

Abstract
Visceral leishmaniasis (VL) is a zoonosis found worldwide. Its incidence has increased in Brazil in recent years, representing a serious public and animal health problem. The strategies applied in Brazil are questionable and are not sufficient to control the disease. Thus, we have compared the efficacy of some of the currently available strategies focused on dogs to prevent and control zoonotic VL in endemic areas by optimizing a mathematical model. The simulations showed that the elimination of seropositive dogs, the use of insecticide-impregnated dog collars, and the vaccination of dogs significantly contribute to reducing the prevalence of infection in both canines and humans. The use of insecticide-impregnated collars presented the highest level of efficacy mainly because it directly affected the force of infection and vector-dog contact. In addition, when used at a coverage rate of 90%, insecticide-impregnated collar was able to decrease the prevalence of seropositive dogs and humans to zero; moreover, because of the easy application and acceptance by the targeted population, these collars may be considered the most feasible for inclusion in public policies among the three simulated measures. Vaccination and euthanasia were efficacious, but the latter method is strongly criticized on ethical grounds, and both methods present difficulties for inclusion in public policies. When we compared the use of euthanasia and vaccination at coverages of 70 and 90%, respectively, the proportion of infected populations were similar. However, on evaluating the implications of both of these methods, particularly the negative aspects of culling dogs and the proportion of animals protected by vaccination, the latter measure appears to be the better option if the total cost is not significantly higher. The comparison of complications and advantages of different control strategies allows us to analyze the optimal measure and offer strategies to veterinary and public health authorities for making decisions to prevent and control zoonotic VL. Hence, improvements in both public and animal health can be achieved in regions with scenarios similar to that considered in the present study; such scenarios are characteristically found in some areas of Brazil and other countries.
Introduction
Visceral leishmaniasis (VL) is a widely distributed zoonosis that is found worldwide [1]. In Brazil, 22,491 confirmed human cases and 1,599 deaths occurred from VL from 2007 to 2013 [2], with gradual spreading across all states and a general association with poor living conditions [3]. The primary etiological agent of VL in the Americas is Leishmania (Leishmania) infantum, which is mainly transmitted through the bites of infected phlebotomine sandflies [4], particularly the specie Lutzomyia longipalpis [5–7]. Infected dogs constitute the main domestic reservoir of the parasite and play a key role in its transmission to humans [8,9].
The current strategies for the prevention and control of VL applied by the Brazilian Health Ministry include 1) early diagnosis and adequate treatment of human cases; 2) use of residual insecticides and sanitary measures targeting the home environment to reduce vector density; and 3) identification and elimination of domestic reservoirs [10]. The elimination of seropositive dogs is increasingly discussed and assessed [11–17], particularly concerning its effect on reducing the prevalence of human and canine disease and its acceptance by the animals’ owners and animal protection institutions [18].
According to Vieira & Coelho [19], approximately 20,000 seropositive dogs are eliminated every year in Brazil. More than 96 million dollars were invested in the program for the control of leishmaniasis from 1988 to 1996, during which more than 150,000 seropositive dogs were euthanized and insecticides were applied in more than one million households [20]. Despite the available resources and the effort invested, the ongoing Brazilian Leishmaniasis Control Program failed to reduce the occurrence of the disease to an acceptable level [3]. Indeed, the prevalence of VL has increased, and the disease has become a serious public health problem in several Brazilian states, indicating that more focused efforts are required [3].
Thus, there is a need for a closer approximation between researchers and public health workers to revise the current control strategies and to define procedures capable of accurately assessing their effects [21]. Alternatively, there are other measures available for prevention and control of VL, which have not yet been implemented on a large scale; these include insecticide-impregnated dog collars, which have been proven efficacious in protecting animals from sandflies [22–25], and Leish-Tec®, which is the currently available vaccine for dogs in Brazil. This vaccine has an efficacy of 71%, as determined by the dogs that remain uninfected.[26].
Mathematical models are an important tool used by researchers for the study of the control measures; they can be used to simulate the population dynamics of infectious diseases [27]. An ever-expanding number of diseases and public health questions are being addressed, and the models are able to supply elements useful for the formulation of public policies for the control of diseases [26,27]. Previously developed VL models in Brazil have focused on evaluating prevention and control measures [13,26,27,14,28,29,21]. However, they do not compare all of the currently available measures applied on dogs, and in different coverages, and they do not consider some particular factors, such as an rently available measures atlable measures at an endemica en and dog cases he recovered staget the third analisis the seropomortalitymorrrrmommbothmortality, the repellent effect of the insecticide-impregnated collars or the efficacy of the available vaccines. In addition, they do not include certain characteristics that are necessary to reflect the biological reality of the dynamic disease, such as the clinical-immunologic conditions of the hosts.
This study adapted a model of VL proposed by Burattini et al. [29]; however, we also included distinct values for the the parameters of the forces of infection to the hosts and vector, and we introduced measures that were not previously addressed. Thus, we compared the efficacy of some of the available measures that focus on dogs, to be used in public policy such as deltamethrin-impregnated collars, vaccination and culling, using the VL mathematical model. This study was developed to contribute information to veterinary and public health authorities regarding the current practices of zoonotic VL prevention and control in endemic scenarios, such as in Brazil. Therefore, we have evaluated the optimal measures necessary to considerably decrease the number of human and dog VL cases.
Materials and Methods
Model
The mathematical model formulated by Burattini et al. [29] was adapted to allow for the simulation of the control measures. For this purpose, the targeted populations were classified based on their clinical-immune status.
It was assumed that the three targeted populations (humans, dogs and vectors) were constant and that the odds of infection were the same among the various hosts’ age ranges, without seasonal variation.
The disease dynamics in the various populations considering the preventive and control measures are depicted in Fig 1.
Fig 1. Model of compartments and the flow among them.

Legend: blue: human populations; pink: vector populations; yellow: dog populations not subjected to interventions; red: vaccinated dog populations; green: collar-wearing dog populations; orange: mortality by euthanasia.
The model is described next.
Humans
Humans are born susceptible (Sh) at a rate of Ωh and are infected at a rate of bahmhV3, in which b is the proportion of infective bites, ah is the average number of daily vector bites on humans, and mh is the vector density per human host (eqs 1 and 2). Following infection, humans become infected but are not infective; thus, they enter compartment Lh. Fraction fm of the infected, non-infective individuals remains asymptomatic at the compartment Ah1 until they recover from the disease, and move to that a rate of βhfm, whereas fraction fd develops symptoms and moves to compartment Ah2 at a rate of βhfd (eqs 2–4). The individuals in compartments Ah1 and Ah2 are considered to be asymptomatic, and they are discriminated according to their next stage. The value of βh is given by the inverse of the time an individual remains non-infective and lacks humoral immunity. The infective individuals in compartment Ah1 become resistant as a function of the development of cell-mediated immunity, and they move to compartment Rh at a rate of δh, whereas the infective individuals in Ah2 develop disease at a rate of φh and move to the compartment of the diseased individuals, Dh. It was assumed that the diseased individuals are hospitalized and thus move to compartment Th at a rate of tth, losing their infective capacity. At the hospital, humans may either die from VL at a rate of αh or recover, whereby they move to compartment Rh at a rate of σh. With the loss of cellular immunity, the recovered individuals become susceptible again, thus moving to compartment Sh at a rate of γh. All humans are subjected to the natural mortality rate μh (eqs 1–7).
| (1) |
| (2) |
| (3) |
| (4) |
| (5) |
| (6) |
| (7) |
Dogs
Dogs are born susceptible, Sd, at a rate of Ωd and enter compartment Ld when they are infected, which occurs at a rate of bacmcV3, in which b is the proportion of infecting bites, ac is the average number of daily vector bites on dogs, and mc is the vector density per canine host (eqs 8 and 9). Following infection, dogs are infected but not infective in this compartment; a fraction (fl) of these individuals remain asymptomatic for their entire lives and move to compartment Ad1, whereas a fraction (fr) remain asymptomatic at the compartment Ad2 until they recover from the disease. Those that develop symptoms (the fraction fe) move to compartment Ad3. The individuals in Ad1, Ad2 and Ad3 are considered asymptomatic, and they are discriminated according to their next stage. The development of infectiveness and humoral immunity, with the move of the individuals in compartment Ld to compartments Ad1, Ad2 and Ad3, occurs at rates of βcfl, βcfr and βcfe, respectively (eqs 9–12); the value of βc is given by the inverse of the time an individual remains non-infective and lacking humoral immunity. Individuals Ad2 become resistant as a function of the development of cell-mediated immunity, and they move to compartment Rd at a rate of δc, whereas individuals Ad3 become diseased at a rate of φc, thus moving to compartment Dd. These latter individuals may die from the disease at a rate of αc or recover (Rd) at a rate of σd. The recovered individuals lose their cellular immunity and become susceptible (Sd) at a rate of γd (eq 13). The treatment of diseased animals was not considered. All dogs were subjected to the natural mortality rate μc (eqs 8–14).
The prevention and control methods are described next.
Insecticide-impregnated Collar: The use of collars as a preventive and control measure was simulated by assuming a rate of application ω to all of the dog population compartments, which is applied independent from the clinical-immune status of the animals. The collars have two effects: 1) they inhibit vector bites, and 2) they cause the death of the insects that bite the animals wearing them [23]. The effect of bite inhibition manifests as a reduction of the value of ac, which becomes acc (eqs 15, 16, 23 and 24). The mortality resulting from the collar insecticide effect was considered instantaneous; k represents the proportion of insects that die after biting a collar-wearing dog. As a result, the rate of infection of insects that bite collar-wearing dogs in compartments Adc1, Adc2 and Adc3 is represented by cclacc(1-k), whereas the rate corresponding to the insects that bite collar-wearing dogs in compartment Ddc is represented by cceacc(1-k) (see eqs 23 and 24).
After feeding on collar-wearing dogs and eventually infecting them, vectors (V3) die at a rate of μr as a result of the collar-induced mortality (eq 25). When the efficacy of the collar is lost, at a rate “ψ”, the animal that is using it returns to the previous compartment without collars (eqs 15–21). At this model is being considered the immediate replacement of the collars in case of loss and damage.
Vaccination: It was assumed that vaccinated animals do not develop infection, and hence do not infect the vector. Vaccination is applied to seronegative, such as susceptible (Sd), recovered (Rd) and newly infected non-infective (Ld) dogs at a rate of ρ. This rate corresponds to the percentage of dogs per year that are intended to receive protection; it was calculated by taking the efficacy of the vaccine into consideration (Table 1). The loss of vaccine-induced immunity occurs at a rate of ε (eq 22).
Table 1. Symbols and biological meanings of the parameters included in the model with the corresponding values and references.
| SYMBOLS AND BIOLOGICAL MEANING | VALUES | REFERENCES | |
|---|---|---|---|
| HUMANS | |||
| μh | Natural mortality rate | 3.69x10-5 day-1 | [62] |
| αh | VL lethality | 1.38x10-2 year-1 | [2] |
| ah | Average daily human bites by vector | 1.4x10-1day-1 | Assumed (based on Ovallos, [63]) |
| mh | Vector density per human | 1.07x10-1 | Assumed (based on Ovallos, 2013—oral communication) |
| βh | Latency period (L→A) | 3.3x10-2day-1 | Estimated (based on Maia et al. [64]) |
| δh | Recovery rate of asymptomatic individuals (A→R) | 9.1x10-4 day-1 | Estimated (based on Badaro et al. [5]; Carvalho et al. [65]; Silva et al.[66]) |
| fm | Proportion of asymptomatic individuals who recover | 83x10-2 | [67] |
| φh | Rate of symptom development (A→D) | 4.8x10-3 day-1 | Estimated (based on Brazilian Ministery, [10]) |
| fd | Proportion of individuals who become symptomatic | 17x10-2 | [67] |
| tth | Treatment rate (T→R) | 2.0x10-2 day-1 | [68] |
| σh | Recovery rate of treated individuals (D→R) | 1.4x10-3 day-1 | Estimated (based on Carvalho et al. [65]; Silva et al.[66]; Alvar [69]) |
| γh | Loss of cell-mediated immunity (R→S) | 5.47x10-4 day-1 | Estimated (based on Badaro et al. [5]; Carvalho et al. [65]; Silva et al.[66]; Alvar [69]) |
| Ωh | Birth rate | αh + μh | |
| DOGS | |||
| μc | Natural mortality rate | 9.23x10-4 day-1 | [70] |
| αc | VL lethality | 2.12 year-1 | [71] |
| ac | Average daily dog bites by vector | 1.4x10-1 day-1 | Assumed (based on Galvis [63]) |
| mc | Vector density per dog | 1.94 | Galvis, 2013 (oral communication) |
| βc | Latency period (L→A) | 3.3x10-2 day-1 | [64] |
| fL | Proportion of individuals that remain asymptomatic | 22x10-2 | [72] |
| δc | Recovery rate of asymptomatic individuals (A→R) | 5.5x10-3 day-1 | Estimated (based on Fisa et al. [73]; Silva et al. [74]) |
| fR | Proportion of asymptomatic individuals that recover | 45x10-2 | [72] |
| φc | Rate of development of symptoms (A→D) | 1.1x10-2 day-1 | Estimated |
| fe | Proportion of individuals that become symptomatic | 32x10-2 | [72] |
| σc | Recovery rate of diseased individuals (D→R) | 2.73x10-3 day-1 | Estimated (based on Garcia et al. [72]; Pozio et al. [71]) |
| γc | Loss of cell-mediated immunity (R→S) | 2.73x10-3 day-1 | Assumed |
| Ωc | Birth rate | αc + μc | |
| VECTOR | |||
| μv | Life expectancy of non-infected vectors | 9.09x10-2 day-1 | [75] |
| μf | Life expectancy of infected, non-infective vectors | 1.67x10-1 day-1 | [75] |
| μm | Life expectancy of infected and infective vectors | 2.5x10-1 day-1 | Estimated (based on Kamhawi [76]) |
| τ | Extrinsic incubation period | 2.0x10-1 day-1 | [76] |
| b | Fraction of infective bites | 1.5x10-1 | Assumed (based on Burattini et al. [29]) |
| chl | Proportion of insects that acquire infection after biting latent humans | zero | [77] |
| che | Proportion of insects that acquire infection after biting diseased humans | 1.2 x10-2 | [77] |
| ccl | Proportion of insects that acquire infection after biting latent dogs | 38.5x10-2 | [78] |
| cce | Proportion of insects that acquire infection after biting diseased dogs | 24.7x10-2 | [78] |
| Ωf | Birth rate | μv + μf + μm + μR | |
| SYMBOLS OF INTERVENTIONS | |||
| μe | Rate of latent dog culling X test sensitivity | Coverage X Ss | |
| μs | Rate of diseased dog culling X test sensitivity | Coverage X Sa | |
| ρ | Rate of dogs protected by vaccination X vaccine efficacy | Coverage X VE | |
| VE | Vaccine efficacy | 75% | Approximated value of vaccine efficacies of Leish-Tec® [26] |
| ε | Loss of vaccine-induced immunity | 2.7x10-3 day-1 | [79] |
| ω | Rate of collar use | Coverage | |
| ψ | Loss of collar effect | 2.8x10-3 day-1 | [23] |
| acc | Average daily collar-wearing dog bites by vector ad X (1 –collar repellent effect) | ad X 10x10-2 | [23] |
| CE | Average rate of collar repellent effect | 90x10-2 | [23] |
| μR | Mortality of insects that bite collar-wearing dogs | acc X k | |
| k | Average collar-induced vector mortality rate | 55x10-2 | [23] |
| Sa | Test sensitivity in asymptomatic dogs | 98x10-2 | [50] |
| Ss | Test sensitivity in symptomatic dogs | 47x10-2 | [50] |
Vaccination does not inhibit the development of disease when dogs are vaccinated during the “immunological window” (Ld), therefore, when dogs are vaccinated while in compartment Ld, they do not move to compartment P but remain in the same compartment, where they undergo the natural course of the infection. However, these individuals must be considered in the calculation of the vaccine doses because they are, in fact, vaccinated.
Euthanasia: The elimination of asymptomatic (Ad1, Ad2, Ad3, Adc1, Adc2 and Adc3) and symptomatic (Dd and Ddc) seropositive dogs occurs at rates μe and μs, respectively (eqs 10–12, 17–19, 13 and 20, respectively). These rates differ because they take into consideration the fact that the test sensitivity varies according to the animals’ clinical status. In this model we assume that the populations are constants, thus all dogs that die are added to the compartment of susceptibles, include those euthanized (eq 8).
The euthanasia of 70 and 50% of the seropositive dogs indicates that the average times that these animals remain in the environment are theoretically 1.37 and 1.67 years, respectively, for asymptomatic animals, and 0.67 and 1.00 years, respectively, for symptomatic animals. The symptomatic dogs remain in the environment for a shorter amount of time compared to the asymptomatic dogs because of the improved sensitivity of the diagnostic test. These data were calculated as the inverse of the life expectancy.
| (8) |
| (9) |
| (10) |
| (11) |
| (12) |
| (13) |
| (14) |
| (15) |
| (16) |
| (17) |
| (18) |
| (19) |
| (20) |
| (21) |
| (22) |
Vector
The vector insects are born susceptible (V1) at a rate of Ωf and become infected upon biting infective individuals (Ah1, Ah2, Dh, Ad1, Ad2, Ad3 and Dd) at a rate that depends on the fraction of insects that acquires infection after a bite (chl, che, ccl and cce, respectively) and the average number of bites on human (ah) or dog (ac) hosts per day (eqs 24 and 25). These parameters differ because they vary in each population. The infected insects (V2) become infective (V3) at a rate of τ, which is defined by the extrinsic incubation period. The vector mortality rate is given by μv, μf and μm for each of its phases (V1, V2 and V3, respectively) (eqs 23–25).
| (23) |
| (24) |
| (25) |
Model parameters
Some of the parameters that we used were obtained from studies performed in the city of Panorama, São Paulo, Brazil, and others were estimated or adjusted to represent the actual situation in that city (Table 1). The canine seroprevalence in that municipality between August 2012 and February 2013 was 25% (LOPES et al., non-published). This region represents a scenario of some visceral leishmaniasis endemic areas in Brazil, and with similar conditions according to the public health system, with low-income, and political structure.
Simulated scenarios
The three preventive and control measures were simulated with 70 and 90% coverage. The simulations were performed using Matlab version R2013a.
Sensitivity of the model
To evaluate the sensitivity of the model parameters, the density of the vector per host, the average daily hosts by the vector, and the life expectancy of the infected vectors were varied by 0.5%, 1%, 4%, 7% and 10%. Thus, the average seroprevalence variations of human and dog populations for each parameter were calculated and are presented in Fig 2.
Fig 2. Effect of the parameter variations in the host seroprevalences.
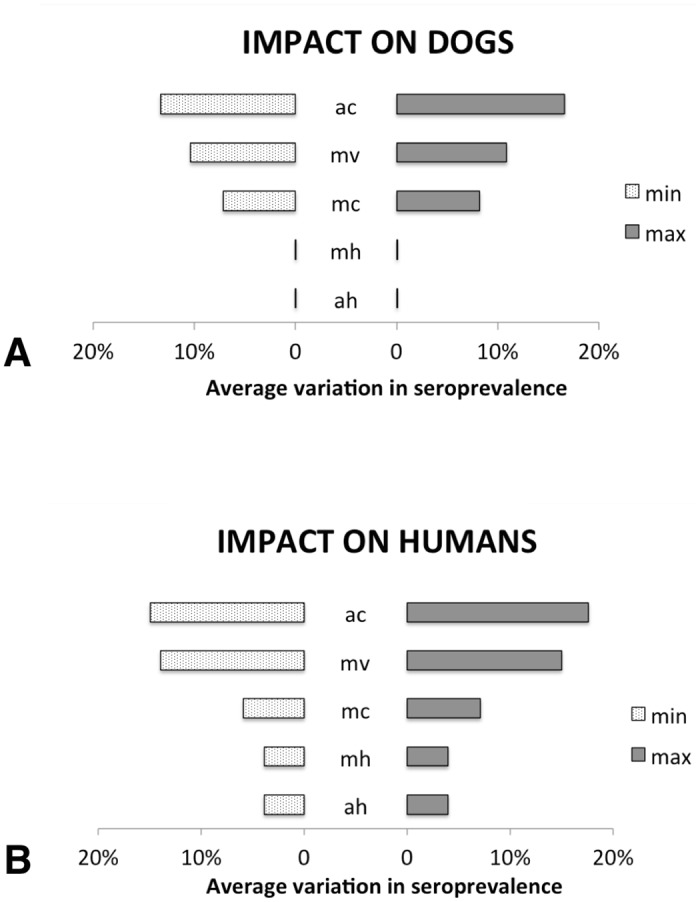
Average variations in dog (A) and human (B) seroprevalences according to the maximum (max) and minimum (min) values of the parameter variations. Legend: ah) average daily human bites by the vector; ac) average daily dog bites by the vector; mh) density of the vector per human; mc) density of the vector per dog; mv) life expectancy of the infected vectors (muf and mum).
Results
Simulation of control measures
The results of the simulations were plotted in graphs representing the dog, human and vector populations as a function of time. These populations were estimated from the time that they reached a stable equilibrium to allow the comparison of the measures applied, as Table 2 shows.
Table 2. Proportions of the human, dog, and vector populations.
| Intervention | Cover | HUMANS | DOGS | VECTORS | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asympt (L+A) | Sick (D) | Recov | Protec | Cover | Susc | Asympt (L+A) | Sick (D) | Recov | Protec | V1 | V2+V3 | ||
| WITHOUT | 25.0% | 2.13% | 8.8% | 0.0% | 86.3% | 25.0% | 2.13% | 8.8% | 0.0% | 93.99% | 6.01% | ||
| VAC | 90% | 3.1% | 0.24% | 0.5% | 44.2% | 90% | 96.7% | 3.1% | 0.24% | 0.5% | 44.2% | 99.20% | 0.80% |
| 70% | 6.9% | 0.57% | 1.5% | 33.1% | 70% | 94.6% | 6.9% | 0.57% | 1.5% | 33.1% | 98.25% | 1.75% | |
| COLL | 90% | 0.2% | 0.01% | 0.0% | 0.0% | 90% | 99.3% | 0.2% | 0.01% | 0.0% | 0.0% | 99.97% | 0.03% |
| 70% | 1.4% | 0.10% | 0.4% | 0.0% | 70% | 98.4% | 1.4% | 0.10% | 0.4% | 0.0% | 99.76% | 0.24% | |
| EUT | 90% | 0.3% | 0.02% | 0.2% | 0.0% | 90% | 99.0% | 0.3% | 0.02% | 0.2% | 0.0% | 99.92% | 0.08% |
| 70% | 2.2% | 0.20% | 1.0% | 0.0% | 70% | 97.6% | 2.2% | 0.20% | 1.0% | 0.0% | 99.47% | 0.53% | |
Impregnated-insecticide collar (COLL), vaccination (VAC) and euthanasia (EUT) according to the coverage (cover.) rates. For humans and dogs: Susc: susceptible; Asympt: asymptomatic (L: latent and A: asymptomatic); sick (D: with symptoms); Recov: recovered; T: humans in treatment; R: hunans recovered; Protec: dogs protected by the vaccine. For vectors: V1: non-infected; V2: infected but not infective; V3: infective.
The measures associated with the lowest proportions of humans and dogs in the infective stages and infected insects were considered the most efficacious measures because they indicated that the prevalence of VL was reduced.
The seroprevalences in Table 2 show that all of the simulated measures had significant favorable effects on the dog and human populations, i.e., the proportions of infected dogs and humans in both the symptomatic and asymptomatic stages decreased substantially until attaining stable equilibrium. The effect of the collar was more intense than that of euthanasia and vaccination for these infected populations. The proportion of asymptomatic dogs and humans prior to the intervention were 25% and 4.81%, respectively; these values decreased by approximately fifteen and ten times, reaching less than 1.5% and 0.4%, respectively, when the collar was used at a coverage rate of 90%. When 90% of the seropositive dogs were culled, these values decreased by approximately ten and eight times, reaching less than 2.5% and 0.6%, respectively, and vaccination of 90% of the seronegative dogs caused these values to decrease by approximately four and three times, reaching less than 7% and 1.7%, respectively.
A 90% coverage rate of the insecticide-impregnated collar resulted in eliminating the sick population of humans and reducing the number of sick dogs to nearly zero percent. Euthanizing 90% of the seropositive dogs decreased the number of sick animals to nearly zero (0.02%) as well, and vaccination reached a rate of 0.24%.
The proportion of susceptible individuals increased significantly, reaching nearly one hundred percent when using the collar and culling in 70% and 90% of the population, respectively. Conversely, with the use of vaccination, the proportion of susceptible dogs was the lowest with respect to the use of other measures and when no measures were used. However, the protected animals represented a significant proportion of the population when the seronegative dogs were vaccinated at rates of 70 or 90%.
The variation in the coverage rates of all three simulated measures, ranging from 70 to 90%, strongly affected the prevalence rates generated in the dog and human populations. When the coverage rate of the collar increases from 70 to 90%, the proportion of sick dogs decreases ten times (from 0.10 to 0.01%), and the proportion of asymptomatic human decreases by five times (from 0.31 to 0.06%). When the coverage of the vaccine increases from 70 to 90%, the proportion of sick dogs and humans is nearly cut in half, from 0.57 to 0.24% and from 0.014 to 0.007%, respectively, and the proportion of asymptomatic dogs and humans is also reduced from 6.9 to 3.1% and from 1.65 to 0.87%, respectively.
The scenario of infected humans and dogs (sick and asymptomatic) is similar when using a vaccination coverage rate of 90% and a euthanasia rate of 70%; however, euthanasia does not result in a protected population.
Sensitivity of the model
Variations in the amplitude of the dog and human seroprevalences highlight that the most sensitive parameters are those that represent the vector contact with dogs, in particular the average daily bites by the vector. The life expectancy of the infected vectors is also sensitive in this model. Both the average daily bites by the vector in humans bitten (ah) and the density of the vector per human (mh) parameters present a similar behavior: they were less sensitive and affected just the infected human population.
Discussion and Conclusion
All of the control measures applied to the dogs, in the different coverages, were associated with a decrease in the prevalence of infection in the human population, indicating the importance of the infected dog population in the occurrence of VL in humans. Similarly, Burattini et al. [29] (based on a mathematical model) and Nunes et al. [30] observed that the establishment of this disease as endemic among humans is highly dependent on its prevalence among the dog population.
Among the control measures simulated in the present study, the deltamethrin-impregnated collar was associated with the most significant effects. The decrease in asymptomatic dogs and humans by approximately fifteen and ten times, respectively, after the use of the collar in 90% of the dogs represents a large number of individuals in the environment. Thus, it is worth noting that the simulation of collar use encompassed a larger number of animals because it included both the seronegative and seropositive dogs. Such observations were also made by Reithinger et al. [25], who stated that the proportion of dogs wearing collars must be quite high to achieve a significant reduction of VL prevalence. In this regard, the application of collars to dogs that replace others in a given population and the rapid replacement of collars are considered crucial because the rate of collar loss or damage, can vary among 4.9% (1,796/36,638) [15], and 23% (289/1,246) [31] or 0.006 per day [25]. In our model we considered the immediately replacement of these collars, which implies in permanent surveillance to ensure the continuous protection as suggested by Oliveira-Lima et al. [31].
The efficacy of collars as a method for the control of VL is a result of two factors. The first is associated with its insecticide effect, in which the number of newly infected insects (represented by compartment V3) decreases because a significant fraction of them die after its contact with the dogs. This effect was also demonstrated indirectly in other studies that simulated the use of insecticides and found a substantial reduction in the disease prevalence in and humans. In another study with topic insecticides, it was observed that it reduced the probability of introduction and establishment of canine leishmaniasis [32]. The other factor concerns the repellent effect of the collar, which manifests as reductions in the average number of bites per day (ac and ah), consequently reducing the force of infection and the rate of infected insects. However, the repellent effect may hinder the insects from biting collar-wearing animals and make them bite other reservoirs.
These two factors are associated with the more sensitive parameters in the model, which include those related to vector contact with dogs and the mortality rates of infected vectors; thus, this measure significantly affects the leishmaniasis dynamic.
The large-scale use of deltamethrin-impregnated dog collars over two years in Italy promoted a reduction of 50% in the incidence of canine VL after the first year and 98% after the second year in one study [33]; another study showed a reduction of 83% after one year [34]. In a study conducted in Iran, the risk of seroconversion after infection with Leishmania spp. decreased among collar-wearing dogs, and the seroprevalence of disease decreased among children [24]. Similarly, the application of collars to 88% of the dogs in Andradina, São Paulo, Brazil, over two years reduced the seroprevalence of canine disease from 10.8 to 4.8% and decreased its incidence among humans [15]. In the present study, the simulated application of collars to 90% of the canine population induced a higher and strong reduction of the seroprevalence among both dogs and humans, from 27.1 to 0.2% and from 4.85 to 0.06%, respectively, which agrees with the empirical data.
The possible occurrence of allergic dermatitis in some of the animals must be considered relative to the large-scale use of collars. In a study by Camargo-Neves et al. [15], the proportion of affected animals was 2.3% (832/36,638). Some cases of dermatitis require treatment; thus, monitoring the animals and providing them with veterinary care are highly important. In addition, the application of collars to 70 or 90% of the dogs in a population, as was simulated in the present study, requires intense effort. Although this strategy does not require previous serologic tests, these coverages correspond to a high number of dogs, because these rates refer to the total population (i.e., seropositive and seronegative animals), and the collars must be replaced every six months or immediately in case of loss and damage.
The per capita incidence of a disease in a population is known as the force of infection, and it can be reduced through vaccination, thus making individuals pass from the status of susceptible to resistant while by-passing the state of infection [35]. According to their efficacy, vaccines may induce the full elimination of an agent by reducing the number of secondary cases [35]. Foroughi-Parvar & Hatam [36] state that vaccines are the best choices to access a convenient and efficacious method for the control of zoonotic VL.
The efficacy of vaccination depends on the coverage rate. Using a mathematical model, Dye [27] confirmed that when a vaccination has 100% efficacy, it is more effective than culling; however, the proportions of animals subjected to vaccination and culling in his study were not made clear. Dye further observed that at the time the study was performed, there were no vaccines with 100% efficacy, which is still the case. The CaniLeish® vaccine, which is available in Europe, displayed similar efficacy (70%) to Leish-Tec®, as used in this study. According to Gradoni et al. [37], studies on vaccines for leishmaniasis are still in need of impetus to develop efficacious and universally applicable vaccines. However, in recent decades, major research has been conducted to innovate new vaccines [36].
In our study, we simulated a vaccine with an efficacy of 75%. Using a higher efficacy in the simulations would result in better outcomes and would also decrease the number of animal subjects to infection, resulting in a low force of infection to susceptible dogs, which significantly influences the disease dynamic, as observed in the sensitivity analysis of the parameter.
The simulated vaccination of dogs in the present study substantially reduced the proportion of infected humans, as was also observed in the theoretical study by Dye [27]. Reis et al. [38] affirmed that the induction of a protective anti-Leishmania immunity response in dogs is a feasible, important, and cost-effective goal that highly affects the control of human leishmaniasis [27]. Palatnik-de-Sousa et al. [39] analyzed studies on dog vaccination conducted in Brazil and found that the reduction of the prevalence of canine and human disease was directly related to the increase in the number of vaccinated dogs.
From an epidemiological viewpoint, the main goal is to reduce the number of non-infected and non-infective animal and human hosts and therefore eliminate the disease agent from the environment. The vaccine was able to considerably decrease the number of infected hosts and was still able to make a large proportion of the protected animals susceptible, which is a great advantage.
In the present model we simulated data about the available vaccine in Brazil (Leishtec®). Although this vaccine presents an importance efficacy a recent study observed local and systemic adverse effects in 13% (6/46) of the vaccinated animals [40]. Therefore, these adverse effects represent a potential limitation of this strategy since it may affect compliance and might require veterinary assistance.
Although Marzochi et al. [41] suggest that vaccination is an efficient control measure and recommend its application concomitantly to the anti-rabies vaccination program, some considerations should be mentioned: 1) the efficacy of the vaccines has not yet been clearly established, 2) their individual cost is high, and 3) the application regimen involves three initial doses and demands previous serologic testing. Furthermore, adding the leishmaniasis vaccine to the anti-rabies vaccination program requires that pet owners take their dogs to a vaccination point, which can be a logistic complication because endemic areas are normally associated with low-income regions [42,43,44,45,46]. Consequently, it is difficult to establish vaccination as a public policy.
The euthanasia of seropositive dogs was efficacious in the present study, to reduce the prevalence of the infection. However, it requires a significant sampling effort and its application is strongly criticized on ethical grounds, with resistance from the population of the dog owners and workers who perform this function. Particularly one of the difficulties of euthanize practice refers to the elimination of asymptomatic infected dogs, because this activity could produce psychological impacts on veterinary medicals by the constant demands to eliminate healthy animals and are in face to moral stress, as pointed by Rollin [47].
The results reported here corroborate those of other studies conducted in Brazil, which also demonstrated the efficacy of the measure, with repercussions on both canine and human populations. In Teresina, Piauí, Werneck et al. [48] assessed the use of an insecticide and the culling of dogs and found that the latter had a significantly higher efficacy compared to the control group. The culling of 48% of the dogs was associated with a reduction in the prevalence of human disease 18 months later. In Jacobina, Bahia, Ashford et al. [12] found that after four years of euthanatizing all seropositive dogs, the canine seroprevalence decreased from 36 to 6% and the incidence of human disease was reduced from ten to two cases among children per year in the intervention area, whereas in the control area, the canine seroprevalence varied from 24 to 28%. In Araçatuba, São Paulo, a negative correlation was also found between the culling of seropositive dogs and the prevalence of human disease; in addition, the results showed that the incidence increased after the intervention was interrupted [17]. In four states in Northeastern Brazil, where the incidence of disease is high, the number of human cases also increased when the culling of dogs was discontinued [13].
According to Courternay et al. [14], euthanasia leads to a significant reduction in the proportion of infective dogs to almost zero, provided by using a diagnostic test with high sensitivity and by eliminate the animals immediately after the diagnosis. Similarly, the use of low-sensitivity serologic tests maintains active reservoirs in endemic areas, which does not reduce the levels of human infection [49]. According to Grimaldi et al. [50], the tests currently used in governmental campaigns, the sensitivity of the screening test is less than 50% among the asymptomatic animals and 98% among the symptomatic ones. In contrast, in a study by Laurenti et al. [51], the test sensitivity was significantly higher in both the asymptomatic and symptomatic animals (92.1 and 89.4%, respectively), and the combination of this test with another attained a sensitivity of 99.1%. In the present study, the sensitivity of the diagnostic test in the asymptomatic animals was simulated to be less than 50%; nevertheless, a significant reduction in the proportion of infective animals was detected after culling.
The application of a mathematical model formulated by Costa et al. [16] assessed the success of a control program involving the euthanasia of symptomatic dogs in areas with low transmission rates (canine seroprevalence = 3%) and in areas with high transmission rates (canine prevalence = 12%), in which both the asymptomatic and symptomatic dogs were euthanized. These data agree with the results of the present study regarding the program success in areas with a high number of dog cases.
In a study by Moreira et al. [52], euthanasia neither increased nor decreased the prevalence of canine disease. That study lasted for two years at a location where the prevalence of canine disease was 31% (Jequié, Bahía) and involved a rather rapid elimination of the seropositive animals up to 14 days after a serodiagnosis was established.
Conversely, although the euthanasia has been applied in Brazil for several years, the number of cases of the disease in the country increased, particularly in urban areas, meaning that this measure was not efficacious [21]. Using a mathematical model, Dye [27] found that euthanasia was the worst option to control disease and was associated with only a small reduction in the human disease prevalence. Moreno & Alvar [8] suggested that the incomplete coverage of seropositive dogs is one reason highlighting the lack of success of this measure. In the present study, the elimination of 70% of the seropositive dogs per year was an efficacious simulated measure, but seropositive dogs and humans still remain in the environment.
Some studies suggest that a significant reduction in the prevalence of canine cases may not occur because of the high dog population turnover rate [53], along with an increasingly younger and thus more disease-susceptible population [30] that can be rapidly infected with the parasite [27]. In towns where the euthanasia of dogs seropositive for VL is performed as a control measure, such as in Araçatuba, São Paulo, from 2002 to 2004, dog turnover occurred in 38.8% (202/521) of the households, and the mean age of dogs was seven months [30]. In another study, 44.5% of the dogs euthanized in 2004 were replaced [54]. In Panorama, São Paulo, 41.5% (496/1,194) of the canine population was two years old or younger, a reflection of the replacement because of compulsory euthanasia [55]. In the model in the present study, the animals that died from euthanasia or VL lethality were born susceptible because that population is constant; nonetheless, the disease prevalence decreased substantially after simulated euthanasia.
Some studies have reported that long delays between diagnosis and euthanasia impair the success of this control measure [40,3,8], partly because the confirmation test may occur in laboratories far from certain municipalities and because of the resistance of the population. This is observed in many large and small endemic municipalities of Brazil, presenting a difficult question to solve.
A euthanasia rate of 70% and a vaccination rate of 90% result in similar outcomes in the infected dogs and humans. However, in view of the implications associated with both measures—the negative features of culling dogs and the proportion of protected animals resulting from the vaccination—the latter method appears to the better option. In addition, it is important to consider the total cost of each measure. The number of animals that must be vaccinated based on the proportion of seronegative dogs is higher than the number that would require euthanasia, which is based on the proportion of seropositive dogs (around 25%). The financial costs of implementing vaccination can be high; however, euthanasia is associated with various disadvantages and difficulties, as previously discussed.
The present model was implemented according to data available in the literature, except for parameters related to the vectorial capacity, such as density of the vector per host and the rate of vectors becoming infected after biting infected hosts. These data are difficult to obtain due to sensitivity of the vector to environmental factors. As cited by EFSA and Cameron et al. [32,56], more information is needed about the sand fly population and their behavior. Thus, it was necessary to fit the parameters, based on the available data, to produce a model that represented the scenarios of VL endemic areas. However, although these parameters were identified as sensitive in the model, this fact does not negate the result’s validation, and it can be applied to regions with similar scenarios. This is the case in some municipalities of the West region of São Paulo State; the canine seroprevalence has reached 30% in Santa Mercedes [57], and in other areas of the country, such as Natal-RN, Cuiabá-MT, Jequié-BA, and Rondônia the seroprevalence was 32% [58], 22%[59], 31% [60], and 28% [61], respectively. In areas with smaller transmission rates, other control measures may produce different results, as observed by Costa et al. [16], who noted that the sensitive parameters related to the vector-dog contact could influence the results substantially.
For a VL control program to be successful, it is necessary to take into account both the efficacy and the feasibility of the measures applied and their acceptance by the targeted population. Based on the strategies simulated in the present study and the socio-economic structure in developing countries, the use of insecticide-impregnated dog collars appears to be the most viable option from an operational point of view. Although this strategy demands a high rate of coverage relative to the total canine population (asymptomatic and symptomatic animals) and replacement of the collars every six months, its advantages include acceptance by the targeted population, simple application at the home of the pet owner, no requirement for previous serologic testing, and efficacy in reducing the seroprevalence among dogs and humans. However, careful attention is required to observe the development of side effects and for replacing the lost or damaged collars.
The implementation of more than one control measure for zoonotic VL used together should present a good efficacy, however the use of only one measure is focused on easily and practicality in terms of instruction for employees, financial resources management, and on the feasibility of operating capacity. Thus, the suggestion of the comparison of scenarios measures applied of isolated form using theoretical studies contribute as a tool in the orientation for making decision by public institutions to prevent and control the disease.
For control measures to be effective, they must be applied on a continuous basis, as shown in our simulations. According to Camargo-Neves et al. [15], currently, the greatest problem in areas where VL is endemic in Brazil is the lack of continuity of preventive and control measures. Furthermore, longitudinal epidemiological and entomological observations during interventions are essential [56]. Hence, lower costs and fewer obstacles in the application of the strategy contribute to its better continuity.
In conclusion, we have developed a mathematical tool that compares different scenarios for implementation of available preventive measures for visceral leishmaniasis, taking into account the disease dynamics in dogs and humans, the distinct capacities of the vector to infect and to be infected by these hosts, the sensitivity of serologic tests, and vaccine and collar efficacies. This model can be applied to other endemic regions by using their epidemiologic data and their respective available prevention and control measures.
In summary, the measures evaluated in this study, when used at high coverage rates, showed significant reduction in number of infected humans (near zero) and also in the number of infected dogs. The use of insecticide-impregnated collars was found to be the optimal measure due to its advantages over the other measures; however, it does require an intense effort because a high coverage rate must be achieved relative to the total canine population. The theoretical exercise performed using simulated scenarios, with measures implemented at different coverage rates, was utilized to compare the capacity for decreasing the VL seroprevalence of humans and dogs. Hence, this data contributes to the aim of improving both public and animal health by elucidating the impact of using these measures on a large scale. Nevertheless, it is important to reinforce that the control of this zoonotic disease requires the cooperation of the population and public health authorities, with an integrated approach that includes education, animal welfare principles, vector control, and environment management.
Data Availability
All relevant data are within the paper.
Funding Statement
This work was supported by the National Council for Scientific and Technological Development - Brazil (CNPq, 142612/2010-3), the Coordination for the Improvement of Higher Education Personnel - Brazil (CAPES, Fellowship BEX 9803/11-4), and the São Paulo Research Foundation -Brazil (FAPESP, 2012/01442-4). The funders had role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1.Alvar J, Vélez ID, Bern C, Herrero M, Desjeux P, Cano J, et al. Leishmaniasis worldwide and global estimates of its incidence. PLoS One. 2012;7: e35671 10.1371/journal.pone.0035671 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Brasil M da S. LV—Casos confirmados Notificados no Brasil. In: SINAN—Sistema de Informação de Agravos de Notificação [Internet]. 2015. Available: http://dtr2004.saude.gov.br/sinanweb/tabnet/dh?sinannet/leishvi/bases/leishvbrnet.def
- 3.Dantas-Torres F, Brandão-Filho SP. Visceral leishmaniasis in Brazil: revisiting paradigms of epidemiology and control. Rev Inst Med Trop Sao Paulo. 2006;48: 151–6. /S0036-46652006000300007 [DOI] [PubMed] [Google Scholar]
- 4.Quinnell RJ, Courtenay O. Transmission, reservoir hosts and control of zoonotic visceral leishmaniasis. Parasitology. 2009;136: 1915–34. 10.1017/S0031182009991156 [DOI] [PubMed] [Google Scholar]
- 5.Badaro R, Jones TC, Carvalho EM, Sampaio D, Reed SG, Barral a, et al. New perspectives on a subclinical form of visceral leishmaniasis. J Infect Dis. 1986;154: 1003–11. Available: http://www.ncbi.nlm.nih.gov/pubmed/3782864 [DOI] [PubMed] [Google Scholar]
- 6.Costa CHN, Gomes RBB, Silva MRB, Garcez LM, Ramos PKS, Santos RS, et al. Competence of the Human Host as a Reservoir for Leishmania chagasi. Cultures. 2000;182: 997–1000. [DOI] [PubMed] [Google Scholar]
- 7.Costa JML. Epidemiologia das Leishmanioses no Brasil. Gaz Médica da Bahia. 2005;75: 3–17. Available: http://www.gmbahia.ufba.br/index.php/gmbahia/article/viewFile/346/335 [Google Scholar]
- 8.Moreno J, Alvar J. Canine leishmaniasis: epidemiological risk and the experimental model. Trends Parasitol. 2002;18: 399–405. Available: http://www.ncbi.nlm.nih.gov/pubmed/12377257 [DOI] [PubMed] [Google Scholar]
- 9.Grégory M, Pomares C, Ferrua B, Marty P. Importance of worldwide asymptomatic carriers of Leishmania infantum (L. chagasi) in human. Acta Trop. 2011;119: 69–75. 10.1016/j.actatropica.2011.05.012 [DOI] [PubMed] [Google Scholar]
- 10.Ministério da Saúde. LEISHMANIOSE VISCERAL—Manual de Vigilância e Controle. Departamento de Vigilância Epidemiológica, Secretaria de Vigilância em Saúde; 2006: 122. [Google Scholar]
- 11.Paranhos-Silva M, Freitas LAR, Santos WC, Grimaldi G Jr, Pontes-de-Carvalho LC, Oliveira-dos-Santos AJ. A cross-sectional serodiagnostic survey of canine leishmaniasis due to Leishmania Chagasi. Am J Trop Med Hyg. 1996;55: 39–44. [DOI] [PubMed] [Google Scholar]
- 12.Ashford D a, David JR, Freire M, David R, Sherlock I, Eulálio MC, et al. Studies on control of visceral leishmaniasis: impact of dog control on canine and human visceral leishmaniasis in Jacobina, Bahia, Brazil. Am J Trop Med Hyg. 1998;59: 53–7. Available: http://www.ncbi.nlm.nih.gov/pubmed/9684628 [DOI] [PubMed] [Google Scholar]
- 13.Palatnik-de-Sousa CB, dos Santos WR, França-Silva JC, da Costa RT, Reis a B, Palatnik M, et al. Impact of canine control on the epidemiology of canine and human visceral leishmaniasis in Brazil. Am J Trop Med Hyg. 2001;65: 510–7. Available: http://www.ncbi.nlm.nih.gov/pubmed/11716106 [DOI] [PubMed] [Google Scholar]
- 14.Courtenay O, Quinnell RJ, Garcez LM, Shaw JJ, Dye C. Infectiousness in a cohort of brazilian dogs: why culling fails to control visceral leishmaniasis in areas of high transmission. J Infect Dis. 2002;186: 1314–20. 10.1086/344312 [DOI] [PubMed] [Google Scholar]
- 15.De Camargo-neves VLF, Rodas LAC, Pauliquévis C Junior. Avaliação da efetividade da utilização das coleiras impregnadas com deltametrina a 4% para o controle da leishmaniose visceral americana no Estado de São Paulo. Bol Epidemiológico Paul. 2004;12: 7–14. [Google Scholar]
- 16.Costa DNCC, Codeço CT, Silva M a, Werneck GL. Culling dogs in scenarios of imperfect control: realistic impact on the prevalence of canine visceral leishmaniasis. PLoS Negl Trop Dis. 2013;7: e2355 10.1371/journal.pntd.0002355 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nunes CM, Pires MM, da Silva KM, Assis FD, Gonçalves Filho J, Perri SHV. Relationship between dog culling and incidence of human visceral leishmaniasis in an endemic area. Vet Parasitol. 2010;170: 131–3. 10.1016/j.vetpar.2010.01.044 [DOI] [PubMed] [Google Scholar]
- 18.Tesh RB. Control of zoonotic visceral leishmaniasis: Is it time to change strategies? American Journal of Tropical Medicine and Hygiene. 1995. pp. 287–292. [DOI] [PubMed] [Google Scholar]
- 19.Vieira JBF, Coelho GE. Leishmaniose visceral ou calazar: aspectos epidemiológicos e de controle. Rev Soc Bras Med Trop. 1998;31: 85–92. [PubMed] [Google Scholar]
- 20.Akhavan D. Análise de custo-efetividade do componente de leishmaniose no projeto de controle de doenças endêmicas no nordeste do Brasil. Rev Patol Trop. 1996;25: 203–252. [Google Scholar]
- 21.Costa CHN, Vieira JB. Mudanças no controle da leishmaniose visceral no Brasil. Rev Soc Bras Med Trop. 2001;34: 223–228. [DOI] [PubMed] [Google Scholar]
- 22.Killick-Kendrick R, Killick-Kendrick M, Focheux C, Dereure J, Puech MP, Cadiergues MC. Protection of dogs from bites of phlebotomine sandflies by deltamethrin collars for control of canine leishmaniasis. Med Vet Entomol. 1997;11: 105–111. 10.1111/j.1365-2915.1997.tb00298.x [DOI] [PubMed] [Google Scholar]
- 23.David JR, Stamm LM, Bezerra HS, Souza RN, Killick-Kendrick R, Lima JW. Deltamethrin-impregnated dog collars have a potent anti-feeding and insecticidal effect on Lutzomyia longipalpis and Lutzomyia migonei. Mem Inst Oswaldo Cruz. 2001;96: 839–47. Available: http://www.ncbi.nlm.nih.gov/pubmed/11562713 [DOI] [PubMed] [Google Scholar]
- 24.Gavgani ASM, Hodjati MH, Mohite H, Davies CR. Effect of insecticide-impregnated dog collars on incidence of zoonotic visceral leishmaniasis in Iranian children: a matched-cluster randomised trial. Lancet. 2002;360: 374–9. Available: http://www.ncbi.nlm.nih.gov/pubmed/12241778 [DOI] [PubMed] [Google Scholar]
- 25.Reithinger R, Coleman PG, Alexander B, Vieira EP, Assis G, Davies CR. Are insecticide-impregnated dog collars a feasible alternative to dog culling as a strategy for controlling canine visceral leishmaniasis in Brazil? Int J Parasitol. 2004;34: 55–62. Available: http://linkinghub.elsevier.com/retrieve/pii/S0020751903002881 [DOI] [PubMed] [Google Scholar]
- 26.Fernandes AP, Coelho EAF, Machado-Coelho GLL, Grimaldi G, Gazzinelli RT. Making an anti-amastigote vaccine for visceral leishmaniasis: Rational, update and perspectives. Curr Opin Microbiol. Elsevier Ltd; 2012;15: 476–485. 10.1016/j.mib.2012.05.002 [DOI] [PubMed] [Google Scholar]
- 27.Dye C. The logic of visceral leishmaniasis control. Am J Trop Med Hyg. 1996;55: 125–30. Available: http://www.ncbi.nlm.nih.gov/pubmed/8780448 [DOI] [PubMed] [Google Scholar]
- 28.Luz PM, Struchiner CJ, Galvani AP. Modeling transmission dynamics and control of vector-borne neglected tropical diseases. PLoS Negl Trop Dis. 2010;4: e761 10.1371/journal.pntd.0000761 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Burattini MN, Coutinho FAB, Lopez LF, Massad E. Modelling the dynamics of leishmaniasis considering human, animal host and vector populations. J Biol Syst. 1998;6: 337–356. 10.1142/S0218339098000224 [DOI] [Google Scholar]
- 30.Nunes CM, De Lima VMF, De Paula HB, Perri SHV, De Andrade AM, Dias FEF, et al. Dog culling and replacement in an area endemic for visceral leishmaniasis in Brazil. Vet Parasitol. 2008;153: 19–23. 10.1016/j.vetpar.2008.01.005 [DOI] [PubMed] [Google Scholar]
- 31.Oliveira-Lima JW, de Souza RN, Teixeira Maria Jania, Pompeu M, Killick-Kendrick R, David JR. Preliminary results of a field trial to evaluate deltamethrin-impregnated collars for the control of canine leishmaniasis in northeast Brazil. Canine leishmaniasis: Moving towards a solution. 2002: 7–14. [Google Scholar]
- 32.EFSA. Scientific Opinion on canine leishmaniosis. EFSA J. 2015;13: 1–77. 10.2903/j.efsa.2015.4075 [DOI] [Google Scholar]
- 33.Maroli M, Mizzoni V, Siragusa C, D’Orazi A, Gradoni L. Evidence for an impact on the incidence of canine leishmaniasis by the mass use of deltamethrin-impregnated dog collars in southern Italy. Med Vet Entomol. 2001;15: 358–363. 10.1046/j.0269-283x.2001.00321.x [DOI] [PubMed] [Google Scholar]
- 34.Ferroglio E, Poggi M, Trisciuoglio a. Evaluation of 65% permethrin spot-on and deltamethrin-impregnated collars for canine Leishmania infantum infection prevention. Zoonoses Public Health. 2008;55: 145–8. 10.1111/j.1863-2378.2007.01092.x [DOI] [PubMed] [Google Scholar]
- 35.Yang HM. Epidemiologia Matemática: estudos dos efeitos da vacinação em doenças de trasmissão direta. 1st ed UNICAMP, editor. Campinas; 2001. [Google Scholar]
- 36.Foroughi-Parvar F, Hatam G. Vaccines for canine leishmaniasis. Adv Prev Med. 2014; 1–9. 10.1155/2014/569193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Gradoni L. Canine Leishmania vaccines: Still a long way to go. Vet Parasitol. Elsevier B.V.; 2015;208: 94–100. 10.1016/j.vetpar.2015.01.003 [DOI] [PubMed] [Google Scholar]
- 38.Reis AB, Giunchetti RC, Carrillo E, Martins-Filho O a, Moreno J. Immunity to Leishmania and the rational search for vaccines against canine leishmaniasis. Trends Parasitol. 2010;26: 341–9. 10.1016/j.pt.2010.04.005 [DOI] [PubMed] [Google Scholar]
- 39.Palatnik-de-Sousa CB, Silva-Antunes I, Morgado ADA, Menz I, Palatnik M, Lavor C. Decrease of the incidence of human and canine visceral leishmaniasis after dog vaccination with Leishmune in Brazilian endemic areas. Vaccine. 2009;27: 3505–12. 10.1016/j.vaccine.2009.03.045 [DOI] [PubMed] [Google Scholar]
- 40.Fernandes CB, Junior JTM, De Jesus C, Da Silva Souza BMP, Larangeira DF, Fraga DBM, et al. Comparison of two commercial vaccines against visceral leishmaniasis in dogs from endemic areas: IgG, and subclasses, parasitism, and parasite transmission by xenodiagnosis. Vaccine. Elsevier Ltd; 2014;32: 1287–1295. 10.1016/j.vaccine.2013.12.046 [DOI] [PubMed] [Google Scholar]
- 41.Marzochi MCDA, Fagundes A, De Andrade MV, de Souza MB, Madeira Ma de F, Mouta-Confort E, et al. Visceral leishmaniasis in Rio de Janeiro, Brazil: eco-epidemiological aspects and control. Rev Soc Bras Med Trop. 2009;42: 570–580. [DOI] [PubMed] [Google Scholar]
- 42.Queiroz MJ a, Alves JGB, Correia JB. Visceral leishmaniasis: clinical and epidemiological features of children in an endemic area. J Pediatr (Rio J). 2004;80: 141–6. Available: http://www.ncbi.nlm.nih.gov/pubmed/15079185 [PubMed] [Google Scholar]
- 43.Werneck GL, Costa CHN, Walker AM, David JR, Wand M, Maguire JH. Multilevel modelling of the incidence of visceral leishmaniasis in Teresina, Brazil. Cad Saude Pública. 2007;135: 195–201. 10.1017/S0950268806006881 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Werneck GL, Maguire JH. Spatial modeling using mixed models: an ecologic study of visceral leishmaniasis in Teresina, Piauí State, Brazil. Cad Saude Publica. 2002;18: 633–637. 10.1590/S0102-311X2002000300012 [DOI] [PubMed] [Google Scholar]
- 45.Martinez E, Cesario C, Silva IDE, Boere V. Domestic dogs in rural area of fragmented Atlantic Forest: potential threats to wild animals. Cienc Rural. 2013;43: 1998–2003. 10.1590/S0103-84782013001100013 [DOI] [Google Scholar]
- 46.Coura-Vital W, Marques MJ, Veloso VM, Roatt BM, Aguiar-Soares RDDO, Reis LES, et al. Prevalence and factors associated with Leishmania infantum infection of dogs from an urban area of Brazil as identified by molecular methods. PLoS Negl Trop Dis. 2011;5: e1291 10.1371/journal.pntd.0001291 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Rollin BE. Euthanasia, moral stress, and chronic Illness in veterinary medicine. Vet Clin North Am—Small Anim Pract. Elsevier Ltd; 2011;41: 651–659. 10.1016/j.cvsm.2011.03.005 [DOI] [PubMed] [Google Scholar]
- 48.Werneck GL, Costa CHN, de Carvalho FAA, Pires e Cruz MDS, Maguire JH, Castro MC. Effectiveness of Insecticide Spraying and Culling of Dogs on the Incidence of Leishmania infantum Infection in Humans: A Cluster Randomized Trial in Teresina, Brazil. PLoS Negl Trop Dis. 2014;8: e3172 10.1371/journal.pntd.0003172 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Braga MDM, Coelho ICB, Pompeu MML, Evans TG, MacAullife IT, Teixeira MJ, et al. Controle do calazar canino: comparação dos resultados de um programa de eliminação rápida de cães sororreagentes por ensaio imuno-enzimático com outro de eliminação tardia de cães sororreagentes por teste de imunofluorescência indireta de eluato de papel. Rev Soc Bras Med Trop. 1998;31: 419–424. [DOI] [PubMed] [Google Scholar]
- 50.Grimaldi G, Teva A, Ferreira AL, dos Santos CB, Pinto I de-S, de-Azevedo CT, et al. Evaluation of a novel chromatographic immunoassay based on Dual-Path Platform technology (DPP® CVL rapid test) for the serodiagnosis of canine visceral leishmaniasis. Trans R Soc Trop Med Hyg. Royal Society of Tropical Medicine and Hygiene; 2012;106: 54–9. 10.1016/j.trstmh.2011.10.001 [DOI] [PubMed] [Google Scholar]
- 51.Laurenti MD, Leandro MVDS, Tomokane TY, De Lucca HRL, Aschar M, Souza CSF, et al. Comparative evaluation of the DPP® CVL rapid test for canine serodiagnosis in area of visceral leishmaniasis. Vet Parasitol. Elsevier B.V.; 2014;205: 444–450. [DOI] [PubMed] [Google Scholar]
- 52.Moreira ED, Mendes De Souza VM, Sreenivasan M, Nascimento EG, Pontes De Carvalho L. Assessment of an optimized dog-culling program in the dynamics of canine Leishmania transmission. Vet Parasitol. 2004;122: 245–52. 10.1016/j.vetpar.2004.05.019 [DOI] [PubMed] [Google Scholar]
- 53.De Camargo-Neves VLF, Aparecida L, Rodas C, Poletto DW, Maria R, Spínola F, et al. Utilização de ferramentas de análise espacial na vigilância epidemiológica de leishmaniose visceral americana—Araçatuba, São Paulo, Use of spatial analysis tools in the epidemiological surveillance of American visceral leishmaniasis. Cad Saude Pública. 2001;17: 1263–1267. [DOI] [PubMed] [Google Scholar]
- 54.Andrade AM, Queiroz LH, Nunes GR, Helena S, Perri V, Nunes M. Reposição de cães em área endêmica para leishmaniose visceral Dog replacement in an area endemic for visceral leishmaniasis. Rev Soc Bras Med Trop. 2007;40: 594–595. [DOI] [PubMed] [Google Scholar]
- 55.Bortoletto DV. Influencia da esterilização cirurgica na população canina de área endêmica para Leishmaniose Visceral. Universidade Estadual Paulista "Julio de Mesquita Filho, Araçatuba: 2011. [Google Scholar]
- 56.Cameron MM, Acosta-Serrano A, Bern C, Boelaert M, den Boer M, Burza S, et al. Understanding the transmission dynamics of Leishmania donovani to provide robust evidence for interventions to eliminate visceral leishmaniasis in Bihar, India. Parasit Vectors. Parasites & Vectors; 2016;9: 25 10.1186/s13071-016-1309-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Laz D, De Camargo-neves VLF, Sampaio S, Kronka S, Sartor I. American Visceral Leishmaniasis: Disease control strategies in Dracena Macroregion in Alta Paulista, SP, Brasil. J Venom Anim Toxins Incl Trop Dis. 2009;15: 305–324. [Google Scholar]
- 58.Lima ID, Queiroz JW, Lacerda HG, Queiroz PVS, Pontes NN, Barbosa JDA, et al. Leishmania infantum chagasi in Northeastern Brazil: Asymptomatic Infection at the Urban Perimeter. Trop Med. 2012;86: 99–107. 10.4269/ajtmh.2012.10-0492 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.de Almeida ADBPF, Sousa VRF, da Cruz FACS, Dahroug MAA, Figueiredo FB, Madeira MDF. Canine visceral leishmaniasis: seroprevalence and risk factors in Cuiabá, Mato Grosso, Brazil. Rev Bras Parasitol Vet. 2012;21: 359–65. Available: http://www.ncbi.nlm.nih.gov/pubmed/23184322 [DOI] [PubMed] [Google Scholar]
- 60.Moreira ED, de Souza VMM, Sreenivasan M, Lopes NL, Barreto RB, de Carvalho LP. Peridomestic risk factors for canine leishmaniasis in urban dwellings: new findings from a prospective study in Brazil. Am J Trop Med Hyg. 2003;69: 393–7. Available: http://www.ncbi.nlm.nih.gov/pubmed/14640499 [PubMed] [Google Scholar]
- 61.Aguiar, Daniel M, Oliveira TMF de S, Cavalcante GT, Labruna MB, Camargo LMA, Machado RZ, et al. Seroprevalence of anti-Leishmania spp. antibodies in rural dogs from the city of Monte Negro, State of Rondônia, Brazil. Rev Bras Parasitol Vet. 2010;19: 71–72. [DOI] [PubMed] [Google Scholar]
- 62.IBGE. Brasil—Tabua completa de mortalidade—Ambos os sexos—2011. In: Instituto Brasileiro de Geografia e Estatística [Internet]. 2011 pp. 0–1. Available: ftp://ftp.ibge.gov.br/Tabuas_Completas_de_Mortalidade/Tabuas_Completas_de_Mortalidade_2011/pdf/ambos_pdf.pdf
- 63.Ovallos FG. Estudo da capacidade vetorial de Mogonemyia migonei (Françca) e de Pintomyia ficheri (Pinto) (Diptera: Psychodidae) para Leishmania (Leishmania) infantum chagasi Cunha e Chagas. Universidade de São Paulo; 2011. [Google Scholar]
- 64.Maia C, Nunes M, Cristóvão J, Campino L. Experimental canine leishmaniasis: clinical, parasitological and serological follow-up. Acta Trop. Elsevier B.V.; 2010;116: 193–9. 10.1016/j.actatropica.2010.08.001 [DOI] [PubMed] [Google Scholar]
- 65.Carvalho EM, Barral A, Pedral-Sampaio D, Barral-Netto M, Badaró R, Rocha H, et al. Immunologic markers of clinical evolution in children recently infected with Leishmania donovani chagasi. J Infect Dis. 1992;165: 535–40. Available: http://www.ncbi.nlm.nih.gov/pubmed/1347057 [DOI] [PubMed] [Google Scholar]
- 66.Silva L de A, Romero HD, Prata A, Costa RT, Nascimento E, Carvalho SFG, et al. Immunologic tests in patients after clinical cure of visceral leishmaniasis. Am J Trop Med Hyg. 2006;75: 739–43. Available: http://www.ncbi.nlm.nih.gov/pubmed/17038704 [PubMed] [Google Scholar]
- 67.Silveira FT, Lainson R, Crescente JA, de Souza A a a, Campos MB, Gomes CMC, et al. A prospective study on the dynamics of the clinical and immunological evolution of human Leishmania (L.) infantum chagasi infection in the Brazilian Amazon region. Trans R Soc Trop Med Hyg. 2010;104: 529–35. 10.1016/j.trstmh.2010.05.002 [DOI] [PubMed] [Google Scholar]
- 68.De Oliveira JM, Fernandes AC, Elizabeth M, Dorval C, Alves TP. Mortalidade por leishmaniose visceral: aspectos clínicos e laboratoriais. Rev Soc Bras Med Trop. 2010;43: 188–193. [DOI] [PubMed] [Google Scholar]
- 69.Alvar J. Las leishmaniasis: de la biología al control [Internet]. 2a. edição Intervet L, editor. Salamanca; 2001. Available: http://pt.scribd.com/doc/57033625/LIBRO-LEISHMAN [Google Scholar]
- 70.Bentubo HDL, Tomaz MA, Bondan EF, Lallo MA. Expectativa de vida e causas de morte em cães na área metropolitana de São Paulo (Brasil). Ciência Rural. 2007;37: 1021–1026. 10.1590/S0103-84782007000400016 [DOI] [Google Scholar]
- 71.Pozio E, Gradoni L, Bettini M, Gramiccia M. Leishmaniasis in Tuscny (Italy): VI. Canine leishmaniasis in the focus of Monte Argentario (Grosseto). Acta Trop. 1981;38: 383–393. [PubMed] [Google Scholar]
- 72.Garcia AM, Rebelo JMM, Caldas A, Gomes R, Vinhas V, Barral A, et al. História natural da infecção causada por Leishmania chagasi em cães (Canis familiaris) domiciliados em área endêmica da Ilha de São Luis—Maranhão, Brasil. Gaz Médica da Bahia. 2009;79: 147–155. [Google Scholar]
- 73.Fisa R, Gállego M, Castillejo S, Aisa MJ, Serra T, Riera C, et al. Epidemiology of canine leishmaniosis in Catalonia (Spain) the example of the Priorat focus. Vet Parasitol. 1999;83: 87–97. Available: http://www.ncbi.nlm.nih.gov/pubmed/10392965 [DOI] [PubMed] [Google Scholar]
- 74.Silva FS. Patologia e patogênese da leishmaniose visceral canina Pathology and pathogenesis of canine visceral leishmaniasis. Rev Trópica—Ciências Agrárias e Biológicas. 2007;1: 20–31. [Google Scholar]
- 75.Rogers ME, Bates P a. Leishmania manipulation of sand fly feeding behavior results in enhanced transmission. PLoS Pathog. 2007;3: e91 10.1371/journal.ppat.0030091 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Kamhawi S. Phlebotomine sand flies and Leishmania parasites: friends or foes? Trends Parasitol. 2006;22: 439–45. 10.1016/j.pt.2006.06.012 [DOI] [PubMed] [Google Scholar]
- 77.Costa CHN, Parente DM, Zacarias DA, Pereira HF, De Mendonça IL, Da Silva LV, et al. Infectivity of symptomatic and asymptomatic, non-HIV and HIV/Leishmania infatum infected, patients to Lutzomyia longipalpis Fifth World Congress on Leishmaniasis—Abstract Book. Porto de Galinhas, Pernambuco, Brazil; 2013. p. 1116. [Google Scholar]
- 78.Laurenti MD, Rossi CN, Da Matta VLR, Tomokane TY, Corbett CEP, Secundino NFC, et al. Asymptomatic dogs are highly competent to transmit Leishmania (Leishmania) infantum chagasi to the natural vector. Vet Parasitol. Elsevier B.V.; 2013; 10.1016/j.vetpar.2013.03.017 [DOI] [PubMed] [Google Scholar]
- 79.Hermont VJ. Leishtec, Manual Técnico—Leishmaniose Visceral Canina [Internet]. 2008. Available: http://www.google.com.br/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CCoQFjAA&url=http://www.hertapecalier.com.br/empresa/pecas.php?campanha=105&ei=PnifUr7lAofOkQeKlIBQ&usg=AFQjCNGEGuJi7rb2GMHP9-NG3YIMMiaUBg&sig2=lgOIiAdxTTtoGFo5E-SVRQ&bvm
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All relevant data are within the paper.