

Abstract
Objectives
Circulating exosomes represent novel biomarkers for multiple diseases. In this study, we investigated whether circulating exosome levels could be used as a diagnostic biomarker for steroid-induced osteonecrosis of the femoral head (ONFH).
Methods
We assessed the serum exosome level of 85 patients with steroid-induced ONFH and 115 healthy donors by Nanosight detection. We then assessed the diagnostic accuracy of serum exosomes by receiver operating characteristic curve analysis.
Results
The circulating exosome level of the ONFH group was significantly lower than that of control group. The area under the curve was 0.72, suggesting that the level of serum exosomes has moderate diagnostic accuracy for steroid-induced ONFH.
Conclusion
Circulating exosome levels are valuable in the diagnosis of steroid-induced ONFH.
Cite this article: H-Y. Zhu, Y-C. Gao, Y. Wang, C-Q. Zhang. Circulating exosome levels in the diagnosis of steroid-induced osteonecrosis of the femoral head. Bone Joint Res 2016;5:276–279. DOI: 10.1302/2046-3758.56.BJR-2015-0014.R1.
Keywords: Exosome, Osteonecrosis, Steroid
Article focus
To develop an economical and convenient method for the diagnosis of steroid-induced osteonecrosis of the femoral head (ONFH).
Key messages
The circulating exosome levels of the ONFH group were significantly lower than that of the control group.
Level of serum exosomes has moderate diagnostic accuracy for steroid-induced ONFH.
Strengths and limitations
Strength: the current study is the first study to reveal the value of serum exosome levels as a diagnostic marker for steroid-induced ONFH.
Limitation: Further studies should be conducted with larger sample sizes in different ethnic groups to validate and extend our findings.
Introduction
Steroid-induced osteonecrosis of the femoral head (ONFH) involves the necrosis of cancellous bone which ultimately leads to the collapse of the femoral head.1,2 The incidence of osteonecrosis ranges from 4.6% to 37% in patients receiving steroid treatment.1,3-6 Intervention at an early stage is the key to successful treatment of steroid-induced ONFH. However, early-stage ONFH could only be definitively diagnosed with MRI scanning which is expensive and inconvenient. It is important to find an economical and convenient method for screening ONFH development in patients receiving steroid therapy. After initial screening, MRI scanning can then be conducted for further confirmation.
Exosomes are 30 nm to 120 nm, cell-secreted vesicles that are present in all biological fluids, including blood, urine and cultured medium of cell cultures.7,8 Exosomes carrying miRNA, mRNA and proteins are important vehicles for intercellular communication in vivo. Recent progress indicated that exosomes in biological fluids are promising disease-related biomarkers for chronic kidney disease,9 pancreatic cancer10 and acute coronary syndrome.11 In this study, we report for the first time that the circulating exosome level in steroid-induced ONFH patients was significantly lower than the level found in a healthy population.
Materials and Methods
Patient information
The study was approved by the Ethics Committee of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital. Written consent was obtained from all donors in accordance with the Declaration of Helsinki. The serum samples were obtained from the ONFH Bank of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital. This study included 85 serum samples from patients with steroid-induced ONFH and 115 serum samples from healthy donors. All patients were diagnosed based on MRI and CT scanning, and had a history of receiving long-term or high-dose steroid therapy. No subject in this study had exposure to all known ONFH risk factors for at least three months before serum samples were obtained. The healthy participants were recruited from the community. All participants in the control group received a general medical examination in Shanghai Jiao Tong University Affiliated Sixth People’s Hospital and no systemic diseases such as hypertension or diabetes were detected. The primary diseases of the ONFH patients are summarised in the supplementary material. All ONFH patients were classified with the Steinberg staging system of ONFH.12
Exosome concentration detection
All the serum samples were immediately frozen and stored at -80°C after isolation from donors. Before detection, randomly generated, eight-digit numbers were assigned to each sample. HZ kept the group information and diluted all the samples with phosphate-buffered saline at a ratio of 1:10.6 YG. detected the exosome level. YW then obtained the group information from the first researcher and was responsible for data analysis. The exosome concentration was determined by the number of particles of size 30 nm to 120 nm using Nanosight (Malvern, United Kingdom). All data in this study were expressed as mean with standard deviation (sd). Receiver operating characteristics (ROC) and other statistical analysis was conducted using SPSS 22.0 (IBM, Armonk, New York).
Results
The demographic characteristics of the patients
The demographic features of all subjects are shown in Table I. There were no significant differences in age, gender, height or weight between the ONFH and control groups.
Table I.
Demographic features of patients with osteonecrosis of the femoral head and healthy donors
| Demographic characteristics | ONFH group (n = 85) | Control group (n = 115) |
|---|---|---|
| Male | 44 | 60 |
| Female | 41 | 55 |
| Age (yrs) | 56.3 sd 7.9 | 55.9 sd 8.3 |
| Height (cm) | 167.2 sd 11.4 | 166.8 sd 11.7 |
| Weight (kg) | 67.9 sd 8.9 | 67.3 sd 9.2 |
Statistical analysis: Student’s t test or chi-squared test
SD, standard deviation
The level of circulating exosomes in steroid-induced ONFH patients was lower than that of healthy donors
The circulating exosome level was determined by detecting the number of particles with sizes ranging from 30 nm to 120 nm (Fig. 1). The exosome level in the control group was 9.1 × 1013/mL (sd 2.5). For the patient group, the serum exosome level was 7.3 × 1013/mL (sd 2.0). The serum exosome level was significantly lower in the patient group than in the healthy donors (p < 0.01, Student’s t-test).
Fig. 1.

Nanosight detection of serum exosome level. Representative outcome is shown. Exosome level was determined by the number of particles from 30 nm to 120 nm.
Diagnostic value of serum exosome for diagnosis of steroid-induced ONFH
The diagnostic value of circulating exosome levels for steroid-induced ONFH were then calculated by ROC curve analysis (Fig. 2). Circulating exosome levels showed moderate diagnostic accuracy for the presence of steroid-induced ONFH (Table II). We further demonstrated that the level of circulating exosomes is not predictive of the stages of steroid-induced ONFH (Table III).
Fig. 2.
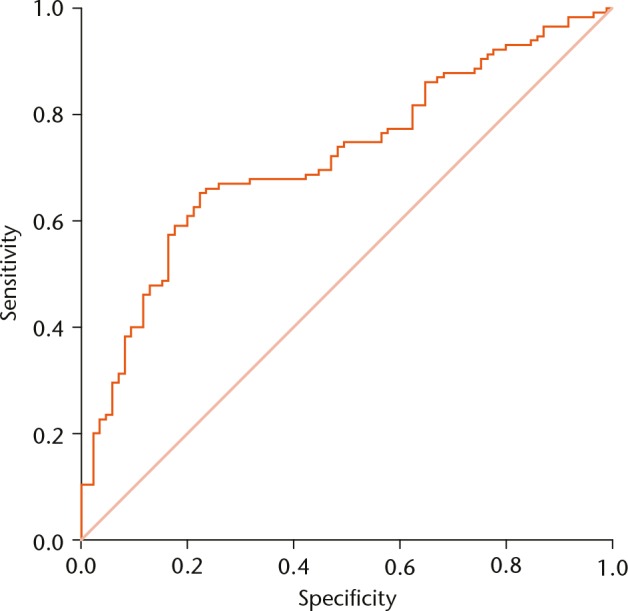
Receiver operating characteristics curve analysis of serum exosome level for detection of steroid-induced osteonecrosis of the femoral head.
Table II.
Area under the curve (AUC) for serum exosome level in the diagnosis of steroid-induced osteonecrosis of the femoral head (ONFH)
| AUC | Cut-off | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|
| 0.72 | 8.4 × 1013/mL | 65.2 | 77.6 | 63.5 | 79.8 |
Receiver operating characteristic (ROC) curve analysis was used to calculate the AUC of serum exosome level for diagnosing steroid-induced ONFH
Table III.
Serum exosome levels in the different stages of steroid-induced osteonecrosis of the femoral head (ONFH)
| Stage I/II (n = 25) | Stage III/IV (n = 30) | Stage V/VI (n = 30) | |
|---|---|---|---|
| Exosome level (13/mL) | 7.2 (sd 2.1) | 7.3 (sd 1.9) | 7.3 (sd 2.0) |
Patients were classified with the Steinberg staging system of ONFH.12
Discussion
Intervention before collapse of the femoral head is the key to success in hip preservative operations. However, the steroid-induced ONFH is a latent disease and usually develops several years after intensive steroid exposure. Additionally, early-stage ONFH is usually asymptomatic, highlighting the need for a convenient laboratory test to detect potential ONFH development. The present study first evaluated the circulating exosome level in patients with steroid-induced ONFH. We demonstrated that the serum exosome level was significantly lower in patients with steroid-induced ONFH compared with healthy donors. ROC analysis demonstrated that the serum exosome level had moderate diagnostic accuracy for the detection of steroid-induced ONFH. The serological examination is more convenient and economical than traditional MRI scanning. After screening by serum exosome level detection, MRI scanning should be conducted for definitive diagnosis.
It is also possible that the change in exosome levels might even precede the alteration in MRI, such as showing the ‘double-line’ sign. Thus, it would be interesting to know whether circulating exosomes can be used as ‘super early’ diagnosis markers for steroid-induced ONFH. A prospective study on a population with intensive steroid exposure might address this question.
In conclusion, circulating exosome level is valuable in the diagnosis of steroid-induced ONFH.
Footnotes
Author Contribution: H-Y. Zhu: Study design.
Y-C. Gao: Collection of serum samples and patient information, Exosome level detection.
Y. Wang: Data analysis and manuscript writing.
C-Q. Zhang: Study design and manuscript revision.
Y-C. Gao is co-first author.
ICMJE conflict of interest: None declared
Supplementary Material
A table showing a summary of the primary diseases of the ONFH patients can be found alongside this paper at http://www.bjr.boneandjoint.org.uk/
Funding Statement
The authors report a grant made to the institution for the work submitted by the Special Fund for Healthy Scientific Research in the Public Interest, China.
References
- 1. Hedri H, Cherif M, Zouaghi K, et al. Avascular osteonecrosis after renal transplantation. Transplant Proc 2007;39:1036-1038. [DOI] [PubMed] [Google Scholar]
- 2. Cooper C, Steinbuch M, Stevenson R, Miday R, Watts NB. The epidemiology of osteonecrosis: findings from the GPRD and THIN databases in the UK. Osteoporos Int 2010;21:569-577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Gontero RP, Bedoya ME, Benavente E, Roverano SG, Paira SO. Osteonecrosis in systemic lupus erythematosus. Reumatol Clin 2014;11:151-155. [DOI] [PubMed] [Google Scholar]
- 4. Shigemura T, Nakamura J, Kishida S, et al. Incidence of osteonecrosis associated with corticosteroid therapy among different underlying diseases: prospective MRI study. Rheumatology (Oxford) 2011;50:2023-2028. [DOI] [PubMed] [Google Scholar]
- 5. LeParc JM, André T, Helenon O, et al. Osteonecrosis of the hip in renal transplant recipients. Changes in functional status and magnetic resonance imaging findings over three years in three hundred five patients. Rev Rhum Engl Ed 1996;63:413-420. [PubMed] [Google Scholar]
- 6. Marston SB, Gillingham K, Bailey RF, Cheng EY. Osteonecrosis of the femoral head after solid organ transplantation: a prospective study. J Bone Joint Surg [Am] 2002;84-A:2145-2151. [DOI] [PubMed] [Google Scholar]
- 7. Keller S, Sanderson MP, Stoeck A, Altevogt P. Exosomes: from biogenesis and secretion to biological function. Immunol Lett 2006;107:102-108. [DOI] [PubMed] [Google Scholar]
- 8. van der Pol E, Boing AN, Harrison P, Sturk A, Nieuwland R. Classification, functions, and clinical relevance of extracellular vesicles. Pharmacol Rev 2012;64:676-705. [DOI] [PubMed] [Google Scholar]
- 9. Lv LL, Cao Y, Liu D, et al. Isolation and quantification of microRNAs from urinary exosomes/microvesicles for biomarker discovery. Int J Biol Sci 2013;9:1021-1031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Madhavan B, Yue S, Galli U, et al. Combined evaluation of a panel of protein and miRNA serum-exosome biomarkers for pancreatic cancer diagnosis increases sensitivity and specificity. Int J Cancer 2015;136:2616-2627. [DOI] [PubMed] [Google Scholar]
- 11. Bi S, Wang C, Jin Y, et al. Correlation between serum exosome derived miR-208a and acute coronary syndrome. Int J Clin Exp Med 2015;8:4275-4280. [PMC free article] [PubMed] [Google Scholar]
- 12. Mont MA, Cherian JJ, Sierra RJ, Jones LC, Lieberman JR. Nontraumatic Osteonecrosis of the Femoral Head: Where Do We Stand Today? A Ten-Year Update. J Bone Joint Surg [Am] 2015;97-A:1604-1627. [DOI] [PubMed] [Google Scholar]