

Abstract
Objective
To compare the safety, efficacy and complications of single vs multiple instillations of povidone iodine (PI) and urographin as a sclerosing agent in the treatment of chyluria.
Patients and methods
The study included 58 patients diagnosed with chyluria between March 2006 and January 2013. The inclusion criteria were either severe attacks of chyluria or patients with mild-to-moderate chyluria who had failed conservative treatment. The patients were randomly allocated to one of two groups: those in Group A had a single instillation of a combination of PI 0.2% plus the contrast-agent urographin 76%, while those in Group B had multiple instillations of the same combination twice daily for 3 successive days.
Results
The mean (SD) age of the patients in Groups A and B was 38.22 (10.67) and 37.9 (10.86) years, respectively. Chyluria was severe in eight patients (14.8%), moderate in 25 (46.3%) and mild in 21 (38.9%). The success rate in Group A (single instillation) was 85.2% and in Group B (multiple instillation) was 88.9%. The recurrence rate in Group A was 14.8% with a disease-free duration (DFD) of 4–15 weeks, while in group B it was 11.1% with a DFD of 6–18 weeks.
Conclusion
There was no significant difference between a single instillation of a combination of PI 0.2% and urographin 76% as a sclerosing agent in the treatment of chyluria and multiple instillations. However, the single instillation protocol is more cost effective with a shorter hospital stay.
Abbreviations: DFD, Disease-free duration; PI, Povidone iodine; RPIS, Retrograde pelvic instillation of sclerosing agent
Keywords: Chyluria, Urographin, Povidone iodine, Safety, Complication
Introduction
Chyluria is a condition characterised by the passage of milky urine due to abnormal communication between the lymphatic system and pyelocalyceal system [1]. Chyluria has the characteristic of remission and exacerbation and this is apparently seen in the countries in which it is endemic, such as India, Japan, North Africa, South-east Asia and South America [2]. It is a debilitating condition due to the continuous loss of protein and fat in the urine, with subsequent weight loss and immune suppression. Chyluria can be classified according to its severity into three grades: mild (intermittent milky urine, no clots, no weight loss, a single calyx involved on retrograde pyelography), moderate (intermittent or continuous milky urine with occasional clots, no weight loss, two calyces involved on retrograde pyelography) and severe (continuous milky urine with clots, weight loss, most of the calyces involved on retrograde pyelography) [3]
The first line of treatment is conservative measures in the form of a low-fat and high-protein diet and anti-filarial drugs, which are not effective in advanced conditions [4].
Renal pelvic instillation sclerotherapy (RPIS) using different agents [e.g. silver nitrate, povidone iodine (PI), potassium iodide, and contrast agents] is the most frequently treatment used for chyluria in the last three decades and it relies on producing fibrosis with subsequent closure of the pyelolymphatic connection [5]. Despite being highly effective, silver nitrate is no longer preferred due to its multiple side-effects [6].
The initial experience of using PI, as a sclerosing agent, for treating chyluria was reported by Shanmugam et al. [7]. Since then, multiple studies have used PI either in isolation or in combination with different agents, such as contrast agents or dextrose 50%. These studies also used PI either as a single instillation or in multiple instillation protocols [1], [5], [8]. Therefore, in the present study, we compared the safety, efficacy and complications of single vs multiple instillations of PI and urographin for the treatment of chyluria.
Patients and methods
This was a prospective randomised study from March 2006 to January 2013, including 58 patients diagnosed with chyluria using routine urine analysis, ether test, and urinary triglyceride assessment. Leucocyte esterase, urine culture and sensitivity were done routinely in all patients to exclude UTI. Pelvi-abdominal ultrasound and CT were performed in all patients.
-
•
Inclusion criteria were either severe attacks of chyluria (continuous chyluria with clots and or considerable weight loss) or patients with mild-to-moderate chyluria and failed response to conservative treatment (in the form of a fat-restricted high-protein diet and diethylecarbamazebine 100 mg three times a day/21 days).
-
•
Exclusion criteria were bilateral cases, mild-to-moderate cases with good response to conservative treatment, and cases with secondary chyluria.
All patients were consented with regards to the benefits and problems of the different lines of treatment, after approval of the study protocol by the Local Ethics Committee. The patients enrolled in the study were randomly allocated into two groups (randomised 1:1, i.e. one patient was allocated to Group A and the next one to Group B). Patients in Group A had a single instillation of a combination of PI 0.2% and the contrast-agent urographin 76% (Bayer™) and those in Group B had multiple instillations of the same combination twice daily for 3 successive days. All patients enrolled were given a heavy fatty meal the night before the procedure (250 mL full cream milk), a wide pore cannula was fixed the day of the procedure and local anaesthesia was given to patients. Initially, the patient is placed in the lithotomy position and the site of chyle efflux localised by diagnostic cystoscopy (Fig. 1). Four patients had bilateral efflux, two from each group and they were therefore excluded. In all the patients, a 6-F ureteric stent (open tip catheter) was inserted under fluoroscopy into the effluxing side and diluted contrast injected to delineate the pelvicalyceal system, detect pyelolymphatic fistula and to adjust the tip of the catheter at the renal pelvis of the affected site. The sclerosing agent was injected, comprising 5 mL PI 0.2% and 5 mL diluted contrast (2.5 mL urographin 76% + 2.5 mL distilled water), using the drip method under fluoroscopy. The combination was retained in the pelvicalyceal system of the affected side for 5 min (by closing the ureteric catheter) and then removed immediately after the procedure in Group A, while in Group B it was left for 3 days during which the patients received another five instillations of the same combination of the sclerosing agent every 12 h from the first instillation. All patients received routine prophylactic antibiotic before the procedure. All patients were observed for loin pain, fever, haematuria and disappearance of milky urine after the procedure. Patients were followed up at 3 months for 2 years, which included history, routine urine analysis and ether test. The disease-free duration (DFD) was calculated for recurrent cases only during the follow-up period and was considered to be the time from clinical and laboratory disappearance of chyluria until the first recurrence. Data were analysed using SPSS, version 16 for windows (2007, SPSS Inc., Chicago, IL, USA). A P < 0.05 was considered to indicate statistical significance. Data are reported as numbers and percentages or as the mean (SD) and median, as appropriate.
Figure 1.
Chyle efflux from a left ureteric orifice.
Results
Fig. 2 shows the flow of patients through the study. Of the 58 patients enrolled, four were subsequently found to have bilateral involvement and were therefore excluded. Table 1 shows the patients’ characteristics and outcomes. Chyluria was severe in eight patients (14.8%), moderate in 25 (46.3%), and mild in 21 (38.9%). Pyelolymphatic communications were detected in 11 patients (40.7%) in Group A and 13 (48.1%) in Group B during retrograde pyelography (Fig. 3). In all patients there was immediate disappearance of the milky urine just after the end of the procedure. Seven patients [four (14.8%) in Group A and three (11.1%) in Group B] had recurrence of chyluria during follow-up.
Figure 2.

Study flowchart.
Table 1.
Patients’ characteristics and outcomes.
| Variable | Group A (one instillation) | Group B (six instillations) | P |
|---|---|---|---|
| Mean (SD) age, years | 38.22 (10.67) | 37.9 (10.86) | 0.929 |
| Sex, n (%) | |||
| Male | 19 (70.4) | 16 (59.3) | |
| Female | 8 (29.6) | 11 (40.7) | 0.392 |
| Recurrence rate, n (%) | 4 (14.8) | 3 (11.1) | 0.685 |
| Mean (SD; range) DFD in recurrent cases, weeks | 9.25 (4.79; 4–15) | 11.33 (6.11; 6–18) | 0.632 |
| Complications, n (%) | |||
| Fever | 1 (3.7) | 3 (11.1) | 0.300 |
| Loin pain | 2 (7.4) | 4 (14.8) | 0.387 |
| Haematuria | 0 | 1 (3.7) | 0.315 |
Figure 3.
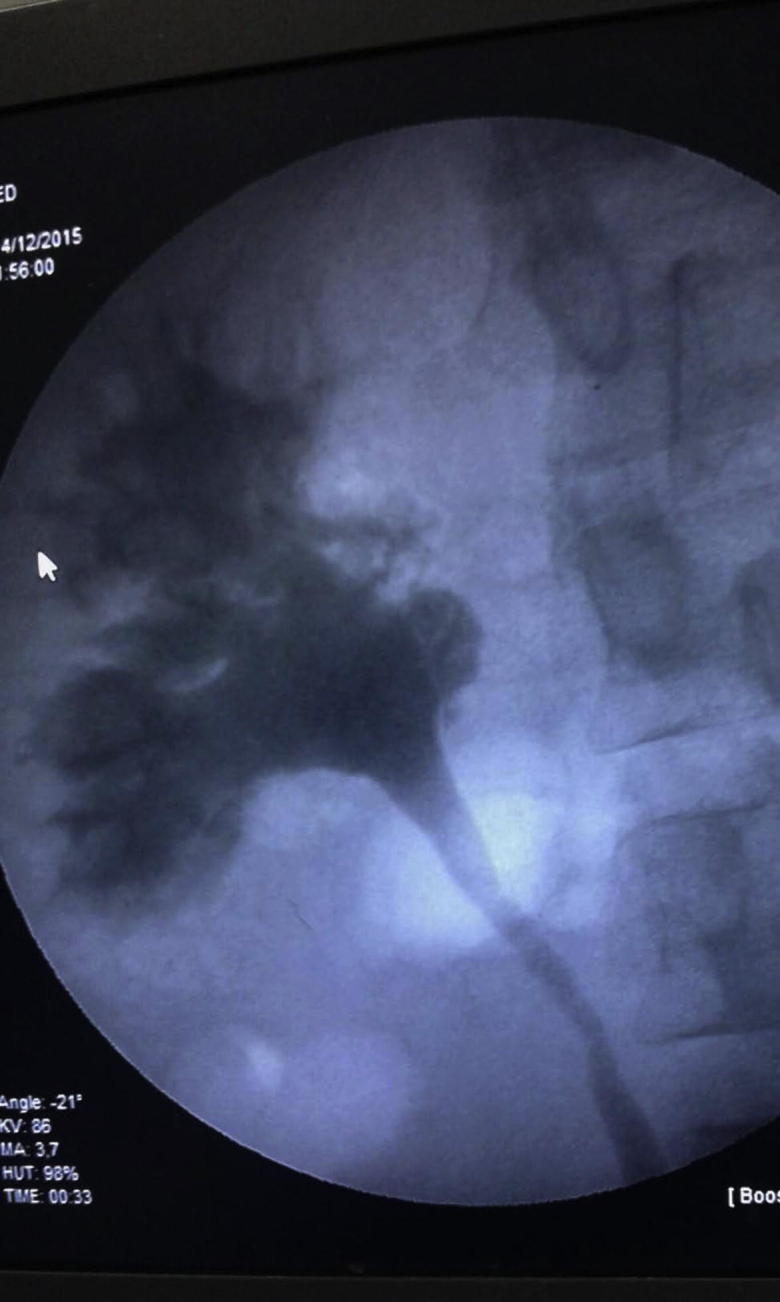
Retrograde pyelography showing pyelolymphatic reflux.
In Group A, the mean (SD; range) DFD in recurrent cases was 9.25 (4.79; 4–15) weeks, while in Group B it was 11.33 (6.11; 6–18) weeks (P = 0.632).
All patients who recurred underwent the same protocol as previously described. Four patients had complete remission of chyluria during the follow-up period and only three had recurrence of chyluria for a second time, and these patients then underwent surgical chylolymphatic disconnection.
Discussion
Chyluria is common in tropical countries and especially among the low socioeconomic class [9]. Also, it is common in certain areas in Egypt especially in the Sharkia Governorate, which is the site of our centre. The treatment of chyluria should be safe, minimally invasive, and cost effective [8]. Mild and moderate cases of chyluria can be treated with conservative treatment including diet modification and anti-filarial drugs [10], [11]. RPIS is the most prevalent form of treatment for chyluria [12].
The mechanism of action of RPIS is to induce an inflammatory reaction, chemical lymphangitis and fibrosis with subsequent closure of the pyelolymphatic fistulae [12]. Silver nitrate was one of the most important sclerosing agents used for many years; however, its use had been restricted due to multiple side-effects, such as interstitial nephritis, ureteric stricture, papillary necrosis, renal failure, and even death [12], [13], [14].
Many authors have described the use of PI as a sclerosing agent in the treatment of chyluria due to its high efficacy, antibacterial properties, availability, and minimal side-effects [1], [7], [8]. Many studies have used PI as a sclerosing agent for the treatment of chyluria either in isolation or in combination with other agents, and also either as a single or multiple instillation [5], [8], [15]. Yet, no definite standard protocol exists for describing the optimum dose, duration, and number of instillation. In our centre, we use a combination of PI 0.2% with contrast agent (urographin 76%) as the sclerosing agent for treating chyluria. All the patients who enrolled in the present study were randomly allocated into two groups, those in Group A received single instillation while those in Group B had six instillations over 3 days at 12 h intervals. We compared the groups for immediate success rate, recurrence rate, DFD, and occurrence of complications such as loin pain, fever, and haematuria. In the present study, the success rate for single instillation was 85.2%, while for multiple instillations it was 88.9%. The recurrence rate in Group A was 14.8% with a DFD of 4–15 weeks, while in Group B it was 11.1% with a DFD of 6–18 weeks. Shrestha and Verma [16] used a single PI instillation and reported a success rate of 83%, with a mean (range) DFD of 17.9 (3–36) months. They had two patients with loin pain who required analgesics. Also, Shanmugam et al. [7] found that the success rate after a single instillation of PI was 100% (total of five patients); however, they had few cases with a short follow-up period. Sharma et al. [5] used a combination of PI and contrast agent, and reported a success rate of 87.5% with an uneventful postoperative period except for minimal pain and dysuria. They had five patients with recurrence, one after 1 month, two after 3 months and two after 6 months. Murthy et al. [15] used nine instillations of PI 0.2%, and reported a success rate of 81%. They had recurrence after 1 month in four patients and repeated the instillation with complete clearance in two of these four patients. Nandy et al. [8] conducted their study on 46 patients using a combination of 5% PI and 50% dextrose solution in six-instillation sessions, and they reported a success rate of 87%. Four patients developed UTI and three with loin pain were all treated conservatively. They had four patients with recurrence. For complications in our present study, we had six patients who developed loin pain requiring parenteral analgesics, four who developed fever, and one who developed haematuria.
The limitations of our present study were the absence of randomised trials comparing single and multiple instillations to allow appropriate calculation of sample size and also the short follow-up period.
Conclusion
In our present study, the combination of PI 0.2% and urographin 76% as a sclerosing agent for the treatment of chyluria had a high success rate with insignificant complications. No significant difference in outcome could be detected between single vs multiple instillations; however, we recommend the single-instillation protocol, as it is more cost effective with a shorter hospital stay.
Source of funding
No funding from individuals or organisations.
Conflicts of interest
None.
Footnotes
Peer review under responsibility of Arab Association of Urology.
References
- 1.Goel S., Mandhani A., Srivastava A., Kapoor R., Gogoi S., Kumar A. Is povidone iodine an alternative to silver nitrate for renal pelvic instillation sclerotherapy in chyluria? BJU Int. 2004;94:1082–1085. doi: 10.1111/j.1464-410X.2004.05108.x. [DOI] [PubMed] [Google Scholar]
- 2.Suri A., Kumar A. Chyluria – SGPGI experience. Indian J Urol. 2005;21:59–62. [Google Scholar]
- 3.Date A., John T.J., Chandy K.G., Rajagopalan M.S., Vaska P.H., Pandey A.P. Abnormalities of the immune system in patients with chyluria. Br J Urol. 1981;53:384–386. doi: 10.1111/j.1464-410x.1981.tb03204.x. [DOI] [PubMed] [Google Scholar]
- 4.Brunkwall J., Simonsen O., Bergqvist D., Jonsson K., Bergentz S.E. Chyluria treated with renal autotransplantation: a case report. J Urol. 1990;143:793–796. doi: 10.1016/s0022-5347(17)40098-x. [DOI] [PubMed] [Google Scholar]
- 5.Sharma G., Chitale V., Karva R., Sharma A., Durug A.B. Fluoroscopy guided instillation therapy in chyluria using combination of povidone iodine with contrast agent. Is a single instillation sufficient? Int Braz J Urol. 2008;34:270–275. doi: 10.1590/s1677-55382008000300003. [DOI] [PubMed] [Google Scholar]
- 6.Mandhani A., Kapoor R., Gupta R.K., Rao H.S. Can silver nitrate instillation for the treatment of chyluria be fatal? Br J Urol. 1998;82:926–927. doi: 10.1046/j.1464-410x.1998.00839.x. [DOI] [PubMed] [Google Scholar]
- 7.Shanmugam T.V., Prakash J.V., Sivashankar G. Povidone iodine used as a sclerosing agent in the treatment of chyluria. Br J Urol. 1998;82:587. doi: 10.1046/j.1464-410x.1998.00861.x. [DOI] [PubMed] [Google Scholar]
- 8.Nandy P.R., Dwivedi U.S., Vyas N., Prasad M., Dutta B., Singh P.B. Povidone iodine and dextrose solution combination sclerotherapy in chyluria. Urology. 2004;64:1107–1109. doi: 10.1016/j.urology.2004.07.035. [DOI] [PubMed] [Google Scholar]
- 9.Hemal A.K., Gupta N.P. Retroperitoneoscopic lymphatic management of intractable chyluria. J Urol. 2002;167:2473–2476. [PubMed] [Google Scholar]
- 10.Henry H.Y., Leong Ch., Ong G.B. Chyluria: result of surgical treatment in 50 cases. J Urol. 1978;119:104–107. doi: 10.1016/s0022-5347(17)57396-6. [DOI] [PubMed] [Google Scholar]
- 11.Zhang X., Ye Z.Q., Chen Z., Chen Z.Q., Zhu Q.G., Xin M. Comparison of open surgery versus retroperitoneoscopic approach to chyluria. J Urol. 2003;169:991–993. doi: 10.1097/01.ju.0000045090.45767.56. [DOI] [PubMed] [Google Scholar]
- 12.Sabnis R.B., Punekar S.V., Desai R.M., Bradoo A.M., Bapat S.D. Instillation of silver nitrate in the treatment of chyluria. Br J Urol. 1992;70:660–662. doi: 10.1111/j.1464-410x.1992.tb15839.x. [DOI] [PubMed] [Google Scholar]
- 13.Kulkarni A.A., Pathak M.S., Sirsat R.A. Fatal renal and hepatic failure following silver nitrate instillation for treatment of chyluria. Nephrol Dial Transplant. 2005;20:1276–1277. doi: 10.1093/ndt/gfh790. [DOI] [PubMed] [Google Scholar]
- 14.Dash S.C., Bhargav Y., Saxena S., Agarwal S.K., Tiwari S.C., Dinda A. Acute renal failure and renal papillary necrosis following instillation of silver nitrate for treatment of chyluria. Nephrol Dial Transplant. 1996;11:1841–1842. [PubMed] [Google Scholar]
- 15.Ramana Murthy K.V., Jayaram Reddy S., Prasad D.V., Purusotham G. Povidone iodine instillation into the renal pelvis in the management of chyluria: our experience. Urol Int. 2010;84:305–308. doi: 10.1159/000288233. [DOI] [PubMed] [Google Scholar]
- 16.Shrestha A., Verma R. Is single dose povidone iodine sclerotherapy effective in chyluria? Kathmandu Univ Med J (KUMJ) 2014;12:107–110. [PubMed] [Google Scholar]