

Abstract
[Purpose] This study compared the effects of pilates and an exercise program on the craniovertebral angle, cervical range of motion, pain, and muscle fatigue in subjects with a forward head posture (FHP). [Subjects and Methods] A total of 28 sedentary females (age 20 to 39 years) with FHP were randomly assigned to pilates (n=14) and combined (n=14) exercise groups. The study was a randomized, controlled, double-blind study with the two groups performing exercise 50 min/day, 3 days/week, with an intensity of 11–15 rating of perceived exertion (RPE) for ten weeks. The main outcome measures were craniovertebral angle, cervical range of motion (ROM), pain levels assessed by visual analog scale (VAS), and neck disability index (NDI). Surface electromyography was also used to measure muscle fatigue. [Results] There were significant increases in craniovertebral angle and cervical ROM in the pilates group, but none in the control group. The only significant differences in muscle activity were recorded in the sternocleidomastoid muscle in the pilates group. Both exercise programs had positive effects on pain measures, as VAS and NDI were significantly decreased. [Conclusion] The results suggest that pilates could be recommended as an appropriate exercise for treatment of FHP in sedentary individuals.
Key words: Forward head posture, Pilates, Exercise
INTRODUCTION
The increasing use of electronic screens, such as smart phones and personal computers, to an average of about 8 hours per day1), has led to an increasing number of people with forward head posture (FHP). FHP is defined as the anterior positioning of the cervical spine1) and is associated with muscle imbalance, pain, fatigue, and limited motion of the cervical spine2). FHP may cause herniated cervical intervertebral discs and other adverse effects, such as chronic low back pain and temporomandibular disorder3).
The craniovertebral angle (CVA) is defined as the angle of the horizontal line running through the C7 spinous process and the line connecting the C7 spinous process to the tragus of the ear. Yip et al.4) reported that participants with significantly smaller craniovertebral angles had FHP and tended to have increased levels of neck pain. Similarly, Sohn and associates5) showed that participants with smaller craniovertebral angles tended to have more tension-type headaches, and lower cervical range of motion. Szeto et al.6) reported a higher frequency of neck and shoulder pain in individuals who spent long periods using computers. Previous research7,8,9) suggests that weakened postural muscles should be strengthened and shortened muscles should be lengthened in order to improve postural alignment and alleviate FHP.
A variety of therapeutic exercises designed to mitigate the symptoms of FHP have been examined4, 10). The majority of treatments have focused on the deep neck flexors, as they play a major role in stabilizing the alignment of the cervical spine11). However, one drawback of focusing on this alignment alone is that the treatment focuses on the symptom and not the reasons why the misalignment has developed. FHP may develop due to genetic and behavioral reasons, such as reading from a sitting position with reading material on a horizontal surface; i.e. looking down at a desk. Individuals may not be aware of their bad posture and thus remain in this straining posture for prolonged periods.
Pilates training is designed to improve general body flexibility and health by emphasizing core strength, posture, and coordination of breathing with movement12). It improves posture by enhancing body awareness13) and can be used as self-exercise, and can be easily tailored for treatment of specific postural misalignments. Based on Kuo et al.13) report that pilates can improve thoracic kyphosis in older adults, we infer that pilates may improve cervical spine health by increasing the craniovertebral angle. Therefore, this study compares the effects of pilates and combined stretching and strengthening exercise programs on CVA, cervical range of motion (ROM), neck and shoulder pain, and muscle fatigue in individuals with FHP. We hypothesize that pilates may be an effective exercise method for alleviating FHP.
SUBJECTS AND METHODS
After the study was approved by the Institutional Review Board of Pusan National University Medical Center (05-2011-038), informed consent was obtained from each participant. Participants were screened primarily on the severity of FHP (when the tragus was in front of the center of shoulder; Fig. 1), and secondarily via e-mail questionnaire to exclude any spinal problems, pain or dysfunction or a visual analogue pain score above 3 of the neck and shoulder region, temporomandibular disease, as well as any other confounding health problems. Additionally any participants with experience in pilates and who were not sedentary were excluded from the study. A total of twenty-eight sedentary females (demographics shown in Table 1) with FHP, between 23 and 39 years of age, were enrolled and randomly assigned into a pilates (PG, n=14) or combined (CG, n=14) exercise groups. All participants were unaware of the exact exercise type until the end of testing period. The pilates and combined exercise instructors were placed in their respective areas and were blinded to the study purpose.
Fig. 1.
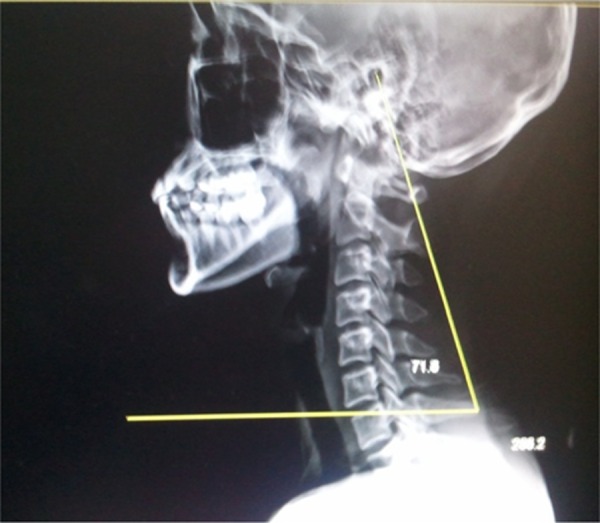
Craniovertebral angle measurement
Table 1. Participant demographic characteristics.
| Characteristics | Pilates group | Control group |
|---|---|---|
| No. of subjects | 14 | 14 |
| Age (yrs) | 29.2 ± 4.3 | 28.9 ± 5.0 |
| Height (cm) | 162.0 ± 6.9 | 162.6 ± 5.2 |
| Weight (kg) | 57.2 ± 7.4 | 55.2 ± 8.7 |
Data are presented as means ± SD.
Both groups exercised for 50 minutes a day, three days a week at an intensity of 11–15 rating of perceived exertion (RPE), with added load each week for ten weeks. The Pilates exercise program consisted of modern pilates that focused on balancing FHP-related major muscle group-stretching of the neck extensors and pectoral muscles and strengthening of the deep neck flexors, shoulder retractors, back, and abdominal muscles with co-activation of the core muscles by focusing on breathing technique10). We used thera-bands to more effectively strengthen the muscles. If any motion caused pain during exercise, the participant was instructed to rest until the pain subsided. The combined exercise program consisted of stretching and strengthening exercises typically used to balance posture14). This exercise also focused on balancing the FHP-related major muscle groups, although without co-activation of the core muscles. Thera-bands were also used to strengthen muscles. All sessions were supervised by either pilates or exercise instructors.
After receiving an oral explanation and reviewing the institutional review board’s informed consent form, the participants underwent screening for FHP. FHP was determined by measuring the CVA15) from a sagittal plane x-ray (Fig. 1). To maximize compliance, participants were instructed to report after work to the hospital to participate. Initial testing was conducted after participant screening and selection. Prior to their participation in the treatment programs, cervical flexion, extension, lateral flexion, and rotation were tested using CROM (Performance Attainment Associates, MN, USA), which was specially designed to measure cervical ROM. All cervical ROM assessments were performed starting at a natural head posture and explained with demonstrations. After performing each exercise three times, the average value was recorded. The visual analogue scale (VAS), a simple, sensitive, and highly reproducible method for measuring pain16), was assessed before and after treatment. Likewise, the neck disability index questionnaire (NDI), a widely used questionnaire that determines how neck pain affects daily life17), was also completed before and after treatment. Electromyography (Telemyo 2400t G2, NORAXON, USA) measurements of the right-side muscles known to have excessive fatigue and affect FHP; i.e., the upper trapezius, sternocleidomastoid (SCM), and C4 paraspinals, were recorded at 1,500 Hz before and after the ten-week treatments10, 18). To obtain each muscle fatigue measurement, the reference voluntary contraction (RVC) values for three seconds in the sitting position were measured.
Noraxon was used to record, analyze, and calculate electromyography-related data. The median frequency (MDF) was calculated as an index of muscle fatigue, with lower median frequency corresponding to increased muscle fatigue. Statistical analyses were performed using PASW Statistics for Windows, version 18.0, and p<0.05 were considered statistically significant differences. To test for the homogeneity of each group, an independent t-test was used before intervention. To verify the interaction between the groups and periods, we used split-plot one-way repeated measures analysis of variance (ANOVA). In addition, post hoc tests were used to analyze the significant differences between each factor in the group before and after intervention.
RESULTS
Descriptive statistics for the two groups and the pre- and post-treatment measurements are shown in Table 2. Two participants in the pilates group dropped out for unknown reasons. Thus, a total of 12 participants were analyzed in the pilates group. There were no statistical differences between the pre-treatment descriptive characteristics and variables of the study participants. There was significant improvement in CVA in the pilates group between the pre- (65.65 ± 4.53°) and post-treatment (70.09 ± 4.78°) measurements (p=0.002). However, there was no significant improvement in the combined exercise group (69.08 ± 2.40°, 69.13 ± 3.19°). Among cervical ROM measurements, there were significant changes in flexion (p=0.017) and right rotation (p=0.034) in the pilates group, but no significant differences in these measurements in the combined exercise group. Similarly, there were significant improvements in extension (p=0.037), right lateral flexion (p=0.006), right rotation (p=0.045), and left rotation (p=0.033) in the pilates group, but not in the combined exercise group. There were no significant differences in VAS between groups. Pain decreased significantly in both the pilates (p<0.001) and combined exercise groups (p<0.0001) after intervention. Likewise, there were no significant changes between groups in NDI (p<0.001 for both), which decreased significantly after intervention. The only significant difference between the Pilates and combined exercise groups in median EMG frequency data was for the SCM (p=0.026).
Table 2. Pre- and post-intervention outcome measures between Pilates and control groups.
| Outcome measures | Pilates | Control | ||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| Craniovertebral angle (°) | 65.6 ± 4.5 | 70.1 ± 4.8** | 69.1 ± 2.4 | 69.1 ± 3.2 |
| Flexion rom (°) | 35.1 ± 6.3 | 46.6 ± 8.8** | 41.6 ± 6.1 | 44.0 ± 6.6 |
| Extension rom (°) | 50.1 ± 11.7 | 57.1 ± 9.3* | 48.5 ± 9.5 | 52.6 ± 7.9 |
| Right side flexion rom (°) | 29.5 ± 3.1 | 34.0 ± 3.8** | 29.6 ± 4.1 | 30.9 ± 4.5 |
| Left side flexion rom (°) | 33.9 ± 5.5 | 36.6 ± 4.6 | 32.1 ± 3.6 | 33.6 ± 4.5 |
| Right rotation rom (°) | 51.5 ± 10.6 | 57.8 ± 5.8* | 54.6 ± 9.1 | 53.3 ± 6.6 |
| Left rotation rom (°) | 52.1 ± 10.1 | 57.2 ± 6.7* | 51.9 ± 8.1 | 55.1 ± 4.6 |
| Vas pain scale | 5.9 ± 1.6 | 2.5 ± 1.5*** | 5.4 ± 1.7 | 2.7 ± 1.8*** |
| Neck disability index | 10.4 ± 3.5 | 5.1 ± 2.1*** | 10.7 ± 3.2 | 5.9 ± 3.4*** |
| Emg data upper trapezius | 41.9 ± 15.6 | 41.3 ± 13.6 | 43.3 ± 21.9 | 27.8 ± 9.5 |
| Emg data scm | 27.3 ± 11.3 | 43.5 ± 17.29** | 49.2 ± 17.6 | 45.2 ± 19.0 |
| Emg data cervical paraspinals | 34.9 ± 13.3 | 42.5 ± 20.2 | 39.9 ± 19.3 | 38.8 ± 25.1 |
Data are presented as means ± SD. *p<0.05, **p<0.01, ***p<0.001 between pre and post measurement.
DISCUSSION
CVA is commonly used as an indicator of FHP, which is due to muscle imbalance, related to pain, fatigue, and limited motion of the cervical spine2, 18, 19). Increased CVA improves FHP, which suggests the potential to mitigate the FHP problem. In this study, Pilates, and not combined exercises, resulted in significantly increased CVA. The Pilates treatment program appeared to significantly improve head posture in participants with FHP. In a similar study, Emery et al.20) reported that a 12-week pilates training program strengthened core muscles and improved thoracic kyphosis. Kuo and associates13) similarly illustrated that even a ten-week pilates training program in individuals aged above 60 years could slightly reduce thoracic kyphosis angle. Additionally, Parrott21) reported that a 14-week pilates exercise program improved standing alignment. FHP in a standing posture is linked with a lack of control of the abdominal muscles, which aggravates thoracic kyphosis, making it more difficult to hold the head sufficiently high to maintain normal eye level22). Based on the results of these previous studies, any improvement in thoracic kyphosis is closely related to an improvement in FHP. Therefore, it seems likely that pilates training, which helps spinal realignment, may improve FHP. The pilates program in this study focused on improving systematic balances rather than specific (cervical or thoracic) regions, which emphasizes core stability and spinal separation. Furthermore, the additional benefits of pilates exercises include decreased hypertension in shortened and weakened muscles during exercise7); improved breathing methods (diaphragmatic and rib breathing) that improve core stability; and increased awareness of postural misalignments. The results of this study indicate that pilates training results in whole-body muscle retraining, which strengthens the deep neck muscles to improve CVA and thus reduce neck pain. In contrast, Kuo et al.13) demonstrated that combined stretching and strengthening exercises using a ball and foam roller improved FHP and round shoulder in eight weeks. Similarly, Harman et al.10) reported that ten weeks of combined exercise improved FHP.
In this study, all categories, except left-side flexion in the pilates group, showed significant increase in the cervical ROM. Although the results of the left-side flexion were not statistically significant, they did show a slight increasing tendency. A lack of ROM in cervical rotation has been associated with chronic headaches5). The International Headache Society, defines headaches associated with soft tissue or bone structures of the neck as cervicogenic headaches. Headache patients with neck and shoulder pain can decrease their pain and increase cervical ROM by practicing Pilates exercises. It is unclear why only the pilates group experienced increased cervical ROM, as resistive exercises for spinal, scapular, and pelvic stability reportedly optimize mechanical movement and increase ROM23).
We hypothesized that the results of the combined exercise group contradicts what we would expect for the following reasons. First, in our study, the combined exercise treatment used a range of exercises that focused on correcting systematic muscle imbalances rather than only focusing on the deep neck muscles, which reduced the amount of time devoted to the neck muscles. Second, using resistance training may prove counterproductive in women with FHP due to overwork of the structures of the weak and unstable cervical disks, creating more movement dysfunction24). Third, pain is associated with altered muscle recruitment patterns; thus, it may be useful to include exercises that can retrain muscle recruitment patterns, especially ones that focus on the theory of stabilizing locally before moving globally7). Furthermore, as pain increases, muscle guarding becomes pronounced, leading to limited motion and constant muscle contraction. This high level of muscle contraction and tone shortens muscles and creates exaggerated muscle imbalances and thus more pain24). Future studies should include treatments with specific phases to correct postural malalignments, such as an initial phase focusing on correcting local malalignments, with a second phase focusing on global malalignments, and finally a phase devoted to generalized strengthening and flexibility.
The results of this study showed significant decreases in VAS and NDI scores for the pilates and combined exercise groups. Our study agrees other study findings4) that the CVA is significantly lower in groups with more self-reported neck pain. In addition, Sohn et al.5) reported that tension-type headaches become more common with decreasing CVA. Likewise, individuals with neck and shoulder pain tend to have higher incidences of headaches5). Therefore, as Pilates exercise increases CVA, its practice should results in a subsequent decrease in neck and shoulder pain, which may inhibit potential headaches25,26,27).
Szeto et al.6) observed higher muscle fatigue in the trapezius muscle in groups of people with FHP. They also reported that excessive computer use tends to exacerbate FHP. In this study, the Pilates group did not have a significant reduction in upper trapezius muscle fatigue, but did show a significant reduction in SCM fatigue. On the contrary, the combined exercise program did not have significantly reduced muscle fatigue, and had increased upper trapezius muscle fatigue. Combined exercise while there is muscle tension around the neck and shoulders due to muscle imbalance maybe counterproductive as other muscles are forced to compensate; that is, become overworked and fatigued.
In conclusion, the results of this study indicate that the pilates program was more effective in improving CVA, cervical ROM, and muscle fatigue than the combination of stretching and resistance exercise. Pilates focuses on strengthening the core muscles, which improves an individual’s overall posture and postural awareness, which in turn increases global and local stability. Therefore, pilates should be recommended as an appropriate method for treatment and prevention of FHP.
REFERENCES
- 1.Hanten WP, Lucio RM, Russell JL, et al. : Assessment of total head excursion and resting head posture. Arch Phys Med Rehabil, 1991, 72: 877–880. [DOI] [PubMed] [Google Scholar]
- 2.Baldry P, Yunus MB, Inanici F: Myofascial Pain and Fibromyalgia Syndromes: a Clinical Guide to Diagnosis and Management. Edinburgh: Churchill Livingstone, 2010. [Google Scholar]
- 3.Ferrari R, Russell AS: Regional musculoskeletal conditions: neck pain. Best Pract Res Clin Rheumatol, 2003, 17: 57–70. [DOI] [PubMed] [Google Scholar]
- 4.Yip CH, Chiu TT, Poon AT: The relationship between head posture and severity and disability of patients with neck pain. Man Ther, 2008, 13: 148–154. [DOI] [PubMed] [Google Scholar]
- 5.Sohn JH, Choi HC, Lee SM, et al. : Differences in cervical musculoskeletal impairment between episodic and chronic tension-type headache. Cephalalgia, 2010, 30: 1514–1523. [DOI] [PubMed] [Google Scholar]
- 6.Szeto GP, Straker LM, O’Sullivan PB: A comparison of symptomatic and asymptomatic office workers performing monotonous keyboard work—2: neck and shoulder kinematics. Man Ther, 2005, 10: 281–291. [DOI] [PubMed] [Google Scholar]
- 7.Janda V: Muscles and Motor Control in Cervicogenic Disorders: Assessment and Management. New York: Churchill Livingstone, 1994. [Google Scholar]
- 8.Kendall FP, Provance PG, McCreary EK, et al. : Muscles, Testing and Function: With Posture and Pain, 5th ed. Baltimore: Lippincott Williams & Wilkins, 2005. [Google Scholar]
- 9.Wright EF, Domenech MA, Fischer JR, Jr: Usefulness of posture training for patients with temporomandibular disorders. J Am Dent Assoc, 2000, 131: 202–210. [DOI] [PubMed] [Google Scholar]
- 10.Harman K, Hubley-Kozey C, Butler H: Effectiveness of an exercise program to improve forward head posture in normal adults: A randomized, controlled 10-week trial. J Manual Manip Ther, 2005, 13: 163–176. [Google Scholar]
- 11.Boyd-Clark LC, Briggs CA, Galea MP: Muscle spindle distribution, morphology, and density in longus colli and multifidus muscles of the cervical spine. Spine, 2002, 27: 694–701. [DOI] [PubMed] [Google Scholar]
- 12.Segal NA, Hein J, Basford JR: The effects of Pilates training on flexibility and body composition: an observational study. Arch Phys Med Rehabil, 2004, 85: 1977–1981. [DOI] [PubMed] [Google Scholar]
- 13.Kuo YL, Tully EA, Galea MP: Sagittal spinal posture after Pilates-based exercise in healthy older adults. Spine, 2009, 34: 1046–1051. [DOI] [PubMed] [Google Scholar]
- 14.Lynch SS, Thigpen CA, Mihalik JP, et al. : The effects of an exercise intervention on forward head and rounded shoulder postures in elite swimmers. Br J Sports Med, 2010, 44: 376–381. [DOI] [PubMed] [Google Scholar]
- 15.Johnson GM: The correlation between surface measurement of head and neck posture and the anatomic position of the upper cervical vertebrae. Spine, 1998, 23: 921–927. [DOI] [PubMed] [Google Scholar]
- 16.Carlsson AM: Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain, 1983, 16: 87–101. [DOI] [PubMed] [Google Scholar]
- 17.Vernon H, Mior S: The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther, 1991, 14: 409–415. [PubMed] [Google Scholar]
- 18.Cailliet R: Neck and Arm Pain (Pain Series). Philadelphia: FA Davis & Co., 1991. [Google Scholar]
- 19.Griegel-Morris P, Larson K, Mueller-Klaus K, et al. : Incidence of common postural abnormalities in the cervical, shoulder, and thoracic regions and their association with pain in two age groups of healthy subjects. Phys Ther, 1992, 72: 425–431. [DOI] [PubMed] [Google Scholar]
- 20.Emery K, De Serres SJ, McMillan A, et al. : The effects of a Pilates training program on arm-trunk posture and movement. Clin Biomech (Bristol, Avon), 2010, 25: 124–130. [DOI] [PubMed] [Google Scholar]
- 21.Parrott A: The effects of pilates technique and aerobic conditioning on dancers’ technique and aesthetic. Kinesiology, 1993, 15: 45–64. [Google Scholar]
- 22.Ehrlich R, Garlick D, Ninio M: The effect of jaw clenching on the electromyographic activities of 2 neck and 2 trunk muscles. J Orofac Pain, 1999, 13: 115–120. [PubMed] [Google Scholar]
- 23.Michele K, Cilette L, Brenda SW: Women’s Health and Fitness Guide. Illinois: Human Kinetics, 2006.
- 24.Shirley S: Diagnosis and Treatment of Movement Impairment Syndromes, 1st ed. St. Louis: Mosby, 2001. [Google Scholar]
- 25.Lee CW, Hyun J, Kim SG: Influence of pilates mat and apparatus exercises on pain and balance of businesswomen with chronic low back pain. J Phys Ther Sci, 2014, 26: 475–477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hyun J, Hwangbo K, Lee CW: The effects of pilates mat exercise on the balance ability of elderly females. J Phys Ther Sci, 2014, 26: 291–293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kim SD: Effects of yoga exercises for headaches: a systematic review of randomized controlled trials. J Phys Ther Sci, 2015, 27: 2377–2380. [DOI] [PMC free article] [PubMed] [Google Scholar]