

ABSTRACT
Immunization coverage in Canada has continued to fall below national goals. The addition of pharmacists as immunizers may increase immunization coverage. This study aimed to compare estimated influenza vaccine coverage before and after pharmacists began administering publicly funded influenza immunizations in Nova Scotia, Canada. Vaccination coverage rates and recipient demographics for the influenza vaccination seasons 2010-2011 to 2012-2013 were compared with the 2013-2014 season, the first year pharmacists provided immunizations. In 2013-2014, the vaccination coverage rate for those ≥5 years of age increased 6%, from 36% in 2012-2013 to 42% (p<0.001). Pharmacists administered over 78,000 influenza vaccinations, nearly 9% of the province's population over the age of five. Influenza vaccine coverage rates for those ≥65 increased by 9.8% (p<0.001) in 2013-2014 compared to 2012-2013. Influenza vaccination coverage in Nova Scotia increased in 2013-2014 compared to previous years with a universal influenza program. Various factors may have contributed to the increased coverage, including the addition of pharmacists as immunizers and media coverage of influenza related fatalities. Future research will be necessary to fully determine the impact of pharmacists as immunizers.
KEYWORDS: Canada, immunization, influenza vaccination, pharmaceutical services, pharmacist, vaccine coverage
Introduction
Seasonal influenza poses a concern for the Canadian population in the fall and winter of each year, infecting 10–20% of the population annually.1 Receipt of seasonal influenza vaccination each year is the safest and most effective way to prevent illness and associated complications.1,2 As of July 2015, seven provinces and three territories in Canada had publicly funded universal influenza vaccination programs, and the three remaining provinces funded vaccinations for many high risk populations; however, coverage has continued to fall below the national goal of 80%.1-3 Pharmacists are regarded as trusted health care providers with the capacity to improve vaccination coverage by increasing accessibility and convenience.4,5 As of September 2015, legislation has passed in 8 of 10 provinces, but none of the three territories, that allows pharmacists with appropriate certification to administer immunizations.6 Legislation passed in 2013 which allowed pharmacists in Nova Scotia, Canada with appropriate certification to administer immunizations to patients five years of age and older.4 Approximately 430 of the 1262 licensed pharmacists in Nova Scotia obtained certification and were utilized as vaccine providers for the first time in the publicly funded universal influenza vaccination program in 2013-2014. As the addition of pharmacists as immunizers in Canada is recent, there is minimal published data on the impact of Canadian pharmacists as immunizers and no published data on the impact in Nova Scotia.7
This study aimed to compare estimated rates of influenza immunization coverage in Nova Scotia, Canada prior to and after the scope of pharmacist practice was expanded to include administration of immunizations. In addition, we characterized the demographics of the population that received their influenza vaccine from pharmacists.
Results
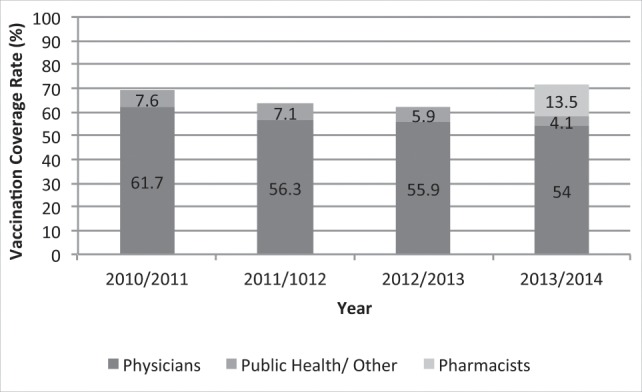
In the 2013-2014 influenza season, Nova Scotia pharmacists administered 78,102 influenza vaccinations, which contributed to an increase of 53,424 (15.8%) in the total number of influenza vaccines administered compared to the 2012-2013 influenza season (391,170 to 337,746, respectively). The overall provincial influenza immunization coverage rate for those 5 years of age or older increased by 5.9% (95% CI, 5.87–6.1) from 35.7% (95% CI, 35.5–35.8%) in 2012-2013 to 41.6% (95% CI, 41.5–41.7%) in 2013–2014 (p < 0.001). Of the 41.6% of Nova Scotia residents who received influenza vaccinations in 2013–2014, pharmacists vaccinated 8.7%, physicians vaccinated 26.6% and public health vaccinated 6.3%. The number of vaccines administered by physicians and public health declined in 2013-2014 from previous years.(Fig. 1)
Figure 1.

Vaccination coverage (%) and total vaccinations administered by year and provider in Nova Scotia, 2010-2011 to 2013-2014.
Of the 78,102 vaccinations administered by pharmacists, the approximate breakdown by age group was as follows: 12.5% aged 5–17 years, 4.1% aged 18-23 years, 54.6% aged 24–64 years, 27.4% greater than 64 years, and age was unknown for 1.4%. In those aged 65 years of age or older, influenza vaccine coverage was 71.6% (95% CI, 71.4–71.8%) in 2013–2014, up from 61.8% (95% CI, 61.5–62%) in 2012-2013 (p<0.001). Prior to the addition of pharmacists immunizing, this patient population reached its highest vaccination coverage of 69.3% in 2010–2011.(Fig. 2)
Figure 2.
Influenza vaccine coverage rates for community residents aged 65 and older by provider group (excluding long term care facilities), Nova Scotia, 2013-2014.
No statistically significant differences were noted with regards to gender distribution between the years or providers evaluated, with a ratio of approximately 55:45, females to males.
Discussion
Influenza coverage rates in Nova Scotia dropped after 2010–2011, remaining fairly steady between 2011–2012 and 2012–2013 before increasing in 2013–2014. Higher vaccination coverage in 2010–2011 may be due to the implementation of universal influenza funding and heightened awareness following the 2009 H1N1 pandemic, however, reasons for the drop in vaccination rates in 2011–2012 are not clear. The vaccination coverage increased in 2013–2014, surpassing the coverage previously noted in 2010–2011. The 2013–2014 season was the first season that pharmacists were regulated to administer injections, and funded to administer influenza vaccinations.
Pharmacists began immunizing in the United States in the mid-1990s and subsequently have more published research, which has consistently shown higher rates of adult immunization in states that allowed pharmacists to vaccinate versus those that did not.8-12 Although we have not compared our vaccination rates to other provinces, we have compared to previous years and similarly found increased influenza vaccination coverage in the year with the addition of pharmacists administering immunizations compared to previous years.
As elderly patients are high risk for complications from influenza, a national goal of 80% vaccination coverage in patients aged 65 years and older has been set.2 While this national target has not been met in any of the years evaluated, the highest level, 71.6%, since the commencement of universal funding in the province was seen in the year that pharmacists provided influenza vaccines in addition to traditional providers. The previous highest coverage rate seen in the age group was 69.3% in the 2010-2011 influenza season (Fig. 2). An increase in vaccination rates among those greater than 65 years of age was previously seen in a study completed in rural communities in British Columbia, Canada.7 The study found that pharmacy-based influenza immunization clinics resulted in a statistically significant increase in vaccination rates from 56.9% to 80.1%(p = 0.01) among those greater than 65 years of age.7 The increase in immunization coverage in seniors in Nova Scotia may in part be due to seniors visiting a pharmacy more often than a physician, thereby providing greater opportunity for pharmacists to recommend and administer influenza vaccine to this population.13
Concerns have been voiced that the addition of pharmacists as immunizers will not increase overall vaccination rates, but shift the provision of vaccines from traditional providers, such as physicians and public health, to pharmacists. In Nova Scotia, the number of vaccines administered by physicians continued to follow the declining trend noted since 2010-2011 (Fig. 1). A decrease in the number of vaccinations administered by public health was noted and was deliberate with fewer influenza vaccination clinics scheduled. This was done in order to transfer some influenza immunization activity to pharmacists, allowing Public Health to focus their resources on other activities. The data for 2010-2011 and 2011-2012 were also confounded by reporting as data available in these seasons did not differentiate between those 5 years of age and older, the age group pharmacists can administer. Therefore the coverage rates in these two influenza seasons are reported for those 6 months of age and older. Since coverage rates observed during these seasons include a larger age range, they would be expected to be higher. Despite the decline in vaccinations administered by physicians and public health, and the larger age range included in 2010-2012, the overall number of vaccines administered and the vaccination coverage in the province increased in 2013-2014. In the US, studies have found that vaccination rates increased overall in states allowing pharmacists to immunize, but that the location where the flu vaccine was administered did not significantly differ between the groups, with the majority still receiving their flu vaccine in a physician's office. This study suggests that the addition of pharmacists may have led to increased advertising and awareness of the importance of influenza vaccines and a subsequent overall increase in vaccination rates from that as opposed to a shift in providers.14 This may be what we are also seeing in NS, as the majority of vaccine recipients are receiving their vaccine in a physician's office. This is an area that requires further study.
The results of our study suggest that the addition of pharmacists as immunizers may be associated with an increase in overall influenza vaccination coverage, specifically in those aged 65 years and older. There are potential limitations to the analysis. First, as aggregate data was used, there were limitations on the availability of age group and gender data in some cases, therefore a comprehensive comparison of various age groups and gender between all years and providers was not possible. Second, as the data was based on information submitted by providers to the Department of Health and Wellness, any billing or coding errors by the providers could affect the results. As the means of collecting immunization administration data did not change over the study period, this should not have affected the overall results of the study. Third, patients under 9 years of age require 2 vaccines when receiving the influenza vaccine for the first time, however investigators were unable to determine how many patients this applied to and therefore data for this population could be over reported. As this potential over reporting would have occurred in all years evaluated, in all provider groups, and because this was an age group that was not immunized in great numbers by pharmacists, it is expected that it had minimal impact on the results. Finally, two situations arose during 2013-2014 that may have further affected the data. First, there were deaths related to H1N1 reported in the country in January 2014 with extensive media coverage, which may have led more people to seek immunization.15 In Nova Scotia, approximately three-quarters of the total immunizations provided by pharmacists were administered prior to the reported H1N1 deaths; however, the impact on the last quarter is not known. Second, there was a perceived “shortage” of influenza vaccine in Nova Scotia due to some distribution delays, as well as redistribution concerns in January 2014 following the H1N1 reports. The effects of this perceived “shortage” are unknown, with various pharmacists reporting that if they had more vaccine available they would have immunized more individuals and others reporting that the perceived shortage encouraged more people to be immunized.
In summary, there was an increase in both the number of influenza vaccines administered and the influenza vaccination coverage rate in Nova Scotia, Canada in the first year that pharmacists administered publicly funded influenza vaccines compared to the previous three influenza seasons. The impact of the limitations in the data and potential confounders is not known. Future research will be necessary to fully determine the impact of pharmacists as immunizers on immunization rates.
Methods
A retrospective analysis of physician and pharmacist billings, as well as district Public Health Services data, was completed to determine influenza vaccination coverage rates in Nova Scotia in four consecutive immunization seasons. As immunization season begins in October of each year, each year of data used was from mid-August of one year through to mid-August of the following year to obtain accurate immunization records. Data were reviewed for 2010-2011, 2011-2012, 2012-2013, and 2013-2014. Coverage rates were determined by analyzing the number of vaccines administered by each provider (physicians, pharmacists, and public health) as a proportion of the census data from the respective year. The demographics of vaccine recipients were divided into age groups and gender and compared between years and providers.
Only those years with a universal public funding program for influenza in Nova Scotia were included in the study (2010-2011 forward) as the first year pharmacists began immunizing was also a universal public funding program year.16 Coverage data during the 2009-2010 season was not analyzed due to the occurrence of the H1N1 pandemic.17
All data were provided by a third party, the Nova Scotia Department of Health and Wellness, in aggregate form and did not contain any patient-specific identifiers.
Data analysis
Estimated immunization rates and 95% confidence intervals were constructed for each year by using the number of influenza immunizations administered, as estimated from billing data and Public Health, as the numerator and the population of interest as the denominator. Census data for the appropriate year was used for population estimates for the total population and grouped by age and sex. Chi-square was used to compare the proportion of the immunized population between years. All data analysis was completed using EXCEL XLSTAT version 2015.
The study received approval from the Capital Health Research Ethics Board, Halifax, Nova Scotia, Canada.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Acknowledgments
The authors would like to thank Elaine Holmes and the Pharmacists as Immunizers Working Group for their support and input on this project.
Funding
This work was supported by a grant from the Drug Evaluation Alliance of Nova Scotia (DEANS).
References
- [1].National Advisory Committee on Immunization (NACI) Statement on Seasonal Influenza Vaccine for 2014-2015 [Internet]. Ottawa (ON: ): Public Health Agency of Canada; 2014. [updated 2014 Sep 19; cited 2015 Aug 05]. Available from: http://www.phac-aspc.gc.ca/naci-ccni/flu-grippe-eng.php [Google Scholar]
- [2].Public Health Agency of Canada Vaccine coverage amongst adult Canadians: Results from the 2012 adult National Immunization Coverage (aNIC) survey [Internet]. Ottawa (ON: ): Public Health Agency of Canada; 2014. [updated 2014 Apr 10; cited 2015 Aug 05]. Available from: http://www.phac-aspc.gc.ca/im/nics-enva/icc-cvc-eng.php [Google Scholar]
- [3].Public Health Agency of Canada Public funding for influenza vaccination by province/ territory (as of March, 2015) [Internet]. Ottawa (ON: ): Public Health Agency of Canada; 2015. [updated 2015 May 21; cited 2015 Aug 05]. Available from: http://www.phac-aspc.gc.ca/im/ptimprog-progimpt/fluvacc-eng.php [Google Scholar]
- [4].Secretariat for the Blueprint for Pharmacy National Coordinating Office Environmental scan: Pharmacy practice legislation and policy changes across Canada [Internet]. Ottawa (ON: ): Canadian Pharmacists Association; 2014. May [cited 2015 Jun 06]. Available from: blueprintforpharmacy.ca/docs/kt-tools/environmental-scan–pharmacy-practice-legislation-and-policy-changes-may-2014.pdf. [Google Scholar]
- [5].Kimmel SR, Burns IT, Wolfe RM, Zimmerman RK. Addressing immunization barriers, benefits, and risks. J Fam Pract 2007; 56(2 Suppl Vaccines):S61-9; PMID:17270112 [PubMed] [Google Scholar]
- [6].Canadian Pharmacists Association Pharmacists' Expanded Scope of Practice [Internet]. Ottawa (ON: ): Canadian Pharmacists Association; 2015. [updated 2015 Sept; cited 2015 Nov 08]. Available from: http://www.pharmacists.ca/index.cfm/pharmacy-in-canada/scope-of-practice-canada/ [Google Scholar]
- [7].Marra F, Kaczorowski J, Gastonguay L, Lynd LD, Kendall P. Pharmacy-based immunization in rural communities strategy (PhICS): A community cluster-randomized trial. Can Pharm J (Ott) 2014; 147(1):33-44; PMID:24494014; http://dx.doi.org/ 10.1177/1715163513514020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Ernst ME, Chalstrom CV, Currie JD, Sorofman B. Implementation of a community pharmacy-based influenza vaccination program. J Am Pharm Assoc (Wash) 1997; NS37:570-80; PMID:9479410 [DOI] [PubMed] [Google Scholar]
- [9].Higginbotham S, Stewart A, Pfalzgraf A. Impact of a pharmacist immunizer on adult immunization rates. J Am Pharm Assoc 2003; 2012; 52:367-71. [DOI] [PubMed] [Google Scholar]
- [10].Loughlin SM, Mortazavi A, Garey KW, Rice GK, Birtcher KK. Pharmacist-managed vaccination program increased influenza vaccination rates in cardiovascular patients enrolled in a secondary prevention lipid clinic. Pharmacotherapy 2007; 27:729-33; PMID:17461708; http://dx.doi.org/ 10.1592/phco.27.5.729 [DOI] [PubMed] [Google Scholar]
- [11].Skelton JB. American Pharmacists Association, Academy of Managed Care Pharmacy. Pharmacist-provided immunization compensation and recognition: white paper summarizing APhA/AMCP stakeholder meeting. J Am Pharm Assoc 2003; 2011; 51:704-12 [DOI] [PubMed] [Google Scholar]
- [12].Van Amburgh JA, Waite NM, Hobson EH, Migden H. Improved influenza vaccination rates in a rural population as a result of a pharmacist-managed immunization campaign. Pharmacotherapy 2001; 21:1115-22; PMID:11560201; http://dx.doi.org/ 10.1592/phco.21.13.1115.34624 [DOI] [PubMed] [Google Scholar]
- [13].Canadian Association of Chain Drug Stores 9000 points of care: improving access to affordable health care [Internet]. Toronto (ON: ): Canadian Association of Chain Drug Stores; 2013. Apr [cited 2015 Aug 26]. Available from: http://9000pointsofcare.ca/the-plan [Google Scholar]
- [14].Steyer TE, Ragucci KR, Pearson WS, Mainous AG III. The role of pharmacists in the delivery of influenza vaccinations. Vaccine 2004. 2/25; 22(8):1001-6; PMID:15161077; http://dx.doi.org/ 10.1016/j.vaccine.2003.08.045 [DOI] [PubMed] [Google Scholar]
- [15].CBC News H1N1 flu in Alberta causes 10 deaths [Internet]. Edmonton (AB: ): CBC/Radio-Canada; 2014. Jan 06 [updated 2014 Jan 06; cited 2015 Aug 05]. Available from: http://www.cbc.ca/news/canada/edmonton/h1n1-flu-in-alberta-causes-10-deaths-1.2486357 [Google Scholar]
- [16].Nova Scotia Department of Health and Wellness Influenza Surveillance Reports [Internet]. Halifax (NS: ): Province of Nova Scotia; 2013. [updated 2015 Sep 3; cited 2015 Sep 21]. Available from: http://www.novascotia.ca/dhw/populationhealth [Google Scholar]
- [17].Infection Prevention and Control Canada Pandemic (H1N1) 2009 virus [Internet]. Winnipeg (MB: ): IPAC Canada; 2009. [updated 2014 Oct 06; cited 2015 Aug 05]. Available from: http://www.ipac-canada.org/links_swineflu.php [Google Scholar]