

Abstract
Objective:
In this study, we aimed to assess knowledge, attitude, and practice of community pharmacists toward administration of over-the-counter (OTC) antidiarrheal drugs in our city pharmacies, Shiraz, Iran.
Methods:
In this descriptive cross-sectional study, 90 pharmacies among 128 pharmacies in our city were randomly chosen. The study was designed into two phases: A standard questionnaire to determine the level of knowledge and attitude of pharmacists and a simulated client method to evaluate practice among them. An educational pamphlet was then given to the pharmacists. One month later, knowledge, attitude, and performance of studied pharmacists were evaluated again using the same method.
Findings:
Our results showed that an average consultation time by female pharmacists was considerably more than male pharmacists (P < 0.001). Before intervention, only 37.8% of pharmacists performed appropriately by prescribing the proper medicine while this increased to 58.44% after intervention. The average score of pharmacists’ knowledge was statistically increased (P < 0.001) and the pharmacists’ performance was significantly improved (P < 0.001) after the educational intervention. In related to the attitude, pharmacists’ tendency toward prescribing oral rehydration salt solutions (ORS) (P < 0.001) and their belief about the great effect of ORS on the treatment of diarrhea increased significantly after the intervention.
Conclusion:
It is concluded that training programs such as educational pamphlets and continuing educational seminars may play important roles in increasing pharmacists’ knowledge and therefore improving their performance in prescribing OTC medicines.
Keywords: Attitude, children, community pharmacists, diarrhea, knowledge, over-the-counter drugs, practice
INTRODUCTION
People's access to medicines is mainly determined according to specific rules of each country. In most countries, including America, drugs are divided into two categories: Prescription only medicines (POMs) and over-the-counters (OTCs).[1] According to the Food and Drug Administration (FDA) of America, there are more than 100,000 OTC medicines with thousands of active ingredients.[2] In the meantime, some countries are trying to transfer some medicines from the list of POMs to the list of OTCs, in order to reduce the cost of treatment.[3] Several studies have shown that people also expect the pharmacist to give them enough instructions when they ask for OTC medicines. One study, for example, revealed that 50% of Europeans consult with pharmacists when requesting OTC drugs.[4,5]
One of the most commonly used OTC medicines is antidiarrheal drugs and only 20% of the patients with diarrhea have prescriptions with themselves when they visit pharmacies. Seemingly, 80% of the patients consult with a pharmacist for the treatment of their disease,[6] which shows the patient's tendency to refer to pharmacists before trying a visit to doctor's offices.
As to the complications of diarrhea, it has been long known as an important cause of child morality particularly in developing countries.[7] Each year, about 5 million infants and children lose their lives because of diarrhea-induced dehydration in Latin America, Africa, and Asia.[8] Attempts are routinely made to relieve the problem; for instance, OTC drugs such as oral rehydration salt solutions (ORS) are used to treat diarrhea in children all over the world. In such regard, World Health Organization recommends ORS as a safe and effective treatment in acute diarrhea.[9] However, several studies have reported the administration of inappropriate medicines for the management of diarrhea.[6,10,11] To the depth of our knowledge, little is known about pharmacists’ views on OTC drugs used for the treatment of diarrheas in children in our country, Iran. Considering to the importance of appropriate treatment of diarrhea, especially in children and infants, in this project, we aimed to assess the knowledge, attitude, and practice of community pharmacists, as first-line health care professions, toward the administration of OTC antidiarrheal drugs in our city, Shiraz, Iran. To the best of our knowledge, this is the first pretest–posttest study on this topic.
METHODS
This is a descriptive cross-sectional study done during 5 months (February 2015 to June 2015). Preintervention, postintervention method was followed. The population involved was pharmacists working in pharmacies in Shiraz, one of the biggest cities in Iran.
Sample size was determined using the followed formula:[12]
In this formula, α is equal to 0.05 and z is 95% sentiment, which is 1.96; p is appropriate performance of pharmacist which is 19.23 and d is the accuracy level which is intended to be 8. Therefore, the estimated sample size would be 90. The list of pharmacies was retrieved from FDA of Shiraz University of Medical Sciences (SUMS). Among 182 pharmacies in Shiraz, 90 pharmacies were randomly selected, using random number generator.[13]
For gathering information about the pharmacists’ knowledge and attitude, a thorough questionnaire was carefully designed using reference books and standardized questionnaires.[14,15] In order to collect data about the pharmacists’ practice, the simulated client method was used. The researcher, acting as a client, asked the pharmacist for a drug to treat the diarrhea of his 3-year-old brother in the daytime. He did not give more information to the pharmacist unless he was asked by the pharmacist to provide more information. In this study, incomplete assessment was defined as asking less than three questions out of the study's list of questions and complete assessment was regarded as asking at least four questions, one of which has to be the patient's age. Therefore, the patient's age was considered as a key question to be asked by the pharmacist. Regarding the pharmacists’ knowledge, the cut-off point was assumed as 10.
Following the performance assessment, the pharmacists’ attitude and knowledge were evaluated through the designed questionnaire that was administered by the researcher and filled by the pharmacist in the pharmacy. The questionnaire contained 13 questions to determine the knowledge and 10 questions to assess the attitude. An educational pamphlet was then given to the pharmacists. One month later, the knowledge, attitude, and performance of the pharmacists were re-studied in the same procedure by a different client.
SPSS software Version 18 (SPSS, Inc., Chicago, IL, USA) was used for data analysis. For continuous variables, mean and standard deviation were provided. Differences in proportions were tested by the Pearson Chi-square when assumptions were met; if not, the Fisher's exact test was used. A P < 0.05 was considered as significance level.
RESULTS
In order to assess 90 pharmacists in preintervention phase, 120 pharmacies were visited. About 63 (70%) of the pharmacists were male, and 27 (30%) were female. The age range of the pharmacists was 24–77 years with the average of 42 ± 12 years. In 45 cases, the pharmacist was the owner of the pharmacy as well. Regardless of the gender, 43.3% of the pharmacists were graduated from SUMS. Considering the degree, 2.2% of pharmacists had Bachelor, 96.7% of them had Pharm.D., and 1.1% had Ph.D.
The results of this study showed that consultation time among female pharmacists (111.15 min, in average) was significantly more than male pharmacists (29.95 min, in average) (P < 0.001). However, the mean duration of consultation was not significantly different between founder pharmacists and nonfounder pharmacists (P > 0.05).
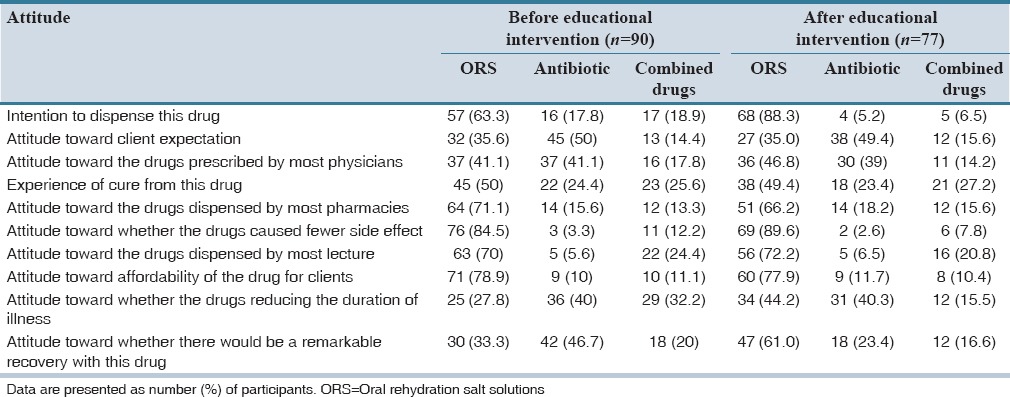
As the results show, even before the intervention, the pharmacists had more tendencies to prescribe ORS than other drugs for the treatment of diarrhea. However, according to the patients’ point of view and their repeated request for antibiotics, the pharmacists thought that antibiotics could have better therapeutic effects on children's diarrhea. Furthermore, the results of the questionnaires revealed that the pharmacists thought that antibiotics had a faster effect and that they could reduce the duration of diarrhea in children. After educational intervention, pharmacists’ tendency toward prescribing ORS (P < 0.001) and their belief about the great effect of ORS on the treatment of diarrhea increased significantly. The results related to pharmacists’ attitudes about the treatment of diarrhea in children is summarized in Table 1.
Table 1.
Attitude of pharmacists about the treatment of children's diarrhea with different drugs before and after the educational intervention
The average knowledge score of the pharmacists was calculated as 8.89 ± 1.35 before educational intervention that increased significantly and reached 11.01 ± 1.04 after the intervention (P < 0.001). Only 37.8% of the pharmacists could get beyond the cut-off point which was 10 whereas this increased to 58.44% after intervention. Moreover, results showed a significant inverse relationship between the pharmacists’ mean score of knowledge and their years after graduation (P = 0.004). In other words, recently graduated pharmacists had more information on OTC medicines used for the treatment of diarrhea than the ones who had graduated much earlier. However, it was not the case after the educational intervention (P = 0.07).
With regard to appropriate questions asked for evaluating the patient by pharmacist, 61 pharmacists (67.8%) asked about the patients’ age as a key question. This percentage significantly increased after the educational intervention (80.5%, P = 0.039).
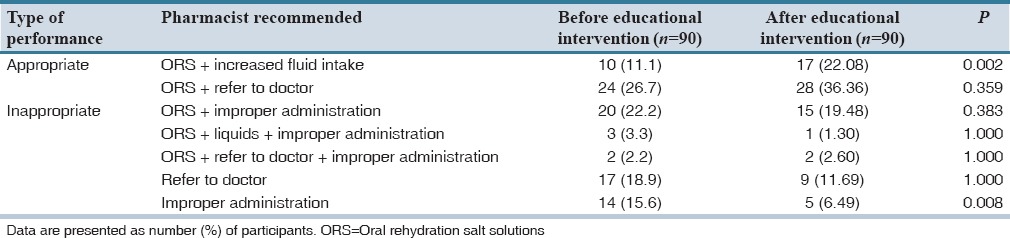
The pharmacists’ initial reactions to the patients’ request for medication (before and after educational intervention) are summarized in Table 2. The number of pharmacists who asked questions before recommendation increased significantly after the invention (P = 0.016). There was no significant difference in other acts of pharmacists before and after the educational invention (P > 0.05). The pharmacists’ final performance data are shown in Table 3. After the educational intervention, the pharmacists showed significantly better performances compared with preintervention state (P < 0.001).
Table 2.
The initial reactions of pharmacists, after patient request for medication before and after the educational intervention
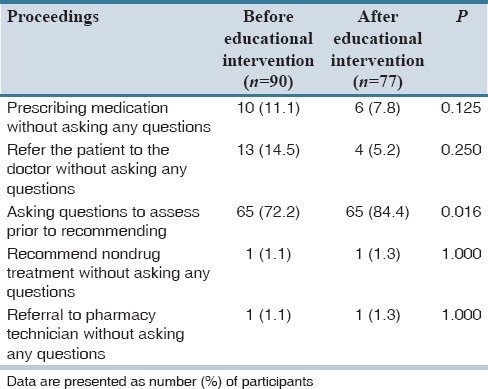
Table 3.
Pharmacists' recommendation after patient request of medication for diarrhea in children before and after the educational intervention
DISCUSSION
The result of the present study showed that pharmacists’ attendance in pharmacies was surprisingly low; more specifically, they were absent in about 25% of references and were not actively present in 24.4%. In another study performed elsewhere in our country, it was found that there were not any pharmacists in 66 out of 133 pharmacies.[12]
According to our results, female pharmacists spent more time for the simulated patients before and after intervention. This is similar to the result of another study done in our country which showed more statistically significant consultation time among female pharmacists compared to males.[12] This finding is not unexpected since women generally make better communication and sympathize better with others than men.
Our results also pointed out that about 60.3% of pharmacists had poor knowledge regarding the application of OTC drugs used for the treatment of children's diarrhea. After the educational intervention, the average score of pharmacists’ knowledge increased significantly and the majority of pharmacists (79.2%) obtained the appropriate knowledge cut-off. This reveals the positive effect of educational intervention on pharmacists’ knowledge.
Regarding the practice, our results indicated that in more than a quarter of cases (27.8%), community pharmacists referred the patient to the doctor immediately after the patient's request without asking him/her any further questions. One of the important points shown in this study was the pharmacists’ lack of familiarity with the patient assessment before advising the treatment recommendation. Therefore, only 37.8% of pharmacists offered appropriate final recommendations, which was far from the ideal practice. Similarly, in another study performed over 101 pharmacies in the Pittsburgh area, 31.7% of the recommendations were appropriate whereas 39.1% were poor and 33.2% were made without prior assessment of the patients’ problems.[16]
It is obvious that failure to completely assess the patients’ problem and improper diagnosis of the patients’ condition could lead to the pharmacists’ inappropriate recommendations. As shown in this study, significantly better performances were seen among the pharmacists after educational intervention compared with preintervention state (P < 0.001) with regard to the prescription of OTC antidiarrheal agents in children. This significant improvement in the functioning shows the usefulness of the educational pamphlets on the community pharmacists’ proper practice.
In addition, it was seen that although pharmacists’ attitude in the field of OTC medicines for the treatment of children's diarrhea was unsatisfactory, their tendency toward prescribing ORS increased significantly and their beliefs about the great effect of ORS on the treatment of diarrhea changed for better after the intervention (P < 0.001). Since pharmacists’ improper attitude may result in their poor performance, improvement in their tendency to prescribe appropriate OTC drugs could be another reason for their better postintervention performance.
The results of this study show that knowledge, attitude, and performance of community pharmacists in prescribing OTC medicines in the field of child diarrhea are not in an ideal condition. It seems that lack of accurate, scientific, and classical knowledge is one of the obvious weaknesses of most community pharmacists leading to inappropriate practice. Training programs such as educational pamphlets and continuing educational seminars may play important roles in increasing pharmacists’ knowledge and therefore improving their performance in prescribing OTC medicines.
AUTHORS’ CONTRIBUTION
Farzaneh Foroughinia: Concepts, Design, Definition of intellectual content, Literature search, Clinical studies, Experimental studies, Data analysis, Statistical analysis, Manuscript preparation, Manuscript editing and review. Pedram Zarei: Literature search, Clinical studies, Experimental studies, Data analysis, Manuscript preparation.
Financial support and sponsorship
Shiraz University of Medical Sciences (grants number: 93-01-05-8321).
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors would like to thank the Center for Development of Clinical Research of Nemazee Hospital for statistical analysis and also Dr. Elham Nasiri for editorial assistance.
REFERENCES
- 1.Taylor J, Berger B, Anderson-Harper H, Grimley D. Pharmacists’ readiness to assess consumers’ over-the-counter product selections. J Am Pharm Assoc (Wash) 2000;40:487–94. [PubMed] [Google Scholar]
- 2.FDA CDER Handbook: Over-the-Counter Drug Products. Archived from the Original on May 12, 2009. [Last retrieved on 2007 Oct 9]. Available from: http://www.fda.gov/downloads/AboutFDA/CentersOffices/CDER/UCM148055.pdf .
- 3.Hughes L, Whittlesea C, Luscombe D. Patients’ knowledge and perceptions of the side-effects of OTC medication. J Clin Pharm Ther. 2002;27:243–8. doi: 10.1046/j.1365-2710.2002.00416.x. [DOI] [PubMed] [Google Scholar]
- 4.Pray WS. Nonprescription Product Therapeutics. 1st ed. Baltimore, MD: Lippincott Williams & Wilkins; 1999. pp. 4–14. [Google Scholar]
- 5.Schulke DG. American Pharmaceutical Association review of literature on prescription to over-the-counter drug switches. Clin Ther. 1998;20(Suppl C):C124–33. doi: 10.1016/s0149-2918(98)80017-9. [DOI] [PubMed] [Google Scholar]
- 6.Das BP, Deo SK, Jha N, Rauniar GP, Naga Rani MA. Knowledge, attitudes and practices (KAP) regarding the management of diarrhea by pharmacists and licensed drug sellers in eastern Nepal. Southeast Asian J Trop Med Public Health. 2005;36:1562–7. [PubMed] [Google Scholar]
- 7.Behrman RE, Kliegman RM, Nelson WE. Infections disease. Nelson text book of pediatrics. 14th edition. Philadelphia: W. B. Saunders co; 1992. [Google Scholar]
- 8.Snyder JD, Merson MH. The magnitude of the global problem of acute diarrhoeal disease: A review of active surveillance data. Bull World Health Organ. 1982;60:605–13. [PMC free article] [PubMed] [Google Scholar]
- 9.The World Health Organization. The Treatment of Diarrhea: A Manual for Physicians and Other Senior Health Workers; 2005. [Last accessed on 2010 Sep 20]. Available from: http://www.whqlibdoc.who.int/publications/2005/9241593180.pdf .
- 10.Saengcharoen W, Lerkiatbundit S. Practice and attitudes regarding the management of childhood diarrhoea among pharmacies in Thailand. Int J Pharm Pract. 2010;18:323–31. doi: 10.1111/j.2042-7174.2010.00066.x. [DOI] [PubMed] [Google Scholar]
- 11.Ogbo PU, Aina BA, Aderemi-Williams RI. Management of acute diarrhea in children by community pharmacists in Lagos, Nigeria. Pharm Pract (Granada) 2014;12:376. doi: 10.4321/s1886-36552014000100002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zargarzadeh A, Mostafavi SA, Chamanara M. Community pharmacists Performance in Management of Cough, Diarrhea and Obesity Using Over-the-counter Medications. J Isfahan Med Sch. 2013;31:161–79. [Google Scholar]
- 13.True Random Number Service. Random Number Generator. [Last cited on 2012 Feb 23]. Available from: http://www.random.org .
- 14.Walker PC. In: Diarrhea. Handbook of Nonprescription Drugs. 14nd ed. Krinsky DL, Berardi RR, editors. Washington, DC: American Pharmacist Association; 2004. pp. 405–32. [Google Scholar]
- 15.D’Arcy PF. The treatment of acute diarrhea information for pharmacists. Geneva: O. Diarrheal Disease control programme, WHO; 1997. [Google Scholar]
- 16.Lamsam GD, Kropff MA. Community pharmacists’ assessments and recommendations for treatment in four case scenarios. Ann Pharmacother. 1998;32:409–16. doi: 10.1345/aph.17287. [DOI] [PubMed] [Google Scholar]