD-WLE, or chromoendoscopy, no difference was found in the adenoma detection rates.57-59 On the other hand, a large prospective trial comparing i-scan with WLE for adenoma detection in average-risk patients found a 3-fold increase in the number of neoplastic lesions detected when i-scan was used.60 These technologies are still developing, and prospective studies are needed to assess the efficacy of FICE and i-scan in an IBD cohort.
Autofluorescence imaging (AFI) uses differences in the emission spectra of tissues to construct chromoendoscopy-like images. After the administration of a photosensitizing agent, the emission spectra of normal, inflamed, hyperplastic, and adenomatous mucosa differ, allowing AFI to act as a surveillance tool.56 In several well-designed studies investigating its role in IBD dysplasia surveillance, AFI has shown to be a highly sensitive modality with a low miss rate for dysplasia and a high negative predictive value.61-63 However, owing to numerous practical and technical limitations, AFI remains restricted to specialized referral centers.
Future Directions and Recommendations for Surveillance in Inflammatory Bowel Disease
Redefining the Endpoints
In the coming years, the realm of IBD-related CRC will become increasingly complex as our understanding of the biology of dysplasia and the technology used to detect it continue to develop. Nonetheless, the ultimate goals in caring for patients with IBD will remain unchanged. These include, first and most importantly, preventing CRC-related morbidity and mortality; second, avoiding unnecessary colectomies in patients with clinically insignificant lesions; third, decreasing patient burden by minimizing the number of procedures and the associated emotional turmoil; and finally, from the perspective of resource utilization, improving the efficiency and minimizing the expense of surveillance and treatment.
These goals should not be overlooked by clinicians and researchers evaluating dysplasia surveillance practices. Although effective and efficient dysplasia detection is a crucial element of surveillance, it is not the paramount outcome measure. Prospective studies are needed to assess whether HD-WLE, traditional chromoendoscopy, and virtual chromoendoscopy achieve more rigorous clinical endpoints—namely, lowering CRC-related morbidity and mortality. Additionally, longitudinal data are needed on the natural history of dysplasia uncovered and resected by means of advanced techniques because a better understanding of the clinical significance of such lesions will help avoid unnecessary colectomies. From the standpoint of practicality and health care economics, it has not yet been shown that the expenses incurred in adopting advanced techniques and in training endoscopists will be outweighed by cost savings of the techniques. Increasing the interval between surveillance examinations owing to the higher false-negative rate of chromoendoscopy may prove to be the true gain for advanced technologies. Before adopting a new set of standards and guidelines, along with changes in training and equipment purchasing, national societies would be wise to consider these variables.
Individualizing Care
In the era of personalized medicine, the “one size fits all” concept will be abandoned, and diagnostic tests and therapies will be tailored to individual patients. With respect to dysplasia surveillance in IBD, this concept has started to take hold. For instance, an understanding of the risk factors for dysplasia, including long-standing colitis, extensive disease, and PSC, has influenced surveillance practices. The current American Gastroenterological Association guidelines recommend that clinicians consider the presence of high-risk features when deciding on surveillance intervals.21 Similarly, the British Society of Gastroenterology guidelines recommend classifying patients into groups of lower, intermediate, and higher risk based on the presence of recognized risk factors and endoscopic findings, moving to a more individualized surveillance practice.22 It should be noted, however, that these recommendations are based on expert opinion in the absence of clinical trials or even observational data (Figure 2).
Figure 2.

An algorithm for the surveillance of dysplasia in patients with inflammatory bowel disease.
a If expertise in CE is available. Note that CE requires excellent bowel preparation and close inspection of mucosal segments with inflammation, pseudopolyps, and scarring.
b If expertise in CE is not available, referral to an expert center should be considered.
CE, chromoendoscopy; HD-WLE, high-definition white-light endoscopy; PSC, primary sclerosing cholangitis.
It may be reasonable to apply a more individualized approach in deciding on the appropriate dysplasia surveillance modality for any given patient. For instance, high-risk patients may be referred for chromoendoscopy at expert centers. Patients at highest risk for CRC, those with a history of dysplasia or extremely long-standing pancolitis, may benefit from a multiple surveillance approach that combines various modalities. Of note, although nontargeted biopsies have been shown to be less effective in detecting dysplasia in patients with IBD, there is evidence that they may help detect “invisible” lesions in patients with UC and concomitant PSC.64 Clinicians may therefore consider using both dye spray and nontargeted biopsies in such patients, which has been described as a belt-and-suspenders strategy by some. Likewise, if dysplasia is uncovered, treatment options can be tailored based on the individual patient’s risk for synchronous and metachronous lesions.
The Current Role of Chromoendoscopy
Chromoendoscopy has shown to be effective and efficient at detecting IBD-related dysplasia. In expert hands, it significantly improves the yield of dysplasia detection in comparison with WLE with random biopsies. Gastro-enterologists who are trained in chromoendoscopy and perform a sufficient volume of surveillance examinations should incorporate this technique into their practice based on available evidence and recent guidelines.21,22 However, as previously outlined, many issues remain unclear, including the long-term implications of dysplasia uncovered with chromoendoscopy and whether chromoendoscopy provides a mortality or morbidity benefit. Ultimately, the most effective surveillance examination is one that is performed thoroughly, conscientiously, and in a timely manner. Thus, if a physician is more adept at WLE and performs the examination well, perhaps this would benefit his or her patients most.
Limitations of Dysplasia Surveillance
Whichever mode or interval of surveillance is chosen, the patient and gastroenterologist must be aware of the inherent limitations of colonoscopic dysplasia surveillance. First, a greater degree of inflammation and the presence of pseudopolyposis or strictures may limit the effectiveness of surveillance with or without any adjunctive technique. Second, it has been recognized that some CRC in IBD arises directly from low-grade lesions, making early detection difficult or impossible.65 Third, the expertise of gastroenterologists may vary widely with regard to their ability to recognize colitis-associated lesions, perform chromoendoscopy, adequately resect polyps, and adhere to surveillance guidelines.66 Fourth, and perhaps most importantly, any program depends on the patient’s and the endoscopist’s commitment and willingness to adhere to recommended surveillance intervals.67 Finally, if dysplasia is discovered, patients must be open to the possibility of colectomy as a treatment option. There are data suggesting that, although patients with UC understand their risk of CRC and undergo surveillance, they may not be prepared to follow recommendations for elective colectomy if dysplasia is found.68 In the coming years, we anticipate studies that will reveal the true clinical utility of adjunctive surveillance, whether with dye spray and chromoendoscopic techniques or with another emerging technique.
Footnotes
The authors have no relevant conflicts of interest to disclose.
References
- 1.Eaden JA, Abrams KR, Mayberry JF. The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut. 2001;48(4):526–535. doi: 10.1136/gut.48.4.526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Canavan C, Abrams KR, Mayberry J. Meta-analysis: colorectal and small bowel cancer risk in patients with Crohn’s disease. Aliment Pharmacol Ther. 2006;23(8):1097–1104. doi: 10.1111/j.1365-2036.2006.02854.x. [DOI] [PubMed] [Google Scholar]
- 3.Ullman TA, Itzkowitz SH. Intestinal inflammation and cancer. Gastroenterology. 2011;140(6):1807–1816. doi: 10.1053/j.gastro.2011.01.057. [DOI] [PubMed] [Google Scholar]
- 4.Bernstein CN, Blanchard JF, Kliewer E, Wajda A. Cancer risk in patients with inflammatory bowel disease: a population-based study. Cancer. 2001;91(4):854–862. doi: 10.1002/1097-0142(20010215)91:4<854::aid-cncr1073>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 5.Lakatos L, Mester G, Erdelyi Z, et al. Risk factors for ulcerative colitis-associated colorectal cancer in a Hungarian cohort of patients with ulcerative colitis: results of a population-based study. Inflamm Bowel Dis. 2006;12(3):205–211. doi: 10.1097/01.MIB.0000217770.21261.ce. [DOI] [PubMed] [Google Scholar]
- 6.Jess T, Loftus EV, Jr, Velayos FS, et al. Risk of intestinal cancer in inflammatory bowel disease: a population-based study from Olmsted County, Minnesota. Gastroenterology. 2006;130(4):1039–1046. doi: 10.1053/j.gastro.2005.12.037. [DOI] [PubMed] [Google Scholar]
- 7.Winther KV, Jess T, Langholz E, Munkholm P, Binder V. Long-term risk of cancer in ulcerative colitis: a population-based cohort study from Copenhagen County. Clin Gastroenterol Hepatol. 2004;2(12):1088–1095. doi: 10.1016/s1542-3565(04)00543-9. [DOI] [PubMed] [Google Scholar]
- 8.Jess T, Horvàth-Puhó E, Fallingborg J, Rasmussen HH, Jacobsen BA. Cancer risk in inflammatory bowel disease according to patient phenotype and treatment: a Danish population-based cohort study. Am J Gastroenterol. 2013;108(12):1869–1876. doi: 10.1038/ajg.2013.249. [DOI] [PubMed] [Google Scholar]
- 9.Jess T, Rungoe C, Peyrin-Biroulet L. Risk of colorectal cancer in patients with ulcerative colitis: a meta-analysis of population-based cohort studies. Clin Gastroenterol Hepatol. 2012;10(6):639–645. doi: 10.1016/j.cgh.2012.01.010. [DOI] [PubMed] [Google Scholar]
- 10.Söderlund S, Brandt L, Lapidus A, et al. Decreasing time-trends of colorectal cancer in a large cohort of patients with inflammatory bowel disease. Gastroenterology. 2009;136(5):1561–1567. doi: 10.1053/j.gastro.2009.01.064. quiz 1818-1819. [DOI] [PubMed] [Google Scholar]
- 11.Beaugerie L, Svrcek M, Seksik P, et al. Risk of colorectal high-grade dysplasia and cancer in a prospective observational cohort of patients with inflammatory bowel disease. Gastroenterology. 2013;145(1):166–175.e8. doi: 10.1053/j.gastro.2013.03.044. [DOI] [PubMed] [Google Scholar]
- 12.Lutgens MW, van Oijen MG, van der Heijden GJ, Vleggaar FP, Siersema PD, Oldenburg B. Declining risk of colorectal cancer in inflammatory bowel disease: an updated meta-analysis of population-based cohort studies. Inflamm Bowel Dis. 2013;19(4):789–799. doi: 10.1097/MIB.0b013e31828029c0. [DOI] [PubMed] [Google Scholar]
- 13.Jess T, Simonsen J, Jørgensen KT, Pedersen BV, Nielsen NM, Frisch M. Decreasing risk of colorectal cancer in patients with inflammatory bowel disease over 30 years. Gastroenterology. 2012;143(2):375–381.e1. doi: 10.1053/j.gastro.2012.04.016. quiz e13-e14. [DOI] [PubMed] [Google Scholar]
- 14.Rutter M, Saunders B, Wilkinson K, et al. Severity of inflammation is a risk factor for colorectal neoplasia in ulcerative colitis. Gastroenterology. 2004;126(2):451–459. doi: 10.1053/j.gastro.2003.11.010. [DOI] [PubMed] [Google Scholar]
- 15.Nieminen U, Jussila A, Nordling S, Mustonen H, Färkkilä MA. Inflammation and disease duration have a cumulative effect on the risk of dysplasia and carcinoma in IBD: a case-control observational study based on registry data. Int J Cancer. 2014;134(1):189–196. doi: 10.1002/ijc.28346. [DOI] [PubMed] [Google Scholar]
- 16.Soetikno RM, Lin OS, Heidenreich PA, Young HS, Blackstone MO. Increased risk of colorectal neoplasia in patients with primary sclerosing cholangitis and ulcerative colitis: a meta-analysis. Gastrointest Endosc. 2002;56(1):48–54. doi: 10.1067/mge.2002.125367. [DOI] [PubMed] [Google Scholar]
- 17.Askling J, Dickman PW, Karlé P, et al. Family history as a risk factor for colorectal cancer in inflammatory bowel disease. Gastroenterology. 2001;120(6):1356–1362. doi: 10.1053/gast.2001.24052. [DOI] [PubMed] [Google Scholar]
- 18.Rutter MD, Saunders BP, Wilkinson KH, et al. Cancer surveillance in longstanding ulcerative colitis: endoscopic appearances help predict cancer risk. Gut. 2004;53(12):1813–1816. doi: 10.1136/gut.2003.038505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bernstein CN, Shanahan F, Weinstein WM. Are we telling patients the truth about surveillance colonoscopy in ulcerative colitis? Lancet. 1994;343(8889):71–74. doi: 10.1016/s0140-6736(94)90813-3. [DOI] [PubMed] [Google Scholar]
- 20.Ullman T, Croog V, Harpaz N, Sachar D, Itzkowitz S. Progression of flat lowgrade dysplasia to advanced neoplasia in patients with ulcerative colitis. Gastroenterology. 2003;125(5):1311–1319. doi: 10.1016/j.gastro.2003.08.023. [DOI] [PubMed] [Google Scholar]
- 21.Farraye FA, Odze RD, Eaden J, Itzkowitz SH. AGA technical review on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease. Gastroenterology. 2010;138(2):746–774-774.e1-4;. doi: 10.1053/j.gastro.2009.12.035. quiz e12-e13. [DOI] [PubMed] [Google Scholar]
- 22.Cairns SR, Scholefield JH, Steele RJ, et al. British Society of Gastroenterology; Association of Coloproctology for Great Britain and Ireland. Guidelines for colorectal cancer screening and surveillance in moderate and high risk groups (update from 2002) Gut. 2010;59(5):666–689. doi: 10.1136/gut.2009.179804. [DOI] [PubMed] [Google Scholar]
- 23.Farraye FA, Odze RD, Eaden J, et al. AGA Institute Medical Position Panel on Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease. AGA medical position statement on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease. Gastroenterology. 2010;138(2):738–745. doi: 10.1053/j.gastro.2009.12.037. [DOI] [PubMed] [Google Scholar]
- 24.Kornbluth A, Sachar DB. Practice Parameters Committee of the American College of Gastroenterology. Ulcerative colitis practice guidelines in adults: American College Of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol. 2010;105(3):501–523. doi: 10.1038/ajg.2009.727. [DOI] [PubMed] [Google Scholar]
- 25.Karlén P, Kornfeld D, Broström O, Löfberg R, Persson PG, Ekbom A. Is colo-noscopic surveillance reducing colorectal cancer mortality in ulcerative colitis? A population based case control study. Gut. 1998;42(5):711–714. doi: 10.1136/gut.42.5.711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Velayos FS, Loftus EV, Jr, Jess T, et al. Predictive and protective factors associated with colorectal cancer in ulcerative colitis: a case-control study. Gastroenterology. 2006;130(7):1941–1949. doi: 10.1053/j.gastro.2006.03.028. [DOI] [PubMed] [Google Scholar]
- 27.Eaden J, Abrams K, Ekbom A, Jackson E, Mayberry J. Colorectal cancer prevention in ulcerative colitis: a case-control study. Aliment Pharmacol Ther. 2000;14(2):145–153. doi: 10.1046/j.1365-2036.2000.00698.x. [DOI] [PubMed] [Google Scholar]
- 28.Lutgens MW, Oldenburg B, Siersema PD, et al. Colonoscopic surveillance improves survival after colorectal cancer diagnosis in inflammatory bowel disease. Br J Cancer. 2009;101(10):1671–1675. doi: 10.1038/sj.bjc.6605359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Rubin CE, Haggitt RC, Burmer GC, et al. DNA aneuploidy in colonic biopsies predicts future development of dysplasia in ulcerative colitis. Gastroenterology. 1992;103(5):1611–1620. doi: 10.1016/0016-5085(92)91185-7. [DOI] [PubMed] [Google Scholar]
- 30.Rutter MD, Saunders BP, Wilkinson KH, Kamm MA, Williams CB, Forbes A. Most dysplasia in ulcerative colitis is visible at colonoscopy. Gastrointest Endosc. 2004;60(3):334–339. doi: 10.1016/s0016-5107(04)01710-9. [DOI] [PubMed] [Google Scholar]
- 31.Rubin DT, Rothe JA, Hetzel JT, Cohen RD, Hanauer SB. Are dysplasia and colorectal cancer endoscopically visible in patients with ulcerative colitis? Gastrointest Endosc. 2007;65(7):998–1004. doi: 10.1016/j.gie.2006.09.025. [DOI] [PubMed] [Google Scholar]
- 32.Rubin PH, Friedman S, Harpaz N, et al. Colonoscopic polypectomy in chronic colitis: conservative management after endoscopic resection of dysplastic polyps. Gastroenterology. 1999;117(6):1295–1300. doi: 10.1016/s0016-5085(99)70279-9. [DOI] [PubMed] [Google Scholar]
- 33.Odze RD, Farraye FA, Hecht JL, Hornick JL. Long-term follow-up after polypectomy treatment for adenoma-like dysplastic lesions in ulcerative colitis. Clin Gastroenterol Hepatol. 2004;2(7):534–541. doi: 10.1016/s1542-3565(04)00237-x. [DOI] [PubMed] [Google Scholar]
- 34.Kisiel JB, Loftus EV, Jr, Harmsen WS, Zinsmeister AR, Sandborn WJ. Outcome of sporadic adenomas and adenoma-like dysplasia in patients with ulcerative colitis undergoing polypectomy. Inflamm Bowel Dis. 2012;18(2):226–235. doi: 10.1002/ibd.21687. [DOI] [PubMed] [Google Scholar]
- 35.Wanders LK, Dekker E, Pullens B, Bassett P, Travis SP, East JE. Cancer risk after resection of polypoid dysplasia in patients with longstanding ulcerative colitis: a meta-analysis. Clin Gastroenterol Hepatol. 2014;12(5):756–764. doi: 10.1016/j.cgh.2013.07.024. [DOI] [PubMed] [Google Scholar]
- 36.Subramanian V, Ramappa V, Telakis E, et al. Comparison of high definition with standard white light endoscopy for detection of dysplastic lesions during surveillance colonoscopy in patients with colonic inflammatory bowel disease. Inflamm Bowel Dis. 2013;19(2):350–355. doi: 10.1002/ibd.23002. [DOI] [PubMed] [Google Scholar]
- 37.Jess T, Frisch M, Simonsen J. Trends in overall and cause-specific mortality among patients with inflammatory bowel disease from 1982 to 2010. Clin Gastroenterol Hepatol. 2013;11(1):43–48. doi: 10.1016/j.cgh.2012.09.026. [DOI] [PubMed] [Google Scholar]
- 38.Rodriguez SA, Eisen GM. Surveillance and management of dysplasia in ulcerative colitis by U.S. gastroenterologists: in truth a good performance. Gastrointest Endosc. 2007;66(5):1070. doi: 10.1016/j.gie.2007.06.029. [DOI] [PubMed] [Google Scholar]
- 39.van den Broek FJ, Stokkers PC, Reitsma JB, et al. Random biopsies taken during colonoscopic surveillance of patients with longstanding ulcerative colitis: low yield and absence of clinical consequences. Am J Gastroenterol. 2014;109(5):715–722. doi: 10.1038/ajg.2011.93. [DOI] [PubMed] [Google Scholar]
- 40.Kiesslich R, Fritsch J, Holtmann M, et al. Methylene blue-aided chromoendoscopy for the detection of intraepithelial neoplasia and colon cancer in ulcerative colitis. Gastroenterology. 2003;124(4):880–888. doi: 10.1053/gast.2003.50146. [DOI] [PubMed] [Google Scholar]
- 41.Matsumoto T, Nakamura S, Jo Y, Yao T, Iida M. Chromoscopy might improve diagnostic accuracy in cancer surveillance for ulcerative colitis. Am J Gastroenterol. 2003;98(8):1827–1833. doi: 10.1111/j.1572-0241.2003.07580.x. [DOI] [PubMed] [Google Scholar]
- 42.Rutter MD, Saunders BP, Schofield G, Forbes A, Price AB, Talbot IC. Pancolonic indigo carmine dye spraying for the detection of dysplasia in ulcerative colitis. Gut. 2004;53(2):256–260. doi: 10.1136/gut.2003.016386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hurlstone DP, Sanders DS, Lobo AJ, McAlindon ME, Cross SS. Indigo carmine-assisted high-magnification chromoscopic colonoscopy for the detection and characterisation of intraepithelial neoplasia in ulcerative colitis: a prospective evaluation. Endoscopy. 2005;37(12):1186–1192. doi: 10.1055/s-2005-921032. [DOI] [PubMed] [Google Scholar]
- 44.Kiesslich R, Goetz M, Lammersdorf K, et al. Chromoscopy-guided endomicroscopy increases the diagnostic yield of intraepithelial neoplasia in ulcerative colitis. Gastroenterology. 2007;132(3):874–882. doi: 10.1053/j.gastro.2007.01.048. [DOI] [PubMed] [Google Scholar]
- 45.Marion JF, Waye JD, Present DH, et al. Chromoendoscopy Study Group at Mount Sinai School of Medicine. Chromoendoscopy-targeted biopsies are superior to standard colonoscopic surveillance for detecting dysplasia in inflammatory bowel disease patients: a prospective endoscopic trial. Am J Gastroenterol. 2008;103(9):2342–2349. doi: 10.1111/j.1572-0241.2008.01934.x. [DOI] [PubMed] [Google Scholar]
- 46.The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon: November 30 to December 1, 2002. Gastrointest Endosc. 2003;58(6 suppl):S3–S43. doi: 10.1016/s0016-5107(03)02159-x. [DOI] [PubMed] [Google Scholar]
- 47.Subramanian V, Mannath J, Ragunath K, Hawkey CJ. Meta-analysis: the diagnostic yield of chromoendoscopy for detecting dysplasia in patients with colonic inflammatory bowel disease. Aliment Pharmacol Ther. 2011;33(3):304–312. doi: 10.1111/j.1365-2036.2010.04525.x. [DOI] [PubMed] [Google Scholar]
- 48.Picco MF, Pasha S, Leighton JA, et al. Procedure time and the determination of polypoid abnormalities with experience: implementation of a chromoendoscopy program for surveillance colonoscopy for ulcerative colitis. Inflamm Bowel Dis. 2013;19(9):1913–1920. doi: 10.1097/MIB.0b013e3182902aba. [DOI] [PubMed] [Google Scholar]
- 49.Davies J, Burke D, Olliver JR, Hardie LJ, Wild CP, Routledge MN. Methylene blue but not indigo carmine causes DNA damage to colonocytes in vitro and in vivo at concentrations used in clinical chromoendoscopy. Gut. 2007;56(1):155–156. doi: 10.1136/gut.2006.107300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Hardie LJ, Olliver JR, Wild CP, Dexter S, Sahay P. Chromoendoscopy with methylene blue and the risk of DNA damage. Gastroenterology. 2004;126(2):623. doi: 10.1053/j.gastro.2003.12.024. [DOI] [PubMed] [Google Scholar]
- 51.Feinstein AR, Sosin DM, Wells CK. The Will Rogers phenomenon. Stage migration and new diagnostic techniques as a source of misleading statistics for survival in cancer. N Engl J Med. 1985;312(25):1604–1608. doi: 10.1056/NEJM198506203122504. [DOI] [PubMed] [Google Scholar]
- 52.Dekker E, van den Broek FJ, Reitsma JB, et al. Narrow-band imaging compared with conventional colonoscopy for the detection of dysplasia in patients with longstanding ulcerative colitis. Endoscopy. 2007;39(3):216–221. doi: 10.1055/s-2007-966214. [DOI] [PubMed] [Google Scholar]
- 53.van den Broek FJ, Fockens P, van Eeden S, et al. Narrow-band imaging versus high-definition endoscopy for the diagnosis of neoplasia in ulcerative colitis. Endoscopy. 2011;43(2):108–115. doi: 10.1055/s-0030-1255956. [DOI] [PubMed] [Google Scholar]
- 54.Ignjatovic A, East JE, Subramanian V, et al. Narrow band imaging for detection of dysplasia in colitis: a randomized controlled trial. Am J Gastroenterol. 2012;107(6):885–890. doi: 10.1038/ajg.2012.67. [DOI] [PubMed] [Google Scholar]
- 55.Pellisé M, López-Cerón M, Rodríguez de Miguel C, et al. Narrow-band imaging as an alternative to chromoendoscopy for the detection of dysplasia in longstanding inflammatory bowel disease: a prospective, randomized, crossover study. Gastrointest Endosc. 2011;74(4):840–848. doi: 10.1016/j.gie.2011.05.013. [DOI] [PubMed] [Google Scholar]
- 56.Naymagon S, Marion JF. Surveillance in inflammatory bowel disease: chromoendoscopy and digital mucosal enhancement. Gastrointest Endosc Clin N Am. 2013;23(3):679–694. doi: 10.1016/j.giec.2013.03.008. [DOI] [PubMed] [Google Scholar]
- 57.Pohl J, Lotterer E, Balzer C, et al. Computed virtual chromoendoscopy versus standard colonoscopy with targeted indigocarmine chromoscopy: a randomised multicentre trial. Gut. 2009;58(1):73–78. doi: 10.1136/gut.2008.153601. [DOI] [PubMed] [Google Scholar]
- 58.Aminalai A, Rösch T, Aschenbeck J, et al. Live image processing does not increase adenoma detection rate during colonoscopy: a randomized comparison between FICE and conventional imaging (Berlin Colonoscopy Project 5, BECOP-5) Am J Gastroenterol. 2010;105(11):2383–2388. doi: 10.1038/ajg.2010.273. [DOI] [PubMed] [Google Scholar]
- 59.Chung SJ, Kim D, Song JH, et al. Efficacy of computed virtual chromoendoscopy on colorectal cancer screening: a prospective randomized, back-to-back trial of Fuji Intelligent Color Enhancement versus conventional colonoscopy to compare adenoma miss rates. Gastrointest Endosc. 2010;72(1):136–142. doi: 10.1016/j.gie.2010.01.055. [DOI] [PubMed] [Google Scholar]
- 60.Hoffman A, Sar F, Goetz M, et al. High definition colonoscopy combined with i-Scan is superior in the detection of colorectal neoplasias compared with standard video colonoscopy: a prospective randomized controlled trial. Endoscopy. 2010;42(10):827–833. doi: 10.1055/s-0030-1255713. [DOI] [PubMed] [Google Scholar]
- 61.Messmann H, Endlicher E, Freunek G, Rümmele P, Schölmerich J, Knüchel R. Fluorescence endoscopy for the detection of low and high grade dysplasia in ulcerative colitis using systemic or local 5-aminolaevulinic acid sensitisation. Gut. 2003;52(7):1003–1007. doi: 10.1136/gut.52.7.1003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.van den Broek FJ, Fockens P, van Eeden S, et al. Endoscopic tri-modal imaging for surveillance in ulcerative colitis: randomised comparison of high-resolution endoscopy and autofluorescence imaging for neoplasia detection; and evaluation of narrow-band imaging for classification of lesions. Gut. 2008;57(8):1083–1089. doi: 10.1136/gut.2007.144097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Fusco V, Ebert B, Weber-Eibel J, et al. Cancer prevention in ulcerative colitis: long-term outcome following fluorescence-guided colonoscopy. Inflamm Bowel Dis. 2012;18(3):489–495. doi: 10.1002/ibd.21703. [DOI] [PubMed] [Google Scholar]
- 64.Navaneethan U, Kochhar G, Venkatesh PG, et al. Random biopsies during surveillance colonoscopy increase dysplasia detection in patients with primary sclerosing cholangitis and ulcerative colitis. J Crohns Colitis. 2013;7(12):974–981. doi: 10.1016/j.crohns.2013.02.009. [DOI] [PubMed] [Google Scholar]
- 65.Harpaz N, Talbot IC. Colorectal cancer in idiopathic inflammatory bowel disease. Semin Diagn Pathol. 1996;13(4):339–357. [PubMed] [Google Scholar]
- 66.Verschuren EC, Ong DE, Kamm MA, Desmond PV, Lust M. Inflammatory bowel disease cancer surveillance in a tertiary referral hospital: attitudes and practice. Intern Med J. 2014;44(1):40–49. doi: 10.1111/imj.12285. [DOI] [PubMed] [Google Scholar]
- 67.Friedman S, Cheifetz AS, Farraye FA, et al. Factors that affect adherence to surveillance colonoscopy in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2013;19(3):534–539. doi: 10.1097/MIB.0b013e3182802a3c. [DOI] [PubMed] [Google Scholar]
- 68.Siegel CA, Schwartz LM, Woloshin S, et al. When should ulcerative colitis patients undergo colectomy for dysplasia? Mismatch between patient preferences and physician recommendations. Inflamm Bowel Dis. 2010;16(10):1658–1662. doi: 10.1002/ibd.21233. [DOI] [PMC free article] [PubMed] [Google Scholar]