

Abstract
Background:
Data on the use of emergency medical services (EMS) by patients with cardiac conditions in the Gulf region are scarce, and prior studies have suggested underutilization. Patient perception and knowledge of EMS care is critical to proper utilization of such services.
Objectives:
To estimate utilization, knowledge, and perceptions of EMS among patients with ST-elevation myocardial infarction (STEMI) in the Emirate of Abu Dhabi.
Methods:
We conducted a multicenter prospective study of consecutive patients admitted with STEMI in four government-operated hospitals in Abu Dhabi. Semi-structured interviews were conducted with patients to assess the rationale for choosing their prehospital mode of transport and their knowledge of EMS services.
Results:
Of 587 patients with STEMI (age 51 ± 11 years, male 95%), only 15% presented through EMS, and the remainder came via private transport. Over half of the participants (55%) stated that they did not know the telephone number for EMS. The most common reasons stated for not using EMS were that private transport was quicker (40%) or easier (11%). A small percentage of participants (7%) did not use EMS because they did not think their symptoms were cardiac-related or warranted an EMS call. Stated reasons for not using EMS did not significantly differ by age, gender, or primary language of the patients.
Conclusions:
EMS care for STEMI is grossly underutilized in Abu Dhabi. Patient knowledge and perceptions may contribute to underutilization, and public education efforts are needed to raise their perception and knowledge of EMS.
Key words: Emergency medical services, perceptions, ST-elevation myocardial infarction
INTRODUCTION
Acute myocardial infarction (AMI) is a leading cause of morbidity and mortality worldwide with approximately one-half of deaths occurring in the prehospital setting.[1,2] In the United Arab Emirates, mortality statistics from 2008 to 2010 showed that cardiovascular disease was the leading cause of death among both the United Arab Emirates nationals and expatriates. In the Emirate of Abu Dhabi,[3] early diagnosis and care by emergency medical services (EMS) can play a crucial role in improving the management and ultimate outcome of patients with AMI.[4,5,6,7,8] Use of EMS may result in the faster initiation of reperfusion therapies, and facilitate quicker and more efficient treatment decisions.[8,9] Of particular importance is the role of EMS in caring for patients with ST-segment elevation myocardial infarction (STEMI), the most serious and time-sensitive type of AMI.[10] STEMI is potentially reversible provided that revascularization is initiated rapidly, as evidence has shown increased mortality associated longer culprit vessel occlusion times.[11,12]
While several international studies have emphasized the need for early activation of EMS in patients with AMI, EMS use is generally low in patients with STEMI.[3,6,7,8,9,13] These low EMS use rates were also found in the first Gulf Registry of Acute Coronary Events (Gulf RACE)[3] and again in the second Gulf RACE-2,[14] which reported EMS use rates of 17% and 25%, respectively, as well as in other studies of Middle Eastern countries.[15] Several studies have examined the issue of EMS transport to the hospital versus self-transport and found that patient characteristics, American Community Survey (ACS) characteristics, and patient's knowledge of ACS symptoms, influence the use of EMS as well.[16,17,18]
Patient perception and knowledge of EMS care is critical to proper utilization of such services. The purpose of this study was to estimate the utilization, knowledge, and perceptions of prehospital EMS among patients with STEMI in the Emirate of Abu Dhabi to determine if demographic and background variables or event characteristics were related to these factors.
METHODS
Study setting
Cardiac catheterization services are provided at five government operated hospitals, four of which are under the Abu Dhabi Health Services Company (SEHA) and one operated by the United Arab Emirates Armed Forces. EMS is operated by the Abu Dhabi Police Emergency and Public Safety Department, in conjunction with National Ambulance Company LLC, which provides emergency technicians and paramedics. The EMS is able to provide advanced cardiac life support and early STEMI recognition by means of 12 lead ECG acquisition and paramedic interpretation.
Design
This was an 18-month, multicenter, prospective study of consecutive patients admitted with STEMI to four government hospitals in the emirates of Abu Dhabi. The United Arab Emirates Armed Forces Hospital, Zayed Military Hospital, was excluded from our research due to EMS not transporting to this hospital. We performed telephonic or face-to-face semi-structured interviews, to assess their rationale for choosing their prehospital mode of transport and their knowledge of EMS contact details.
Mode of transport was ascertained by the way of both EMS and hospital electronic medical record data and confirmed with the patient at interview. The following questions were asked of all patients regardless of mode of transport utilized:
Do you know what the emergency number is to call an ambulance?
When you decided to go to the hospital, how did you get there, by ambulance or did you use private transport?
Patients who made the use of private transport instead of EMS were asked the following additional question:
What made you not call for an ambulance, but instead make use of private transport?
These questions were asked in the patient's native language with the assistance of staff in the hospital or with the assistance of follow-up investigators if the patient was discharged before interview.
Statistical analysis
Analyses consisted of both descriptive and inferential statistics. Descriptive statistics were computed for all the study variables including the demographic and background variables as well as the reasons for using private transportation. Inferential analyses were performed to determine if relationships existed between the demographic and background variables, on the one hand, and the reasons for taking private transportation on the other.
The dependent variable, reason for taking private transportation, was categorical. Most of the demographic and background variables were also categorical, and therefore, a series of Chi-square tests of independence were performed.
One demographic variable, age, was continuous, and therefore, a one-way ANOVA was performed to determine if the participants' reasons for using private transportation differed according to their age. Analyses were performed using SPSS Version 22.0 (IBM Corporation, Armonk, NY, USA) and a P ≤ 0.05 was considered to be statistically significant.
Ethics
The study protocol was approved by the Research Ethics Committees of Sheikh Khalifa Medical City, Mafraq, Al Ain, and Tawam hospitals as well as the University of Cape Town Human Research Ethics Committee (HREC 286/2013). Written consent to follow-up was obtained from patients before discharge, and an explanation of the research was provided in the patient's native language. EMS and in-hospital electronic medical records were also utilized for patients' data collection.
RESULTS
Baseline demographics
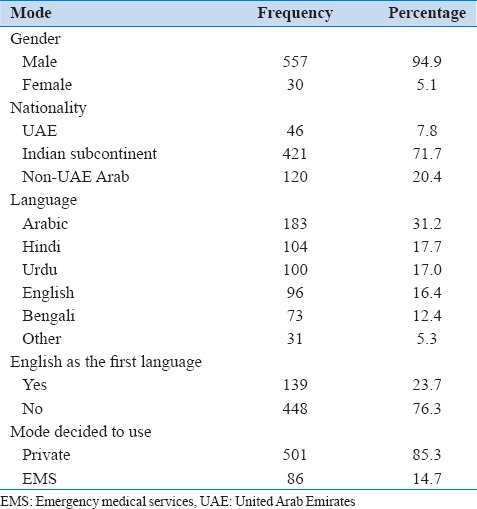
The study yielded 587 patients for inclusion. Most participants (n = 557, 94.9%) were male, and the average age was 51 (±11) years. However, this finding is not surprising considering that the United Arab Emirates has a large expatriate workforce which is predominately male.[19] The most common countries of origin were the India subcontinent (n = 421, 71.7%). Arabic was the most common language (n = 183, 31.2%), with substantial percentages of these participants being able to comprehend basic English (n = 96, 16.4%), Hindi (n = 104, 17.7%), and Urdu (n = 100, 17.0%).
English was the first language of only 23.7% (n = 139) of the participants [Table 1]. Most participants (n = 501, 85.3%) used private transportation to get to the hospital, and only a small percentage (n = 86, 14.7%) used EMS.
Table 1.
Descriptive statistics for reasons for mode of transport (n=587)
Transport demographics
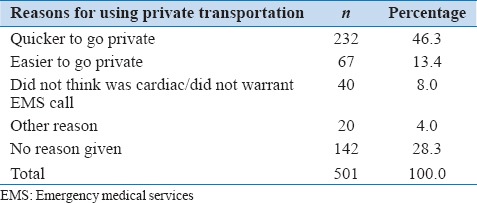
The reasons for using private transportation are shown in Table 2. The most common responses were that it was quicker (232, 46.3%) and easier (67, 13.4%) to go through private means. A smaller percentage of participants stated that they had not called EMS because they did not think their symptoms were cardiac-related (40, 8.0%). Patients with missing data were excluded from analysis.
Table 2.
Descriptive statistics for reasons for using private transportation (n=501)
Over half (323, 55.0%) of the participants stated that they did not know the telephone number for EMS in Abu Dhabi.
There were no differences between males and females in terms of their reasons for using private transportation rather than EMS (P = 0.26). There was also no statistically significant differences in age between individuals citing different reasons for using private transportation (P = 0.68) participants from Pakistan were less likely to feel that it was quicker to go through private transportation (37.2%) compared to between 42.3% and 56.6% for individuals from other countries, and individuals from the United Arab Emirates and Syria were less likely to feel that it was easier to go through private transportation (3.8% and 5.6%, respectively, compared to between 12.2% and 16.8% for individuals from other countries).
Participants with knowledge of the EMS number and those without that knowledge were compared in terms of their reason for using private transportation, and the results indicated a significant difference between the groups (P = 0.03) [Table 3]. Participants who knew the number for EMS 15.4% (but nevertheless took private transportation) were more likely to think that their event was not a cardiac event or did not warrant an EMS call than those who did not know the number 7.1% [Table 4].
Table 3.
Cross-tabulation of gender, nationality, language, and English as the first language versus reasons for using private transportation (n=501)
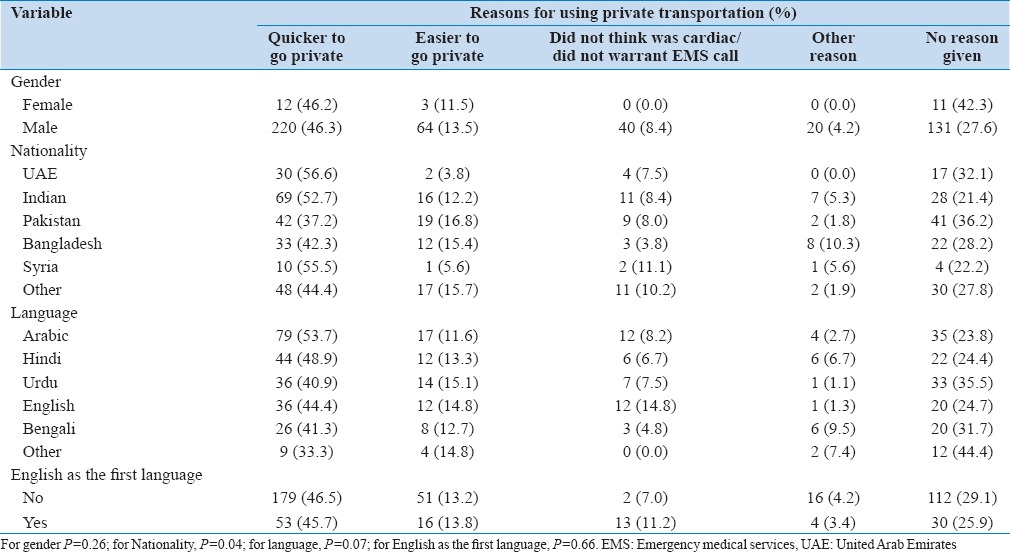
Table 4.
Cross-tabulation of city of event, transfers, and knowledge of the emergency medical services number versus reasons for using private transportation*
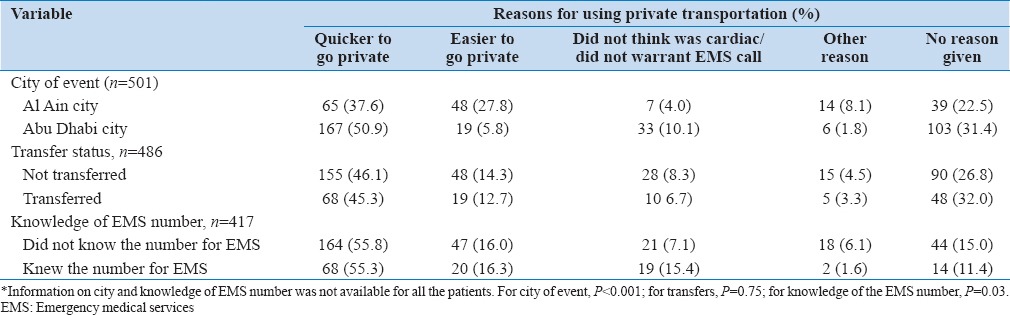
There was a significant difference in reasons for using private transportation between the two cities (P < 0.001) [Table 4]. Residents of Abu Dhabi City were more likely to feel it was quicker to use private transportation (50.9%). However, the residents of Al Ain City were more likely to feel it was easier to use private transportation (27.8%). There was no significance difference in reasons for using private transportation and those who were transferred (P = 0.75).
DISCUSSION
Our findings showed persistent underuse of EMS, with rates comparable to those of previous regional studies. It has been shown that EMS use rates vary between countries but were predominantly low, including 2% in Yemen, 7% in Kuwait, 17% in the United Arab Emirates, 23% in Bahrain, and 30% in Qatar.[14] Interestingly, a study conducted in Turkey found that despite a high knowledge of the emergency services number, only 29% of STEMI patients used EMS.[15]
In other countries such as the United States and China, EMS utilization rates varied between 20% and 50%.[20,21,22,23] However, higher rates of EMS have been reported in other studies. For example of 619 patients with an STEMI presenting to a Singapore hospital, 58.6% arrived by EMS.[17] Mathews et al. reported that in data from the National Cardiovascular Registry (ACTION Registry–GWTG), detailing almost 40,000 STEMI patients, EMS transport was used by 60%.[16]
Our study also indicated that public awareness of how to access EMS was a barrier to utilization. A high percentage of patients were not aware of the emergency contact number for the EMS in Abu Dhabi. This included patients for whom EMS was called on their behalf. Our research found that majority of the patients who used private transport did so as they thought that it would be a quicker means to access emergency health care.
In our study, we found that many participants were from foreign countries and with Arabic or English not as their first language, raising the question could complicate any public education campaigns to benefit future cardiac patients? Our findings emphasize the need for greater public education and awareness, with regards to not only the benefits of using EMS during chest pain events but also the signs and symptoms of cardiac emergencies.
The public should be educated to the fact that EMS is not only a transport modality, but that early treatment can be initiated en route, and cardiac interventions services can be activated before patient arrival. Education should also be directed at lower-income patients such as those involved with manual labor and encompass languages including Urdu, Hindi, Malayalam, and Bengali, as these patients comprised a large percentage of our study population. Strategies should focus on enhancing awareness of this particular population demographic, in their native languages dialects, with greater emphasis perhaps placed on newspapers and television as well as education in the workplace and the accommodations facilities under the auspices of government health-care programs. The internet and electronic social media platforms may not be the best way to educate these potential patients.
Limitations
We acknowledge the potential for referral bias, as a disproportionate number of patients may also have presented to private facilities that have interventional cardiology services in these two cities. We also acknowledge that despite previous research in the Middle East describing low EMS use rates, our results may not be generalizable due to postresearch recommendation changes in these countries having been initiated.
CONCLUSIONS
EMS care for STEMI is grossly underutilized in Abu Dhabi. Patient knowledge and perceptions may contribute to this underutilization, and public education efforts are needed to raise awareness of both the signs and symptoms of ACS and the importance of EMS utilization. Current public education appears to be ineffective and needs to target more specific demographic groups. It is hoped that the results of this study can be used as a foundation for future research and assist with public education strategies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors gratefully acknowledge the invaluable assistance provided by the following nursing staff without whom this research would not have been possible. 1) C. DMello RN, BSN, Invasive Cardiology Department, Al Ain Hospital, Al Ain, UAE. 2) V. Morales RN and M. Aujero RN, Coronary Care Unit, Sheikh Khalifa Medical City, Abu Dhabi, UAE.
REFERENCES
- 1.World Health Organization Fact Sheet No. 317. Cardiovascular Diseases. [Last accessed on 2015 Apr 30]. Available from: http://www.who.int/mediacentre/factsheets/fs317/en/print.html .
- 2.Fares S, Zubaid M, Al-Mahmeed W, Ciottone G, Sayah A, Al Suwaidi J, et al. Utilization of emergency medical services by patients with acute coronary syndromes in the Arab Gulf states. J Emerg Med. 2011;41:310–6. doi: 10.1016/j.jemermed.2010.05.002. [DOI] [PubMed] [Google Scholar]
- 3.HAAD Surveillance Section. Mortality (Death) Rate in Abu Dhabi. Health Authority Abu Dhabi. 2011. [Last cited on 2015 Mar 11]. Available from: http://www.haad.ae/HAAD/LinkClick.aspx?fileticket=sPsbfispbxk%3d and tabid=1216 .
- 4.Fukuoka Y, Dracup K, Ohno M, Kobayashi F, Hirayama H. Predictors of in-hospital delay to reperfusion in patients with acute myocardial infarction in Japan. J Emerg Med. 2006;31:241–5. doi: 10.1016/j.jemermed.2005.12.019. [DOI] [PubMed] [Google Scholar]
- 5.Song L, Hu DY, Yan HB, Yang JG, Sun YH, Li C, et al. Influence of ambulance use on early reperfusion therapies for acute myocardial infarction. Chin Med J (Engl) 2008;121:771–5. [PubMed] [Google Scholar]
- 6.Ting HH, Rihal CS, Gersh BJ, Haro LH, Bjerke CM, Lennon RJ, et al. Regional systems of care to optimize timeliness of reperfusion therapy for ST-elevation myocardial infarction: The Mayo Clinic STEMI protocol. Circulation. 2007;116:729–36. doi: 10.1161/CIRCULATIONAHA.107.699934. [DOI] [PubMed] [Google Scholar]
- 7.Terkelsen CJ, Lassen JF, Norgaard BL, Gerdes JC, Poulsen SH, Bendix K, et al. Reduction of treatment delay in patients with ST-elevation myocardial infarction: Impact of pre-hospital diagnosis and direct referral to primary percutaneous coronary intervention. Eur Heart J. 2005;26:770–7. doi: 10.1093/eurheartj/ehi100. [DOI] [PubMed] [Google Scholar]
- 8.Tubaro M, Danchin N, Goldstein P, Gerasimos F, Hasin Y, Heras M, et al. Pre-hospital treatment of STEMI patients. A scientific statement of the Working Group Acute Cardiac Care of the European Society of Cardiology Acute Coronary Syndromes. Rev Esp Cardiol. 2012;65:60. doi: 10.3109/17482941.2011.581292. [DOI] [PubMed] [Google Scholar]
- 9.Hassan AK, Liem SS, van der Kley F, Bergheanu SC, Wolterbeek R, Bosch J, et al. In-ambulance abciximab administration in STEMI patients prior to primary PCI is associated with smaller infarct size, improved LV function and lower incidence of heart failure: Results from the Leiden MISSION! Acute myocardial infarction treatment optimization program. Catheter Cardiovasc Interv. 2009;74:335–43. doi: 10.1002/ccd.21980. [DOI] [PubMed] [Google Scholar]
- 10.Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction – Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction) Circulation. 2004;110:588–636. doi: 10.1161/01.CIR.0000134791.68010.FA. [DOI] [PubMed] [Google Scholar]
- 11.Lambert L, Brown K, Segal E, Brophy J, Rodes-Cabau J, Bogaty P. Association between timeliness of reperfusion therapy and clinical outcomes in ST-elevation myocardial infarction. JAMA. 2010;303:2148–55. doi: 10.1001/jama.2010.712. [DOI] [PubMed] [Google Scholar]
- 12.Miedema MD, Newell MC, Duval S, Garberich RF, Handran CB, Larson DM, et al. Causes of delay and associated mortality in patients transferred with ST-segment-elevation myocardial infarction. Circulation. 2011;124:1636–44. doi: 10.1161/CIRCULATIONAHA.111.033118. [DOI] [PubMed] [Google Scholar]
- 13.Mingo S, Goicolea J, Nombela L, Sufrate E, Blasco A, Millán I, et al. Primary percutaneous angioplasty. An analysis of reperfusion delays, their determining factors and their prognostic implications. Rev Esp Cardiol. 2009;62:15–22. [PubMed] [Google Scholar]
- 14.AlHabib KF, Alfaleh H, Hersi A, Kashour T, Alsheikh-Ali AA, Suwaidi JA, et al. Use of emergency medical services in the second gulf registry of acute coronary events. Angiology. 2014;65:703–9. doi: 10.1177/0003319713502846. [DOI] [PubMed] [Google Scholar]
- 15.Demirkan B, Ege MR, Dogan P, Ipek EG, Güray U, Güray Y. Factors influencing the use of ambulance among patients with acute coronary syndrome: Results of two centers in Turkey. Anadolu Kardiyol Derg. 2013;13:516–22. doi: 10.5152/akd.2013.171. [DOI] [PubMed] [Google Scholar]
- 16.Mathews R, Peterson ED, Li S, Roe MT, Glickman SW, Wiviott SD, et al. Use of emergency medical service transport among patients with ST-segment-elevation myocardial infarction: Findings from the National Cardiovascular Data Registry Acute Coronary Treatment Intervention Outcomes Network Registry-Get with the Guidelines. Circulation. 2011;124:154–63. doi: 10.1161/CIRCULATIONAHA.110.002345. [DOI] [PubMed] [Google Scholar]
- 17.Chia YC. Modes of arrival, door to balloon time and its impact on morbidity and mortality for ST elevation myocardial infarction Tan Tock Seng Hospital. Singapore Crit Care. 2012;16(Suppl 1):P183. [Google Scholar]
- 18.Rathore SS, Curtis JP, Chen J, Wang Y, Nallamothu BK, Epstein AJ, et al. Association of door-to-balloon time and mortality in patients admitted to hospital with ST elevation myocardial infarction: National cohort study. BMJ. 2009;338:b1807. doi: 10.1136/bmj.b1807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.National Bureau of Statistics U. Statistics by Title. UAE Statistics. 2015. [Last cited on 2015 Nov 02]. Available from: http://www.uaestatistics.gov.ae/EnglishHome/ReportsByDepartmentEnglish/tabid/104/Default.aspx?MenuId=1 & NDId=457 .
- 20.Hutchings CB, Mann NC, Daya M, Jui J, Goldberg R, Cooper L, et al. Patients with chest pain calling 9-1-1 or self-transporting to reach definitive care: Which mode is quicker? Am Heart J. 2004;147:35–41. doi: 10.1016/s0002-8703(03)00510-6. [DOI] [PubMed] [Google Scholar]
- 21.Scherer TM, Russ S, Jenkins CA, Jones ID, Slovis CM, Cunningham BL. Predictors of transport by private vehicle versus ambulance to the emergency department in patients with ST-elevation myocardial infarction and impact on door-to-balloon time. Prehosp Disaster Med. 2012;27:226–30. doi: 10.1017/S1049023X12000696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Song L, Yan H, Hu D. Patients with acute myocardial infarction using ambulance or private transport to reach definitive care: Which mode is quicker? Intern Med J. 2010;40:112–6. doi: 10.1111/j.1445-5994.2009.01944.x. [DOI] [PubMed] [Google Scholar]
- 23.Weiner SG, Wu JT, Bhatti P, Goetz JD. Mode of arrival does not predict myocardial infarction in patients who present to the ED with chest pain. Int J Emerg Med. 2009;2:241–5. doi: 10.1007/s12245-009-0126-7. [DOI] [PMC free article] [PubMed] [Google Scholar]