

Abstract
Background
More than one in five patients who undergo treatment for breast cancer will develop breast cancer‐related lymphedema (BCRL). BCRL can occur as a result of breast cancer surgery and/or radiation therapy. BCRL can negatively impact comfort, function, and quality of life (QoL). Manual lymphatic drainage (MLD), a type of hands‐on therapy, is frequently used for BCRL and often as part of complex decongestive therapy (CDT). CDT is a fourfold conservative treatment which includes MLD, compression therapy (consisting of compression bandages, compression sleeves, or other types of compression garments), skin care, and lymph‐reducing exercises (LREs). Phase 1 of CDT is to reduce swelling; Phase 2 is to maintain the reduced swelling.
Objectives
To assess the efficacy and safety of MLD in treating BCRL.
Search methods
We searched Medline, EMBASE, CENTRAL, WHO ICTRP (World Health Organization's International Clinical Trial Registry Platform), and Cochrane Breast Cancer Group's Specialised Register from root to 24 May 2013. No language restrictions were applied.
Selection criteria
We included randomized controlled trials (RCTs) or quasi‐RCTs of women with BCRL. The intervention was MLD. The primary outcomes were (1) volumetric changes, (2) adverse events. Secondary outcomes were (1) function, (2) subjective sensations, (3) QoL, (4) cost of care.
Data collection and analysis
We collected data on three volumetric outcomes. (1) LE (lymphedema) volume was defined as the amount of excess fluid left in the arm after treatment, calculated as volume in mL of affected arm post‐treatment minus unaffected arm post‐treatment. (2) Volume reduction was defined as the amount of fluid reduction in mL from before to after treatment calculated as the pretreatment LE volume of the affected arm minus the post‐treatment LE volume of the affected arm. (3) Per cent reduction was defined as the proportion of fluid reduced relative to the baseline excess volume, calculated as volume reduction divided by baseline LE volume multiplied by 100. We entered trial data into Review Manger 5.2 (RevMan), pooled data using a fixed‐effect model, and analyzed continuous data as mean differences (MDs) with 95% confidence intervals (CIs). We also explored subgroups to determine whether mild BCRL compared to moderate or severe BCRL, and BCRL less than a year compared to more than a year was associated with a better response to MLD.
Main results
Six trials were included. Based on similar designs, trials clustered in three categories.
(1) MLD + standard physiotherapy versus standard physiotherapy (one trial) showed significant improvements in both groups from baseline but no significant between‐groups differences for per cent reduction.
(2) MLD + compression bandaging versus compression bandaging (two trials) showed significant per cent reductions of 30% to 38.6% for compression bandaging alone, and an additional 7.11% reduction for MLD (MD 7.11%, 95% CI 1.75% to 12.47%; two RCTs; 83 participants). Volume reduction was borderline significant (P = 0.06). LE volume was not significant. Subgroup analyses was significant showing that participants with mild‐to‐moderate BCRL were better responders to MLD than were moderate‐to‐severe participants.
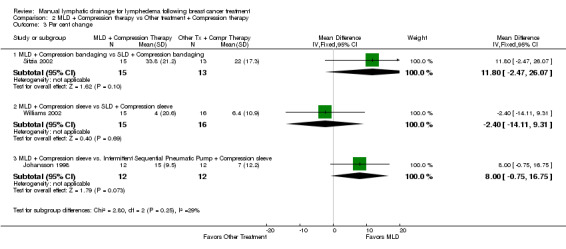
(3) MLD + compression therapy versus nonMLD treatment + compression therapy (three trials) were too varied to pool. One of the trials compared compression sleeve plus MLD to compression sleeve plus pneumatic pump. Volume reduction was statistically significant favoring MLD (MD 47.00 mL, 95% CI 15.25 mL to 78.75 mL; 1 RCT; 24 participants), per cent reduction was borderline significant (P=0.07), and LE volume was not significant. A second trial compared compression sleeve plus MLD to compression sleeve plus self‐administered simple lymphatic drainage (SLD), and was significant for MLD for LE volume (MD ‐230.00 mL, 95% CI ‐450.84 mL to ‐9.16 mL; 1 RCT; 31 participants) but not for volume reduction or per cent reduction. A third trial of MLD + compression bandaging versus SLD + compression bandaging was not significant (P = 0.10) for per cent reduction, the only outcome measured (MD 11.80%, 95% CI ‐2.47% to 26.07%, 28 participants).
MLD was well tolerated and safe in all trials.
Two trials measured function as range of motion with conflicting results. One trial reported significant within‐groups gains for both groups, but no between‐groups differences. The other trial reported there were no significant within‐groups gains and did not report between‐groups results. One trial measured strength and reported no significant changes in either group.
Two trials measured QoL, but results were not usable because one trial did not report any results, and the other trial did not report between‐groups results.
Four trials measured sensations such as pain and heaviness. Overall, the sensations were significantly reduced in both groups over baseline, but with no between‐groups differences. No trials reported cost of care.
Trials were small ranging from 24 to 45 participants. Most trials appeared to randomize participants adequately. However, in four trials the person measuring the swelling knew what treatment the participants were receiving, and this could have biased results.
Authors' conclusions
MLD is safe and may offer additional benefit to compression bandaging for swelling reduction. Compared to individuals with moderate‐to‐severe BCRL, those with mild‐to‐moderate BCRL may be the ones who benefit from adding MLD to an intensive course of treatment with compression bandaging. This finding, however, needs to be confirmed by randomized data.
In trials where MLD and sleeve were compared with a nonMLD treatment and sleeve, volumetric outcomes were inconsistent within the same trial. Research is needed to identify the most clinically meaningful volumetric measurement, to incorporate newer technologies in LE assessment, and to assess other clinically relevant outcomes such as fibrotic tissue formation.
Findings were contradictory for function (range of motion), and inconclusive for quality of life.
For symptoms such as pain and heaviness, 60% to 80% of participants reported feeling better regardless of which treatment they received.
One‐year follow‐up suggests that once swelling had been reduced, participants were likely to keep their swelling down if they continued to use a custom‐made sleeve.
Keywords: Female, Humans, Bandages, Breast Neoplasms, Breast Neoplasms/therapy, Drainage, Drainage/methods, Lymphedema, Lymphedema/etiology, Lymphedema/therapy, Massage, Quality of Life, Randomized Controlled Trials as Topic
Plain language summary
Manual lymphatic drainage for lymphedema following breast cancer treatment
Background
More than one in five of breast cancer patients will develop breast cancer‐related lymphedema (BCRL). BCRL is a swelling that can occur in the arm, breast, or chest wall as a result of breast cancer surgery and/or radiation therapy. BCRL can negatively impact comfort, function, and quality of life
Manual lymphatic drainage (MLD) is a hands‐on therapy that is commonly used for BCRL and often as part of complex decongestive therapy (CDT). CDT consists of MLD, compression bandaging, lymph‐reducing exercises (LREs), and skin care.
The Review Questions
Is MLD safe and effective in treating BCRL?
Study Characteristics
We found six trials published through May, 2013, totaling 208 participants.
Key Results
When women were treated with a course of intensive compression bandaging, their swelling went down about 30% to 37%. When MLD was added to the intensive course of compression bandaging, their swelling went down another 7.11%. Thus, MLD may offer benefit when added to compression bandaging.
Examining this finding more closely showed that this significant reduction benefit was observed in people with mild‐to‐moderate lymphedema when compared to participants with moderate‐to‐severe lymphedema. Thus, our findings suggest that individuals with mild‐to‐moderate BCRL are the ones who may benefit from adding MLD to an intensive course of treatment with compression bandaging. This finding, however, needs to be confirmed by further research.
When women were given a standard elastic compression sleeve plus MLD and compared to women who received a standard compression sleeve plus a nonMLD treatment, results were mixed (sometimes favoring MLD and sometimes favoring neither treatment.)
One‐year follow‐up suggests that once swelling had been reduced, participants were likely to keep their swelling down if they continued to use a custom‐made sleeve.
MLD is safe and well tolerated.
Findings were contradictory for function (range of motion), with one trial showing benefit and the other not. Two trials measured quality of life, but neither trial presented results comparing the treatment group to the control, so findings are inconclusive.
No trial measured cost of care.
Quality of the Evidence
Trials were small ranging from 24 to 45 participants. Most trials appeared to randomize participants adequately. However, in four trials the person measuring the swelling knew what treatment the participants were receiving, and this could have biased results.
Background
Description of the condition
More than one in five women with breast cancer will develop breast cancer‐related lymphedema (BCRL) (DiSipio 2013; Paskett 2012). BCRL is an abnormal accumulation of lymph fluid in the tissues on the affected side of the body following breast cancer treatment as a result of surgical procedures and/or radiation therapy. Breast cancer surgery can cause lymphedema through several mechanisms: surgical removal of lymphatic structures such as nodes and vessels can impair lymph carrying capacity. Surgical scarring can diminish lymph transport by occlusion of lymph vessels and/or loss of elasticity in lymph vessels. Surgical removal or damage of muscle tissue can diminish the muscle’s compressive force on the lymph vessels and impair the "muscle pump" (Ridner 2013). Radiation therapy can also cause BCRL through several mechanisms including direct tissue damage, node damage, and/or scarring and fibrosis, all reducing lymph carrying capacity (Ahmed 2011; Kwan 2010).
Although recent changes in diagnosis and treatment of breast cancer (such as sentinel node biopsy, changes in radiation therapy, and less invasive surgical techniques due to earlier diagnosis) have reduced the risk of BCRL, BCRL remains a major problem for women with breast cancer. Six‐month prevalence rates, for any six months within a three‐year window, have been estimated at 23% to 29% (Paskett 2007). Prospective incidence rates of BCRL range between 20% to 40% for the first three years following breast cancer surgery (Armer 2009; Clark 2005; Geller 2003). Incidence rates vary according to the type of breast cancer treatment received, with women who receive both axillary radiation and axillary lymph node resection showing the highest incidence (Shah 2012).
Risk factors for BCRL include higher stage of breast cancer, higher number of lymph nodes removed, obesity, poorer performance status, receipt of adjuvant chemotherapy or radiation therapy (Helyer 2010; Miaskowski 2013) and certain genes (Miaskowski 2013). Exercise such as strength training has been associated with lower risk of BCRL (Park 2008; Swenson 2009).
BCRL can affect the arm, hand, fingers, wrist, elbow, shoulder, neck, breast, chest or any combination of these areas. Arm BCRL is the most widely studied and is classified according to the excess volume of the affected arm compared to the unaffected arm. A common arm classification is mild (< 20% excess volume), moderate (20% to 40% excess volume) and severe (> 40% excess volume) (Partsch 2010). Arm BCRL is often not diagnosed until the patient, herself, notices subtle signs of swelling such as the inability to wear rings or watches, or has symptoms such as discomfort, heaviness or tightness in the limb or region. In some cases the skin may appear shiny, veins may be less visible, and tissue may feel firmer than normal.
Truncal BCRL (chest, axilla, shoulder, breast and/or upper back) has not been as well documented as arm BCRL (Brennan 1996) but is also associated with physical and psychological sequelae. Truncal BCRL may be assessed with skin fold calipers, tissue dielectric constant, ultrasonic skin thickness measurement or bioimpedance. However, visual observation remains the most practical assessment of truncal lymphedema: for example, asymmetry, bra strap and seam indentations, orange peel phenomenon, changes in skin color, palpation of tissue texture and skin folds between affected and non‐affected side. Truncal BCRL may present with or without arm BCRL and visa versa (Ridner 2010b).
In addition to the excess fluid build up, BCRL can create considerable disability, pain (Brennan 1996), limited motion, heaviness, numbness, psychosocial morbidity (Mirolo 1995; Passik 1998), and diminished quality of life (Brennan 1992; Tobin 1993). Left untreated, BCRL can progress, and the skin over the affected area can lose its elasticity; and the person can become prone to repeated infections and fibrosis (Petrek 1998). However, early detection and treatment of BCRL can both reduce lymphatic swelling and maintain that reduction over time (Hayes 2012). Thus, altering the progression of this potentially disabling condition through effective early intervention is important.
Description of the intervention
Manual lymphatic drainage (MLD) is a light but very specific hands‐on therapy designed to reduce lymph swelling by enhancing lymphatic drainage. MLD therapists are trained in the anatomy and physiology of the lymphatic system to facilitate lymph drainage of the vessels. MLD is sometimes administered alone, but often is administered as part of a fourfold conservative treatment known as complex decongestive therapy (CDT). The four components of CDT are MLD, compression therapy, lymph‐reducing exercises and skin care.
CDT is the most common treatment for many types of lymphedema and involves two phases. In Phase 1, which lasts two to four weeks, the goal is to reduce the swelling through MLD and compression bandaging. The therapist also instructs the patient on good skin care practices to ensure the skin remains healthy and free of infection and prescribes specialized lymph‐reducing exercises. Modifications of CDT can involve replacing the compression bandaging with a compression sleeve (Cohen 1998).
In Phase 2, after the limb is sufficiently reduced in volume, the patient is then fitted with a compression garment (Foldi 1998). In Phase 2, the goal is to maintain the volume reductions achieved in Phase 1 through self‐administered compressive therapy, lymph‐reducing exercises, and self‐lymphatic drainage. MLD is generally not prescribed in Phase 2 unless needed; however, there is evidence to suggest that many participants continue with maintenance MLD in addition to self‐massage (Ridner 2010a; Ridner 2012). Also, the patient continues with skin care.
For the purposes of this review, "compression therapy" is used to describe the compression part of the lymphedema therapy, whether it is bandaging, sleeve, or custom‐fitted garment. Many studies have shown that the compression therapy part of the CDT, usually beginning with compression bandaging and then later through a compression sleeve, can effectively reduce swelling. CDT is used synonymously in the medical literature with complete decongestive physiotherapy or decongestive lymphatic therapy.
How the intervention might work
Under normal conditions, the body’s circulation results in fluid exchange at the arterial side of the capillaries into the interstitial space. Most of this interstitial fluid is returned into the circulation by the venous ends of the capillaries. The remaining interstitial fluid along with protein molecules, bacteria, viruses, and waste products are picked up by small lymph vessels and becomes lymphatic fluid (Ridner 2013). The research of Levick 2010 suggests that tissue fluid balance is critically dependent on lymphatic function in most tissues.
The lymphatic fluid is carried to larger lymph vessels, and eventually is emptied back into the venous circulation (Lawenda 2009). The lymphatic fluid is not ‘pumped’ through the body by a central pump like the heart; rather, it is moved by the rhythmic contractions of the muscular walls of lymphangions, which are segmented portions of the lymph vessels separated by a valve on either side. The sequential, segment‐to‐segment contractions of the lymphangions are under the control of the autonomic nervous system, but can be augmented by external stimuli on the lymphatics, such as from compression of surrounding muscles and filamentary support structures or local arterial pulsation. When damage occurs to the lymphatic system, drainage of interstitial fluid may become compromised. The resulting lymph stasis causes a build up of interstitial fluid or the condition known as ‘lymphedema’.
MLD is a type of specialized manual therapy based on the anatomy of the lymph system. It is believed to work by enhancing movement of lymph fluid, decreasing interstitial fluid, and softening fibrosis (Moseley 2007). It is proposed that MLD can 'assist nature' by stimulating the natural peristaltic contractions of the lymphangions (Mislin 1961). Thus MLD reduces swelling by stimulating lymphangion pumping, reducing hydrostatic resistance to lymph flow, and rerouting lymph away from areas of stasis and into viable lymphatic vessels (Leduc 1998). The ability of MLD to reduce lymphatic swelling has been well demonstrated (Williams 2010; Williams 2002).
Because MLD is frequently administered as part of CDT, the other three components of CDT are briefly described below.
Compression therapy helps reduce interstitial fluid by decreasing its formation and preventing lymph back flow into the interstitial space (Moseley 2007). Compression also assists the pumping action of muscles by creating a resistance against which muscles can work. This is called the "muscle pump" effect. Compression therapy in Phase 1 is usually done using multi‐layered compression bandaging, which consists of gauze for wrapping the fingers and hand, a stockinette sleeve which protects the skin, soft cotton wrap or high density foam and two to three layers of short‐stretch bandaging. Short‐stretch bandages are used so that as the limb is moved, the muscles contract against the resistance of the inelastic bandages. Distinct variations within the sub‐bandage pressures can enhance lymphatic and venous function. Compression therapy in Phase 2 of CDT is designed to maintain the volume reductions from the first phase, and may be achieved by use of a compression sleeve or custom‐fitted garment, with or without a glove or hand gauntlet that is worn during the day. In some cases, compression bandages are worn at night.
Lymph‐reducing exercises aim specifically at promoting lymph flow and reducing swelling. These exercises involve "active, repetitive, non‐resistive motion of the involved body part" and "are similar to some movements of low impact Tai Chi and Qigong" and always done "with compression on the involved extremity" (NLN 2011). The compression allows the muscles to contract against resistance creating a more effective "muscle pump" which enhances lymphatic and venous return. Examples of lymph‐reducing exercises are available on the web (Zuther 2011a).
Skin Care. People with BCRL are at increased risk of skin infection because the swelling from BCRL stretches the skin putting it at increased risk of injury. Furthermore, the high protein content of lymphatic fluid serves as a medium where bacteria may thrive causing a skin infection known as cellulitis. Cellulitis can spread to deeper tissues and/or systemically through the body. Thus, in skin care education, participants learn how to keep the skin supple and protected from breaks and tears, and how and why to use pH‐neutral creams or lotions, and low‐pH soaps to discourage bacterial colonization.
Why it is important to do this review
Women with BCRL show medical costs $14,887 to $23,167 higher than women with breast cancer without BCRL. Indirect costs (e.g., work days lost) are also higher for BCRL (Shih 2009). Early detection and treatment can reduce overall costs by maintaining affected limbs at minimal volumes (Stout 2012b) and treating other comorbidities before they become chronic (Hayes 2012). Thus, early and cost‐effective interventions are important.
MLD is generally considered within the context of CDT, and its relative contribution to CDT needs to be evaluated. CDT is recognized as the therapy of choice by "the International Society of Lymphology (ISL), the National Lymphedema Network (NLN), the Lymphology Association of North America (LANA), the American Lymphedema Framework Project (ALFP), and the North American Lymphedema Education Association (NALEA)" (Zuther 2011a). Practice guidelines (Harris 2012), reviews (Brennan 1996; Kligman 2004; Megans 1998; Rockson 1998), and a consensus statement (Bernas 2001) also recommend CDT as the preferred treatment for BCRL.
However, a practitioner‐based survey (Kärki 2009) shows that although MLD is theoretically given as part of CDT, in reality, MLD is often given without compression therapy. Thus, MLD needs to be evaluated both within the context of CDT and as a stand‐alone modality.
Systematic reviews examining MLD for BCRL present contradictory findings from no benefit (Huang 2013), to small benefit (McNeely 2011), to substantial benefit (Moseley 2007) to inconclusive benefit (Devoogdt 2010). This review is the first to use primarily individual patient data to calculate missing or unreported primary outcomes, and thus explore the current contradictory findings of present reviews.
It is also important to assess whether there are certain groups of participants who may be responders to MLD. McNeely 2004, for example, observed that participants with mild (< 15% excess volume at baseline) or early (< 12 months' BCRL duration) appeared to benefit from MLD more than those with moderate/severe BCRL, or those with durations 12 months or more. This requires further exploration. This review is the first to utilize available individual patient data to further explore possible subgroups of responders.
Objectives
To assess the efficacy and safety of manual lymphatic drainage (MLD) in treating breast cancer‐related lymphedema (BCRL).
Methods
Criteria for considering studies for this review
Types of studies
We included randomized or quasi‐randomized (i.e., allocated by alternate assignment, date of birth etc) trials of any language.
Types of participants
We included participants who have been diagnosed with BCRL in any body area (i.e., arm, hand, trunk).
Arm BCRL diagnosis has been defined as any of the following. Compared to the unaffected arm, the affected arm had (1) a 2‐cm or greater increase at any point on an arm circumference measure, or (2) a 200 mL or greater increase in water displacement measure, or (3) a 10% or greater excess volume. If Bioimpedance or Tissue Dialectric Constant was used as the outcome, we accepted the criteria for BCRL defined by the authors. Truncal BCRL definitions have been less clearly defined in the medical literature and, therefore, we accepted definitions as specified by the authors of those trials.
Types of interventions
We included trials where MLD was given to one group and not to the other and, thus, could be evaluated.
Types of outcome measures
Primary outcomes
The primary volumetric outcomes were selected because all of them take into consideration the volume of the unaffected limb in the formulae.
(1) Volumetric changes in arm, hand, breast, or trunk
For the arm, the volume could be measured in any of the following ways, all of which made a comparison with the unaffected side.
Lymphedema volume (LE volume) ‐ defined as the amount of excess fluid in mL remaining in the arm after treatment, calculated by subtracting the unaffected arm volume after treatment from the affected arm volume after treatment.
Volume reduction ‐ defined as the amount of fluid reduction in mL from before to after treatment, calculated by subtracting the lymphedema volume of the affected arm at the end of treatment from the lymphedema volume of the affected arm before treatment.
Per cent reduction ‐ the proportion of fluid reduced relative to the baseline excess volume, calculated as volume reduction divided by baseline lymphedema volume multiplied by 100.
For additional explanations of these terms see Table 1 .
1. Volumetric Definitions and Formulae.
| Volumetric Outcome | Definition / Explanation | Formula | Other terms for this outcome in the included studies |
| Lymphedema Volume | The excess volume in the limb. The volume is measured in milliliters (mL). It is called ‘lymphedema volume’ because it is the amount of the limb volume that is attributed to lymphedema. Lymphedema volume is NOT the total volume of the limb. To calculate the lymphedema volume, you have to compare the affected limb to the unaffected limb by subtracting. In this review, we are interested in the lymphedema volume (or excess volume) that remains in the limb after treatment. | Post‐treatment total volume of the affected arm minus post‐treatment total volume of the unaffected arm. |
Lymphedema volume has also been called absolute lymphedema volume, post‐intervention volume (McNeely 2004), and excess limb volume (Williams 2002) |
| Volume Reduction | An estimate of how much the limb has been reduced (in ml) presumably from the treatment. | Lymphedema volume at baseline minus the lymphedema volume after treatment. OR Excess volume before treatment minus the excess volume after treatment. |
Volume reduction has also been called the mean lymphedema volume reduction (Johansson 1998; Johansson 1999) and mean change lymphedema volume (McNeely 2004) |
| Per cent Reduction | The decrease in excess volume relative to the amount of excess volume at baseline. Both the lymphedema volume and the volume reduction are considered absolute values not relative values. However, when absolute values are used, a person with a large excess limb volume might get a 2% reduction, but the amount can look large because the beginning volume was large. By contrast, a person with a small beginning volume, can get a 30% reduction, and it can look small in absolute terms. Thus, it is valuable to have a third way to think about lymphedema outcomes, and that is to look at the per cent change because that is a relative value. | Difference Test A – Difference Test B ____________________________________ x 100 Difference Test A Where difference is the affected arm volume minus the unaffected arm volume (McNeely 2004) Another way to think of per cent reduction is this formula: Excess volume at baseline – Excess volume post‐treatment ______________________________________________x100 Excess volume at baseline |
Per cent Reduction has also been called the percentage lymphedema reduction (Johansson 1998; Johansson 1999), per cent change, per cent reduction in lymphedema volume (McNeely 2004), percentage change in excess limb volume (Sitzia 2002) |
Change could also be measured through skin thickness, bioimpedance or Tissue Dielectric Constant.
(2) Adverse events
Follow‐up times
Follow‐up times are defined from the time of the last MLD treatment.
Immediate follow‐up: One day to two weeks following the last treatment.
Short‐term follow‐up: More than two weeks but less than three months.
Intermediate‐term follow‐up: Three months to less than one year.
Long‐term follow‐up: One year or more.
Secondary outcomes
(1) Functional measures
Range of motion
Strength
(2) Subjective sensations
(3) Quality of life and other psychosocial outcomes
(4) Cost of care
(5) Any other outcome reported by the trial
Search methods for identification of studies
Electronic searches
We searched the following databases.
(a) The Cochrane Breast Cancer Group's Specialised Register. Details of the search strategies used by the Group for the identification of studies and the procedure used to code references are outlined in the Group's module (www.mrw.interscience.wiley.com/cochrane/clabout/articles/BREASTCA/frame.html). Trials coded with the key words 'lymphoedema', 'lymphedema', 'complete decongestive therapy', 'complex decongestive therapy', 'manual lymphatic drainage', 'complete decongestive physiotherapy', 'sequential pneumatic compression', and 'decongestive lymphatic therapy' were extracted and considered for inclusion in the review.
(b) MEDLINE (via OvidSP) (until 24 May 2013). See Appendix 1 for the search strategy.
(c) Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library, Issue 4, April 2013). See Appendix 2 for the search strategy.
(d) Embase (via Embase.com) (until 24 May 2013). See Appendix 3 for the search strategy.
(e) The WHO International Clinical Trials Registry Platform (ICTRP) search portal (http://apps.who.int/trialsearch/Default.aspx), for all prospectively registered and ongoing trials until 23 May 2013. See Appendix 4 for the search strategy.
Searching other resources
Bibliographic searching
We reviewed references lists of retrieved studies.
Personal communication
We contacted lymphedema investigators to provide details of any outstanding clinical trials and any relevant unpublished material.
Grey literature searching
We handsearched the journal Lymphology (Time period searched ‐ July 2004 ‐ May 2013).
We searched a private lymphedema database of 721 records developed and maintained by one of the review authors (RW).
We searched our own files on Lymphedema for published articles, unpublished studies, ongoing studies, conference proceedings, notes, and contact details of researchers in the field.
-
We searched the following Lymphedema web sites.
The British Lymphology Society (www.thebls.com) (July 2004 and May 2013).
The National Lymphedema Network (www.lymphnet.org) (July 2004 and May 2013).
Australasian Lymphology Association (www.lymphoedema.org.au) (July 2004 and May 2013).
International Society of Lymphology (http://www.u.arizona.edu/˜witte/ISL.htm) (July 2004 and May 2013).
Data collection and analysis
Selection of studies
Two review authors per trial (KJ, RW, DH, JE, MM) assessed the titles and abstracts from reference lists for possible inclusion. These review authors read the full text of articles to make the final decision for inclusion. Disagreements were resolved by discussion (KJ, RW, DH, JE, MM). When inclusion was still questionable even with the full text, the author of the article was contacted (JE) to determine whether the article met inclusion criteria. Duplicate publications of the same study were noted, but each trial was counted only once.
We planned to include trials of all languages; however, we did not need to obtain translations of any trials as all relevant trials were published in English.
Data extraction and management
At least two review authors per trial (TB, DH, LB, JE) extracted the characteristics for each trial. The results were compared, disagreements resolved by discussion (JE, EM) and a composite table was created. We extracted information on the trial design (parallel or cross‐over), number randomized/analyzed, recruitment method and location where study took place, country of study, definition of LE used in the study, area of the body (i.e. arm, trunk) assessed, method of assessment (i.e. water displacement, circumference using measuring tape), inclusion/exclusion criteria, outcomes, follow‐up times, adverse events, dropouts and withdrawals, and findings as they were reported in the paper.
When there was more than one publication for a study, we used the primary publication and listed this as the primary publication and then used the other publications for supplementary information.
Assessment of risk of bias in included studies
Two review authors (EM, JE) per trial independently assessed risk of bias, rating each risk‐of‐bias item as "low risk of bias", "unclear", or "high risk of bias" based on the Cochrane Handbook for Systematic Reviews of Interventions recommendations (Higgins 2011). When information was missing from the publication, we contacted the authors when possible. Disagreements were resolved by discussion (EM, JE). Our reasoning for each rating is described in the Characteristics of included studies.
In addition to the pre‐specified 'Risk of bias' items, we added 'Treatment Adherence' as a further potential source of bias. We consider adherence with therapy to be a vital component because in the first phase of treatment, adherence means receiving the prescribed therapy sessions as planned and following the home regimen. The second phase of complete decongestive therapy (CDT/CDP) (the maintenance phase), depends almost exclusively on participants' adherence with the home regimen (compression therapy, exercises, skin care, self‐massage) as there is theoretically little to no treatment from practitioners. Thus, adherence has two dimensions: (1) whether participants attended their required number of sessions, and (2) whether participants performed their home self‐care regimens.
For the first phase of treatment, a trial was rated as "low risk of bias" if the results stated the mean or median number of sessions attended, and if that number was close to the target number of sessions in the methods section. A trial was rated as "unclear" if there was no mention of the number of total sessions participants attended, and "high risk of bias" if the number of sessions attended was notably lower than the target number described in the methods section.
For the second phase of treatment, a trial was rated as "low risk of bias" if it mentioned that there was a method such as a diary to check self‐care adherence AND that method showed that there was high adherence. A trial was rated as "unclear" if there was a method stated to measure adherence but no mention of the results of that method. A trial was rated as "high risk of bias" if there was a method stated to measure adherence and the results showed that there was high non‐adherence with self‐care.
We also assessed the adequacy of the MLD treatments because inadequate treatments could bias results towards a type II error (false negative). There are different types of MLD, but similar principles are followed in each. Two MLD therapists per trial (MM, CT, KJ, DK) were given the excerpts of the MLD descriptions, inclusion criteria and other relevant methods, but were blinded to the study authors/citation. They were asked to rate the MLD treatment as 'adequate', 'not adequate', or 'not enough information to decide'. Disagreements were resolved by discussion.
Measures of treatment effect
We analyzed continuous data (i.e., volumetric changes or visual analogue scales) as mean differences with 95% confidence intervals. The only dichotomous outcome, adverse events, was not a pooled effect, and therefore, reported in absolute numbers in the Characteristics of included studies table.
Unit of analysis issues
The only unit of analysis issue we anticipated was the possible use of cross‐over designs, in which we made the a priori decision to use only first‐cycle data.
Dealing with missing data
To minimize the issue of missing data on the primary outcome of volumetric change, we obtained the raw data from as many trials as we could. We were able to obtain volumetric data on four of the six trials. Thus, if only one of the three volumetric change outcomes was presented in the paper, we were able to calculate the other two from the raw data. To minimize the issue of missing data for the dichotomous outcome (adverse events), we obtained information from the authors if there was nothing reported in the papers.
Assessment of heterogeneity
We used the Chi2 test (Cochran 1954) and the I2 statistic (Higgins 2003) to test for heterogeneity. For the Chi2 test, our cut point was a P < 0.10, and for the I2 statistic, our cut point was > 50%. If there was evidence of heterogeneity, we planned to use a random‐effects model (DerSimonian 1986). If there was no evidence of statistically significant heterogeneity, we planned to use a fixed‐effect model (Mantel 1959). For comparison purposes, we calculated both fixed‐effect and random‐effects models on pooled statistics.
Assessment of reporting biases
To minimize the effect of publication bias, we searched the gray literature, wrote to authors of trials, and handsearched the journal, Lymphology.
Data synthesis
We entered trial data into Review Manger 5.2 (RevMan) and pooled data using a fixed‐effect model of inverse variance. We analyzed continuous data as mean differences with 95% confidence intervals.
We extracted outcomes from the papers and recorded them in the Characteristics of included studies table. Outcomes were pooled when sufficient data were available in the papers or from the trialists' data sets. Outcomes that were not able to be pooled are described in narrative form in the Results section.
Subgroup analysis and investigation of heterogeneity
We conducted subgroup analyses using the per cent volume reduction as the outcome measure, the statistical measure of mean per cent reduction, and a fixed‐effect model in RevMan.
BCRL Severity: We used individual patient data for the subgroup analysis and combined data from trials with similar designs, i.e., MLD + compression bandaging versus compression bandaging alone (trial design: MLD + x versus x alone) (Johansson 1999: McNeely 2004 ) or MLD + compression sleeve versus nonMLD treatment + compression sleeve (trial design: MLD + x versus nonMLD + x) (Johansson 1998; Williams 2002). We dichotomized the baseline per cent excess volume as mild (< 15% ) versus moderate/severe BCRL (> 15%) according to McNeely 2004. We also performed the same analyses using the commonly accepted more conservative estimates of mild LE (< 20% excess volume), moderate (20% to 40% excess), and severe (> 40% excess) (Partsch 2010).
We also wanted to explore whether there was an identifiable per cent excess volume cut point (other than the a priori conventional cut points for "mild") that would be associated with response to MLD. We dichotomized the per cent excess volume by one percentage point at a time beginning at 20%, to investigate whether there would be a highest cut point where statistical significance would be evident.
BCRL Duration: Based on earlier findings by McNeely 2004, we also explored whether BCRL of shorter duration (less than 12 months) compared to 12 months or more would be associated with response to MLD. Duration of BCRL was defined as the time since the diagnosis of BCRL. We explored other duration cut points in six‐month increments in either direction from the original 12‐month cut point (i.e., 18 months, 24 months and six months) to further explore whether there was a temporal cut point associated with response to MLD.
Sensitivity analysis
Due to the different treatment and control groups, we did not have a sufficient number of trials in any comparison category to conduct sensitivity analysis. However, whenever we pooled data, we calculated both the fixed‐effect and random‐effects models for comparison purposes.
Results
Description of studies
Results of the search
One thousand, one‐hundred and ten records were retrieved through the search strategies and other handsearched sources. After removing duplicates, we had 834 records. Although we did fairly extensive searching of gray literature, we did not find any trial that did not also appear in at least one electronic database. Of the 834 records remaining after duplicate removal, we excluded 805 based on the information in the title and/or abstract, primarily because they did not represent original research but rather pertained to the management of lymphedema in general, instructions for manual lymphatic drainage (MLD), or benefits of MLD in general terms. Of those abstracts that did present original research, our major reasons for excluding them were either that the study participants were not exclusively breast cancer‐related lymphedema participants; there was no control group; or interventions were given other than MLD. Refer to the Characteristics of excluded studies section.
We retrieved the full papers for the remaining 29 citations. After full‐text review, we excluded 23 papers and these are listed with the reasons in the Characteristics of excluded studies. Six trials met the inclusion criteria (Andersen 2000; Johansson 1998; Johansson 1999; McNeely 2004; Sitzia 2002; Williams 2002). Refer to Figure 1.
1.

Study flow diagram for review.
Included studies
There were six included studies: Andersen 2000; Johansson 1998; Johansson 1999; McNeely 2004; Sitzia 2002; Williams 2002. The Characteristics of included studies table shows the most important characteristics of these included trials. All trials were in English although country of trial varied: Canada (McNeely 2004), Denmark (Andersen 2000), Sweden (Johansson 1998; Johansson 1999 ), and United Kingdom (Sitzia 2002; Williams 2002).
Interventions used in the trials
All trials combined MLD with some form of compression therapy. MLD was not given as a stand‐alone treatment in any of the trials, and complex decongestive therapy (CDT) was not given as the baseline intervention in any of the trials.
Trials fell into three categories.
(1) MLD + standard physiotherapy versus standard physiotherapy
One trial assessed standard physiotherapy (compression therapy, lymph‐reducing exercises (LREs), skin care), with or without MLD (Andersen 2000). Compression therapy was a two‐stage process: For the first couple of weeks, participants used decreasing sizes of Jobst compression garments to reduce the edema, then they were fitted for a custom‐made sleeve‐and‐glove garment.
(2) MLD + compression bandaging versus compression bandaging
Two trials assessed the effectiveness of MLD as an adjunct to compression bandaging (Johansson 1999; McNeely 2004). Thus, baseline compression bandaging was given to both groups, and MLD was given to one group and not the other.
(3) MLD + compression therapy versus nonMLD treatment + compression therapy
Three trials (Johansson 1998; Sitzia 2002; Williams 2002) assessed MLD compared with another active treatment. Thus, baseline compression therapy was given to both groups. MLD was given to one group and a different nonMLD treatment added to the control group. The nonMLD treatment for the control group was intermittent sequential pneumatic pump in one trial (Johansson 1998) and simple lymphatic drainage in the other two trials (Sitzia 2002; Williams 2002). Simple lymphatic drainage can be administered by a therapist or by the patient, herself, because it is designed to facilitate lymphatic movement in the areas of the body by focusing on areas that the patient can reach. Therefore, the back is not treated in simple lymphatic drainage, but the chest and axilla are. In one trial (Williams 2002), the patient performed the simple lymphatic drainage, and in the other simple lymphatic drainage trial (Sitzia 2002), the therapist performed simple lymphatic drainage.
Timing of addition of MLD
In four trials, compression therapy was given concurrently with MLD (Andersen 2000; McNeely 2004; Sitzia 2002; Williams 2002) while in two trials (Johansson 1998; Johansson 1999), compression therapy was administered two weeks prior to MLD, and then in the third week, MLD was added to compression therapy.
Types of baseline interventions
CDT was not given in any trial. Five trials gave compression therapy (Johansson 1998; Johansson 1999; McNeely 2004; Sitzia 2002; Williams 2002); one trial gave standard therapy: compression sleeve, lymphedema exercises and skin care to both groups, with or without MLD (Andersen 2000). No trial assessed MLD as a stand‐alone intervention.
Types of baseline compression therapy
Type of baseline compression therapy given to both treatment and control groups varied among trials. Three trials used compression bandaging (Johansson 1999; McNeely 2004; Sitzia 2002); three trials used compression sleeves (Andersen 2000; Johansson 1998; Williams 2002).
Outcomes reported
All trials assessed arm volume reduction as the primary outcome (either as a per cent reduction, lymphedema volume, or volume reduction). Only one trial also assessed truncal lymphedema (Williams 2002).
Trial designs
All trials were parallel‐group designs with the exception of one cross‐over trial (Williams 2002) for which we used only first‐cycle data. Andersen 2000 permitted those in the control group to optionally cross‐over at three months, so that if they desired, they could get MLD during the maintenance phase.
Follow‐up and sample size
Follow‐up times were presented immediately post‐treatment for all trials except one (Andersen 2000), and that trial followed up for one year. All trials assessed Phase 1 (decongestion phase), and only one (Andersen 2000) also assessed Phase 2 (maintenance phase).
Trials were small with a median of 35 total participants per trial (range 24 to 45) and a total of 208 participants. We were able to obtain individual patient data from four trials for subgroup analyses (Johansson 1998; Johansson 1999; McNeely 2004; Williams 2002). Only one trial (Andersen 2000) had more than one publication.
Excluded studies
Studies were excluded if they used a non‐manual form (i.e., electronic) of lymphatic drainage in place of MLD, if they used a different type of massage instead of MLD, if they used MLD in both groups (thereby making it impossible to distinguish the relative effect of MLD), if they altered more than the MLD component of CDT (thereby making it impossible to distinguish the relative effect of MLD), or if they addressed prevention rather than treatment of BCRL. The Characteristics of excluded studies table lists the studies we excluded as well as the reason for exclusion.
Risk of bias in included studies
Methodological quality varied among studies (Figure 2).
2.

'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Random sequence generation
We included one quasi‐randomized trial, Johansson 1999 (random sequence generation via alternate assignment, medical record number) that was judged as high risk of bias on this domain. Four trials received a low risk of bias score on randomization: Johansson 1998 (shuffled cards), McNeely 2004, Sitzia 2002 (used a computerized randomization program), and Williams 2002 (used a random number table), while one trial (Andersen 2000) received an 'unclear' risk of bias judgement because although randomization was stated, details were lacking. Because we included one quasi‐randomized trials, we paid special attention to the reported baseline demographic and medical characteristics of participants in the two groups. In all trials, the baseline information appeared comparable between the two groups.
Allocation concealment
Three trials received low risk of bias ratings for allocation concealment: Johansson 1998 used sequentially numbered opaque envelopes; McNeely 2004 clearly stated "allocation sequence was concealed from research personnel involved in screening, scheduling and enrolling participants"; and Williams 2002 called a centralized office for the next group assignment. One trial (Johansson 1999), received a high‐risk‐of‐bias score for using alternate assignment, and two trials (Andersen 2000; Sitzia 2002) received an 'unclear' rating because although randomization was stated, details of allocation concealment were lacking.
Blinding
Blinding of participants
MLD and CDT are highly physical, intensive interventions. It is impossible to blind participants to the treatment group assignment. Patient blinding would have only been possible had there been a sham MLD treatment compared with a real treatment, and no trial used that design. Therefore, none of the trials (Andersen 2000; Johansson 1998; Johansson 1999; McNeely 2004; Sitzia 2002; Williams 2002) reported patient blinding. However, inability to blind participants and the potential for performance bias, is most important in trials in which the primary outcome is a subjective self‐report (Manheimer 2011; Wood 2008). The primary outcome in these trials was volume change, which is an objective outcome measured by an outcomes assessor and is not a subjective self‐report. Measures of function, such as range of motion and strength are also objective measures assessed by an outcomes assessor. Thus, for these outcomes, we do not consider performance bias to be a major concern.
However, the lack of patient blinding could present a concern in subjective self‐reported outcomes (i.e., sensations of pain, heaviness, tension), quality of life, or other self‐reported psychosocial outcomes such as body image. Trials where there is a therapist‐administered intervention in one group, but not in the other may be especially prone to biasing subjective outcomes because the therapist's touch, time, and attention can provide powerful nonspecific effects.
Blinding of outcomes assessor
Both limb volume and functional outcomes of range of motion and strength are objective outcomes assessed by a person other than the patient. Therefore, it is important that the assessor be blinded to the treatment group assignment. Four trials (Johansson 1998; Johansson 1999; Sitzia 2002; Williams 2002) did not blind the outcomes assessor and were therefore judged as having a high‐risk of bias; one trial (McNeely 2004) clearly blinded the outcomes assessor, and one trial (Andersen 2000) was unclear from the publication, and the author could not be contacted.
Incomplete outcome data
The number of dropouts and withdrawals was low. Generally, reasons were described for dropouts that were unrelated to the treatment. When it was treatment‐related, it was due to the irritation of compression therapy. No attrition was mentioned related to MLD. Therefore, attrition bias (either from large dropout rates or differential dropouts) is not believed to be a major concern and all included studies (Andersen 2000; Johansson 1998; Johansson 1999; McNeely 2004; Sitzia 2002; Williams 2002 ) were judged as having a low risk of bias for this domain.
Selective reporting
Selective outcomes reporting also was not likely to be a problem in this set of studies as most studies reported outcomes regardless of whether they were statistically significant or not, and all trials presented data on the main outcome of volumetric change. However, one trial (Andersen 2000) was assessed as unclear risk of bias because one outcome measure (the European Organisation for Research and Treatment of Cancer (EORTC)) was mentioned as having been measured, but results were not reported. The discrepancy between assessment and reporting, therefore, was the reason for this score.
Other potential sources of bias
We also considered adherence and treatment adequacy as potential sources of bias.
Adherence
Adherence with therapist‐administered treatments was high in five trials based on publication and/or confirmation from the authors (Johansson 1998; Johansson 1999; McNeely 2004; Sitzia 2002; Williams 2002) and unclear in one trial (Andersen 2000) based on insufficient reporting.
Home‐care regimens were part of two trials (Andersen 2000; Williams 2002). Home‐care regimens were self‐massage (Williams 2002) or lymph‐reducing exercises (Andersen 2000). These trials mentioned that participants kept diaries, and Williams 2002 provided adherence data that showed adherence to be high, and thus was rated a low risk of bias. Andersen 2000 reported that exercise adherence diaries were kept, but did not report diary results, and thus, was rated 'unclear.'
Only Andersen 2000 provided long‐term follow‐up results (i.e., Phase 2/maintenance phase) and noted that in this phase, adherence with compression sleeve was high and thus was rated low risk of bias.
MLD treatment adequacy
The lymphedema reviewers rated all MLD treatments as adequate; however, one reviewer mentioned concern that standard elastic compression sleeves in Phase 1 might not provide adequate volume reductions (Johansson 1998; Williams 2002). Another reviewer raised a concern about the pressure of the lymphatic pump in a control group (Johansson 1998).
Effects of interventions
MLD + standard physiotherapy versus standard physiotherapy
One trial, Andersen 2000, reported on this comparison. "Standard physiotherapy" in this trial had all four of the components of CDT; however, because compression bandages (considered an integral part of CDT) were not used, but rather other compression garments used instead, the intervention was not termed 'CDT'.
Primary outcomes
(1) Volumetric changes in arm, hand, breast or trunk
(a) lymphedema (LE) volume
No trials reported on this outcome.
(b) volume reduction
No trials reported on this outcome.
(c) per cent reduction
Andersen 2000 reported there were no significant between‐groups differences at the end of phase I (P = 0.66), so the authors combined the data from both groups and reported an overall statistically significant 43% reduction from baseline (P ≤ 0.001).
Phase II (maintenance phase): This was the only trial to present maintenance phase follow‐up results: At three‐month follow‐up, there was no statistically significant between‐groups difference: 60% (95% confidence interval (CI): 43% to 78%) reduction in standard physiotherapy group; 48% (95% CI: 32% to 65%) in standard physiotherapy plus MLD. At 12‐month follow‐up, data were combined for both groups and showed an overall 66% reduction from baseline (P ≤ 0.001).The authors note, "The results of treatment depend on compliance of the participants, assessed by their use of the compression garment."
(2) Adverse events
There were two dropouts, and neither dropped out due to an adverse event from MLD. One had a recurrence and one was less than four months post‐treatment. No infections were reported for either group.
Secondary outcomes
(1) Functional measures
Range of motion was assessed by Andersen 2000 as flexion/extension and abduction/adduction and the authors reported there were no between‐groups differences, but significant within‐groups improvements in both groups. Data in numeric form were not presented in the paper.
(2) Subjective sensations
Andersen 2000 found no between‐groups differences, but significant within‐groups improvements for both groups for subjective sensations of pain and heaviness. Data in numeric form were not presented in the paper.
(3) Quality of life and other psychosocial outcomes
Andersen 2000 reported measuring quality of life using the EORTC (European Organization for Research and Treatment of Cancer) but did not report the results.
(4) Cost of care
Cost of care was not reported.
(5) Any other outcome reported by the trial
Subjective outcomes: Andersen 2000 found no between‐groups differences, but significant within‐groups improvements for both groups for other subjective outcomes of aching and discomfort.
MLD + compression bandaging versus compression bandaging
Two trials reported on this comparison: Johansson 1999 and McNeely 2004.
Primary outcomes
(1) Volumetric changes in arm, hand, breast or trunk
(a) lymphedema (LE) volume
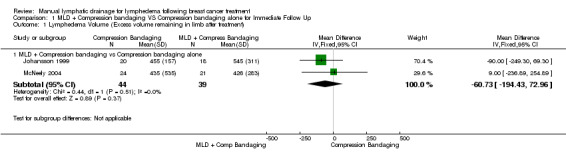
At immediate post‐treatment follow‐up, there were no significant between‐groups differences in lymphedema volume in mL either for individual or two pooled trials (mean difference (MD) ‐60.73 mL, 95% CI ‐194.43 mL to 72.96 mL; P = 0.37; 2 trials; 83 participants). See Figure 3 (Analysis 1.1).
3.

Forest plot of comparison: 1 MLD + Compression bandaging VS Compression bandaging alone for Immediate Follow Up, outcome: 1.1 Lymphedema Volume (Excess volume remaining in limb after treatment).
1.1. Analysis.
Comparison 1 MLD + Compression bandaging VS Compression bandaging alone for Immediate Follow Up, Outcome 1 Lymphedema Volume (Excess volume remaining in limb after treatment).
(b) volume reduction
At immediate post‐treatment follow‐up, two pooled trials showed borderline significance favoring MLD (MD 26.21 mL, 95% CI ‐1.04 mL to 53.45 mL; P = 0.06; 2 trials; 83 participants). See Figure 4 (Analysis 1.2).
4.

Forest plot of comparison: 1 MLD + Compression bandaging VS Compression bandaging alone for Immediate Follow Up, outcome: 1.2 Volume reduction in mL.
1.2. Analysis.

Comparison 1 MLD + Compression bandaging VS Compression bandaging alone for Immediate Follow Up, Outcome 2 Volume reduction in mL.
(c) per cent reduction
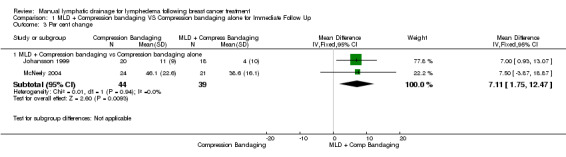
At immediate post‐treatment follow‐up, two pooled trials showed a 7.11% additional per cent reduction for the MLD group than the compression bandaging group (MD 7.11%, 95% CI 1.75% to 12.47%; P = 0.009; 2 trials; 83 participants). See Figure 5 (Analysis 1.3).
5.

Forest plot of comparison: 1 MLD + Compression bandaging VS Compression bandaging alone for Immediate Follow Up, outcome: 1.3 Per cent change.
1.3. Analysis.
Comparison 1 MLD + Compression bandaging VS Compression bandaging alone for Immediate Follow Up, Outcome 3 Per cent change.
(2) Adverse events
Adverse events were reported in only one trial (McNeely 2004). Adverse events for two participants were their reason for dropping out. One patient had a skin reaction to bandaging, and another patient had elbow discomfort from bandaging. No adverse events were reported from MLD. No infections were reported. Contact with the trial authors (Johansson 1999; McNeely 2004) stated that infections were not a problem in the trial in either group.
Secondary outcomes
(1) Functional measures
Neither trial assessed range of motion or strength.
(2) Subjective sensations
Only one trial, Johansson 1999, assessed the following subjective symptoms and reported the following results in the paper.
Pain: significant within‐groups reductions were noted for both groups, but no between‐groups differences were found (Johansson 1999).
Heaviness: significant within‐groups reductions were noted for both groups, but no between‐groups differences were found (Johansson 1999).
Tension: significant within‐groups reductions were noted for both groups, but no between‐groups differences were found (Johansson 1999).
(3) Quality of life and other psychosocial outcomes
Neither trial reported on this outcome.
(4) Cost of care
Neither trial examined cost of care.
(5) Any other outcome reported by the trial
No other outcomes were reported.
MLD + compression therapy versus non MLD treatment + compression therapy
Three trials fit this comparison category (Johansson 1998; Sitzia 2002; Williams 2002). One trial (Johansson 1998) measured volumetric change using water displacement, and two trials (Sitzia 2002; Williams 2002) used circumferential measurement. In all three trials, follow‐up times were immediate post‐treatment only. These trials used different active control groups; thus, the means and confidence intervals are provided in forest plots for individual trials separately according to comparison groups, and results were not pooled (Figure 6; Figure 7; Figure 8).
6.
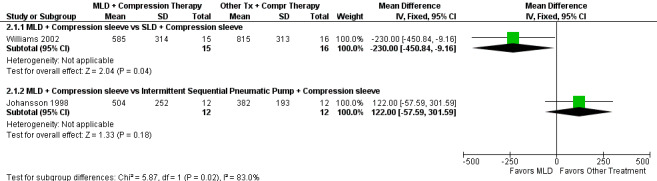
Forest plot of comparison: 2 MLD + Compression therapy vs Other treatment + Compression therapy, outcome: 2.1 Lymphedema volume (excess volume remaining in limb after treatment).
7.

Forest plot of comparison: 2 MLD + Compression therapy vs Other treatment + Compression therapy, outcome: 2.2 Volume reduction in mL.
8.
Forest plot of comparison: 2 MLD + Compression therapy vs Other treatment + Compression therapy, outcome: 2.3 Per cent change.
Primary outcomes
(1) Volumetric changes in arm, hand, breast or trunk
(a) lymphedema (LE) volume
Two trials measured LE volume (Johansson 1998; Williams 2002). In Williams 2002, MLD plus compression sleeve significantly reduced LE volume compared to simple lymphatic drainage plus compression sleeve (MD ‐230.00 mL, 95% CI ‐450.84 mL to ‐9.16 mL; P = 0.04; one trial; 31 participants). In Johansson 1998, there was no difference when comparing MLD plus compression sleeve versus intermittent pneumatic pump plus compression sleeve (MD 122.00 mL, 95% CI ‐57.59 mL to 301.59 mL; P = 0.18; one trial; 24 participants). One trial measured trunk LE (Williams 2002), but between‐groups differences were not reported. It was only reported that the MLD group had statistically significantly greater within‐groups reduction in trunk LE than did the control group of simple lymphatic drainage done by the patient. See Figure 6 (Analysis 2.1).
2.1. Analysis.

Comparison 2 MLD + Compression therapy vs Other treatment + Compression therapy, Outcome 1 Lymphedema volume (excess volume remaining in limb after treatment).
(b) volume reduction
Of the two trials with data that could be analyzed for this outcome (Johansson 1998; Williams 2002), MLD plus compression sleeve versus intermittent pneumatic pump plus compression sleeve Johansson 1998 showed a statistically significant benefit favoring the MLD intervention (MD 47.00 mL, 95% CI 15.25 mL to 78.75 mL; one trial; 24 participants) (Johansson 1998). The results for Williams 2002 were not significant (MD 10.00 mL, 95% CI ‐90.54 mL to 110.54 mL; P = 0.85; one trial; 31 participants). See Figure 7 (Analysis 2.2).
2.2. Analysis.

Comparison 2 MLD + Compression therapy vs Other treatment + Compression therapy, Outcome 2 Volume reduction in mL.
(c) per cent reduction
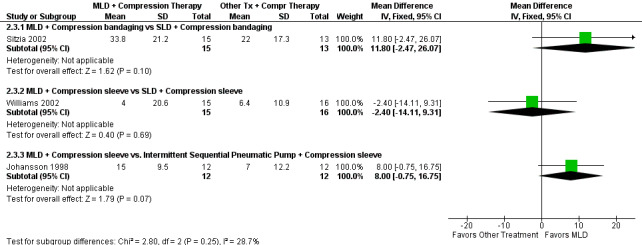
Of the three trials that reported on this outcome (Johansson 1998; Sitzia 2002; Williams 2002), there were no significant between‐groups differences for per cent reduction for any trial. Although in one trial, Johansson 1998, MLD compared with intermittent sequential pneumatic pump approached significance at P = 0.07 favoring MLD. The designs and results were as follows: Johansson 1998: MLD plus compression sleeve versus intermittent pneumatic pump plus compression sleeve (MD 8.00%, 95% CI ‐0.75% to 16.75%; P = 0.08; one trial; 24 participants); Sitzia 2002: MLD plus compression bandaging versus simple lymphatic drainage by therapist plus compression bandaging (MD 11.80%, 95% CI ‐2.47% to 26.07%; P = 0.10; one trial; 28 participants); Williams 2002: MLD plus compression sleeve versus simple lymphatic drainage by patient plus compression sleeve (MD ‐2.40%, 95% CI ‐14.11% to 9.31%; P = 0.69; one trial; 31 participants). See Figure 8 (Analysis 2.3).
2.3. Analysis.
Comparison 2 MLD + Compression therapy vs Other treatment + Compression therapy, Outcome 3 Per cent change.
(2) Adverse events
No trial reported adverse events. Infections were not reported in any trial, and contact with authors (Johansson 1998; Sitzia 2002; Williams 2002) stated infections were not a problem in either group, and there were no adverse events from MLD.
Secondary outcomes
(1) Functional measures
Range of motion: range of motion was measured in one trial (Johansson 1998) giving baseline compression sleeve to both groups and then adding MLD versus sequential pneumatic compression (SPC) pump. Five mobility measurements were taken: elbow flexion, shoulder flexion, shoulder abduction, shoulder inward and outward rotation. All five measures of the affected arm compared to the unaffected arm were statistically significantly diminished at baseline, but authors note, "Treatment with MLD or SPC did not change arm mobility." Numeric data were not provided in the paper.
Strength: strength was measured as four assessments: isometric muscle strength for shoulder flexion, abduction, adduction, and hand gripping force (Johansson 1998) and showed no between‐groups differences. Numeric data were not provided in the paper.
(2) Subjective sensations
Pain: there were no between‐groups differences on pain; however, Johansson 1998 noted that only a few people reported having pain. Williams 2002, reporting only within‐groups findings, stated that the MLD group was more likely than the self‐administered simple lymphatic drainage group to improve pain scores. Numeric data were not provided in the paper.
Heaviness: during the initial two weeks of therapy when both groups were given a baseline compression sleeve, Johansson 1998 reported a statistically significant improvement in heaviness compared to baseline. During the third week, when MLD was given to one group and SPC to the other, the authors state, "only the MLD group showed a further decrease of heaviness P = 0.008." However, there were no significant differences between the two groups. Williams 2002, reporting only within groups, stated that the MLD group was more likely than the self‐administered SLD group to improve heaviness scores. Numeric data were not provided in the papers.
Tension: during the initial two weeks of therapy when both groups were given a baseline compression sleeve, Johansson 1998 reported there was a statistically significant improvement in tension compared to baseline. During the third week, when MLD was given to one group and SPC to the other, the authors stated within groups results: "only the MLD group showed a further decrease of tension P=0.01." However, there were no between‐groups differences. Numeric data were not provided in the paper.
Discomfort and Fullness: within‐groups differences but not between‐groups differences were reported in Williams 2002. They reported that the MLD group was significantly more likely than the control group of self‐administered SLD to improve scores on discomfort and fullness.
(3) Quality of life and other psychosocial outcomes
One trial (Williams 2002) assessed quality of life using the EORTC QLQ‐C30 quality of life questionnaire and presented data only as within groups stating that the MLD group had improvement in emotional function on scales of worry, irritability, tension and depression. MLD also showed within‐groups improvement on dyspnea and reduced sleep disturbance. They further noted there were not corresponding within‐groups improvements for these measures in the simple lymphatic drainage group.
(4) Cost of care
No trial examined cost of care.
(5) Any other outcome reported by the trial
Dermal thickness: dermal thickness was measured using ultrasound in one trial (Williams 2002). The MLD group had significantly greater within‐groups reduction in dermal thickness than did the control group. Between‐groups differences were not reported.
Subgroup analyses
We obtained individual patient data for the two trials with designs MLD + compression bandaging versus compression bandaging alone (trial design: MLD + x versus x alone) (Johansson 1999; McNeely 2004).
When we applied McNeely's severity classifications (mild BCRL was defined as 15% or less excess volume), there was a statistically significant response favoring the addition of MLD to bandaging (P = 0.005) versus bandaging alone (MD 27.37%, 95 CI 8.23% to 48.51; 20 participants). Statistical significance was not noted in the moderate/severe group.
When we applied the more conservative estimate of mild BCRL (less than 20% excess volume at baseline), we similarly found an effect favoring MLD over compression bandaging alone (P = 0.02), (MD 16.40%, 95% CI 2.17% to 30.62%; 28 participants) that was not noted in the compared to moderate/severe LE.
When we explored a cut point of percentage excess volume at baseline for a group who may benefit from MLD, we found a statistically significant benefit favoring MLD for those with mild‐to‐moderate BCRL (less than 23% excess volume) (MD 12.09% 95% CI 0.15% to 24.04%; 36 participants) (P = 0.05), but not for moderate‐to‐severe BCRL. Higher cut points were not significant.
When we analyzed BCRL of shorter duration (less than 12 months) compared to longer duration (12 or more months), we did not find statistical significance favoring MLD (P = 0.10) in the shorter duration group, nor were the results significant at six or 18 months. At 24 months and through 110 months' duration, results favored MLD at each time point compared to compression bandaging alone.
We also obtained the data for two trials with designs MLD + compression sleeve versus nonMLD treatment + compression sleeve (trial design: MLD + x versus nonMLD + x) (Johansson 1998; Williams 2002). Using the same methods as above, we found no significant trends for either severity or duration.
Discussion
Summary of main results
We have reviewed the results of six clinical trials assessing the relative contribution of manual lymphatic drainage (MLD) in treating breast cancer‐related lymphedema (BCRL). Several outcomes have been examined including the objective outcomes of lymphedema (LE) volumetric changes and range of motion as well as the subjective outcomes of pain, tension, heaviness, and quality of life. All trials added some type of compression therapy to MLD; no trial assessed MLD as a stand‐alone therapy.
Volumetric changes in lymphedema of the arm, hand, breast or trunk
One trial (Andersen 2000) examined per cent reduction by using standard physiotherapy with/without MLD and found no between‐groups differences, and an overall reduction of 43% from baseline in the two groups combined. Two trials examined per cent reduction in lymphedema by using MLD and compression bandaging (Johansson 1999; McNeely 2004). The addition of MLD to bandaging provided a 7.11 % additional per cent reduction compared to the control group. The additional volume reduction is surprisingly similar between the two trials given their different designs: McNeely 2004 gave MLD in the first week and prior to each session of compression bandaging, whereas Johansson 1999 gave two weeks of compression bandaging alone to both groups before giving MLD plus compression bandaging to the treatment group in the third week. One might assume that because volume reductions are the greatest in the first week (Leduc 1998), the trial giving MLD in the third week would show a smaller contribution of MLD. Indeed, the trial giving MLD in the third week (Johansson 1999) showed smaller absolute reductions than the trial providing MLD throughout the intervention period of four weeks (McNeely 2004), but the relative reductions were the same.
There are three possible explanations for the similarity of relative reductions: Chance, bias, or a true finding. If the results are due to chance, then future attempts to replicate these results would most likely show a different finding. If the results are due to bias, it may be that as Oremus 2012 has suggested, lower‐quality designs in LE tend to produce larger effects. Thus, the quasi‐randomized design administering MLD in the third week, (Johansson 1999) may have overestimated effects. If the results are due to a true finding, then the 7.11% reduction in both trials may represent a portion of lymphatic fluid, albeit small, that is more conducive to being mobilized by MLD than by compression bandaging. It may also be that the limb may be more conducive to improved lymphatic drainage once the initial limb reduction has been achieved with compression therapy. The I2 = 0 showing no statistical heterogeneity between the two trials lends credence to the idea that although the trials used different designs; they are, in fact, very similar. By either design, compression bandaging achieved greater volume reductions than MLD, and support a commonly held notion that MLD should be considered within the context of compression therapy (Lasinski 2013; Leduc 1998).
The other two volumetric outcomes showed mixed results: there was no significant change in LE volume between treatment groups whereas volume reduction approached significance, favoring MLD. The lack of a significant difference of LE volume may be because the participants who had the greatest relative reductions (per cent reductions) had lower excess volumes to begin with (i.e., mild BCRL) and the group means could have been influenced by a few severe cases that obscured any detection of a mean benefit. It may also be that the absolute amounts of fluid reduction from MLD are small amounts and not reflected in LE volume, which is an estimate of absolute rather than relative reduction.
Three trials examined MLD plus compression therapy versus nonMLD treatment and compression therapy (Johansson 1998; Sitzia 2002; Williams 2002) and the three trials were too different from one another to be pooled and results varied according to the volumetric outcome used. The inconsistent results within the same trial depending on the volumetric outcome used has also been reported in a recent randomized trial (Dayes 2013) suggesting more research needs to be done to determine the most clinically meaningful volumetric measurement. The work of Ancukiewicz 2012 suggests relative rather than absolute values are more reliable. Other technologies such as bioimpedance and tissue dielectric constant also need to be explored as potentially clinically meaningful outcomes.
The trials using standard sleeves as the baseline compression therapy (Johansson 1998; Williams 2002) showed smaller per cent reductions than those using compression bandaging or a custom‐made sleeve‐and‐glove garment applied after successive standard sleeves first reduced volume.
Subgroup Analyses
A question raised by this review is whether there is a subgroup of participants for whom MLD might be more beneficial. Notably, there are limitations to subgroup analyses, for numbers are small, and multiple testing can result in Type I (false positive) errors. Thus, the subgroup analyses finding that mild‐to‐moderate BCRL (less than a 23% baseline excess volume) was associated with a significant response to MLD should not be taken as confirmatory evidence, but rather should be tested in a randomized controlled trial. Such a trial might include only participants with up to 23% excess volume and be designed to elucidate the effectiveness of the MLD component of complex decongestive therapy (CDT). The subgroup findings are consistent with prior studies showing that mild BCRL responds better to CDT in general than do moderate or severe cases (Didem 2005; Ramos 1999; Wozniewski 2001). McNeely 2004 has previously noted that mild participants appeared to show a greater relative response to MLD, and suggested a mechanism of action. In mild BCRL, the lymphatic system would be relatively intact and thus, more readily improved. Thus, MLD would be more capable of both stimulating lymphatic flow and rerouting lymphatic flow via collaterals. By contrast, the more severely edematous limbs, apparently unresponsive to MLD, may have more secondary damage to their lymphatic system and thus, only respond to compression bandaging through its influence on microvascular pressure. The tissue changes in more severe edema are characterized by more fat tissue and fibrosis, likely resulting in a poorer response to treatment with MLD.
Our finding of an apparent subgroup of responders raises important questions about how to interpret the varied results of the six trials in this review. For example, Sitzia 2002, using baseline compression bandaging, found no additional benefit of MLD. While this may be due to true equivalence of the two therapies, it may also be due to an inclusion criteria that excluded mild BCRL. A similar question could be asked for Andersen 2000, who found no between‐groups difference for per cent reduction in a design of standard care with/without MLD and included BCRL severity up to 30% excess baseline volume.
The subgroup analyses of the two trials (Johansson 1998; Williams 2002) which gave an active therapy to the control group used compression sleeves instead of compression bandaging showed no association between mild BCRL and response to MLD. The lack of a significant finding in the sleeve trials may indicate equivalence of active treatments, low power, or the possibility that standard sleeves might not sufficiently decongest lymphedemic areas or retain the volume reductions achieved by manual therapies in Phase 1.
Other outcomes
The functional outcome of range of motion showed contradictory results because of the two trials measuring range of motion; one reported improvements in both groups (Andersen 2000), and the other reported improvements in neither group (Johansson 1998). The functional outcome of strength was measured in only one trial (Johansson 1998), there were no improvements for either group.
Subjective sensations of pain, heaviness, and tightness were highly influenced by treatment in the four trials in which those outcomes were measured with all groups showing significant improvement from baseline but no between‐groups differences. More research needs to be done to tease apart whether one intervention is better than another at improving subjective symptoms of discomfort and how long these improvements can be maintained.
Quality of life (QoL) outcomes were inconclusive because, of the two trials that measured them, one did not report results, and the other reported within‐groups results only. Yet, QoL is affected in BCRL (Ahmed 2008; Chachaj 2010; Lee 2012; Maunsell 1993; Pusic 2013; Ridner 2011; Sagen 2009). Furthermore, at the time the trials were done, lymphedema‐specific QoL scales such as the ULL‐27 (Augustin 2005); FLQA‐L (Launois 2000); Lymph‐IFC (Devoogdt 2011) and LYMQOL (Keeley 2010) were either nonexistent or in their infancy. Future research should utilize lymphedema‐specific quality‐of‐life measures because QoL in BCRL is complicated and often related to lymphedema‐specific symptoms that are not well captured in more general QoL scales. Moreover, volume reductions alone may not be sufficient to improve women’s impaired psychosocial ratings (Tobin 1993), because QoL scores are often related to other comorbidities such as pain and dysfunction (Hormes 2010). The possibility that exercise may be able to address other comorbidities and, thus, improve quality of life (Schmitz 2012) provides a reason to investigate combination therapy of exercise with CDT.
Adverse events were minimal, and MLD was well tolerated. When trials reported adverse events, they were limited to one or two participants, usually from bandaging irritation and none due to MLD. Further contact with authors confirmed that adherence with receiving MLD was high (only one to three dropouts in a trial). Thus, with high adherence to MLD and no participant experiencing an adverse event from MLD, MLD appears safe and well tolerated in this population.
Overall completeness and applicability of evidence
All trials presented data on the main outcome of volumetric change. There were three volumetric change measures (per cent reduction, LE volume ‐ excess mL left in the arm at the end of the trial, and volume reduction ‐ the estimated mL reduced from pre‐ to post‐treatment). Some trials reported on all three, and some only one; however, we were able to calculate the others for the four trials from which we received the raw data, so we believe the data displaying volumetric changes are highly complete. Thus, the volumetric evidence is sufficiently complete that a physician, therapist, or patient could see the relative contribution of MLD.
Completeness of the other important outcomes was lacking. Functional measures (range of motion, strength), quality of life, and subjective sensations were assessed in less than half the trials and difficult to interpret. Kligman 2004 suggests including these measures because they help translate research into practice.
Quality of the evidence
The evidence from this review supports the common practice of combining MLD with compression bandaging for the treatment of BCRL and shows MLD is well tolerated. However, the data from this review were not sufficient to address the objectives of assessing quality of life or functional improvement. Furthermore, in some practice settings, MLD is given without compression therapy, and no trial in this review assessed MLD alone.
Methodological quality of the evidence varied among the trials with some trials being scored as "low risk of bias" on nearly all measures, and other trials being scores "unclear" or "high risk of bias" on some items. There was an insufficient number of trials within any subgroup to assess whether the effects of MLD varied with any of the 'Risk of bias' domains in the trials. However, we note that the greatest number of weak methodological scores appear for blinding where four of the six trials did not use a blinded outcomes assessor when measuring volumetric outcomes.
Potential biases in the review process
It is unlikely that an important bias was introduced in the search for trials. We have comprehensively searched across databases, searched the gray literature, corresponded with trialists, and used no language exclusions. We have used state‐of‐the‐art methods in evaluating trials and conducting data analysis. If there is any bias that has influenced the review, it may be that we have included one quasi‐randomized trial, which may have biased towards positive results. However, McNeely 2011, a systematic review using only randomized trials reached similar conclusions to ours.
Agreements and disagreements with other studies or reviews
We have observed that outcomes capturing the multiple comorbidities of BCRL and the psychosocial/quality‐of‐life aspects of BCRL were measured in less than half the trials, and these observations are consistent with Kärki 2009 who observed a lack of patient‐centered outcomes in BCRL trials.
We have noted that in trials combining compression bandaging with MLD, the compression bandaging yields greater volume reduction than does MLD. In the control groups which received only compression bandaging, limb reductions were 30% (Johansson 1999) and 38.6% (McNeely 2004). These reductions from compression bandaging alone are comparable to the 36% in a control group of compression bandaging with nonlocal remedial exercise for BCRL (Didem 2005) and estimates from a recent systematic review (McNeely 2011).
We have also noted that MLD gives mixed results: when added to compression bandaging, it yields a small relative benefit, but when compared to another active treatment with baseline compression sleeves to both groups, results sometimes show a significant difference favoring MLD, and other times, show no significant difference between MLD and another active treatment. Dayes 2013, in a randomized trial of CDT versus compression alone, noted similar inconsistency in volumetric outcomes suggesting more research needs to be done to identify the most clinically meaningful volume measure.
Most importantly, our findings reconcile the apparent conflicting findings of other reviews on the role of MLD in treating BCRL. Two reviews, McNeely 2011 using only randomized data, and Moseley 2007 using both randomized and uncontrolled data estimated there is a benefit of MLD. Their selected outcome was a composite of volumetric outcomes including percentage reduction. Our data on percentage reduction, had we pooled trials across assorted control groups, would concur with these reviews. We did not present a global pooled point estimate in our review due to differences across treatment and control groups. By contrast, Huang 2013 reports no effect of MLD. Their selected outcome was LE volume. Our data on LE volume, had we pooled trials across assorted control groups, would concur with Huang 2013 with no significant result for MLD.
Thus, the apparent contradictory findings of different reviews of MLD are explainable by the outcome selected. What explains the different findings based on different outcomes? It is perhaps that the participants who had the greatest per cent reductions had lower excess volumes to begin with. These would be those with mild BCRL or mildly moderate BCRL, the group identified in our subgroup analysis as perhaps being more likely to respond to MLD. Those with larger baseline volumes may have shown larger absolute reductions, but these may have been small in percentage points.
Authors' conclusions
Implications for practice.
Manual lymphatic drainage (MLD) is safe and well tolerated.
MLD may offer additional benefit when added to intensive compression bandaging for reducing swelling.
Subgroup analysis suggests that Individuals with mild‐to‐moderate breast cancer‐related lymphedema (BCRL) may be the ones who benefit from adding MLD to an intensive course of treatment with compression bandaging. This finding, however, needs to be confirmed by further research.
In trials where MLD and sleeve were compared to a nonMLD treatment and sleeve, volumetric outcomes were inconsistent within the same trial, and therefore, not generalizable. Trials using standard sleeves did not appear to be as effective as trials using compression bandaging or fitted garment for reducing swelling.
The impact on QoL is not known as no between‐groups results have been presented.
The results of function measured as range of motion were mixed in two trials.
For symptoms such as pain and heaviness, many participants reported feeling better from baseline regardless of which treatment they received. There were no between‐groups differences.
One‐year follow‐up suggests that once swelling was reduced, participants were able to keep their swelling down by continuing to use a custom‐made sleeve. It is also important to do regular check‐ups for volume status to make sure that the treatments are continuing to maintain limb volume over time (Johansson 2010).
All the trials included in this review used some compression intervention in addition to MLD, and no trial examined MLD alone although there is evidence from practitioner surveys that MLD is often given alone (Kärki 2009). Thus, an important question is unanswered, namely, whether MLD alone would be of benefit especially in participants with mild BCRL?
Implications for research.
(1) The relative contribution of MLD to complex decongestive therapy (CDT) should be examined. We were not able to answer the question of the relative contribution of MLD to CDT because no trial included all the CDT components. A limitation of trials designed to assess MLD in the absence of all four CDT components is that potential synergisms between components may be missed.. For example, few trials in this review incorporated lymph‐reducing exercises. Yet, Didem 2005, showed 55.7% per cent reductions in the intervention group which received all four CDT components, and only a 36% per cent reduction in the control group which had no MLD and replaced the lymph‐reducing exercises with nonlocal exercises. The control group results raise the question as to whether the notable lower per cent reductions were in part due to losing the synergistic effect of both the MLD and lymph‐reducing exercises. The question of synergism between components can be addressed in a 2 x 2 factorial design that gives compression bandaging to all groups. The MLD and lymph‐reducing exercises could be altered so that one group gets neither, one group gets both, and two groups get only one of the two. Thus, individual as well as combined effects could be explored.
(2) The clinical relevance of the various volumetric outcomes should be established. We have noted inconsistent findings across three volumetric outcomes. Within the same trial, one volumetric outcome might show statistical significance and another would not. More research needs to be done to establish which is the most clinically relevant volumetric outcome. There is also a need for the development and testing of measurement instruments that are more sensitive to early increase of fluid in the subcutaneous tissue such as Bioimpedance and Tissue Dielectric Constant that are easy to use in practice.
(3) Trials should include volumetric outcomes beyond arm volume. Only one trial in this review included truncal BCRL, and none addressed breast lymphedema (LE). However, both Williams 2010 and Lasinski 2013 suggest MLD may play an important role in areas such as chest wall or breast swelling that are not conducive to compression therapy, and this needs further investigation.
(4) Trials should include quality of life and other psychosocial outcomes. Future research needs to focus on quality of life using lymphedema‐specific quality‐of‐life scales. Other psychosocial outcomes, such as decreased body image, depression, anxiety, social withdrawal, and sexual dysfunction were not reported in any trials. These need to be included in research because patient‐centered outcomes, more than volume alone, are likely to influence clinical practice (Kligman 2004). Where these instruments are lacking, they need to be further developed and tested specifically for lymphedema.
(5) Trials need longer follow‐up times. All trials in this review ended immediately at the end of treatment with the exception of Andersen 2000. However, important clinical outcomes such as fibrotic formation and cellulitis episodes require long‐term follow‐up. For example, Dayes 2013 recently noted that participants with a lymphedema diagnosis greater than one year showed more benefit from CDT than from compression garments alone. They proposed that "longstanding lymphedema with tissue fibrosis may not be amenable to compression alone but may respond to gentle massage breaking down scarring" (Dayes 2013 2013). Similarly, Leduc 1998 proposed that MLD reduces fibrotic formation by moving protein out of the interstitial space. Other important questions can be answered with long‐term follow‐up: Does MLD affect the condition of the skin and tissues, in terms of fibrosis, scarring, and post‐radiation changes? What about long‐term effects on the lymphatics? Does MLD assist in re‐establishing lymphatic drainage in areas damaged by cancer treatments? Does it assist in building collateral vessels and so over time help control swelling?
(6) Trials should investigate functional outcomes and combine therapies that might optimize functional improvements. Of the few trials in this review that assessed function, results were contradictory. Future trials should investigate functional outcomes and combine therapies that potentially complement one another by combining those for reducing swelling with those for improving function (i.e., MLD/CDT plus aerobic and/or resistance training). Recent exercise trials of cardiovascular/strength training to improve function have shown promising results (Courneya 2012a; Courneya 2012b; Johansson 2005; McNeely 2006; McNeely 2009; McNeely 2012; NLN 2011).
The enthusiasm for exercise for BCRL can be attributed to three recent findings: First, exercise is safe and contrary to past beliefs, does not increase the incidence or flare ups of BCRL (McNeely 2010), and may actually protect against flare ups (Schmitz 2009). Secondly, a variety of exercise types has been shown to be safe for women with BCRL including water exercise (Johansson 2013), resistance training when gradually increased (Schmitz 2012), aerobic exercise plus resistance training (McKenzie 2003), and pole walking (Jönsson 2009), Thirdly, pain/tenderness may be reduced by exercise (Schmitz 2009).
Finally, functional improvements should be defined in practical terms, not just as improved strength or range or motion, but also as how well an intervention improves activities of daily living such as the ability to perform household chores, carry heavy objects, open a jar, and push a door (Levy 2012). Factorial designs can permit the assessment of individual therapies alone and in combination.
(7) Identifying potential subgroups of responders may help to individualize BCRL treatment in the future. Our subgroup analysis showed that participants with less than 23% excess volume at baseline (mild‐to‐moderate participants) may be the best responders to MLD. A randomized trial should examine this further.
Although duration of BCRL appears to be associated with response to MLD at various time points, subgroup analyses from other randomized trials show conflicting results of duration; McNeely 2004 found less than one year duration associated with treatment response, and Dayes 2013 found more than one year duration was associated with treatment response. Clearly more work needs to be done to understand the effect of duration of lymphedema on treatment response and how it may be confounded by severity.
If treatment of BCRL is to be individualized to optimize benefit and cost efficiency, it would be important to identify other subgroups, and more than one possible subgroup can be examined in the same trial. For example, are radiation‐induced stenotic/fibrotic changes less responsive to MLD than lymphatic damage from surgical scarring? Stratifying on radiation damage could examine this question.
(8) MLD alone should be examined. All the trials included in the review used some compression intervention in addition to MLD, and no trial examined MLD alone. A trial design of MLD alone should be designed especially in participants with mild‐to‐moderate BCRL. A three‐arm trial of MLD and compression therapy alone and in combination would efficiently answer the question of the relative contributions of each.
(9) Trials should focus on primary prevention. Because BCRL comes from surgery and/or radiation treatments for breast cancer, true primary prevention should focus on identifying the surgical and radiographic techniques that yield the lowest incidence of BCRL without compromising efficacy. Weight management should also be investigated as a primary prevention method.
(10) More high‐quality studies are warranted. The ''Risk of bias' tool in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) can serve as a guideline for rigorous trial design.
History
Protocol first published: Issue 1, 2002 Review first published: Issue 5, 2015
| Date | Event | Description |
|---|---|---|
| 12 January 2009 | Amended | Converted to new review format. |
Acknowledgements
We would like to express our appreciation to the Cochrane Breast Cancer Group editorial base and to Dr. John Sitzia, who provided additional information on his trial included in this review. We would also like to express appreciation to the Cochrane Complementary Medicine Field for providing funding for this review.
Appendices
Appendix 1. Medline Search Strategy
| # ▲ | Searches |
| 1 | randomised controlled trial.pt. |
| 2 | randomized controlled trial.pt. |
| 3 | controlled clinical trial.pt. |
| 4 | randomized.ti,ab. |
| 5 | randomised.ti,ab. |
| 6 | placebo.ti,ab. |
| 7 | randomly.ti,ab. |
| 8 | trial.ti,ab. |
| 9 | groups.ti,ab. |
| 10 | drug therapy.sh. |
| 11 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 |
| 12 | exp Lymphedema/ |
| 13 | lymphedema.mp. |
| 14 | lymphoedema.mp. |
| 15 | exp Edema/ and exp Arm/ |
| 16 | (arm adj2 edema).mp. |
| 17 | (arm adj2 oedema).mp. |
| 18 | upper extremity edema.mp. |
| 19 | upper extremity oedema.mp. |
| 20 | lymphedemic.mp. |
| 21 | lymphoedemic.mp. |
| 22 | 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 |
| 23 | complete decongestive therapy.mp. |
| 24 | conservative treatment.mp. |
| 25 | complete decongestive physiotherapy.mp. |
| 26 | CDP.mp. |
| 27 | manual lymphatic drainage.mp. |
| 28 | MLD.mp. |
| 29 | sequential pneumatic compression.mp. |
| 30 | complex decongestive therapy.mp. |
| 31 | decongestive lymphatic therapy.mp. |
| 32 | Foldi method.mp. |
| 33 | Vodder method.mp. |
| 34 | exp Drainage/ and exp Lymphedema/ |
| 35 | ((complete or complex) adj5 decongestive therap*).mp. |
| 36 | (complete adj5 decongestive physiotherap*).mp. |
| 37 | (decongestive adj5 lymphatic therap*).mp. |
| 38 | (manual adj2 lymphatic adj2 drain* adj5 therap*).mp. |
| 39 | (manual adj2 lymphatic adj2 drain*).mp. |
| 40 | exp Massage/ |
| 41 | massage.mp. |
| 42 | exp Compression Bandages/ |
| 43 | compression garment.mp. |
| 44 | compression hosiery.mp. |
| 45 | compression bandage*.mp. |
| 46 | compression therap*.mp. |
| 47 | 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 |
| 48 | 11 and 22 and 47 |
| 49 | Animals/ |
| 50 | Humans/ |
| 51 | 49 not 50 |
| 52 | 48 not 51 |
Appendix 2. CENTRAL Search Strategy
#1 MeSH descriptor: [Lymphedema] explode all trees
#2 lymphoedema* or lymphedema* or lymphatic oedema* or lymphatic edema* or oedema* or edema* or arm oedema or arm edema or upper extremity oedema or upper extremity edema or lymphoedemic or lymphedemic
#3 #1 and #2
#4 complete decongestive therap* or conservative treatment or complete decongestive physiotherap* or CDP or manual lymphatic drain* or MLD or sequential pneumatic compression or complex decongestive therap* or decongestive lymphatic therap* or Foldi method or Vodder method or massage or compression bandag* or compression garment* or compression hosiery or compression therap*
#5 MeSH descriptor: [Massage] explode all trees
#6 #4 or #5
#7 #3 and #6
Appendix 3. EMBASE Search Strategy
#1
random* OR factorial* OR crossover* OR cross AND over* OR placebo* OR (doubl* AND blind*) OR (singl* AND blind*) OR assign* OR allocat* OR volunteer* OR 'crossover procedure'/exp OR 'double blind procedure'/exp OR 'randomized controlled trial'/exp OR 'single blind procedure'/exp
#2
'lymphoedema'/exp OR lymphoedema
#3
'lymphedema'/exp OR lymphedema
#4
'arm edema'/exp OR 'arm edema'
#5
'arm oedema'
#6
arm NEAR/3 (oedema OR edema)
#7
'upper extremity edema'
#8
'upper extremity oedema'
#9
lymphedemic
#10
lymphoedemic
#11
#2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10
#12
'complete decongestive therapy'
#13
'conservative treatment'/exp OR 'conservative treatment'
#14
'complete decongestive physiotherapy'
#15
'cdp'/exp OR cdp
#16
'manual lymphatic drainage'
#17
mld
#18
'sequential pneumatic compression'
#19
'complex decongestive therapy'
#20
'decongestive lymphatic therapy'
#21
'foldi method'
#22
'vodder method'
#23
'lymphatic drainage'/exp OR 'lymphatic drainage'
#24
(complex OR complete) NEAR/5 'decongestive therapy'
#25
complete NEAR/5 'decongestive physiotherapy'
#26
decongestive NEAR/5 'lymphatic therapy'
#27
'manual lymphatic drainage therapy'
#28
'manual lymphatic drainage'
#29
'massage'/exp OR massage
#30
'compression bandages'/exp OR 'compression bandages'
#31
'compression garment'/exp OR 'compression garment'
#32
'compression hosiery'
#33
'compression bandage'/exp OR 'compression bandage'
#34
'compression therapy'/exp OR 'compression therapy'
#35
#12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 OR #34
#36
#1 AND #11 AND #35
#37
#36 AND [humans]/lim AND [embase]/lim
Appendix 4. WHO ICTRP Search Strategy
Basic Searches:
1. Complete decongestive therapy for lymphedema following breast cancer treatment
2. Complete decongestive therapy AND lymphoedema
3. Complete decongestive therapy AND lymphedema
Advanced Searches:
1. Title: complete decongestive therapy for lymphedema following breast cancer treatment
Recruitment Status: ALL
2. Title: complete decongestive therapy for lymphoedema following breast cancer treatment
Recruitment Status: ALL
3. Condition: lymphoedema*
Intervention: complete decongestive therapy OR conservative treatment OR complete decongestive physiotherapy OR CDP OR manual lymphatic drainage OR MLD OR sequential pneumatic compression OR complex decongestive therapy OR decongestive lymphatic therapy OR Foldi method OR Vodder method
Recruitment Status: ALL
4. Condition: lymphedema*
Intervention: complete decongestive therapy OR conservative treatment OR complete decongestive physiotherapy OR CDP OR manual lymphatic drainage OR MLD OR sequential pneumatic compression OR complex decongestive therapy OR decongestive lymphatic therapy OR Foldi method OR Vodder method
Recruitment Status:
ALL
Data and analyses
Comparison 1. MLD + Compression bandaging VS Compression bandaging alone for Immediate Follow Up.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Lymphedema Volume (Excess volume remaining in limb after treatment) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 MLD + Compression bandaging vs Compression bandaging alone | 2 | 83 | Mean Difference (IV, Fixed, 95% CI) | ‐60.73 [‐194.43, 72.96] |
| 2 Volume reduction in mL | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 MLD + Compression bandaging vs Compression bandaging alone | 2 | 83 | Mean Difference (IV, Fixed, 95% CI) | 26.21 [‐1.04, 53.45] |
| 3 Per cent change | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 3.1 MLD + Compression bandaging vs Compression bandaging alone | 2 | 83 | Mean Difference (IV, Fixed, 95% CI) | 7.11 [1.75, 12.47] |
Comparison 2. MLD + Compression therapy vs Other treatment + Compression therapy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Lymphedema volume (excess volume remaining in limb after treatment) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 MLD + Compression sleeve vs SLD + Compression sleeve | 1 | 31 | Mean Difference (IV, Fixed, 95% CI) | ‐230.0 [‐450.84, ‐9.16] |
| 1.2 MLD + Compression sleeve vs Intermittent Sequential Pneumatic Pump + Compression sleeve | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 122.0 [‐57.59, 301.59] |
| 2 Volume reduction in mL | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 MLD + Compression sleeve vs SLD + Compression sleeve | 1 | 31 | Mean Difference (IV, Fixed, 95% CI) | 10.0 [‐90.54, 110.54] |
| 2.2 MLD + Compression sleeve vs Intermittent sequential pneumatic pump + Compression sleeve | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 47.0 [15.25, 78.75] |
| 3 Per cent change | 3 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 3.1 MLD + Compression bandaging vs SLD + Compression bandaging | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | 11.80 [‐2.47, 26.07] |
| 3.2 MLD + Compression sleeve vs SLD + Compression sleeve | 1 | 31 | Mean Difference (IV, Fixed, 95% CI) | ‐2.40 [‐14.11, 9.31] |
| 3.3 MLD + Compression sleeve vs. Intermittent Sequential Pneumatic Pump + Compression sleeve | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 8.0 [‐0.75, 16.75] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Andersen 2000.
| Methods | RCT Parallel groups design; participants in control group given the option to cross over at three months N = (A/R) 42/44 TYPE OF LYMPHEDEMA: Arm LE DEFINITION FOR INCLUSION: 200 mL and/or 2 cm excess arm volume but < 30% Excess volume Note: Publication reports: "participants with severe lymphedema, defined as a difference in arm volume exceeding 30%, were not included but were offered DLT, including compression bandaging. However, if they declined to receive this more extensive treatment, they were allowed to participate in the study." PARTICIPANTS RECRUITED FROM: An outpatient lymphedema clinic in an oncology department COUNTRY: Denmark |
|
| Participants |
INCLUSION CRITERIA: Limb volume < 30% swelling (mild to moderate). One or more symptoms of LE (numbness, tightness, stiffness, pain, aching, heaviness or other kinds of discomfort). Post surgery at least 4 m. EXCLUSION CRITERIA: Evidence of recurrence. Bilateral breast cancer. LE treatment in the previous 3 m. Severe LE (arm volume > 30%). |
|
| Interventions |
INTERVENTION n = 20 MLD + custom‐made sleeve‐and‐glove garment providing 32‐40 mmHg compression (Jobst‐Elvarex, compression class 2, Beiersdorf, Sweden), education in lymphedema exercise and skin care Plus 8 Vodder sessions over 2 w about 1 h/session (ts = 8) plus education in self‐massage. CONTROL n = 22 CDT alone: Custom‐made sleeve‐and‐glove providing 32‐40 mmHg compression (Jobst‐Elvarex, compression class 2, Beiersdorf, Sweden), education in lymphedema exercises and skin care. Note: The compression therapy in both groups is reported in two stages: "For the first couple of treatment weeks, our follow‐up used decreasing sizes of Jobst compression garments to reduce the edema. Then measurements were taken for a custom‐made compression garment. In general, the garments were replaced every 2‐6 months to maintain the proper amount of compression." |
|
| Outcomes |
FOLLOW‐UP TIMES: Follow‐up:1, 3, 6, 9, 12 m from baseline, so first follow‐up was 2 w post‐tx REPORTED FINDINGS: LE volume (water displacement and circumference) Volumetry: One month: No statistically significant between‐groups difference: Both groups combined showed statistically significant 43% reduction from baseline (P =< 0.001) 3 months: No statistically significant between‐groups difference: 60% (95% CI: 43% to 78%) reduction in standard therapy group; 48% (95% CI: 32% to 65%) in standard therapy plus MLD. 12 months: both groups combined showed a 66% reduction from baseline P =< 0.001. QoL (EORTCQLQ‐C30 Cancer Questionnaire): results not reported Subjective Sensations: Shoulder mobility: "Both groups obtained a significant reduction in limb volume, a decrease in discomfort and an increased joint mobility during treatment." |
|
| Notes |
DROPOUTS AND WITHDRAWALS: 2 patients were dropped – one had a recurrence and one was less than 4 months post‐treatment. ADVERSE EVENTS: None reported, unable to determine if assessed. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | ‘Study design’ section, “The patients were randomly assigned to receive standard therapy or…” Also, the subtitle of the article is “A randomized study”. However, there are no details about the method of randomization. (According to Chapter 8 of the CH, a judgment of unclear is used for the following: “Insufficient information about the sequence generation process to permit judgement of ‘Yes’ or ‘No’… A simple statement such as ‘we randomly allocated’ or ‘using a randomized design’ is often insufficient to be confident that the allocation sequence was genuinely randomized…If there is doubt, then the adequacy of sequence generation should be considered to be unclear.”) |
| Allocation concealment (selection bias) | Unclear risk | There is not enough information to determine the adequacy of concealment. |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | No blinding of participants or personnel. Unclear, for outcome assessor: The ‘Discussion’ section (2nd paragraph) states the following: “One person (LA), an experienced and certified lymphotherapist…carried out all treatments in the present study.” However, the article does not report whether LA also did the outcomes assessments. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Adequate: Results (1st paragraph): “Forty‐four patients were randomized, but 2 patients, one in each treatment group, were subsequently found not to be eligible (one was found to have lymphedema caused by a local recurrence and one was randomized less than 4 months after surgery).” However, these 2 ineligible patients are unlikely to contribute to incomplete outcome data. Section 8.12.1 of The Cochrane Handbook has the following guidance about this: “ Some exclusions of participants may be justifiable, in which case they need not be considered as leading to missing outcome data (Fergusson 2002). For example, participants who are randomized but are subsequently found not to have been eligible for the trial may be excluded, as long as the discovery of ineligibility could not have been affected by the randomized intervention, and preferably on the basis of decisions made blinded to assignment. ” Besides these 2 ineligible patients, there was one other dropout before the 3 month cross‐over point (‘Results’ 1st paragraph): “This allowed data to be obtained on 42 patients at 1 month, on 41 patients at 3 months…” In the section ‘Statistical methods’: “The effect of treatment was analyzed by intention to treat.” Because the publication does not state how imputations were done for any missing data, it is not clear if this was truly intention‐to‐treat. However, whether or not a true intention‐to‐treat analysis was used is largely not relevant because there was only 1 dropout (other than the 2 exclusions) prior to the cross‐over at 3 months. |
| Selective reporting (reporting bias) | Unclear risk | Unclear – “The women also completed the EORTC QLQ‐C30 questionnaire for breast cancer, but these data are not reported in the present study.” Because these data were collected but not reported, this raises the question of selective reporting. |
| Adherence with Treatment Sessions and Home Program | Unclear risk | Treatment visits: Unclear (not reported) Exercises: Adequate: ‘Results’ (last paragraph): “There was no difference between groups in the compliance of the patients concerning use of compression sleeves or performance of arm exercise. The analysis showed that the effect of treatment on lymphedema was significantly related to the use of compression sleeves in both groups (P < 0.001). This effect was constant over time.” Because there were no differences between the two groups in the use of compression sleeves or exercises, this criterion was rated as ‘adequate’ (i.e., a low risk of bias) |
Johansson 1998.
| Methods | Parallel group design, quasi‐randomized N = (A/R) 24/28 Arm LE TYPE OF LYMPHEDEMA: Arm. LE DEFINITION FOR INCLUSION: >10% arm volume difference between abnormal and contralateral arm. PATIENTS RECRUITED FROM: Lymphedema Unit, University Hospital, Lund. COUNTRY: Sweden. |
|
| Participants |
INCLUSION CRITERIA: No history of LE before breast cancer surgery. EXCLUSION CRITERIA: Previous contralateral breast disease or intercurrent disease affecting the swollen arm. Difficulties in participating in the study such as dementia. Complete resolution LE after compression sleeve treatment. |
|
| Interventions |
INTERVENTION: W 1 and 2: Standard compression sleeve in daytime. W 3 and 4: MLD + compression sleeve (Vodder technique 45 m/d for 2 w) (ts = 10). CONTROL: W 1 and 2: Standard compression sleeve in daytime. W3 and 4: Pneumatic pump 2 h/d at 40‐60 mmHg. |
|
| Outcomes |
FOLLOW‐UP TIMES: Immediate after W2 and Immediate after W4. REPORTED FINDINGS: Volume outcomes: Part I Compression sleeve only – both groups had 7% reduction, or 49 ml in LE. P = 0.05. Part II – MLD group had 15% reduction, or 75 mL. P < 0.001. SPC group had 7% reduction, or 28 mL. P = 0.003 Shoulder mobility: "In test 2 [after two weeks of compression sleeve], there was reduced arm mobility compared to the unaffected contralateral arm in the total group. Treatment with MLD or SPC did not change arm mobility from test 2 to test 3." Isometric muscle strength: "Mean + SD for the total group in test 2 for shoulder flexion on the affected side was 7.5 + 1.8 kg, for abduction 7.0 + 1.7 kp, for adduction 5.8 + 1.6 kp, for gripping force 36.7 + 13.2 kp/cm2. No significant changes over time were seen for any of these in the two groups at test 3." Sensations: "During part I, a significant decrease in feeling of tension (P=0.004) and heaviness (P=0.01) in the arm was found in the total group. In Part II, only the MLD group showed a further decrease of tension (P=0.01) and heaviness (P=0.008). In a separate analysis, the data were stratified to exclude patients who had scored 100 (no discomfort) on the scales in test 2. The results revealed the significance to be greater but still only for MLD as regards to tension and heaviness. There was no significant difference between the two groups in Part II." Part II – MLD group showed additional decrease in tension ( P = 0.01) and additional decrease in heaviness (P = 0.008) |
|
| Notes |
DROPOUTS AND WITHDRAWALS: 4 participants were excluded from study completion. (1 resolved completely after W1 and 2 compression sleeve; 2 had breast cancer recurrence; 1 had erysipelas, 1 could not adhere to measurement protocol). ADVERSE EVENTS: None reported. Contact with author indicated there were no other adverse events. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | ‘Clinical population’ section states: “After written and informed consent, the patients were randomly allocated to either MLD or SPC therapy for two weeks (Part II).” Per author: Shuffling cards. |
| Allocation concealment (selection bias) | Low risk | Per author: Sequentially numbered, opaque, sealed envelopes were done ahead of enrolment and the next in sequence opened when a person enrolled. |
| Blinding (performance bias and detection bias) All outcomes | High risk | Given the design, the participants could not be blinded. Per author: Outcomes assessor was not blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Adequate: ‘Clinical population’ section: “Any patients who after Part I did not fulfil the criteria of lymphedema (21) were excluded from Part II. After written and oral consent, the patients were randomly allocated to either MLD or SPC therapy for two weeks (Part II)…Two patients in each group were dropped during Part II; two because of recurrent breast cancer, and one because of erysipelas during the period of treatment and one who was unable to participate in repeated measuring. Demographics of the remaining 24 women are shown in Table 1.” Because the number of dropouts are small, evenly balanced across groups, and unlikely to be related to treatment assignment or treatment outcome, there is low risk of bias for incomplete outcome data. |
| Selective reporting (reporting bias) | Low risk | Adequate: No evidence of selective outcome reporting, as all relevant outcomes (e.g., limb volume measurement, shoulder mobility, muscle strength, subjective assessment) are reported. Although limb volume measurement was only measured using the water displacement method, this method has high accuracy and reliability and it is unlikely that different results would be obtained by measuring the participants’ arm circumferences. |
| Adherence with Treatment Sessions and Home Program | Low risk | Per author: Attendance was not a problem. Participants attended almost all the sessions. |
Johansson 1999.
| Methods | Parallel groups design, quasi‐randomized N = (A/R) 38/40 TYPE OF LYMPHEDEMA: Arm. LE DEFINITION FOR INCLUSION: LE Def: >10% excess arm volume difference between affected and contralateral arm. PATIENTS RECRUITED FROM: Department of Surgery, University Hospital, Lund. COUNTRY: Sweden. |
|
| Participants |
INCLUSION CRITERIA: No history of LE before breast cancer surgery. Undergone axillary node dissection. EXCLUSION CRITERIA: Previous contralateral breast disease or intercurrent disease affecting the swollen arm. Difficulties in participating in the study such as dementia. Complete resolution LE after elastic compression sleeve treatment. |
|
| Interventions |
INTERVENTION: W 1 and 2: CB alone. W3: CB + MLD: Vodder technique, 45 m/d for 5 d (ts = 5). CONTROL: W1‐3: CB alone with low‐stretch compression bandaging. Bandage changed every 2nd day. |
|
| Outcomes |
FOLLOW‐UP TIME: Immediate after W2; Immediate after W3 REPORTED FINDINGS: Volumetry: At test 2 [after only compression bandaging for 2 weeks] there was a188 ml (26%) (P =< 0.001) in both groups compared to baseline At test 3 [after MLD or no MLD} There was a 20ml (4%) P =< 0.8) further reduction in the CB group There was a 47 ml (11%) (P =< 0.001) in the CB+MLD Subjective sensations: "There were no differences in mean score between the two groups in test 1 [baseline]. From test 1 to test 3, [with‐in group analysis] a decreased feeling of pain (P=0.03) heaviness and tensions (both P<0.001) was found in the CB+MLD group. Decreased pain P=.03 heaviness/tension P=<.001 both) in CB+MLD group only. In the CB group, [within‐groups analysis] the feeling of heaviness (P=0.006) and tension (P<0.001) was decreased. There were no significant differences between the two groups at test 3." |
|
| Notes |
DROPOUTS AND WITHDRAWALS: Two participants were dropped from the study. One for numbness/weakness during bandaging; one unable to participate in serial measurements ADVERSE EVENTS: None reported. Communication with author indicated there were no other adverse events. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Inadequate (high risk of bias): ‘Clinical population’ section: “After written and oral information and approval by the patients, they were allocated to either CB treatment alone (CB group) or to CB in combination with MLD (CB + MLD group). The series was determined so that the patients were consecutively numbered and the patients with even numbers were included in the CB group and those with odd numbers in the CB + MLD group.” ‘Discussion’ section: “The patients in this study were allocated consecutively (i.e., not randomly but alternatively) to the two treatment groups when they were referred to the Lymphedema Unit. The patients were referred from many different clinics and the severity or the incoming order sequence was not influenced by any referring doctor.” The randomization appeared to create roughly comparable groups: ‘Clinical population’ section: “Other characteristics of which there was no difference between the groups are presented in Table 1.” |
| Allocation concealment (selection bias) | High risk | Alternate assignment, according to Cochrane Handbook, is not adequately concealed. |
| Blinding (performance bias and detection bias) All outcomes | High risk | Participants were not able to be blinded due to different treatments Per author: Outcomes assessor was not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Adequate: ‘Clinical population’ section: “In this prospective study, 40 consecutive women [were included for Part I]…After written and oral information and approval by the patients, they were allocated to either CB treatment alone (CB) or to CB in combination with MLD (CB + MLD group)…After 2 weeks (Part I) MLD was added to the CB treatment in 17 of the patients for 5 days for another week (Part II), whereas the other 18 patients continued with CB alone…Two patients in the CB group were dropped during Part I; one because of feelings of numbness and weakness in the arm during bandaging and one who was unable to participate in serial measurements. [These two patients were assumedly not randomized, because the randomization occurred at the end of Part I.] The mean +/‐ SD (range) age of the remaining 38 women was 64 +/‐12 (37‐83) years in the CB group (n=18) and 58 +/‐12 (41‐80) years in the CB + MLD group (n=20).” The tables in the Results section indicated that there were 18 participants in CB group and 20 in CB + MLD group. Thus, there is a small discrepancy in the numbers of participants included in Part II: it is not clear from the text copied above whether there were 18 and 20 analyzed in the two groups or whether there were 18 and 17 (for CB and CB+MLD respectively). It was also not clear how many patients were randomized and the reasons for the dropouts. However, even under the worst case scenario, if all 38 patients who completed Part I (i.e., the 40 patients who started minus the 2 patients who dropped out during Part I) were randomized and 35 were included in the analysis (i.e., 18 + 17), these 3 dropouts out of 38 randomized would still be a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | Adequate: No evidence of selective outcome reporting, as the most important and expected outcomes were reported (i.e., limb volume measurement, subjective assessment). Although limb volume measurement was only measured using the water displacement method, this method has high accuracy and reliability and it is unlikely that different results would be obtained by measuring the participants’ arm circumferences. |
| Adherence with Treatment Sessions and Home Program | Low risk | Per author: Attendance was not a problem. Participants attended almost all the sessions. Exercises: NA – The study did not use an exercise intervention |
McNeely 2004.
| Methods | RCT, Parallel groups design N = (A/R) 45/50 TYPE OF LYMPHEDEMA: Arm. LE DEFINITION FOR INCLUSION: LE Def: 150 mL excess arm volume. PATIENTS RECRUITED FROM: Rehabilitation Center at the Cross Center Institute. COUNTRY: Canada. |
|
| Participants |
INCLUSION CRITERIA: Unilateral breast surgery including an axillary node dissection following BC diagnosis. No LE treatment within last 6 m. No one was excluded who was wearing a compression sleeve for maintenance. However, to control for any potential treatment effect from the sleeve, a minimum 4‐m wait period was observed. EXCLUSION CRITERIA: Metastatic or local recurrence. Undergoing radiotherapy or chemotherapy, infection in affected limb. Hypertension, heart disease, renal insufficiency, and venous thrombosis. |
|
| Interventions |
INTERVENTION: MLD + compression bandaging: MLD Vodder 45 m 5d/w for 4 w (ts = 20) bandages changed daily. CONTROL: Compression bandaging: for 4 w Short stretch bandages with gradient pressure, gauze to fingers and hand, foam1/2 cm wrapped around arm and hand. Worn continuously until next tx. Bandages changed daily. |
|
| Outcomes |
|
|
| Notes |
DROPOUTS AND WITHDRAWALS: Five participants did not complete the study. One developed a skin reaction; one withdrew due to elbow discomfort; one left for a family illness and two quit due to dissatisfaction with treatment response. ADVERSE EVENTS: See above. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Adequate: ‘Methods and Materials: Settings and Participants’ section: “A physical therapist was responsible for screening subjects for eligibility and the referring physician was contacted for approval. Subjects were randomized to one of the two treatment groups by use of a computer‐generated code.” The baseline characteristics of the patients, reported in Table 1, shows no significant difference between groups for all variables, suggesting the randomization created two comparable groups. |
| Allocation concealment (selection bias) | Low risk | Adequate: “The allocation sequence was concealed from research personnel involved in screening, scheduling and enrolling participants.” |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Adequate: “Two independent assessors (IA), blinded to the subjects’ treatment assignment, administered the outcome measurements. The independent assessors were qualified physical therapists familiar with, and trained in, the measurement procedure.” |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Adequate: ‘Results’ section (2nd paragraph): “A total of 45 subjects completed the study. Two subjects withdrew as a result of adverse events. One subject in the MLD/CB group withdrew after she developed a skin reaction to the bandaging. One subject in the CB group withdrew in the second week of treatment due to discomfort in the elbow region from the constant CB. Three other subjects in the CB group withdrew from the study: one due to illness of a family member and two as a result of dissatisfaction with treatment response. One subject in the MLD/CB group, though completing the study, was excluded from analysis for the water displacement volumetry as an error was found in the recording of the arm volume. Figure 2 presents the flow of participants through each stage of the study.” |
| Selective reporting (reporting bias) | Low risk | Adequate: No evidence of selective outcome reporting. “Both water displacement volumetry and measurement of circumference were used to assess lymphedema volume…” In addition, the last paragraph of the Discussion section explicitly states that range of motion and subjective outcomes were not assessed as part of this study. |
| Adherence with Treatment Sessions and Home Program | Low risk | Adequate: Per author: Treatment sessions were well attended. There was no home program. |
Sitzia 2002.
| Methods | RCT, Parallel groups design N = (A/R) 27/28 TYPE OF LYMPHEDEMA: Arm. LE DEFINITION FOR INCLUSION: > 20% excess arm volume. PATIENTS RECRUITED FROM: New referrals to lymphedema clinic, Worthington Hospital. COUNTRY: England. |
|
| Participants |
INCLUSION CRITERIA: Breast cancer treatment including surgery to axilla, radiotherapy to breast and axilla. No previous LE tx except support hosiery. No active disease. EXCLUSION CRITERIA: None stated. |
|
| Interventions |
INTERVENTION: MLD + CB: LeDuc standardized protocol, 90 m/d for 2 w (ts = 10) CONTROL: SLD + CB: 30 m/d for 2 w |
|
| Outcomes | Arm volume AS % reduction (circumference measured by tape measure). FOLLOW‐UP TIMES: No follow‐up post 2 week treatment. REPORTED FINDINGS: Limb volume (per cent change), circumference by tape measure. 33.8% reduction MLD ; 22% SLD |
|
| Notes |
DROPOUTS AND WITHDRAWALS: One patient refused to return for week two of treatment. ADVERSE EVENTS: None reported, unable to determine if assessed. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Adequate: ‘Consent and randomization’ section: “They would be allocated at random by a computer program to one of two treatments…Twenty‐eight women consented to inclusion in the study. Randomisation performed using a computer‐generated code, and trial data were managed by a non‐clinical researcher attached to Worthing Nursing Development Unit” |
| Allocation concealment (selection bias) | Unclear risk | Unclear: From the description above, it looks like allocation concealment may have been used (i.e., “trial data were managed by a non‐clinical researcher”), but it is not certain. The 1st paragraph of the ‘Results’ states the following: “Characteristics of the two groups are listed in Table 3. No significant difference was found for any characteristic between the two groups.” Thus, the randomization likely created two comparable groups. |
| Blinding (performance bias and detection bias) All outcomes | High risk | Inadequate: “All treatments for all patients were carried out by the same lymphoedema specialist nurse (LS), who had received MLD training…To maintain reliability, in this study all [outcome] measurements for all patients were carried out by the same lymphoedema specialist nurse (LS).” |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Adequate: ‘Results’ 2nd paragraph: “One participant in the SLD group failed to complete the full treatment course; she attended for treatment for five days, but was unwilling to return to the hospital for the remainder of the intensive treatment period. No data from this patient were included in the analyses presented below.” The analysis presented included 27 of the 28 patients randomized, so it is assumed that only this one patient was lost to follow‐up. |
| Selective reporting (reporting bias) | Low risk | Adequate: ‘Abstract’: “The sole outcome measure was percentage change in excess limb volume (PCEV) following treatment.” ‘Patients and methods: Outcome measures’: “A recent review of the accuracy of assessment methods for lymphoedematous limbs concluded that this ‘tape measure’ method of measurement is accurate and reliable when used by a single operator using a good technique (Stanton et al. 2000).” Thus, because the limb volume was the sole outcome, and also because the ‘tape measure’ method is an accurate way to assess limb volume (and would likely give the same results as the water displacement method), there is a low risk of selective outcome reporting. |
| Adherence with Treatment Sessions and Home Program | Low risk | Treatment visits: Unclear: The publication only described the adherence with the treatment course for the one loss to follow‐up (described above under ‘Incomplete outcome data’), and there is no mention of adherence of the other patients. Exercises: Unclear: ‘Discussion’ 2nd to last paragraph: “Thirdly, the behavior of study participants with regard to arm exercises was not monitored in this study; we do not know if all participants carried out the exercises as prescribed, and so can reach no conclusions regarding the contribution made by exercise to reduction in PCEV. It would be advisable to include some monitoring procedure, such as a patient self‐completed diary in any future work.” |
Williams 2002.
| Methods | RCT Cross‐over design N = (A/R) 29/31 TYPE OF LYMPHEDEMA: Arm and trunk. LE DEFINITION FOR INCLUSION: > 10% excess volume. PATIENTS RECRUITED FROM: Lymphedema clinic at a large cancer hospital. COUNTRY: United Kingdom. |
|
| Participants |
INCLUSION CRITERIA; Unilateral breast cancer‐related LE for more than 3 months, two limb volume measurements > 10% excess volume, > 1 year post cancer treatment. Clinically detectable trunk swelling. EXCLUSION CRITERIA: Using diuretics/other edema‐influencing drugs. Active cancer. |
|
| Interventions |
INTERVENTION: MLD + elastic sleeve (n = 15) MLD: Vodder sessions, standardized protocol, Vodder technique, for 3 weeks at 45 m/d for 5 d (t = 15 s), 6‐week washout, then 3 weeks of SLD. CONTROL: SLD + elastic sleeve (n = 16) for 3 weeks at 20 m/d, kept diaries of compliance. 6‐week washout, then 3 weeks of MLD. Per author: 'Fitted elastic sleeves' were standard sleeves, not custom made. |
|
| Outcomes |
FOLLOW‐UP TIMES: Immediate after W3, W9, W12. REPORTED FINDINGS: Within groups: MLD reduction of 71 mL P = 0.013; SLD reduction of 30 mL P = 0.08 Trunk volume (MLD only) .23 mm reduction P = 0.04 Deltoid Skin Thickness (MLD only) 15mm reduction P = 0.03 QoL (MLD only) 7.2 EMCT P = 0.006, dyspnea ‐4.6 P = 0.04, sleep disturbance ‐9.2 P = 0.03 |
|
| Notes |
DROPOUTS AND WITHDRAWALS: Two participants were excluded from study completion. One developed a herpes infection and the other developed a chest infection ADVERSE EFFECTS: None reported. Communication with author indicated there were no other adverse events. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Adequate: Per author: The central research office for the hospital randomized according to what I think was a random number table. |
| Allocation concealment (selection bias) | Low risk | Adequate: Per author: " I had to telephone a central research office for the hospital and they assigned according to their method. Randomization could not be altered." |
| Blinding (performance bias and detection bias) All outcomes | High risk | Inadequate: ‘Assessments and outcome measures’: The principal researcher (A.F.W.) undertook all the measurements and did not provide any of the MLD treatments… ‘Discussion’: “Although the researcher did not provide the MLD treatments or take part in the randomization process, she was aware, at each measurement point, of what treatments had been provided and, thus, may have unintentionally biased the data. Subjects were also aware of which treatment intervention they were receiving at each point during the trial.” Subjective outcomes (e.g., quality of life) were also measured in this trial, and because the patients, who were not blinded, assessed these outcomes, there was also no blinding for the subjective outcomes. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Adequate: As described in the first paragraph of the ‘Results’ section, there were only 2 dropouts out of 31 participants randomized, and both dropouts occurred after the cross‐over, so there were no dropouts for the analysis used in this review. |
| Selective reporting (reporting bias) | Low risk | Adequate: ‘Discussion’: “The study used a variety of outcome measures. The method of measuring and calculating limb volume in this study has been shown to be reliable, particularly when used in a consistent manner by the same operator (Stanton et al., 2000).” All expected outcomes were reported, including arm volume and subjective outcomes. Arm volume was measured in several ways, including the ‘tape measure’ method, which is reliable and would likely give same results as other methods of measurement. |
| Adherence with Treatment Sessions and Home Program | Low risk | Treatment visits: Per author: "The sessions were really well attended given that there were 15 in total. I think very few women were unable to attend‐ apart from the 2 who had to drop out." Exercises: NA: No reporting of an exercise intervention in this trial. However, “The SLD was taught by the researcher and therapists and performed by subjects for 20 min each day during the SLD period…Their technique was monitored weekly during the study and each participant kept a diary recording the areas covered and time taken each day for SLD.” Data set of diary data shows high adherence with SLD. |
BC = breast cancer CB = compression bandaging CDT = complex decongestive therapy CI = confidence interval DLT = decongestive lymphatic therapy LE = lymphedema MLD = manual lymphatic drainage QoL = quality of life RCT = randomized controlled trial SD = standard deviation SLD = simple lymphatic drainage (self‐massage) SPC = sequential pneumatic compression
d = day or days w = week or weeks m = month or months min = minutes ts = total sessions tx = treatment
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Badger 1999 | Evaluates compression therapy not MLD |
| Bertelli 1991 | Applies electric not manual lymph drainage |
| Box 2002a | MLD not given as an standard intervention per communication with author |
| Box 2002b | MLD not given as an standard intervention per communication with author |
| Devoodgt 2011 | Prevention trial |
| Didem 2005 | Trial altered the remedial exercises between groups not just the MLD treatment |
| Erickson 2001 | Review |
| Fiaschi 1998 | Gives MLD to both groups in order to evaluate compression therapy |
| Forchuk 2004 | MLD not the massage technique used per communication with the author |
| Gurdal 2012 | MLD given to both groups |
| Hornsby 1995 | Self‐massage not MLD used as intervention |
| Hutzschenreuter 1991 | No control group |
| Johansson 2010 | Cohort study |
| Le Vu 1997 | MLD appears not to be the physiotherapy technique used but author could not be located. |
| Morgan 1992 | No control group |
| Paskett 2008 | Review |
| Radakovic 1998 | Used elastic bandages for compression therapy instead of non elastic bandages |
| Szolnoky 2002 | MLD given to both groups |
| Szuba 2002 | MLD given to both groups |
| Torres Lacomba 2010 | Prevention trial |
| Venturini 1990 | Applies electric not manual lymph drainage |
| Zanolla 1984 | Allocation method not report and author could not be contacted |
| Zimmerman 2012 | Prevention trial |
MLD = manual lymphatic drainage
Characteristics of ongoing studies [ordered by study ID]
Martin 2011.
| Trial name or title | Manual lymphatic drainage therapy in patients with breast cancer related lymphoedema |
| Methods | Randomized, parallel group design |
| Participants | "A randomized, controlled clinical trial in 58 women with post‐mastectomy lymphoedema. The therapy will be administered daily for four weeks and the patient’s condition will be assessed one, three and six months after treatment." |
| Interventions | "The control group includes 29 patients with standard treatment (skin care, exercise and compression measures, bandages for one month and, subsequently, compression garments). The experimental group includes 29 patients with standard treatment plus Manual Lymphatic Drainage." |
| Outcomes | "The primary outcome parameter is volume reduction of the affected arm after treatment, expressed as a percentage. Secondary outcome parameters include: duration of lymphoedema reduction and improvement of the concomitant symptomatology (degree of pain, sensation of swelling and functional limitation in the affected extremity, subjective feeling of being physically less attractive and less feminine, difficulty looking at oneself naked and dissatisfaction with the corporal image)." |
| Starting date | Unknown |
| Contact information | ClinicalTrials (NCT): NCT01152099 |
| Notes |
Differences between protocol and review
In our protocol, we proposed to examine the trials pertaining to CDT and to MLD. However, since that protocol was written, another Cochrane review (Preston 2004) has examined CDT. Therefore, our focus is on MLD.
Also, when we wrote the protocol, some assessment methods such as tissue dielectric constant and bioimpedance were nonexistent or in their infancy. We have opted to include them as acceptable means of assessing LE in order to reflect the state of the art practice; however, it should be noted that even though we permitted these assessments, none of the included trials used them.
Finally, there are outcomes which appear in this review that do not appear in the protocol. Again, this is because since the time of the protocol submission, outcomes in this area have continued to evolve. We have elected to include these additional outcomes for the sake of comprehensiveness not only for this review, but so that anyone doing research in this field, could see in a thumbnail sketch using this review ALL the outcomes that had been used in prior trials. The category under secondary outcomes entitled "other" captures these outcomes that have not been prespecified in the protocol.
Contributions of authors
Draft the protocol: KJ, LB, DH, JE
Study selection: KJ, RW, DH, JE
Extract data from studies: TB, LB, DH, EM, MM, JE
Enter data into RevMan: EM, JE
Perform ratings of MLD treatments KJ, CT, MM, DK
Carry out the analysis: EM, JE
Interpret the analysis:TB, LB, DH, EM, MM, JE, KJ, AW, RW
Draft the final review: TB, LB, EM, JE, MM, KJ, CT, AW, RW
Disagreement resolution: JE
Update the review: This is the first version.
Sources of support
Internal sources
None, Other.
External sources
-
NCCAM‐NIH USA, USA.
Eric Manheimer was partially funded by grant number R24 AT001293 from the National Center for Complementary and Alternative Medicine (NCCAM) of the US National Institutes of Health. The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the NCCAM, or the US National Institutes of Health.
-
NCCAM‐NIH USA, USA.
Jeanette Ezzo was partially funded by grant R24 AT001293 from NCCAM (National Center for Complementary and Alternative Medicine) of the US National Institutes of Health.
Declarations of interest
None known.
New
References
References to studies included in this review
Andersen 2000 {published data only}
- Andersen L, Hojris I, Erlandsen M, Andersen J. Treatment of breast‐cancer‐related lymphedema with or without manual lymphatic drainage‐ a randomized study. Acta Oncologica 2000;39:399‐405. [DOI] [PubMed] [Google Scholar]
Johansson 1998 {published data only}
- Johansson K, Lie E, Ekdahl C, Lindfeldt J. A randomized study comparing manual lymph drainage with sequential pneumatic compression for the treatment of postoperative arm lymphedema. Lymphology 1998;31:56‐64. [PubMed] [Google Scholar]
Johansson 1999 {published data only}
- Johansson K, Albertsson M, Ingvar C, Ekdahl C. Effects of compression bandaging with or without manual lymph drainage treatment in patients with postoperative arm lymphedema. Lymphology 1999;32:103‐10. [PubMed] [Google Scholar]
McNeely 2004 {published data only}
- McNeely ML, Magee DJ, Lees AW, Bagnall KM, Haykowsky M, Hanson J. The addition of manual lymph drainage to compression therapy for breast cancer related lymphedema: A randomized controlled trial. Breast Cancer Research and Treatment 2004;86:95‐106. [DOI] [PubMed] [Google Scholar]
Sitzia 2002 {published data only}
- Sitzia J, Sobrido L, Harlow W. Manual lymphatic drainage compared with simple lymphatic drainage in the treatment of post‐mastectomy lymphoedema: A pilot randomised trial. Physiotherapy 2002;88(2):99‐107. [Google Scholar]
Williams 2002 {published data only}
- Williams AF, Vadgama A, Franks PJ, Mortimer PS. A randomized controlled crossover study of manual lymphatic drainage therapy in women with breast cancer‐related lymphedema. European Journal of Cancer Care 2002;11:254‐61. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Badger 1999 {published data only}
- Badger CM, Peacock JL, Mortimer PS. A randomized controlled, parallel group clinical trial comparing multilayer bandaging followed by hosiery versus hosiery alone in the treatment of patients with lymphedema. Cancer 2000;88(12):2832‐7. [PubMed] [Google Scholar]
Bertelli 1991 {published data only}
- Bertelli G, Venturini M, Forno G, Macchiavello F, Dini D. Conservative treatment of post‐mastectomy lymphedema: A controlled randomized trial. Annals of Oncology 1991;2:575‐8. [DOI] [PubMed] [Google Scholar]
Box 2002a {published data only}
- Box R, Reul‐Hirche HM, Bullock‐Saton JE, Furnival CM. Shoulder movement after breast cancer surgery: Results of a randomised controlled study of postoperative physiotherapy. Breast Cancer Research and Treatment 2002;78:35‐50. [DOI] [PubMed] [Google Scholar]
Box 2002b {published data only}
- Box RC, Reul‐Hirche HM, Bullock‐Saxton JE, Furnival CM. Physiotherapy after breast cancer surgery: Results of a randomised controlled study to minimise lymphoedema. Breast Cancer Research and Treatment 2002;78:51‐64. [DOI] [PubMed] [Google Scholar]
Devoodgt 2011 {published data only}
- Devoogdt N, Christiaens MR, Geraerts I, Truijen S, Smeets A, Leunen K, et al. Effect of manual lymph drainage in addition to guidelines and exercise therapy on arm lymphoedema related to breast cancer: randomised controlled trial. BMJ 2011;343(d5326):1‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
Didem 2005 {published data only}
- Didem K, Ufuk YS, Serdar S, Zümre A. The comparison of two different physiotherapy methods in treatment of lymphedema after breast surgery. Breast Cancer Research and Treatment 2005;93:49‐54. [DOI] [PubMed] [Google Scholar]
Erickson 2001 {published data only}
- Erickson VS, Pearson ML, Ganz PA, Adams J, Kahn KL. Arm edema in breast cancer patients. Journal of the National Cancer Institute 2001;93(2):96‐111. [DOI] [PubMed] [Google Scholar]
Fiaschi 1998 {published data only}
- Fiaschi E, Francesconi G, Fuimicelli S, Nicolini A, Camici M. Manual lymphatic drainage for chronic post‐mastectomy lymphoedema treatment. Panminerva Medicine 1998;40:48‐50. [PubMed] [Google Scholar]
Forchuk 2004 {published data only}
- Forchuk C, Baruth P, Prendergast M, Holliday R, Bareham R, Brimner S, et al. Postoperative arm massage: A support for women with lymph node dissection. Cancer Nursing 2004;27(1):25‐32. [DOI] [PubMed] [Google Scholar]
Gurdal 2012 {published data only}
- Gurdal SO, Kostanoglu A, Cavdar I, Ozbas A, Cabioglu N, Ozcinar B, et al. Comparison of intermittent pneumatic compression with manual lymphatic drainage for treatment of breast cancer‐related lymphedema. Lymphatic Research and Biology 2012;10(3):129‐35. [DOI] [PubMed] [Google Scholar]
Hornsby 1995 {published data only}
- Hornsby R. The use of compression to treat lymphedema. Professional Nurse 1995;11(2):127‐8. [PubMed] [Google Scholar]
Hutzschenreuter 1991 {published data only}
- Hutzschenreuter PO, Wittlinger H, Wittlinger G, Kurz I. Post‐mastectomy arm lymphedema: Treated by manual lymph drainage and compression bandage therapy. PMR 1991;1(6):166‐70. [Google Scholar]
Johansson 2010 {published data only}
- Johansson K, Branje E. Arm lymphoedema in a cohort of breast cancer survivors 10 years after diagnosis. Acta Oncologica 2010;49:166‐73. [DOI] [PubMed] [Google Scholar]
Le Vu 1997 {published data only}
- Vu B, Dumortimer A, Buhlaume MV, Mouriesse H, Barreau‐Pouhaer L. Efficacy of massage and mobilization of the upper limb after surgical treatment of breast cancer [Efficacite du massage et de la mobilisation du membre superieur apres traitement chirurgical du cancer du sein]. Bulletin du Cancer 1997;84(10):957‐61. [PubMed] [Google Scholar]
Morgan 1992 {published data only}
- Morgan RG, Casley‐Smith Jr, Mason MR, Casley‐Smith JR. Complex physical therapy for the lymphoedamatous arm. Journal of Hand Surgery (British Volume) 1992;17B:437‐41. [DOI] [PubMed] [Google Scholar]
Paskett 2008 {published data only}
- Paskett E. Breast cancer–related lymphedema: attention to a significant problem resulting from cancer diagnosis. Journal of Clinical Oncology 2008;26(35):5666‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Radakovic 1998 {published data only}
- Radakovic N, Popovic‐Petrovic S, Vranjes N, Petrovic T. A comparative pilot study of the treatment of arm lymphedema by manual drainage and sequential external pneumatic compression (SEPC) after mastectomy. Archives of Oncology 1998;6(4):177‐8. [Google Scholar]
Szolnoky 2002 {published data only}
- Szolnoky G, Lakatos B, Keskeny T, Dobozy A. Advantage of combined decongestive lymphatic therapy over manual lymph drainage: A pilot study. Lymphology 2002;35(Suppl 1):277‐82. [Google Scholar]
Szuba 2002 {published data only}
- Szuba A, Achalu R, Rockson SG. Decongestive lymphatic therapy for patients with breast carcinoma‐associated lymphedema. A randomized, prospective study of a role for adjunctive intermittent pneumatic compression. Cancer 2002;95(11):2260‐7. [DOI] [PubMed] [Google Scholar]
Torres Lacomba 2010 {published data only}
- Torres Lacomba M, Yuste Sánchez MJ, Zapico Goñi A, Prieto Merino D, Mayoral del Moral O, Cerezo Téllez E, et al. Effectiveness of early physiotherapy to prevent lymphoedema after surgery for breast cancer: randomised, single blinded, clinical trial. BMJ 2010;340(b5396):1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Venturini 1990 {published data only}
- Venturini M, Forno G, Bertelli G, Vidili MG, Macchiavello F, Dini D. Compression therapy in postmastectomy lymphedema (PML): Results of our phase II‐III studies and future research lines. Breast Cancer Research and Treatment 1990;16(2):188. [Google Scholar]
Zanolla 1984 {published data only}
- Zanolla R, Monzeglio C, Balzarini A, Martino G. Evaluation of the results of three different methods of postmastectomy lymphedema treatment. Journal of Surgical Oncology 1984;26:210‐13. [DOI] [PubMed] [Google Scholar]
Zimmerman 2012 {published data only}
- Zimmerman A, Wozniewski M, Szklarska A, Lipowicz A, Szuba A. Efficacy of manual lymphatic drainage in preventing secondary lymphedema after breast cancer surgery. Lymphology 2012;45:103‐12. [PubMed] [Google Scholar]
References to ongoing studies
Martin 2011 {published data only}
- Martín ML, Hernández MA, Avendaño C, Rodríguez F, Martínez H. Manual lymphatic drainage therapy in patients with breast cancer related lymphoedema. BMC Cancer 2011;11(94):1‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Ahmed 2008
- Ahmed RL, Prizment A, Lazovich D, Schmitz KH, Folsom AR. Lymphedema and quality of life in breast cancer survivors: the Iowa Women's Health Study. Journal of Clinical Oncology 2008;26(35):5689‐96. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ahmed 2011
- Ahmed RL, Schmitz KH, Prizment AE, Folsom AR. Risk factors for lymphedema in breast cancer survivors, the Iowa Women's Health Study. Breast Cancer Research and Treatment 2011;130(3):981‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ancukiewicz 2012
- Ancukiewicz M, Miller CL, Skolny MN, O'Toole J, Warren LE, Jammallo LS, et al. Comparison of relative versus absolute arm size change as criteria for quantifying breast cancer‐related lymphedema: the flaws in current studies and need for universal methodology. Breast Cancer Research and Treatment 2012;135(1):145‐52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Armer 2009
- Armer JM, Stewart BR, Shook RP. 30‐month post‐breast cancer treatment lymphoedema. Journal of Lymphoedema 2009;4(1):14‐8. [PMC free article] [PubMed] [Google Scholar]
Augustin 2005
- Augustin M, Bross F, Földi E, Vanscheidt W, Zschocke I. Development, validation and clinical use of the FLQA‐L, a disease‐specific quality of life questionnaire for patients with lymphedema. VASA. Journal of Vascular Diseases 2005;34(1):31‐5. [DOI] [PubMed] [Google Scholar]
Bernas 2001
- Bernas MJ, Witte CL, Witte MH for the International Society of Lymphedema Executive Committee. The diagnosis and treatment of peripheral lymphedema: Draft revision of the 1995 consensus document of the International Society of Lymphology executive committee for discussion at the September 3‐7, 2001, XVIII International Congress of Lymphology in Genoa, Italy. Lymphology 2001;34:84‐90. [PubMed] [Google Scholar]
Brennan 1992
- Brennan MG. Lymphedema following the surgical treatment of breast cancer; a review of pathophysiology and treatment. Journal of Pain and Symptom Management 1992;7(2):110‐6. [DOI] [PubMed] [Google Scholar]
Brennan 1996
- Brennan MG, DePompolo RW, Garden FH. Focused review: Postmastectomy lymphedema. Archives of Physical Medicine and Rehabilitation 1996;77:S74‐80. [DOI] [PubMed] [Google Scholar]
Chachaj 2010
- Chachaj A, Małyszczak K, Pyszel K, Lukas J, Tarkowski R, Pudełko M, et al. Physical and psychological impairments of women with upper limb lymphedema following breast cancer treatment. Psycho‐oncology 2010;19(3):299‐305. [DOI] [PubMed] [Google Scholar]
Clark 2005
- Clark B, Sitzia J, Harlow W. Incidence and risk of arm oedema following treatment for breast cancer: a three‐year follow‐up study. QJM 2005;98:343–8. [DOI] [PubMed] [Google Scholar]
Cochran 1954
- Cochran WG. The combination of estimates from different experiments. Biometrics 1954;10:101‐29. [Google Scholar]
Cohen 1998
- Cohen SR, Payne DK, Tunkel RS. Lymphedema: Strategies for management. Cancer (Supplement) 1998;83(12):980‐7. [DOI] [PubMed] [Google Scholar]
Courneya 2012a
- Courneya KS, Karvinen KH, McNeely ML, Campbell KL, Brar S, Woolcott CG, et al. Predictors of adherence to supervised and unsupervised exercise in the Alberta Physical Activity and Breast Cancer Prevention Trial. Journal of Physical Activity & Health 2012;9(6):857‐66. [DOI] [PubMed] [Google Scholar]
Courneya 2012b
- Courneya KS, Stevinson C, McNeely ML, Sellar CM, Friedenreich CM, Peddle‐McIntyre CJ, et al. Predictors of follow‐up exercise behavior 6 months after a randomized trial of supervised exercise training in lymphoma patients. Psychooncology 2012;21(10):1124‐31. [DOI] [PubMed] [Google Scholar]
Dayes 2013
- Dayes IS, Whelan TJ, Julian JA, Parpia S, Pritchard KI, D’Souza DP, et al. Randomized trial of decongestive lymphatic therapy for the treatment of lymphedema in women with breast cancer. Journal of Clinical Oncology 2013;31(35):1‐7. [DOI] [PubMed] [Google Scholar]
DerSimonian 1986
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7:177‐88. [DOI] [PubMed] [Google Scholar]
Devoogdt 2010
- Devoogdt N, Kampen M, Geraerts I, Coremans T, Christiaens MR. Different physical treatment modalities for lymphoedema developing after axillary lymph node dissection for breast cancer: a review. European Journal of Obstetrics and Gynecology and Reproductive Biology 2010;149(1):3‐9. [DOI] [PubMed] [Google Scholar]
Devoogdt 2011
- Devoogdt N, Kampen M, Geraerts I, Coremans T, Christiaens MR. Lymphoedema Functioning, Disability and Health questionnaire (Lymph‐ICF): reliability and validity. Physical Therapy 2011;91(6):944‐57. [DOI] [PubMed] [Google Scholar]
DiSipio 2013
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta‐analysis. Lancet Oncology 2013;14(6):500‐15. [DOI] [PubMed] [Google Scholar]
Fergusson 2002
- Fergusson D, Aaron SD, Guyatt G, Hébert P. Postrandomisation exclusions: the intention to treat principle and excluding patients from analysis. BMJ 2002;325(7365):652‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Foldi 1998
- Foldi E. The treatment of lymphedema. Cancer (Supplement) 1998;83(12):2833‐4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Geller 2003
- Geller BM, Vacek PM, O'Brien P, Secker‐Walker RH. Factors associated with arm swelling after breast cancer surgery. Journal of Women's Health 2003;12(9):921‐30. [DOI] [PubMed] [Google Scholar]
Harris 2012
- Harris SR, Schmitz KH, Campbell KL, McNeely ML. Clinical practice guidelines for breast cancer rehabilitation: syntheses of guideline recommendations and qualitative appraisals. Cancer 2012;118(8 Suppl):2312‐24. [DOI] [PubMed] [Google Scholar]
Hayes 2012
- Hayes SC, Johansson K, Stout NL, Prosnitz R, Armer JM, Gabram S, et al. Upper‐body morbidity after breast cancer: Incidence and evidence for evaluation, prevention, and management within a prospective surveillance model of care. Cancer 2012;118:2237‐49. [DOI] [PubMed] [Google Scholar]
Helyer 2010
- Helyer LK, Varnic M, Le LW, Leong W, McCready D. Obesity is a risk factor for developing postoperative lymphedema in breast cancer patients. Breast Journal 2010;16(1):48‐54. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Altman DG, on behalf of the Cochrane Statistical Methods Group and the Cochrane Bias Methods Group (Editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. The Cochrane Collaboration, 2011. [Google Scholar]
Hormes 2010
- Hormes JM, Bryan C, Lytle LA, Gross CR, Ahmed RL, Troxel AB, et al. Impact of lymphedema and arm symptoms on quality of life in breast cancer survivors. Lymphology 2010;43(1):1‐13. [PubMed] [Google Scholar]
Huang 2013
- Huang TW, Tseng SH, Lin CC, Bai CH, Chen CS, Hung CS, et al. Effects of manual lymphatic drainage on breast cancer‐related lymphedema: a systematic review and meta‐analysis of randomized controlled trials. World Journal of Surgical Oncology 2013;11(15):1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Johansson 2005
- Johansson K, Tibe K, Weibull A, Newton RC. Low intensity resistance exercise for breast cancer patients with arm lymphedema with or without compression sleeve. Lymphology 2005;38:167‐80. [PubMed] [Google Scholar]
Johansson 2013
- Johansson K, Hayes S, Speck RM, Schmitz KH. Water‐based exercise for patients with chronic arm lymphedema: a randomized controlled pilot trial. American Journal of Physical Medicine and Rehabilitation 2013;92(4):312‐9. [DOI] [PubMed] [Google Scholar]
Jönsson 2009
- Jönsson C, Johansson K. Pole walking for patients with breast cancer‐related arm lymphedema. Physiotherapy Theory and Practice 2009;25(3):165‐73. [DOI] [PubMed] [Google Scholar]
Keeley 2010
- Keeley V, Crooks S, Locke J, Veigas D, Riches K, Hilliam R. A quality of life measure for limb lymphoedema (LYMQOL). Journal of Lymphoedema 2010;5(1):1‐5. [Google Scholar]
Kligman 2004
- Kligman L, Wong R, Johnston M, Laetsch N, and members of the Supportive Care Guidelines Group. The treatment of lymphedema related to breast cancer: A systematic review and evidence summary. Supportive Care in Cancer 2004;12:421‐31. [DOI] [PubMed] [Google Scholar]
Kwan 2010
- Kwan ML, Darbinian J, Schmitz KH, Citron R, Partee P, Kutner SE, et al. Risk factors for lymphedema in a prospective breast cancer survivorship study: the Pathways Study. Archives of Surgery 2010;145(11):1055‐63. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kärki 2009
- Kärki A, Anttila H, Tasmuth T, Rautakorpi UM. Lymphoedema therapy in breast cancer patients: a systematic review on effectiveness and a survey of current practices and costs in Finland. Acta Oncologica 2009;48(6):850‐9. [DOI] [PubMed] [Google Scholar]
Lasinski 2013
- Lasinski B. Complete decongestive therapy for treatment of lymphedema. Seminars in Oncology Nursing 2013;29(1):20‐7. [DOI] [PubMed] [Google Scholar]
Launois 2000
- Launois R, Alliot F. Quality of life scale in upper limb lymphoedema – a validation study. Lymphology 2000;33:266‐74. [Google Scholar]
Lawenda 2009
- Lawenda BD, Mondry TE, Johnstone PA. Lymphedema: A primer on the identification and management of a chronic condition in oncologic treatment. CA: A Cancer Journal for Clinicians 2009;59:8‐24. [DOI] [PubMed] [Google Scholar]
Leduc 1998
- Leduc O, Leduc A, Bourgeois P, Belgrado JP. The physical treatment of upper limb edema. Cancer (Supplement) 1998;83:2835‐9. [DOI] [PubMed] [Google Scholar]
Lee 2012
- Lee SH, Min YS, Park HY, Jung TD. Health‐related quality of life in breast cancer patients with lymphedema who survived more than one year after surgery. Journal of Breast Cancer 2012;15(4):449‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Levick 2010
- Levick JR, Michel CC. Microvascular fluid exchange and the revised Starling principle. Cardiovascular Research 2010;87(2):198‐210. [DOI] [PubMed] [Google Scholar]
Levy 2012
- Levy EW, Pfalzer LA, Danoff J, Springer BA, McGarvey C, Shieh CY, et al. Predictors of functional shoulder recovery at 1 and 12 months after breast cancer surgery. Breast Cancer Research and Treatment 2012;134(1):315‐24. [DOI] [PubMed] [Google Scholar]
Manheimer 2011
- Manheimer E. Selecting a control for in vitro fertilization and acupuncture randomized controlled trials (RCTs): how sham controls may unnecessarily complicate the RCT evidence base. Fertility & Sterility 2011;95(8):2456‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mantel 1959
- Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. Journal of the National Cancer Institute 1959;22(4):719‐48. [PubMed] [Google Scholar]
Maunsell 1993
- Maunsell E, Brisson J, Deschenes L. Arm problems and psychological distress after surgery for breast cancer. Canadian Journal of Surgery 1993;36:315‐20. [PubMed] [Google Scholar]
McKenzie 2003
- McKenzie DC, Kalda AL. Effect of upper extremity exercise on secondary lymphedema in breast cancer patients: a pilot study. Journal of Clinical Oncology 2003;21(3):463‐6. [DOI] [PubMed] [Google Scholar]
McNeely 2006
- McNeely ML, Campbell KL, Rowe BH, Klassen TP, Mackey JR, Courneya KS. Effects of exercise on breast cancer patients and survivors: a systematic review and meta‐analysis. CMAJ: Canadian Medical Association Journal 2006;175(1):34‐41. [DOI] [PMC free article] [PubMed] [Google Scholar]
McNeely 2009
- McNeely ML, Campbell KL, Courneya KS, Mackey JR. Effect of acute exercise on upper‐limb volume in breast cancer survivors: a pilot study. Physiotherapy Canada 2009;61(4):244‐51. [DOI] [PMC free article] [PubMed] [Google Scholar]
McNeely 2010
- McNeely ML. Early physiotherapy after surgery for breast cancer can reduce the incidence of lymphoedema in the following 12 months. Journal of Physiotherapy 2010;56(2):134. [DOI] [PubMed] [Google Scholar]
McNeely 2011
- McNeely ML, Peddle CJ, Yurick JL, Dayes IS, Mackey JR. Conservative and dietary interventions for cancer‐related lymphedema: a systematic review and meta‐analysis. Cancer 2011;117(6):1136‐48. [DOI] [PubMed] [Google Scholar]
McNeely 2012
- McNeely ML, Parliament MB, Seikaly H, Jha N, Magee DJ, Haykowsky MJ, et al. Predictors of adherence to an exercise program for shoulder pain and dysfunction in head and neck cancer survivor. Support Care in Cancer 2012;20(3):515‐22. [DOI] [PubMed] [Google Scholar]
Megans 1998
- Megans A, Harris S. Physical therapist management of lymphedema following treatment for breast cancer: a critical review of it effectiveness. Physical Therapist 1998;78(12):1302‐11. [DOI] [PubMed] [Google Scholar]
Miaskowski 2013
- Miaskowski C, Dodd M, Paul SM, West C, Hamolsky D, Abrams G, et al. Lymphatic and angiogenic candidate genes predict the development of secondary lymphedema following breast cancer surgery. PLoS One 2013;8(4):e60164. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mirolo 1995
- Mirolo BR, Bunce IH, Chapman M, Olsen T, Eliadis P, Hennessy JM, et al. Psychosocial benefits of postmastectomy lymphedema therapy. Cancer Nursing 1995;18(3):197‐205. [PubMed] [Google Scholar]
Mislin 1961
- Mislin H. Experimental detection of autochthonous automatism of lymph vessels [Experimenteller Nachweis der autochthonen Automatie der Lymphgefässe]. Experientia 1961;17(1):29‐30. [DOI] [PubMed] [Google Scholar]
Moseley 2007
- Moseley AL, Carati CJ, Piller NB. A systematic review of common conservative therapies for arm lymphoedema secondary to breast cancer treatment. Annals of Oncology 2007;18(4):639‐46. [DOI] [PubMed] [Google Scholar]
NLN 2011
- NLN Medical Advisory Committee. National Lymphedema Network Position Statement on Exercise. National Lymphedema Network 2011; Vol. May:1‐5.
Oremus 2012
- Oremus M, Dayes I, Walker K, Raina P. Systematic review: conservative treatments for secondary lymphedema. BioMed Central Cancer 2012;12(6):1‐15. [DOI] [PMC free article] [PubMed] [Google Scholar]
Park 2008
- Park JH, Lee WH, Chung HS. Incidence and risk factors of breast cancer lymphoedema. Journal of Clinical Nursing 2008;17(11):1450‐9. [DOI] [PubMed] [Google Scholar]
Partsch 2010
- Partsch H, Stout N, Forner‐Cordero I, Flour M, Moffatt C, Szuba A, et al. Clinical trials needed to evaluate compression therapy in breast cancer related lymphedema (BCRL). Proposals from an expert group. International Angiology 2010;29(5):442‐53. [PubMed] [Google Scholar]
Paskett 2007
- Paskett ED, Naughton MJ, McCoy TP, Case LD, Abbott JM. The epidemiology of arm and hand swelling in premenopausal breast cancer survivors. Cancer Epidemiology, Biomarkers, and Prevention 2007;16:775‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
Paskett 2012
- Paskett ED, Dean JA, Oliveri JM, Harrop JP. Cancer‐related lymphedema risk factors, diagnosis, treatment, and impact: a review. Journal of Clinical Oncology 2012;30(30):3726‐33. [DOI] [PubMed] [Google Scholar]
Passik 1998
- Passik SD, McDonald MV. Psychosocial aspects of upper extremity lymphedema in women treated for breast carcinoma. Cancer (Supplement) 1998;83(12):2817‐20. [DOI] [PubMed] [Google Scholar]
Petrek 1998
- Petrek JA, Heelan MC. Incidence of breast carcinoma‐related lymphedema. Cancer (Supplement) 1998;83(12):2776‐81. [DOI] [PubMed] [Google Scholar]
Preston 2004
- Preston N, Seers K, Mortimer P. Physical therapies for reducing and controlling lymphoedema of the limbs. Cochrane Database of Systematic Reviews 2004, Issue July. [DOI: 10.1002/14651858.CD003141.pub2] [DOI] [PubMed] [Google Scholar]
Pusic 2013
- Pusic AL, Cemal Y, Albornoz C, Klassen A, Cano S, Sulimanoff I, et al. Quality of life among breast cancer patients with lymphedema: a systematic review of patient‐reported outcome instruments and outcomes. Journal of Cancer Survivorship: Research and Practice 2013;7(1):83‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ramos 1999
- Ramos SM, O'Donnell LS, Knight G. Edema volume, not timing, is the key to success in lymphedema treatment. American Journal of Surgery 1999;178(4):311‐5. [DOI] [PubMed] [Google Scholar]
RevMan [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Ridner 2010a
- Ridner SH, Deng J, Fu MR, Radina E, Thiadens SR, Weiss J, et al. Symptom burden and infection occurrence among individuals with extremity lymphedema. Lymphology 2012;45(3):113‐23. [PubMed] [Google Scholar]
Ridner 2010b
- Ridner SH, Murphy B, Deng J, Kidd N, Galford E, Dietrich MS. Advanced pneumatic therapy in self‐care of chronic lymphedema of the trunk. Lymphatic Research & Biology 2010;8(4):209‐15. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ridner 2011
- Ridner SH, Dietrich MS, Kidd N. Breast cancer treatment‐related lymphedema self‐care: education, practices, symptoms, and quality of life. Support Care Cancer 2011;19(5):631‐7. [DOI] [PubMed] [Google Scholar]
Ridner 2012
- Ridner SH, Fu MR, Wanchai A, Stewart BR, Armer JM, Cormier JN. Self‐management of lymphedema: a systematic review of the literature from 2004 to 2011. Nursing Research 2012;61(4):291‐9. [DOI] [PubMed] [Google Scholar]
Ridner 2013
- Ridner S. Pathophysiology of lymphedema. Seminars in Oncology Nursing 2013;29(1):4‐11. [DOI] [PubMed] [Google Scholar]
Rockson 1998
- Rockson SG. Precipitating factors in lymphedema: Myths and realities. Cancer (Supplement) 1998;83(12):2814‐6. [DOI] [PubMed] [Google Scholar]
Sagen 2009
- Sagen A, Kåresen R, Sandvik L, Risberg MA. Changes in arm morbidities and health‐related quality of life after breast cancer surgery – a five‐year follow‐up study. Acta Oncologica 2009;48(8):1111‐8. [DOI] [PubMed] [Google Scholar]
Schmitz 2009
- Schmitz KH, Ahmed RL, Troxel A, Cheville A, Smith R, Lewis‐Grant L, et al. Weight lifting in women with breast‐cancer‐related lymphedema. New England Journal of Medicine 2009;361(7):664‐73. [DOI] [PubMed] [Google Scholar]
Schmitz 2012
- Schmitz KH, Stout NL, Andrews K, Binkley JM, Smith RA. Prospective evaluation of physical rehabilitation needs in breast cancer survivors: a call to action. Cancer 2012;118(8):2187‐90. [DOI] [PubMed] [Google Scholar]
Shah 2012
- Shah C, Arthur D, Riutta J, Whitworth P, Vicini FA. Breast‐cancer related lymphedema: A review of procedure‐specific incidence rates, clinical assessment aids, treatment paradigms, and risk reduction. Breast Journal 2012;18(4):357‐61. [DOI] [PubMed] [Google Scholar]
Shih 2009
- Shih YC, Xu Y, Cormier JN, Giordano S, Ridner SH, Buchholz TA, et al. Incidence, treatment costs, and complications of lymphedema after breast cancer among women of working age: a 2‐year follow‐up study. Journal of Clinical Oncology 2009;27(12):2007‐14. [DOI] [PubMed] [Google Scholar]
Stout 2012b
- Stout NL, Pfalzer LA, Springer B, Levy E, McGarvey CL, Danoff JV, et al. Breast cancer‐related lymphedema: comparing direct costs of a prospective surveillance model and a traditional model of care. Physical Therapy 2012;92(1):142‐63. [DOI] [PMC free article] [PubMed] [Google Scholar]
Swenson 2009
- Swenson KK, Nissen MJ, Leach JW, Post‐White J. Case‐control study to evaluate predictors of lymphedema after breast cancer surgery. Oncology Nursing Forum 2009;36(2):185‐93. [DOI] [PubMed] [Google Scholar]
Tobin 1993
- Tobin M, Lacey HJ, Meyer L, Mortimer PS. The psychological morbidity of breast cancer‐related arm swelling. Cancer 1993;72:3248‐52. [DOI] [PubMed] [Google Scholar]
Williams 2010
- Williams A. Manual lymphatic drainage: Exploring the history and evidence base. British Journal of Community Nursing 2010;15(4 Suppl 1):S18‐S24. [DOI] [PubMed] [Google Scholar]
Wood 2008
- Wood L, Egger M, Gluud LL, Schulz KF, Jüni P, Altman DG, et al. Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions and outcomes: meta‐epidemiological study. BMJ 2008;336(7644):601‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wozniewski 2001
- Wozniewski M, Jasinski R, Pilch U, Dabrowska G. Complex physical therapy for lymphedema of the limbs. Physiotherapy 2001;87(5):252‐6. [Google Scholar]
Zuther 2011a
- Zuther J. Decongestive and breathing exercises for lymphedema. http://www.lymphedemablog.com/2011/01/06/decongestive‐and‐breathing‐exercises‐for‐lymphedema/ Accessed Oct 13, 2013.