

Abstract
Thrombotic events are relatively common in high altitude areas and known to occur in young soldiers working at high altitude without usual risk factors associated with thrombosis at sea-level. However, till now, cases with thrombotic events were reported only in lowlanders staying at high altitude. These two cases of pulmonary embolism demonstrate that thrombotic events can occur in highlanders after a prolonged stay at the extreme altitude.
Key words: High altitude, pulmonary embolism, thrombosis
INTRODUCTION
Thrombotic events are relatively common in high altitude areas and known to occur in young soldiers working at high altitude without usual risk factors associated with thrombosis at sea-level. However, until now, cases with thrombotic events were reported only in lowlanders staying at high altitude. A thrombotic event in highlanders has not been reported. Here, we are reporting two cases of pulmonary embolism developing after prolonged stay at extreme altitude in individuals who are natives of high altitude by birth.
CASE REPORTS
Case 1
A 29-year-old serving soldier with no co-morbid illness was air evacuated to our hospital (located at a height of ~11,500 ft) from a location at a height of 17,000 ft with complaints of pleuritic chest pain (left side), breathlessness, and hemoptysis (single episode), since 12 h. He denies the history of fever, anorexia, weight loss, calf pain, swelling, and trauma. He was a smoker with pack year of 8.5, but denies any other addiction. He was native of high altitude staying at an altitude of 12,000 ft since birth and denies any history of de-induction to lower altitude since 1-year. He was working at a height of 14,000 ft for last 8 months and at a height of 17,000 ft for 1-month.
Clinical examination at our hospital revealed the following: Average built (weight 59 kg, height 168 cm), temperature 98°F, pulse rate 72/min, respiratory rate 20/min, blood pressure 124/70 mm Hg, oxygen saturation on room air 88%, and 94% of oxygen inhalation. Chest auscultation revealed coarse crepts in the left infra-axillary area. Electrocardiogram revealed no significant abnormality. Chest radiograph revealed cardiomegaly with consolidation in left lower zone. Hematological investigations revealed hemoglobin of 19.0 g/dl with normal total leukocyte count, normal biochemical, and metabolic profile.
In view of prolonged stay at extreme high altitude, sudden onset of symptoms, chest radiograph findings with normal total leukocyte counts, the possibility of pulmonary embolism was considered, and urgent computerized tomography pulmonary angiography was done, which revealed a filling defect in the segmental arterial branch supplying lateral basal segment of left lower lobe along with consolidation of corresponding lung segment suggestive of pulmonary embolism [Figure 1]. He was started on low molecular weight heparin and was switched over to long-term oral anticoagulation. The subsequent recovery was uneventful and patient was discharged on oral anticoagulants.
Figure 1.
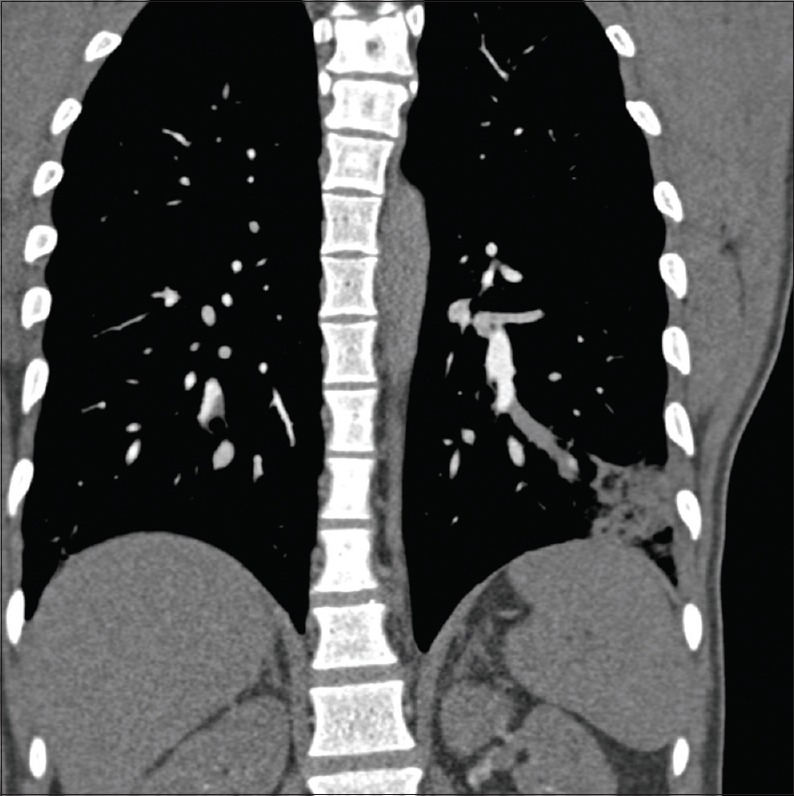
Computerized tomography pulmonary angiography showing filling defect in segmental branch supplying lateral basal segment of left lower lobe along with consolidation of corresponding lung segment suggestive of pulmonary embolism
Case 2
A 36-year-old serving soldier with no co-morbid illness was air evacuated to our hospital (located at a height of ~11,500 ft) from a location at a height of 17,000 ft with complaints of chest pain and breathlessness for last 1-day. He denies the history of hemoptysis, trauma, calf swelling, and pain. He had symptoms of runny nose, cough, and fever 2 days back along with the history of less water intake during that period. He was a smoker (pack year 7.5) but stopped smoking 2 years back and also denies any other addiction. He was a native resident of high altitude staying at an altitude of 11,500 ft since birth and denies any history of descent to lower altitude, since last 3 years.
Clinical evaluation at our hospital revealed the following: Average built (weight 70 kg, height 165 cm), blood pressure 130/78 mm Hg, pulse rate 98/min, respiratory rate 30/min, oxygen saturation of 78% on room air, and 91% of oxygen supplementation. Chest auscultation revealed coarse crepts in right infra-scapular and the infra-axillary area along with decreased breath sound in left infra-scapular area. Electrocardiogram revealed no significant abnormality. Chest radiograph revealed consolidation in right lower zone with blunting of left costophrenic angle. Hematological investigation revealed hemoglobin of 18.1 g/dl with normal total leukocyte counts, normal metabolic, and biochemical parameters except raised total serum bilirubin of 2.5 mg/dl, direct bilirubin 1.3 mg/dl, SGOT 33 IU/L, and SGPT 59 IU/L.
In view of prolonged stay at extreme altitude, sudden onset of symptoms, chest radiograph findings with raised hemoglobin, the possibility of pulmonary embolism was considered, and urgent computerized tomography pulmonary angiography was done, which revealed filling defects in segmental branches supplying posterior basal and medial basal segments of left lower lobe; similar filling defects in segmental arterial branches supplying posterior basal and lateral basal segments of right lower lobe along with consolidation of corresponding lung segments with mild left sided pleural effusion suggestive of bilateral pulmonary embolism [Figures 2 and 3].
Figure 2.
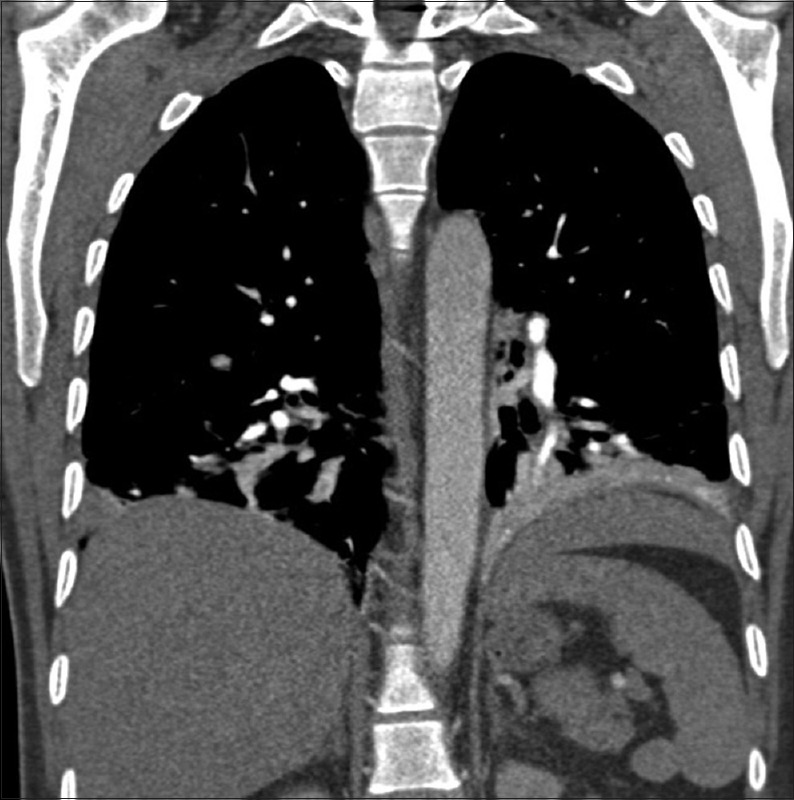
Computerized tomography pulmonary angiography showing filling defects in segmental arterial branches supplying posterior basal and lateral basal segments of right lower lobe along with consolidation of corresponding lung segments
Figure 3.
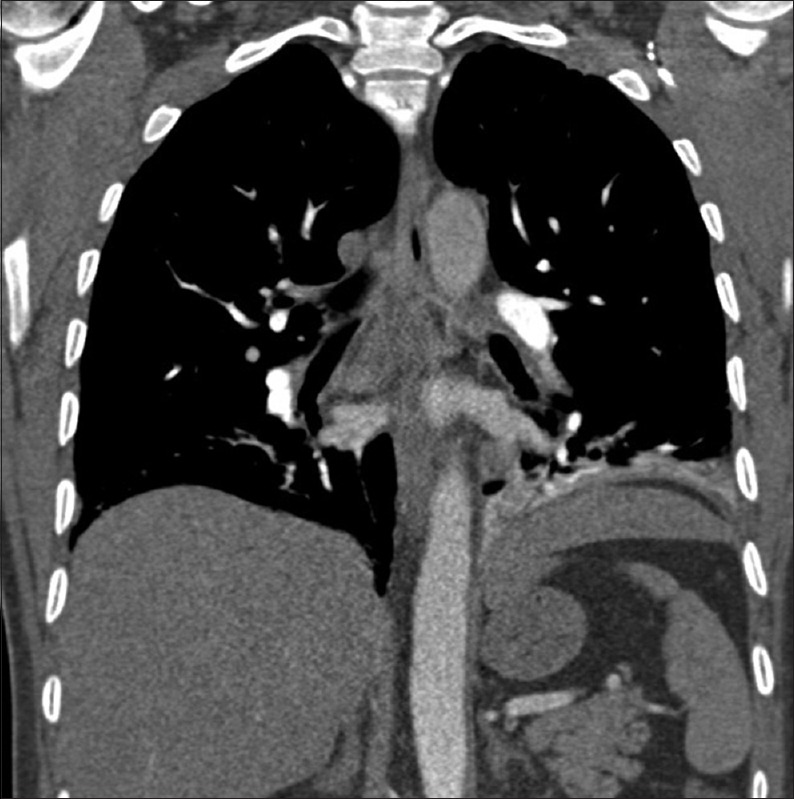
Computerized tomography pulmonary angiography showing filling defects in segmental branches supplying posterior and medial basal segments of left lower lobe, along with consolidation of corresponding lung segments with mild left sided pleural effusion
Echocardiography revealed free floating right ventricular thrombus. He was given intravenous tissue plasminogen activator with 10 mg bolus followed by 90 mg over 2 h. Repeat echocardiography performed after 12 h revealed no evidence of right ventricular thrombus. Subsequently, he was started on low molecular heparin and switched over to long-term oral anticoagulants. His recovery was uneventful and patient was discharged on oral anticoagulants.
DISCUSSION
Pulmonary embolism is relatively common in high altitude areas and known to occur in young soldiers working at high altitude without the usual risk factors. Ward reported three cases of deep vein thrombosis (DVT) of calf veins in climbers after ascent to extreme high altitude.[1] Similar cases of DVT in patients climbing to Mt Goodwin Austin and during Canadian Everest expedition 2000 have also been reported.[2,3] Dickinson et al. reported seven deaths in unacclimatized trekkers at a height above 5,000 feet, 5 of them had a pulmonary embolism, but only one had demonstrable DVT of calf vein.[4]
Singh and Chohan had reported thrombotic occlusive hypertensive vascular disease in Indian soldiers residing at high altitude for the duration of 5–24 months.[5] They showed the three DVT cases of calf veins apart from thrombosis of the cerebral, coronary, and mesenteric arteries. Presti et al. found the incidence of chronic massive thrombosis of the pulmonary artery to be 0.9% in high altitude.[6] Anand et al. have also demonstrated systemic venous thrombosis in soldiers staying at extreme high altitude for prolonged periods of time.[7] Anand et al. demonstrated 20 DVT cases of calf veins in Indian soldiers residing above 5,000 m for more than 10 months.[8] They also reported a 30 times higher risk of spontaneous vascular thrombosis (commonly DVT) on long-term stay at high altitude in Indian soldiers. Similar DVT of calf veins was demonstrated in Pakistani soldiers staying at high altitude for a prolonged period of time.[9]
A study by Kumar has demonstrated 24.5 times higher risk of DVT after a long-term stay of lowlanders at high altitude as compared to people staying at low altitude.[10] Another study to determine the frequency of different risk factors for pulmonary embolism in soldiers serving at high altitude in Pakistan has documented high altitude as the only risk factor in 50% patients (25 out of 50 patients).[11] Recently, we also reported a case of right ventricular thrombus with a bilateral pulmonary embolism in a serving soldier after a prolonged stay at high altitude without any risk factor.[12]
Jha et al. studied the clinical profile of 30 cases of stroke and reported that long-term stay at high altitude with polycythemia and hypercoagulable state were associated with higher risk of stroke.[13] In a prospective cohort study by Kotwal et al., demonstrated that the combination of erythrocytosis, increased platelet count, platelet activation, and raised fibrinogen level combined with hypoxia and dehydration at high altitude leads to thrombosis in normal individuals or in asymptomatic cases with inherited/acquired thrombophilia.[14]
Low humidity and increased resting respiratory rate at high altitude leading to increased insensible water loss, dehydration, and relative hemo-concentration, bad weather conditions resulting in prolonged periods of inactivity; and hence, venous stasis may also contribute to thrombosis. Pro-coagulant disorders such as protein C deficiency, fibrinolytic enzyme deficiency or antiphospholipid antibody syndrome can lead to thrombosis even at moderate altitude. Kotwal et al. while studying 21 cases of stroke in young at high altitude found hyper homocystinemia in three patients, protein C and protein S deficiency in one each.[14]
Hence, it is certain that thrombotic episodes occur on exposure to high altitude in the form of pulmonary, splenic, mesenteric, cerebral, or peripheral thrombosis. Unusual environmental conditions in high altitude such as extreme cold, hypoxia, prolonged immobilization, polycythemia, smoking, and dehydration contribute to hypercoagulable state (as in our patients).
One of our cases was having right ventricular thrombus with bilateral pulmonary embolism which carries a very high mortality. In a study, cases of right heart thrombus had twice the mortality rate at 14 days and 3 months of 21% and 29%, respectively, compared to mortality rate of 11% and 16%, respectively, in cases of pulmonary embolism.[15] The mortality in the cases of right heart thrombus treated with heparin alone, thrombolysis, and surgical embolectomy was 23.5%, 20.8%, and 25%, respectively.
In another retrospective study, of 177 cases with right heart thrombus, mortality rate in cases with no therapy, anticoagulation therapy, surgical embolectomy, and thrombolysis were 100%, 28.6%, 23.8%, and 11.3%, respectively.[16] Further analysis revealed the association of improved survival rate associated with thrombolysis therapy compared to other treatment options. The difference in the treatment-associated mortality in cases of right heart thrombus is attributed to subject selection, presence of co-morbidities, and varying the number of cases treated in the three treatment groups. The most common complication associated with thrombolysis was bleeding, which occurred in 21.9% of the cases compared to a rate of 7.9% in cases treated with heparin alone.[17] A review of described recent studies showing occurrence of bleeding between 20% and 25% of treated cases and 5–10% major bleeding.[18] The most common site for major bleed was intracranial with a mortality of 50%.[18]
Few studies describe the effect of high altitude on thrombotic profile in natives of high altitude. Hurtado[19] reported shortening of clotting time in high altitude natives in Peruvian Andes. The incidence of thrombotic events related atherosclerosis in high altitude natives has been found to be lesser compared to sea-level population.[20] However, the effect of ascent to greater heights on high altitude natives is yet be studied in greater depth. The rise in hematocrit due to hypoxia at heights greater than the height of the location of birth or prolonged stay could predispose high altitude natives to thrombosis like in polycythemia due to other conditions.[21]
Platelet adhesiveness was found to be elevated in permanent residents of high altitude.[22] The combination of these factors along with reduced mobility, dehydration, and additional risk of smoking could have possibly resulted in thrombosis in our cases. High altitude natives are invariably part of expeditions as support staff or porters. A high index of suspicion for pulmonary embolism as one of the possibilities should be exercised for high altitude natives also to enable early detection and prompt evacuation.
Until now, cases of thrombotic events were reported only in lowlanders staying at high altitude. This case report demonstrates that thrombotic events can occur in highlanders after a prolonged stay at the extreme altitude.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ward M. Mountain Sickness: A Clinical Study of Cold and High Altitude. London: Crosby Lockwood Staples; 1975. pp. 123–7. [Google Scholar]
- 2.Genton E, Ross AM, Takeda YA, Vogel JH. Hypoxia, High Altitude and the Heart, Advances in Cardiology. 3rd ed. Basel: Karger; 1970. Alterations in blood coagulation at high altitude; pp. 32–7. [Google Scholar]
- 3.Robinson V. Physician's Logs; Expedition Everest 2000. Can Broadcast Corp Gaz. 2000:22–3. [Google Scholar]
- 4.Dickinson J, Heath D, Gosney J, Williams D. Altitude-related deaths in seven trekkers in the Himalayas. Thorax. 1983;38:646–56. doi: 10.1136/thx.38.9.646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Singh I, Chohan IS. Blood coagulation changes at high altitude predisposing to pulmonary hypertension. Br Heart J. 1972;34:611–7. doi: 10.1136/hrt.34.6.611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Presti B, Berthrong M, Sherwin RM. Chronic thrombosis of major pulmonary arteries. Hum Pathol. 1990;21:601–6. doi: 10.1016/s0046-8177(96)90005-2. [DOI] [PubMed] [Google Scholar]
- 7.Anand AC, Saha A, Seth AK, Chopra GS, Nair V, Sharma V. Symptomatic portal system thrombosis in soldiers due to extended stay at extreme high altitude. Hepatology. 2005;20:777–8. doi: 10.1111/j.1440-1746.2005.03723.x. [DOI] [PubMed] [Google Scholar]
- 8.Anand AC, Jha SK, Saha A, Sharma V, Adya CM. Thrombosis as a complication of extended stay at high altitude. Natl Med J India. 2001;14:197–201. [PubMed] [Google Scholar]
- 9.Hussain T, Niaz A. Deep vein thrombosis at high altitude. J Pak Med Assoc. 2002;52:440. [PubMed] [Google Scholar]
- 10.Kumar S. High altitude induced deep venous thrombosis. A study of 28 cases. Indian J Surg. 2006;68:84–8. [Google Scholar]
- 11.Khalil KF, Saeed W. Pulmonary embolism in soldiers serving at high altitude. J Coll Physicians Surg Pak. 2010;20:468–71. [PubMed] [Google Scholar]
- 12.Singhal S, Paliwal V, Bhattachar SA, Pathak K. Successful treatment of free floating right ventricular thrombus with acute pulmonary embolism. Heart India. 2015;3:21–3. [Google Scholar]
- 13.Jha SK, Anand AC, Sharma V, Kumar N, Adya CM. Stroke at high altitude: Indian experience. High Alt Med Biol. 2002;3:21–7. doi: 10.1089/152702902753639513. [DOI] [PubMed] [Google Scholar]
- 14.Kotwal J, Chopra GS, Sharma YV, Kotwal A, Bhardwaj JR. Study of the pathogenesis of thrombosis at high altitude. Indian J Hematol Blood Transfus. 2004;22:17–21. [Google Scholar]
- 15.Torbicki A, Galie N, Covezzoli A, Rossi E, De Rosa M, Goldhaber SZ. ICOPER study group. Right heart thrombi in pulmonary embolism. Result from the International Cooperative Pulmonary Embolism Registry. J Am Coll Cardiol. 2003;41:2245–51. doi: 10.1016/s0735-1097(03)00479-0. [DOI] [PubMed] [Google Scholar]
- 16.Rose PS, Punjabi NM, Pearse DB. Treatment of right heart thromboemboli. Chest. 2002;121:806–14. doi: 10.1378/chest.121.3.806. [DOI] [PubMed] [Google Scholar]
- 17.Konstantinides S, Geibel A, Olschewski M, Heinrich F, Grosser K, Rauber K, et al. Association between thrombolytic treatment and the prognosis of hemodynamically stable patients with major pulmonary embolism: Results of a multicenter registry. Circulation. 1997;96:882–8. doi: 10.1161/01.cir.96.3.882. [DOI] [PubMed] [Google Scholar]
- 18.Almoosa K. Is thrombolytic therapy effective for pulmonary embolism? Am Fam Physician. 2002;65:1097–102. [PubMed] [Google Scholar]
- 19.Hurtado A. Studies at high altitude. Blood observations on Indian natives of the Peruvian Andes. Am J Physiol. 1932;100:487–505. [Google Scholar]
- 20.Mortimer EA, Jr, Monson RR, MacMahon B. Reduction in mortality from coronary heart disease in men residing at high altitude. N Engl J Med. 1977;296:581–5. doi: 10.1056/NEJM197703172961101. [DOI] [PubMed] [Google Scholar]
- 21.Pearson TC, Wetherley-Mein G. Vascular occlusive episodes and venous haematocrit in primary proliferative polycythaemia. Lancet. 1978;2:1219–22. doi: 10.1016/s0140-6736(78)92098-6. [DOI] [PubMed] [Google Scholar]
- 22.Sharma SC, Balasubramanian V, Chadha KS. Platelet adhesiveness in permanent residents of high altitude. Thromb Haemost. 1980;42:1508–12. [PubMed] [Google Scholar]