

Abstract
Objective
Determine whether prolonged consumption of high or low protein diets modifies the thermogenic response to a standard meal.
Methods
Twenty-four healthy individuals were randomized to overfeeding diets containing low (5%, n=8), normal (15%, n=9), or high (25%, n=7) protein for 56 days while inpatient. The thermic effect of food (TEF) was measured over 4 hours by indirect calorimetry following a standard meal (20% of energy, 20% protein) or a meal that matched the study diet (“study meal”).
Results
As expected, the TEF following the study meal (i.e. either low, normal or high protein content) was significantly associated with dietary protein (P=0.007), and the TEF was significantly increased in the high protein diet (15.4%) versus the normal protein (5.6%) and low protein diets (6.4%) (P=0.05 and P=0.03, respectively). However, returning to a standard meal (20% protein) after 42 days of overfeeding the study diets, the TEF response did not differ from baseline between groups or within subjects regardless of the prolonged intake of the habitual study diet (HP: P=0.32, LP: P=0.11, NP: P=0.79).
Conclusion
TEF is related to acute dietary protein intake but not altered by prolonged intake of high energy diets with high or low protein content.
Keywords: protein, thermic effect of food, energy expenditure, high protein, low protein
Introduction
Dietary interventions high in protein have increased in popularity for weight loss due to their reported effects to increase satiety, decrease food intake, and increase energy expenditure (1, 2, 3, 4). High protein diets have also been demonstrated to induce adaptive thermogenesis (i.e., a compensatory increase or decrease in energy expenditure in response to changes in body weight to oppose the maintenance of the new body weight (5)). This higher level of energy expenditure could be a mechanism that supports the long-term maintenance of weight loss with high protein diets (5). Adaptive thermogenesis with overfeeding high protein diets has been explained by increases in basal metabolic rate (6) and also increased physical activity (7). However, it is not known whether high protein diets can cause long lasting adaptive changes in the thermic effect of food (TEF) such that TEF in response to a standard meal remains increased after finishing the diet.
In this single-blind, randomized controlled trial, the metabolic implications of over-consuming a low (5%), normal (15%), or high (25%) protein diet on TEF were assessed over 56 days of controlled feeding. This study allows for assessments of TEF in four conditions: in response to a standard meal at 1) baseline (Day 0) and 2) following 42 days of overfeeding; and in response to the study meal (low, normal or high protein) on 3) day 1 and 4) day 56 of consumption of the assigned diet. The aim of this study was to evaluate the acute and prolonged change of TEF in response to dietary protein intake during overfeeding. We hypothesized that six weeks of overfeeding a high protein diet could nutritionally program the body to maintain an elevated metabolic cost for digestion, i.e. an elevated TEF. We tested our hypothesis by measuring the resting metabolic rate (VO2, VCO2) and respiratory quotient (RQ) before and after standard and study meal ingestion.
Methods
Design
This is a planned analysis of the PROOF (Protein Overfeeding) Study; a previously described single-blind, randomized controlled trial (6). Briefly, subjects were randomized to over-consume a low (5%), normal (15%) or high protein (25%) diet 40% above basal energy requirements for 56 days while residing on a metabolic ward. This trial is registered as NCT00565149 on clinicaltrials.gov.
Subjects
This study was approved and monitored by the Pennington Biomedical Institutional Review Board and subjects provided consent prior to study participation. Twenty eight subjects were enrolled in this trial and twenty four completed all TEF testing.
Body composition
Body composition was assessed by dual x-ray absorptiometry (Hologics QDR 4500A whole body scanner) and analyzed using QDR software version 11.1 (Hologics).
Thermic Effect of Food (TEF) Testing
TEF was assessed in response to two meal challenges: a standard meal and a study meal (specific to each of the study diets of overfed low, normal or high protein). TEF response to a standard meal (20% protein and approximately 20% of baseline total daily energy expenditure, or TDEE) was measured before and after 42 days of overfeeding by metabolic cart (DeltaTrac II™, Datex-Ohmeda, Helsinki, Finland) with the participant laying supine. TEF response to a meal specific of the study diet (either low, normal, or high protein; with carbohydrate constant and approximately 40% of TDEE) was measured on the first and last day of the overfeeding protocol, Days 1 and 56 respectively, by metabolic chamber with activity restricted to sedentary behaviors (8). Diet foods, compositions, and energy content are detailed in Table 1 and in-depth descriptions of the study diets have been previously reported (6). Following a 30 minute rest, a fasting 30 minute resting metabolic rate (RMR) test was performed. Subjects ingested a meal over the next 30 minutes and then 30-minute metabolic rate assessments were performed +30, +90, +150, and +210 minutes from meal administration. Energy expenditure (EE) was calculated for each minute from VO2 and VCO2 using Weir's equation (9). The first 10 minutes of each RMR test as well as minutes with coughing, sneezing, etc. were excluded. TEF was calculated as the change in postprandial energy expenditure from baseline (fasting) multiplied by the test length (kcal/4hr) and as a percentage of energy intake, i.e. calories of test meal. While physical activity is restricted for TEF measured by metabolic cart, activity in the metabolic chamber assumed usual sedentary behavior. Individual activity data (% activity) recorded by the metabolic chamber was incorporated into the statistical analyses as a covariate.
Table 1. TEF Meal Compositions.
| Energy | Protein | Total Fat | Carbohydrate | Meal Composition | |||||
|---|---|---|---|---|---|---|---|---|---|
| kcals | % of Baseline TDEE | % of energy | Grams | % of energy | Grams | % of energy | Grams | ||
| Standard meal – Day 0 and Day 42 | |||||||||
| High Protein Group | 481 ± 94 | 19 ± 1 | 19 ± 0.1 | 23 ± 5 | 27 ± 0.4 | 15 ± 3 | 54 ± 0.4 | 65 ± 13 | Eggs, bread, butter, reduced fat milk, and orange juice |
| Normal Protein Group | 483 ± 94 | 20 ± 1 | 19 ± 0.1 | 23 ± 5 | 27 ± 0.3 | 15 ± 3 | 54 ± 0.2 | 65 ± 13 | |
| Low Protein Group | 503 ± 57 | 22 ± 1 | 19 ± 0.1 | 24 ± 3 | 27 ± 0.2 | 15 ± 2 | 54 ± 0.2 | 68 ± 8 | |
| Study meal – Overfeeding Day 1 and Day 56 | |||||||||
| High Protein Group | 732 ± 138 | 30 ± 1 | 14 ± 0.7 | 26 ± 4 | 23 ± 2.3 | 19 ± 4 | 64 ± 1.8 | 116 ± 22 | Bread, fruit cocktail, yogurt, granola, milk |
| Normal Protein Group | 945 ± 293 | 38 ± 2 | 9 ± 1.0 | 21 ± 4 | 42 ± 2.2 | 44 ± 15 | 50 ± 2.1 | 119 ± 37 | Bread, butter, grapes, yogurt, granola, milk |
| Low Protein Group | 1198 ± 321 | 52 ± 4 | 4 ± 0.4 | 12 ± 3 | 47 ± 4.4 | 63 ± 21 | 51 ± 4.2 | 151 ± 32 | Bread, butter, grapes, yogurt, brownie, cranberry juice, milk |
Values reported as mean ± SE.
Statistical Analysis
Analyses were completed using SAS/STAT® software, Version 9.4 of the SAS System for Windows (Cary, NC, USA). Tests were performed with significance level α=0.05, and findings considered significant when P<α. Linear mixed effects models for repeated measures were used to determine whether differences in %TEF existed between diet groups at specific study visits or within diet groups over time. Comparisons were made using two-sample t-tests of the least squares means (LSM) to investigate between-group differences at end-of-study and within-group changes from baseline to end-of-study. The relationship between protein intake (grams) and %TEF was evaluated using the R2 statistic from a simple linear regression model. Fixed effects included when modelling %TEF following study meals were diet group, study visit, timing of the postprandial hood, and activity. Random subject effects were used to account for within-subject correlations between repeated measures within and across study visits. For the standard meal models, only diet group, study visit, and the random subject effect were included. Least squares means of %TEF adjusted for all other model covariates were obtained from the models for all diet groups at each study visit.
Results
Subjects
This cohort, aged 18 to 35 years old (mean 24±0.9), was comprised of 15 male and 9 female participants who self-identified as Caucasian (n=6), black (n=16) and other (n=2). Population characteristics as well as TEF responses at enrollment and following 42 and 56 days of overfeeding are detailed in Supplemental Table 1.
TEF Increases with a High Protein Diet
At the start of the study, the acute TEF response to the study diets was significantly associated with grams of protein consumed, r=0.53, P=0.007, Figure 1, and after 56 days of the study diet TEF remained elevated in response to the high protein test meal (15.4±3.1%) versus the normal (5.6±2.8%, P=0.03) and low protein test meals (6.4±2.9%, P=0.05), Supplemental Table 1 and Figure 1 inset. TEF on the last day of the study diet (Day 56) was not different compared to the first day of the study diet, Day 1 (High Protein Day 1: High Protein Day 56 P=0.16, Normal Protein Day 1: Normal Protein Day 56 P=0.53, Low Protein Day 1: Low Protein Day 56 P=0.85, Supplemental Table 1).
Figure 1.
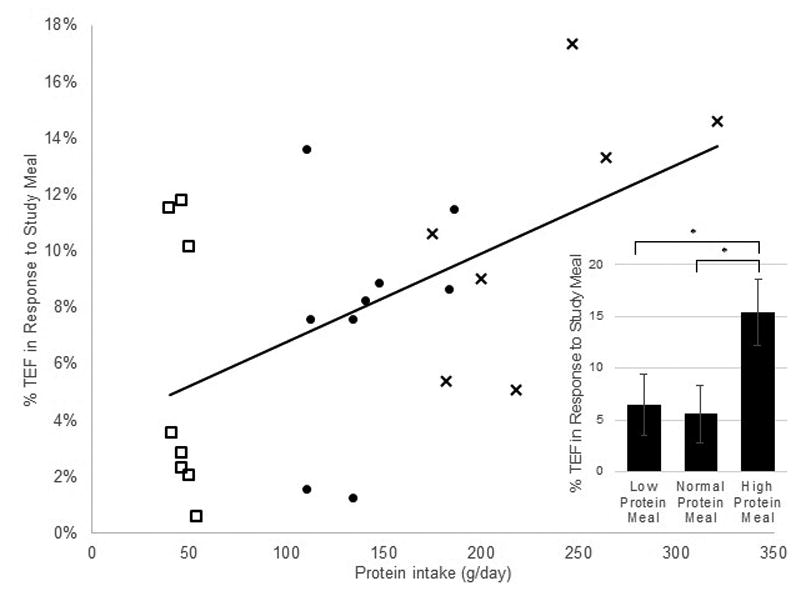
Thermic effect of food (% of energy intake) in response to an overfed meal of low, normal or high protein (compositions in Table 1) on Day 1, correlated with grams of protein/day; r= 0.53, p=0.007 (□= Low protein diet, ●= Normal protein diet, X = High protein diet) and Day 56 (inset).
No evidence of metabolic adaptation in TEF with overfeeding
The TEF in response to a standard meal (20% energy requirement, 20% protein) was not different between groups at Day 0 (P=0.80) or after 42 days of consuming diets with different amounts of protein, and was not significantly different from Day 0 (HP: P=0.32, NP: P=0.79, LP: P=0.11). Individual data is shown in Figure 2.
Figure 2.
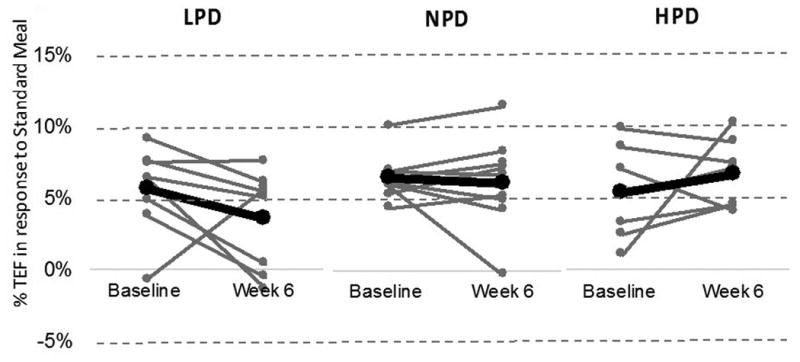
Thermic effect of food (% of energy intake) is not different in response to the same standard meal at baseline and after six weeks of overfeeding a low, normal or high protein diet; gray lines indicate individual participants, black lines are mean change within respective groups. Fixed effects included when modelling percent TEF were diet group, study visit, and the random subject effect were included.
Discussion
The aim of this study was to extend the finding that higher protein intake increases thermogenesis and evaluate whether an increase in thermic effect of food would persist following prolonged overfeeding of a high protein diet. As expected, we observed that the TEF was increased in response to a high protein diet and was correlated with protein intake. However, we saw no evidence that prolonged intake of a diet which was either high or low in protein could increase or decrease, respectively, the thermogenic response to a standard meal. Therefore, we conclude that the TEF is primarily regulated by acute factors, such as protein and energy intake, and is not a physiological response that can be permanently adapted or modified by prolonged changes in the habitual diet.
Another interesting observation was the high inter-individual variability of TEF responses among participants. While consuming the same food and living in the same controlled environment, TEF responses varied across a 10% range. A review of literature supports these findings, as TEF has been shown to be variable among individuals of different ages, races, weights, and metabolic health (8, 10). Additionally, protein prescriptions were based on percent of energy, not grams per day of body weight, thus inter-individual variability may also be attributed to differential protein balance. Despite this variability, we were able to observe a diet effect which contributes to the strength of our findings. Future directions could include a comparison of acute TEF response following prolonged change in dietary protein with energy intake clamped to differentiate between prolonged overfeeding, variable macronutrient intake, and effects of body composition changes.
While utilization of data from the highly controlled, well-reviewed PROOF study is a strength, leveraging data to answer a research question for which the study was not intentionally designed introduces the limitations of small sample size, significant changes in fat and fat free mass post overfeeding, and TEF assessments by two different indirect calorimetric instruments (bedside and whole room) with variable meal sizes, however we ensured in our analyses to only compare within and not between methodologies to account for this difference.
The protein-induced effect on metabolism is well known. Based upon the physiology of macronutrient digestion, dietary protein costs more of its usable energy to metabolize compared to fat and carbohydrates, 20-30% versus 5-10% and 0-3% respectively (11). However, contrary to our hypothesis, this elevation of TEF is not a learned or adaptive response to a prolonged diet. We observed upon immediately returning to a normal protein (20%) diet after six weeks of high protein overfeeding, the TEF showed no positive carryover effects of overfeeding or consuming a high protein diet. Although our study population was in positive energy balance, with additional studies perhaps this finding could be translated to individuals losing weight or maintaining weight loss with high protein diets. Our findings indicate that continual compliance with a dietary program, in this case with a high protein diet, is essential in order to take advantage of the beneficial increase in metabolism.
In summary, TEF when consuming a high protein diet was elevated in direct relation to protein intake when compared to a normal or low protein diet. This elevation is an acute response and there was no carry over thermogenesis observed following prolonged high protein consumption.
Supplementary Material
What is already known about this subject?
Most individuals have a metabolic adaptation in response to overfeeding.
Metabolic adaptation is hypothesized to be one mechanism protecting against weight gain.
Dietary protein exerts well known effects on energy metabolism, including thermogenesis, but it is not known whether these effects are transient or long lasting.
What does this study add?
This is a highly controlled, overfeeding study with dual measures of thermic effect of food by bedside and whole room indirect calorimetry in response to standard meal challenges and meals with low, normal and high protein content.
The results add to the body of literature supporting the ability of dietary protein to exert acute effects on thermogenesis.
This study shows no carry-over of the acute thermogenic effects of dietary protein following extended high protein consumption. In other words, the increased TEF is due to the content of each meal, not habitual protein intake.
Acknowledgments
We thank Dr. Eric Ravussin for his guidance on analysis of calorimetry data, study participants, and research staff. This work was published in abstract form and presented at Obesity Week on November 6, 2014 (12).
This work was supported by the US Department of Agriculture, grant #2010-34323-21052 and funding from Louisiana State University. This research was approved by the Pennington Biomedical Institutional Review Board. JHB is supported in part by 1 U54 GM104940 from the National Institute of General Medical Sciences of the National Institutes of Health which funds the Louisiana Clinical and Translational Science Center.
GAB and SRS designed and conducted the study. EFS and JHB analyzed and interpreted the results. EFS, LMR and GAB wrote the manuscript.
Footnotes
Disclosure Statement: The authors have nothing to disclose.
References
- 1.Weigle DS, Breen PA, Matthys CC, Callahan HS, Meeuws KE, Burden VR, et al. A high-protein diet induces sustained reductions in appetite, ad libitum caloric intake, and body weight despite compensatory changes in diurnal plasma leptin and ghrelin concentrations. Am J Clin Nutr. 2005;82:41–48. doi: 10.1093/ajcn.82.1.41. [DOI] [PubMed] [Google Scholar]
- 2.Anderson GH, Moore SE. Dietary proteins in the regulation of food intake and body weight in humans. J Nutr. 2004;134:974S–979S. doi: 10.1093/jn/134.4.974S. [DOI] [PubMed] [Google Scholar]
- 3.Whitehead JM, McNeill G, Smith JS. The effect of protein intake on 24-h energy expenditure during energy restriction. Int J Obes Relat Metab Disord. 1996;20:727–732. [PubMed] [Google Scholar]
- 4.Brehm BJ, D'Alessio DA. Benefits of high-protein weight loss diets: enough evidence for practice? Curr Opin Endocrinol Diabetes Obes. 2008;15:416–421. doi: 10.1097/MED.0b013e328308dc13. [DOI] [PubMed] [Google Scholar]
- 5.Rosenbaum M, Leibel RL. Adaptive thermogenesis in humans. Int J Obes (Lond) 2010;34(Suppl 1):S47–55. doi: 10.1038/ijo.2010.184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bray GA, Smith SR, de Jonge L, Xie H, Rood J, Martin CK, et al. Effect of dietary protein content on weight gain, energy expenditure, and body composition during overeating: a randomized controlled trial. Jama. 2012;307:47–55. doi: 10.1001/jama.2011.1918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Apolzan JW, Bray GA, Smith SR, de Jonge L, Rood J, Han H, et al. Effects of weight gain induced by controlled overfeeding on physical activity. Am J Physiol Endocrinol Metab. 2014;307:E1030–1037. doi: 10.1152/ajpendo.00386.2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tataranni PA, Larson DE, Snitker S, Ravussin E. Thermic effect of food in humans: methods and results from use of a respiratory chamber. Am J Clin Nutr. 1995;61:1013–1019. doi: 10.1093/ajcn/61.4.1013. [DOI] [PubMed] [Google Scholar]
- 9.Weir JB. New methods for calculating metabolic rate with special reference to protein metabolism. The Journal of physiology. 1949;109:1–9. doi: 10.1113/jphysiol.1949.sp004363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Watanabe T, Nomura M, Nakayasu K, Kawano T, Ito S, Nakaya Y. Relationships between thermic effect of food, insulin resistance and autonomic nervous activity. J Med Invest. 2006;53:153–158. doi: 10.2152/jmi.53.153. [DOI] [PubMed] [Google Scholar]
- 11.Westerterp-Plantenga MS, Nieuwenhuizen A, Tome D, Soenen S, Westerterp KR. Dietary protein, weight loss, and weight maintenance. Annu Rev Nutr. 2009;29:21–41. doi: 10.1146/annurev-nutr-080508-141056. [DOI] [PubMed] [Google Scholar]
- 12.Frost EA, Redman LM, Bray GA. ObesityWeek. Boston, Massachusetts: 2014. Effect of Dietary Protein Intake on Diet-Induced Thermogenesis During Overfeeding. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.