

Abstract
Aim:
To estimate the prevalence of visual impairment (VI) due to uncorrected refractive error (URE) and to assess the barriers to utilization of services in the adult urban population of Delhi.
Materials and Methods:
A population-based rapid assessment of VI was conducted among people aged 40 years and above in 24 randomly selected clusters of East Delhi district. Presenting visual acuity (PVA) was assessed in each eye using Snellen's E chart. Pinhole examination was done if PVA was <20/60 in either eye and ocular examination to ascertain the cause of VI. Barriers to utilization of services for refractive error were recorded with questionnaires.
Results:
Of 2421 individuals enumerated, 2331 (96%) individuals were examined. Females were 50.7% among them. The mean age of all examined subjects was 51.32 ± 10.5 years (standard deviation). VI in either eye due to URE was present in 275 individuals (11.8%, 95% confidence interval [CI]: 10.5–13.1). URE was identified as the most common cause (53.4%) of VI. The overall prevalence of VI due to URE in the study population was 6.1% (95% CI: 5.1 CI: 5.1–7.0). The elder population as well as females were more likely to have VI due to URE (odds ratio [OR] = 12.3; P < 0.001 and OR = 1.5; P < 0.02). Lack of felt need was the most common reported barrier (31.5%).
Conclusions:
The prevalence of VI due to URE among the urban adult population of Delhi is still high despite the availability of abundant eye care facilities. The majority of reported barriers are related to human behavior and attitude toward the refractive error. Understanding these aspects will help in planning appropriate strategies to eliminate VI due to URE.
Keywords: Barriers, population-based, uncorrected refractive error, urban, visual impairment
Visual impairment (VI) due to an uncorrected refractive error (URE) is an important major public health problem throughout the world, especially in developing countries. Global estimation indicates that of the 285 million with VI, 43% (122 million) are due to UREs,[1] whereas the proportion of blind due to URE is low globally (3%), but in India it is the second highest (19.6%) cause of blindness.[2] It is a well-known fact that if refractive error (RE) is not corrected, this will lead to severe social and economic impact on individuals' livelihood irrespective of age, sex, race, and ethnicity.[2] Despite the availability of an easy and cost-effective remedy for RE, many people both from urban and rural community, especially in low- or middle-income countries, still suffer from VI due to URE.
There is paucity of literature about URE from different regions of the Indian subcontinent. Few population-based studies are available from Southern part of India. One study showed that URE accounts 16% of the blindness and 46% of the VI across all age groups in the state of Andhra Pradesh.[3,4] Rapid assessment of VI (RAVI) in the same state revealed that URE was the leading cause of VI accounting for 47.6% of all VI.[5] In contrast to South India, very limited or no study on URE in adult population is available from North India though some studies exist among children. A country like India where the population is so diverse and heterogeneous in nature, it is imperative to have scientifically valid data from North India so that appropriate public health strategies can be designed to tackle the problem. We, therefore, planned to conduct RAVI among the adult population of urban Delhi instead of conducting an exhaustive and detailed epidemiological study which is more time-consuming and resource-intensive. This paper reports part of the Delhi-RAVI study on magnitude of VI due to URE and barriers to correction of RE among the urban Delhi population aged 40 years and above.
Materials and Methods
Sample size calculation
Sample size was calculated based on an assumed prevalence of VI (<20/60 in the better eye) of 15% in the age groups of 40 years and above,[6] relative precision of 15%, 95% confidence interval (CI), design effect of 2 with cluster size of 400–500, power of 80%, and nonresponse rate of 15%. The final calculated sample size was 2370 persons.
Study area
The East district of Delhi was chosen for present study. East district is situated on the Eastern bank of river Yamuna that divides Delhi into two parts. It has three different sub-districts. As per 2011 census, it had a population of 1,707,725 (11% of Delhi population) with a population density of 26,683/km2.[7] The sex ratio of district was 883 with decadal growth rate of 16.68%. The literacy rate of district is 88.75%.[7] Most of the households in the area belongs to resettlement colonies and are of migrants from neighboring states. Health services in the area are provided by the government sector and by a large number of private practitioners.
Sampling methodology
The detailed methodology was explained in the Delhi-RAVI study.[8] However, in brief, a multistage cluster random sampling technique was used in the study. In the first stage of sampling, out of three sub-districts of East Delhi, one sub-district, Preet Vihar was selected randomly for the study. It has a population of 266,494 (male: 52.7%) with 27 administrative wards. Further, six wards were randomly selected. As per census 2011, a total of 603 census enumeration block (CEB) were registered in these six wards. These CEB were considered as “clusters” in this study which has an estimated population of 400–500 with nearly 100–125 individuals aged 40 years and above. To meet the required sample size, 24 of 603 CEBs, i.e., clusters were randomly selected. A total of minimum 100 subjects of aged 40 years and above were examined from each randomly selected CEB. We followed compact segment sampling technique to select households.
Study definitions
In this study, URE was defined as presenting distance visual acuity (VA) <20/60 in any eye, that improved to better than or equal to 20/60 with pinhole examination in the absence of any significant internal and external finding such as corneal opacities, cataract, aphakia. VI was defined as presenting VA (PVA) <20/60 in the better eye. Blindness was defined as PVA <20/200 in the better eye. In cases, if there was more than one cause for VI, then as per WHO convention, the one which was more easily treatable or correctable to achieve VA better than 20/60 was considered as the primary cause of VI.
Data collection and examination
The tool used to collect data for this study was part of Delhi-RAVI study that was explained in a previous manuscript.[8] The survey was conducted during January to February 2013. Three different survey teams, each team comprising of one supervisor, one ophthalmologist, two optometrists, and three health workers were deputed for data collection. Ophthalmologist was involved because we intended to do ophthalmic examination to identify avoidable causes of blindness and VI in people aged 40 years and above. Optometrists examined distance and near VA and pinhole examination with assistance of one health worker each. Third health worker enumerated and took the consent. Detail of training and assessment of inter-observer agreement was explained in the previous manuscript.[8] The data were collected in a door-to-door survey from the selected CEB till 100 subjects of aged 40 years and above were examined. Distance VA was measured with a modified Snellen “E” chart with two optotype of 20/60 and 20/200. If necessary, the distance between subjects and chart is decreased as per standard protocol to record VA worse than 20/200. If VA <20/60, then pinhole assessment was done. VA of both eyes was recorded sequentially, i.e., right eye then left eye. All VA was measured at outdoors shaded but well-illuminated location. Detailed lens and retinal examination were also done with portable slit lamp and direct ophthalmoscope, in eye with PVA better than 20/60. Data were also collected using validated questionnaires to elicit information on barriers to correction of refractive error.
Ethical approval
Ethical approval was sought from Institute Ethics Committee. Survey was also undergone in accordance with ethical principles and adhered to Declaration of Helsinki. Informed and written consent were taken from each study subject before examination.
Data management
The data were collected onto a standardized RAVI Form that was developed for the survey and entered into especially designed database software on Microsoft access. Regular consistency checking, cleaning were performed before analysis. Data were analyzed using STATA-13 software package (Stata Corp., College Station Texas, USA). Descriptive statistics of basic demographic characteristics of study population was done. Multiple logistic regressions analysis was used to assess the association of relevant variables. The level of significant was set at P < 0.05.
Results
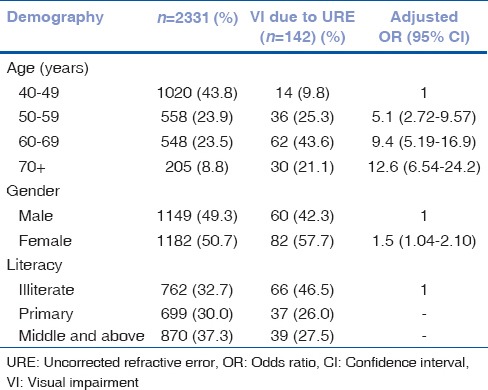
Of the 2421 individuals enumerated from 24 blocks, 2331 individuals were examined with 96.3% coverage (49.3% males vs. 50.7% females) [Table 1]. The mean age of all examined subjects was 51.32 ± 10.5 years old (standard deviation) with maximum examination being age groups 40–49 years (43.8%). While around 33% of the subjects were illiterate, 3.5% were graduates and above.
Table 1.
Association between sociodemographic profiles with visual impairment due to uncorrected refractive error
Uncorrected refractive error and visual impairment
Of the examined 2331 individuals, the VI in either eye due to URE was present in 275 individuals (11.8%, 95% CI: 10.5–13.1). Out of total visually impaired (PVA <20/60 in the better eye) subjects (n = 266), URE was the most common cause of VI 142 (53.4%), followed by cataract (90, 33.8%) and surgical complication (9, 3.4%), and posterior segment diseases (8, 3.0%), respectively. Five individuals of total URE were blind (PVA <20/200 in the better eye), contributing 9.8% of the total blindness (51). The overall prevalence of VI due to URE in the study population was 6.1% (95% CI: 5.1–7.0), whereas the age-adjusted prevalence was 5.8%. Prevalence of VI due to URE was lowest among the 40–49 years age groups (1.4%) and highest in 70+ age groups (14.6%).
Multiple logistic regression showed that odds of having VI due to URE was significantly higher among older age groups a (P < 0.001; odds ratio [OR] = 4.9; 9.2; 12.3 for age groups 50–59; 60–69; 70+ respectively); there was a 50% higher risk of having VI due to URE in females as compared to males (adjusted OR = 1.5; 95% CI: 1.04–2.10; P < 0.02) [Table 1].
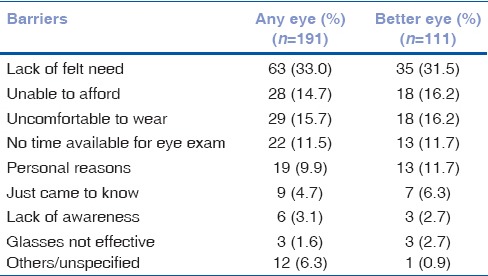
Barriers
One of the objectives of this study was to determine the reasons for not availing refractive error services despite the availability. In the study, 191 out of total 275 subjects with URE in any eye, and 111 of the total 142 subjects with URE in the better eye filled the barriers forms completely [Table 2]. Maximum number of respondents (any eye vs. better eye; 33% vs. 31.5%) reported that they were aware of the problem, but they did not feel the need for consultation; 28.7% in any eye and 16.2% in the better eye due to financial constraints. Similarly, 15.2% and 16.2% of the total due to personal reason such as uncomfortable to wear, teased about wearing spectacles, changes of facial appearances, slightly more than 11% in the both conditions due to lack of time.
Table 2.
Barriers to services utilization for refractive error (presenting visual acuity <20/60)
Discussion
This study, which is a part of the RAVI in Delhi reports the prevalence of VI due to URE and its barriers to correction in 40 years and above age groups of urban East Delhi.
The current study showed that URE is the most common cause of VI (53.4%) and the prevalence of VI due to the URE in the study population (VA <20/60 in the better eye) is 6.1%. Several studies have also reported that prevalence of VI attributed to URE is in the range of 4.8–18%.[9,10] A similar proportion within this range was also shown in our study (6.1%). Despite multiple studies conducted elsewhere on URE, comparison across the studies were difficult due lack of consistency in terms of case definition and demography.
VI due to URE was found to be higher in older age groups as well as female subjects. This finding was consistent with results from other studies conducted in Southern part of India,[5] Fotouhi et al. in Tehran[10] and Chan et al. in Eritrea of North East Africa.[11] The higher prevalence amongst the elder, indicate the urgency for corrections among these populations because uncorrected refractive error will further compound the already existing biological or geriatric comorbidities or disabilities, thereby leading to deterioration in the quality of life.[12] Appropriate and cost-effective intervention for URE in older population should be considered to have a better life. For example, multilevel efforts to provide refraction services, screening campaigns, creating more awareness among elderly population, working with existing health care delivery system. The strategy highlighted in the National Policy for Senior Citizen,[13] i.e., restoration of eyesight and vision among senior citizen under National Programme for Control of Blindness (NPCB) needs to be implemented in the time bound manner, like the NPCB presbyopia scheme under the 12th year plan.
Numerous studies have revealed that the lack of felt need for consultation and economic constraints were two most common reported barriers to correction for refractive error in developing countries.[14] Rapid assessment of refractive error study from South India also reported that these two barriers were 23% and 31%,[15] and 30% and 34% from Eritrea respectively. In this study also, it was reported 31.5% and 16.2% in case of better eye, respectively. Others reported barriers in case of better eye from our study were uncomfortable with the glasses (16.2%), lack of time for eye examination (11.7%), and lack of awareness (2.7%). Many of these barriers are related to human behaviors and attitudes. Marmamula et al. from South India classified barriers to services utilization from a population-based cross-sectional study as “relatively easy to change” and “difficult to change.”[15] The most common barrier in this study, i.e., lack of felt need comes under difficult to change which is related to human behaviors. Considering the second most common, i.e. unable to afford is also indirectly related to human behaviors and attitudes toward the refractive error. This finding reflected that despite such a cost-effective and cheaper measures are available in urban area to correct refractive error, people living in the urban resettlement colony are not willing to spend their household income for correction of refractive error. Ironically, anecdotal evidence showed that each family owns multiple electronic gadgets such as television with cable connections, multiple mobile phones, and music system. This implies lesser seriousness on refractive error amongst urban dweller. One probable reason could be that people in the urban resettlement are migrants and prefer spending their household income on purchasing these electronic gadgets rather than spending on health.
Awareness and education activities and sensitization among urban resettlement and migrants need to be done regarding consequence and impact refractive errors if uncorrected. Further studies are warranted on qualitative or human behaviors pertaining to behavioral and social science research to explore people's attitude or behaviors toward the refractive errors. This will act as a supplement tool while developing intervention strategies. Understanding the diverse individual, familial, social, and cultural factors that influence the individual's adoption, or maintenance of health promoting or protecting behavior can be useful in planning appropriate strategies and implementation to ensure the provision of optimal eye health-care services of India.
Although there are some inherent limitation in the use of the rapid assessment technique and used of pinhole for defining refractive errors, the results of the study provide valuable baseline information for planning of refractive error services. The prevalence of refractive error cannot be highlighted since unaided vision assessment was not done during the study. Further, the results also revealed that need of behavioral and social science research to know the community perception on refractive error and spectacles uses.
Conclusion
More than half of visual impairment amongst urban adult population of Delhi is due to uncorrected refractive error. Elderly population and females are more likely to suffer. The human behavior factors like lack of felt need for consultation and financial constraints were the two most common reported barriers for service utilization of refractive error.
Financial support and sponsorship
Sightsavers India, a non-governmental organization funded the VISION DELHI project. The RAVI survey was conducted as part of this project to provide baseline information about the need of refractive error services in this region.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96:614–8. doi: 10.1136/bjophthalmol-2011-300539. [DOI] [PubMed] [Google Scholar]
- 2.Naidoo K, Ravilla D. Delivering refractive error services: Primary eye care centres and outreach. Community Eye Health. 2007;20:42–4. [PMC free article] [PubMed] [Google Scholar]
- 3.Dandona L, Dandona R, Srinivas M, Giridhar P, Vilas K, Prasad MN, et al. Blindness in the Indian state of Andhra Pradesh. Invest Ophthalmol Vis Sci. 2001;42:908–16. [PubMed] [Google Scholar]
- 4.Dandona R, Dandona L, Srinivas M, Giridhar P, McCarty CA, Rao GN. Population-based assessment of refractive error in India: The Andhra Pradesh eye disease study. Clin Experiment Ophthalmol. 2002;30:84–93. doi: 10.1046/j.1442-6404.2002.00492.x. [DOI] [PubMed] [Google Scholar]
- 5.Marmamula S, Madala SR, Rao GN. Prevalence of uncorrected refractive errors, presbyopia and spectacle coverage in marine fishing communities in South India: Rapid Assessment of Visual Impairment (RAVI) project. Ophthalmic Physiol Opt. 2012;32:149–55. doi: 10.1111/j.1475-1313.2012.00893.x. [DOI] [PubMed] [Google Scholar]
- 6.Marmamula S, Narsaiah S, Shekhar K, Khanna RC, Rao GN. Visual impairment in the South Indian state of Andhra Pradesh: Andhra Pradesh -rapid assessment of visual impairment (AP-RAVI) project. PLoS One. 2013;8:e70120. doi: 10.1371/journal.pone.0070120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Register General, Ministry of Home Affairs, Government of India, Census Data. 2011. [Last accessed on 2014 Oct 18]. Available from: http://www.censusindia.gov.in/
- 8.Gupta N, Vashist P, Malhotra S, Senjam SS, Misra V, Bhardwaj A. Rapid assessment of visual impairment in urban population of Delhi, India. PLoS One. 2015;10:e0124206. doi: 10.1371/journal.pone.0124206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Robinson B, Feng Y, Woods CA, Fonn D, Gold D, Gordon K. Prevalence of visual impairment and uncorrected refractive error – Report from a Canadian urban population-based study. Ophthalmic Epidemiol. 2013;20:123–30. doi: 10.3109/09286586.2013.789915. [DOI] [PubMed] [Google Scholar]
- 10.Fotouhi A, Hashemi H, Raissi B, Mohammad K. Uncorrected refractive errors and spectacle utilisation rate in Tehran: The unmet need. Br J Ophthalmol. 2006;90:534–7. doi: 10.1136/bjo.2005.088344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chan VF, Mebrahtu G, Ramson P, Wepo M, Naidoo KS. Prevalence of refractive error and spectacle coverage in Zoba Ma'ekel Eritrea: A rapid assessment of refractive error. Ophthalmic Epidemiol. 2013;20:131–7. doi: 10.3109/09286586.2013.783082. [DOI] [PubMed] [Google Scholar]
- 12.Evans BJ, Rowlands G. Correctable visual impairment in older people: A major unmet need. Ophthalmic Physiol Opt. 2004;24:161–80. doi: 10.1111/j.1475-1313.2004.00197.x. [DOI] [PubMed] [Google Scholar]
- 13.Social Defence for Senior Citizens.Policies/Acts/Rules/Codes/Circulars, National Policy on Senior Citizens 2011, Ministry of Social Justice and Empowerment, Government of India. [Last accessed on 2015 Oct 12]. Available from: http://www.socialjustice.nic.in/consd.php .
- 14.Naidoo KS, Jaggernath J. Uncorrected refractive errors. Indian J Ophthalmol. 2012;60:432–7. doi: 10.4103/0301-4738.100543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Marmamula S, Keeffe JE, Raman U, Rao GN. Population-based cross-sectional study of barriers to utilisation of refraction services in South India: Rapid Assessment of Refractive Errors (RARE) Study. BMJ Open. 2011;1:e000172. doi: 10.1136/bmjopen-2011-000172. [DOI] [PMC free article] [PubMed] [Google Scholar]