

Abstract
Treatment of gastroesophageal reflux disease in the United States today is binary, with the majority of patients with gastroesophageal reflux disease being treated with antisecre-tory medications and a minority of patients, typically those with volume regurgitation, undergoing Nissen fundoplication. However, there has been increasing dissatisfaction with proton pump inhibitor therapy among a significant number of patients with gastroesophageal reflux disease owing to cost, side effects, and refractory symptoms, and there has been a general reluctance to undergo surgical fundoplication due to its attendant side-effect profile. As a result, a therapy gap exists for many patients with gastroesophageal reflux disease. Alternative techniques are available for these gap patients, including 2 endoscopic fundoplication techniques, an endoscopic radiofrequency energy delivery technique, and 2 minimally invasive surgical procedures. These alternative techniques have been extensively evaluated; however, there are limitations to published studies, including arbitrary definitions of success, variable efficacy measurements, deficient reporting tools, inconsistent study designs, inconsistent lengths of follow-up postintervention, and lack of comparison data across techniques. Although all of the techniques appear to be safe, the endoscopic techniques lack demonstrable reflux control and show variable symptom improvement and variable decreases in proton pump inhibitor use. The surgical techniques are more robust, with evidence for adequate reflux control, symptom improvement, and decreased proton pump inhibitor use; however, these techniques are more difficult to perform and are more intrusive. Additionally, these alternative techniques have only been studied in patients with relatively normal anatomy. The field of gastroesophageal reflux disease treatment is in need of consistent definitions of efficacy, standardized study design and outcome measurements, and improved reporting tools before the role of these techniques can be fully ascertained.
Keywords: Gastroesophageal reflux disease, Nissen fundoplication, proton pump inhibitor
In the past 15 years, an array of innovative endoscopic and surgical techniques have been developed to treat patients with symptomatic gastroesophageal reflux disease (GERD) who are dissatisfied with proton pump inhibitors (PPIs) or Nissen fundoplication. Despite extensive study, however, key questions remain as to the role of these therapies, their individual efficacies and comparative benefits, the most appropriate target populations for specific techniques, and how to best evaluate them. The answers to these questions can help improve the treatment of GERD, which currently affects up to 30% of the adult population in the United States and costs billions of dollars in pharmaceutical, endoscopic, and surgical outlays.1 GERD also adversely affects quality of life, can progress to substantial complications such as stricture formation, and is the leading cause of Barrett esophagus and adenocarcinoma of the esophagus.2,3
Acid suppression therapy, mainly PPIs, has long been the standard treatment for GERD, and this treatment has been shown to be generally safe and effective for the majority of GERD patients. PPIs are most effective for acid-related symptoms such as heartburn and esophagitis; however, PPI therapy is less effective for regurgitation, as PPIs do not address the underlying incompetency of the lower esophageal sphincter (LES).4 Acid suppression therapy alters the composition of the refluxate, particularly its acidity, but does not prevent abnormal reflux, leaving a subset of patients at risk for ongoing symptoms and progression of disease.5 A recent study has demonstrated that up to 30% to 40% of patients on PPI therapy (even those on double-dose therapy) continue to experience heartburn or regurgitation symptoms despite adequate healing of esophagitis.6 This statistic, coupled with the potential PPI side-effect profile (eg, possible risk of osteoporosis, Clostridium difficile infection, community-acquired pneumonia) and ongoing cost, makes alternative GERD therapy necessary.
The main alternative therapy for GERD patients dissatisfied with PPIs has traditionally been surgical gastric fundoplication, originally referred to as Nissen. Fundo-plication surgery has recently been demonstrated to be as effective as, or superior to, chronic PPI therapy; however, Nissen surgery is associated with a significant side-effect profile that includes gas bloat syndrome, flatulence, inability to belch or vomit, and dysphagia, all of which negatively impact quality-of-life scores in surgical patients.7 Utilizing the gastric fundus as a wrap creates a tightly augmented LES that reduces the total number of reflux episodes to below what is considered normal. As a result, Nissen fundoplication is highly effective at preventing reflux but also prevents the normal venting of swallowed air. The inability to vent (belch), as well as the reduced number of normal reflux episodes following fundoplication surgery, contributes to the side effects of bloating and flatulence. Due to the pronounced side-effect profile related to Nissen surgery, the popularity of this procedure has been declining in recent years, and there appears to be no net benefit over PPI therapy to warrant its use in the typical GERD patient treated with PPIs.8,9
Treatment of GERD in the United States is therefore essentially binary, with most GERD patients undergoing PPI therapy and a smaller number of patients, mainly those with volume regurgitation, undergoing Nissen fun-doplication with its attendant side effects. A significant therapy gap exists, consisting of patients who are dissatisfied with PPI therapy yet are reluctant to undergo surgical fundoplication. If approximately 30% to 40% of the 20 million Americans on daily PPI therapy are dissatisfied with their results, and fewer than 20,000 patients undergo Nissen surgery annually, then approximately 6 to 8 million GERD patients might be available for some type of alternative endoscopic or surgical therapy consisting of either a less-obtrusive surgical procedure or an endoscopic antireflux technique.9
Currently available endoscopic antireflux techniques include 2 fundoplication procedures (transoral incisionless fundoplication [TIF; EsophyX, EndoGastric Solutions] and the SRS Endoscopic Stapling System [Medigus]) and radiofrequency (RF) energy delivery to the LES (Stretta, Mederi Therapeutics), which is a somewhat older modality that was recently reintroduced. New surgical techniques include sphincter augmentation of the LES using a magnetic implant that encircles the native LES (LINX, Torax Medical), which is available in the United States and Europe, and a surgically implanted LES pacemaker (EndoStim, EndoStim BV) that is currently available only in Europe. This article reviews the use of these devices for the treatment of GERD.
The Ideal Gap Therapy
Several alternative treatment options are available for patients with GERD who remain symptomatic on PPI therapy and who wish to avoid traditional fundoplication. Ideally, whichever surgical or endoscopic gap therapy these patients choose would be minimally invasive, would be highly efficacious with regard to long-term symptom and pH control, would result in little to no anatomic distortion, would be completed in an outpatient setting in less than an hour, would be safe with no long-term sequelae, would allow a normal diet immediately upon completion, and would be reversible. However, it is difficult to establish what exactly constitutes efficacy, which type of study is needed to prove efficacy, what constitutes long-term follow-up, and what the tradeoff is between efficacy and side effects.10-13
Neither PPI consumption nor symptom improvement alone is sufficient to demonstrate scientific value, particularly if measured in the short term (≤1 year).10,12 In clinical practice, therapeutic response is primarily based on long-term improvement of symptoms and long-term response to PPIs. Consistent with clinical practice, extended follow-up (ideally 3-5 years) focused on the maintenance and durability of symptom improvement and/or discontinuation of PPI therapy would lend more credence to these outcome measures.
Given the above concerns, pH data are of outsize importance, as assessment of pH is the only objective scientific variable available that is largely free of placebo response and can consistently be compared across studies.11 Issues remain, however, including whether significantly improved pH scores that remain in an abnormal range for the study group are acceptable results, or whether only normalized pH scores should be accepted as evidence of efficacy. Moreover, a consensus needs to be reached regarding whether normal values should be accepted as a mean for the group or if a certain percentage of patients who achieve normal pH scores should be considered evidence of an effective result. Further questions remain concerning how to treat patients who are symptomatically improved, either partially or completely, yet still have abnormal pH scores. To a patient, symptom improvement and medication usage are paramount, but persistently abnormal pH scores signify ongoing reflux with the potential for future complications or progression of disease. Traditionally, many clinicians would consider lack of objective reflux control despite symptom improvement as failure of an antireflux technique,12,13 although others have recently become more sanguine about this outcome.14
Additionally, there is disagreement regarding optimal study design and the minimal required length of patient follow-up. Many clinicians demand randomized, controlled trials (RCTs) because intervention studies without controls are susceptible to placebo effects with regard to early assessment of subjective variables such as symptoms and PPI use. This is particularly true if study follow-ups are 1 year or less.13,15 Sham-controlled trials can help clarify the placebo-response issue, but the benefit of a control population in this setting is unclear if pH scores do not improve in the intervention group. It should be noted that most published RCTs in the field of GERD intervention are small and short-term only, with patients either crossed over or primary outcomes assessed at 6 months or earlier.15
Given the chronic nature of GERD, longer-term trials (with at least 3-5 years of follow-up), even if uncontrolled, might better inform patient decisions. Such trials could possibly have more value than a short-term RCT as long as they contain predefined success criteria and demonstrate adequate objective pH control (ie, the majority of study patients achieve normal pH scores measured at least 1 year postintervention). A review of several sham-controlled trials demonstrated that the placebo effect on measured acid exposure is small or nonexistent, and any placebo effect on subjective symptoms or PPI use would almost certainly fade at 3 to 5 years.11
Optimal Study Design Principles and Definitions of Efficacy
A reasonable starting point might be to consider the principles listed below regarding study design and definitions of efficacy.
For studies with short-term follow-up (≤1 year), RCTs are mandatory to account for any placebo effect regarding symptom assessment and PPI use. For studies with 3- to 5-year follow-up, an uncontrolled study design is acceptable as long as objective data exist to demonstrate reflux control (eg, ≥50% patients normalize pH scores at 1 year).
Any RCT that demonstrates subjective symptom and PPI improvement but not pH control (eg, either pH scores do not improve, or they do improve but <50% of patients normalize pH) must then continue to follow patients for 3 to 5 years to determine the long-term outcomes of the subjective symptoms.
Successful symptom control is defined as complete cessation of classic GERD symptoms (eg, heartburn, regurgitation) in at least 50% of the study patients at 1 year for a RCT and at 3 to 5 years for an uncontrolled trial with demonstrable pH control. A consensus definition of complete control will be required, as will modification and validation of existing scales.10
Partial symptom control can be assessed, but is not an acceptable outcome.
Successful PPI control is defined as either complete elimination of PPI use or as-needed use only (≤1 PPI/week) in at least 50% of the study patients at 1 year for a RCT, or at 3 to 5 years for an uncontrolled trial with demonstrable pH normalization in at least 50% of the study population.
Partial PPI improvement with more than as-needed use (eg, 50% reduction in PPI dosage or decreased frequency of PPI use where patients remain PPI-dependent) can be assessed, but is not an acceptable outcome.
pH data should be assessed at 1 year postintervention. pH data obtained at 6 months, even via a RCT, could be misleading due to a potential edema effect at the gastroesophageal junction, and early pH data will miss delayed technique failure.
Surgical and Endoscopic Gap Therapies
Although a complete review of the data regarding the 2 endoscopic fundoplication techniques, the endoscopic RF technique, and the 2 newer surgical antireflux techniques is beyond the scope of this article, the following summary can be offered based on the principles detailed above. It should be noted that others in the field may provide alternative definitions of success and would draw different conclusions. It should also be noted that GERD patients who have been offered these therapies have, to date, been highly selected and have had relatively normal anatomy (hiatal hernia <3 cm in length), no Barrett esophagus, and no severe esophagitis.
Endoscopic Radiofrequency Delivery
The Stretta technique involves delivery of RF energy to a broad region of the LES via a balloon-based, 4-electrode needle array (Figure 1).16 The exact mechanism of action is unclear but likely involves post—RF ablation scarring and fibrosis of the esophageal submucosa and/or disruption of neural signaling leading to modestly increased LES tone vs compliance/yield effects.17 There have been 4 RCTs of the Stretta technique (both sham- and PPI-controlled), all relatively small and with short-term follow-up only (3-12 months), as well as numerous short- and longer-term uncontrolled trials.17-22 A recent comprehensive meta-analysis of these RCTs, using pooled data, demonstrated no significant benefit of Stretta over sham with regard to pH improvement (only a small number of patients normalized pH); there was no mean change in LES pressure, no statistical improvement in stopping PPIs, and no improvement in overall GERD symptom scores.17
Figure 1.
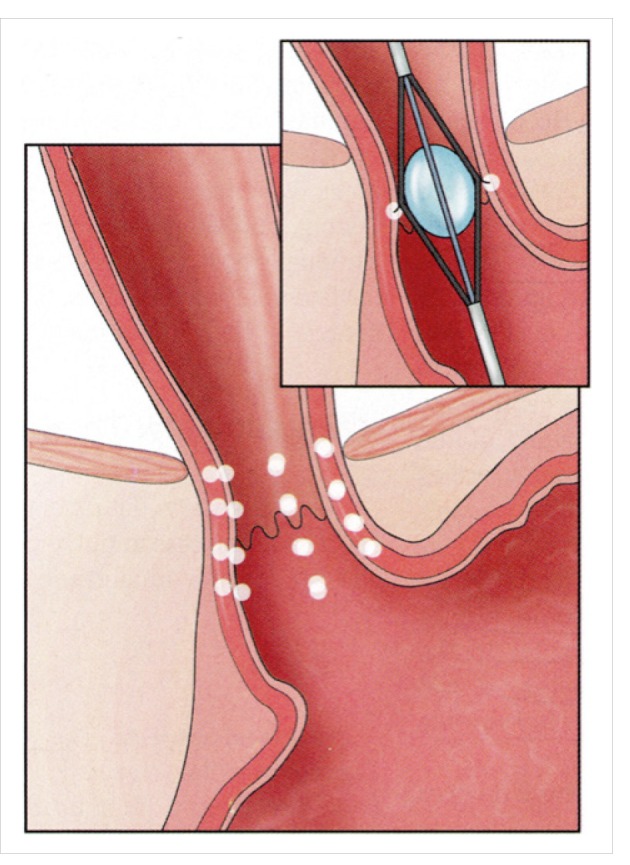
A diagrammatic depiction of radiofrequency delivery of energy to the region of the lower esophageal sphincter using a 4-needle balloon array. Radiofrequency energy is delivered circumferentially in 4 locations above and below the Z line.
Reproduced from Min MX and Ganz RA.16
Some of the long-term uncontrolled trials have demonstrated improvement in symptoms, PPI use, and pH parameters; however, pH values remained in an abnormal range, with few patients normalizing pH scores.22 The procedure does appear to be safe, with few serious adverse events. Thus, this author believes that the Stretta technique appears to be well tolerated, although the treatment effects on GERD symptoms and PPI reduction are either absent or modest at best, with no demonstrable adequate pH control.17,22
Endoscopic Fundoplication
TIF and the Medigus endoscopic stapling procedure create endoscopic fundoplications but are limited to patients with essentially normal anatomy, as the techniques cannot perform hernia repair (Figure 2).16 There have been 4 PPI-or sham-controlled RCTs involving the TIF procedure, all with short-term follow-up (6-12 months), although only 3 studies involved patients with the traditional GERD symptoms of both heartburn and regurgitation.14,23,24 A study by Hunter and colleagues demonstrated improvement in pH scores at 6 months, but scores remained in an abnormal range,14 whereas a study by Witteman and colleagues demonstrated improvement in pH scores at 6 months; however, by 12 months, the scores deteriorated and there was no demonstrable improvement in pH.23 In this latter study, normalization of pH was achieved in only 29% of patients. Hakansson and colleagues demonstrated pH improvement at 6 months in the TIF group, although only approximately half of the patients had completed pH data.24
Figure 2.

A diagrammatic depiction of transoral incisionless fundoplication.
Reproduced from Min MX and Ganz RA.16
In the study conducted by Hunter and colleagues, significant improvement in symptoms was limited to regurgitation; the study does not disclose the actual global GERD symptom scores and there was no difference in composite symptom scores at 6 months between the TIF group and the PPI group.14 Eighty percent of TIF patients remained off of PPI therapy, however.14 The study by Witteman and colleagues demonstrated significant symptom improvement at 12 months, but with only 39% of patients completely off of PPIs.23 Witteman and colleagues concluded that the endoscopically created antireflux barrier using the TIF technology deteriorated with increased follow-up duration and that TIF was not equivalent to PPIs in GERD treatment in terms of acid control.23 At 6 months, Håkansson and colleagues showed that 59% of TIF patients were in clinical remission with complete cessation of PPIs compared to 18% of the sham group.24 TIF appeared to be safe in these studies, with few adverse events reported.
There are limited data available for the SRS fundo-plication system. In a 6-month uncontrolled trial, pH scores were improved but remained in abnormal range postprocedure.25 Symptom scores and PPI usage also improved but were recorded only at 6 months. Of 69 patients enrolled, there were 3 episodes of pneumome-diastinum, 1 pleural effusion, and 1 esophageal leak, although most patients tolerated the procedure well. More studies are needed before any conclusions can be drawn about this technique and how this fundoplication compares to the TIF procedure.
Magnetic Sphincter Augmentation
No RCTs have been conducted regarding magnetic sphincter augmentation using the LINX device (Figure 3), but there have been prospective, multicenter, long-term (2-5 years), uncontrolled trials with rigorous patient follow-up and prespecified success criteria.26-28 These studies demonstrated excellent pH control with more than 50% of patients normalizing pH scores at 1 year, and significant improvements in symptom scores and PPI usage, compared to baseline, at the 5-year interval. At 5 years, 85% of patients were completely off of PPIs.28 As previously discussed, the lack of a control group makes these trials susceptible to a short-term placebo effect with regard to early assessment of the subjective variables; however, it should be noted that the sustained objective elimination of pathologic esophageal acid exposure in the majority of patients at 1 year and the long-term nature of the follow-up helps corroborate the treatment effect. The totality of clinical data showed significant improvement across all parameters measured, including esophageal acid exposure, heartburn, regurgitation, PPI use, and GERD quality-of-life scores.
Figure 3.

A diagrammatic depiction of magnetic sphincter augmentation. The magnetic device is shown in the closed (A) and open (B) positions.
Reproduced from Ganz RA et al.26
The surgical placement of the magnetic device is safe with no infection, migration, erosion, or perioperative complications noted in long-term trials.26-28 A few erosions (without perforation) have been sporadically reported outside of trials, however.29 The procedure is performed on an outpatient basis with immediate resumption of a normal diet and is completely reversible upon removal of the magnets with no anatomic distortion, as the procedure spares the fundus. The removal rate in trials is approximately 6%, and the only significant adverse event is dysphagia, which affects approximately 6% of patients on a long-term basis.26-28 The procedure appears to work by augmenting the native LES and preventing premature LES effacement and opening. There may also be favorable compliance and yield curve char-acteristics.30 Based on these data, magnetic sphincter augmentation approaches Nissen level of efficacy, with fewer side effects, albeit with studies limited to a select GERD population.
Lower Esophageal Sphincter Pacing
Another surgical procedure, which is not currently available in the United States, is pacing of the LES using EndoStim, a surgically implanted pacemaker. Two RCTs of this technique are pending, and no results are currently available. Uncontrolled trials, some reported out to 2 years, demonstrate excellent pH control, with pH normalization in more than 50% of patients, and significant improvements in GERD symptoms and PPI use, with 70% to 80% of patients reporting complete cessation of PPI use.31-33 Previous studies in both animals and humans have demonstrated that electrical stimulation of the LES can increase resting LES tone using either microstimulators or paired electrodes; constant or pulsed stimulation; and various frequencies, voltages, and pulse param-eters.31 The EndoStim technology utilizes 5- to 10-mm electrodes, 30-minute pacing sessions with 90-minute breaks 12 times daily, and pulses of 5 mA, 20 Hz, and 220 ms. Stimulation sessions can be modulated if patients have persistent symptoms either by changing electrodes, increasing the number of stimulation sessions per day, or increasing the voltage amplitude. The procedure appears safe, with no significant perioperative complications noted and no postprocedure dysphagia reported.32,33
Conclusion
The chronic burden of GERD, dissatisfaction with PPI agents, and reluctance to undergo Nissen fundoplication due to its side-effect profile have left a therapy gap. There are now several new endoscopic and surgical techniques that have emerged to fill the need for alternative therapies. In general, the endoscopic therapies described in this article, although potentially effective in some short-term studies, appear to be less robust, with less durable results, and will likely require additional improvements and study before they are widely adopted. The surgical options described are more intrusive yet still minimally invasive, and appear to approach Nissen levels of efficacy and durability, although the patients studied to date have been restricted to those with relatively normal anatomy. There are great limitations in this field related to inconsistent definitions of success, deficient GERD symptom scales with no clear definition of asymptomatic patients, variable study designs and lengths of follow-up, uncertainty as to the appropriate GERD populations for each technique, and lack of studies comparing techniques across populations, making concrete recommendations difficult. Hopefully, many of these issues will be clarified going forward and will allow for a better understanding of the true role of these techniques in the treatment of GERD.
Footnotes
Dr Ganz has no relevant conflicts of interest to disclose.
References
- 1.Shaheen NJ, Hansen RA, Morgan DR, et al. The burden of gastrointestinal and liver diseases, 2006. Am J Gastroenterol. 2006;101(9):2128–2138. doi: 10.1111/j.1572-0241.2006.00723.x. [DOI] [PubMed] [Google Scholar]
- 2.Becher A, El-Serag H. Systematic review: the association between symptomatic response to proton pump inhibitors and health-related quality of life in patients with gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2011;34(6):618–627. doi: 10.1111/j.1365-2036.2011.04774.x. [DOI] [PubMed] [Google Scholar]
- 3.Lagergren J, Bergström R, Lindgren A, Nyrén O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999;340(11):825–831. doi: 10.1056/NEJM199903183401101. [DOI] [PubMed] [Google Scholar]
- 4.Kahrilas PJ, Jonsson A, Denison H, Wernersson B, Hughes N, Howden CW. Regurgitation is less responsive to acid suppression than heartburn in patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2012;10(6):612–619. doi: 10.1016/j.cgh.2012.01.022. [DOI] [PubMed] [Google Scholar]
- 5.Blonski W, Vela MF, Castell DO. Comparison of reflux frequency during prolonged multichannel intraluminal impedance and pH monitoring on and off acid suppression therapy. J Clin Gastroenterol. 2009;43(9):816–820. doi: 10.1097/MCG.0b013e318194592b. [DOI] [PubMed] [Google Scholar]
- 6.Castell DO, Kahrilas PJ, Richter JE, et al. Esomeprazole (40 mg) compared with lansoprazole (30 mg) in the treatment of erosive esophagitis. Am J Gastroenterol. 2002;97(3):575–583. doi: 10.1111/j.1572-0241.2002.05532.x. [DOI] [PubMed] [Google Scholar]
- 7.Lundell L, Miettinen P, Myrvold HE, et al. Nordic GERD Study Group. Comparison of outcomes twelve years after antireflux surgery or omeprazole maintenance therapy for reflux esophagitis. Clin Gastroenterol Hepatol. 2009;7(12):1292–1298. doi: 10.1016/j.cgh.2009.05.021. [DOI] [PubMed] [Google Scholar]
- 8.Wang YR, Dempsey DT, Richter JE. Trends and perioperative outcomes of inpatient antireflux surgery in the United States, 1993-2006. Dis Esophagus. 2011;24(4):215–223. doi: 10.1111/j.1442-2050.2010.01123.x. [DOI] [PubMed] [Google Scholar]
- 9.DeMeester TR The David Sun lecture: détente in the therapy of GERD. [January 4, 2015]. http://universe-syllabi.gi.org/acg2010_30_nar.pdf
- 10.Chassany O, Holtmann G, Malagelada J, Gebauer U, Doerfler H, Devault K. Systematic review: health-related quality of life (HRQOL) questionnaires in gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2008;27(11):1053–1070. doi: 10.1111/j.1365-2036.2008.03683.x. [DOI] [PubMed] [Google Scholar]
- 11.Rothstein RI. Endoscopic therapy of gastroesophageal reflux disease: outcomes of the randomized-controlled trials done to date. J Clin Gastroenterol. 2008;42(5):594–602. doi: 10.1097/MCG.0b013e31816bcde5. [DOI] [PubMed] [Google Scholar]
- 12.Pandolfino JE, Krishnan K. Do endoscopic antireflux procedures fit in the current treatment paradigm of gastroesophageal reflux disease? Clin Gastroenterol Hepatol. 2014;12(4):544–554. doi: 10.1016/j.cgh.2013.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hogan WJ. Clinical trials evaluating endoscopic GERD treatments: is it time for a moratorium on the clinical use of these procedures? Am J Gastroenterol. 2006;101(3):437–439. doi: 10.1111/j.1572-0241.2006.00523.x. [DOI] [PubMed] [Google Scholar]
- 14.Hunter JG, Kahrilas PJ, Bell RC, et al. Efficacy of transoral fundoplication vs omeprazole for treatment of regurgitation in a randomized controlled trial. Gastroenterology. 2015;148(2):324–333.e5. doi: 10.1053/j.gastro.2014.10.009. [DOI] [PubMed] [Google Scholar]
- 15.Elmunzer BJ. Increasing the impact of randomized, controlled trials in gastrointestinal endoscopy. Gastroenterology. 2015;149(3):521–525. doi: 10.1053/j.gastro.2015.07.022. [DOI] [PubMed] [Google Scholar]
- 16.Min MX, Ganz RA. Update in procedural therapy for GERD—magnetic sphincter augmentation, endoscopic transoral incisionless fundoplication vs laparoscopic Nissen fundoplication. Curr Gastroenterol Rep. 2014;16(2):374–379. doi: 10.1007/s11894-014-0374-4. [DOI] [PubMed] [Google Scholar]
- 17.Lipka S, Kumar A, Richter JE. No evidence for efficacy of radiofrequency ablation for treatment of gastroesophageal reflux disease: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2015;13(6):1058–1067.e1. doi: 10.1016/j.cgh.2014.10.013. [DOI] [PubMed] [Google Scholar]
- 18.Corley DA, Katz P, Wo JM, et al. Improvement of gastroesophageal reflux symptoms after radiofrequency energy: a randomized, sham-controlled trial. Gastro-enterology. 2003;125(3):668–676. doi: 10.1016/s0016-5085(03)01052-7. [DOI] [PubMed] [Google Scholar]
- 19.Coron E, Sebille V, Cadiot G, et al. Consortium de Recherche Indépendant sur le Traitement et L’exploration du Reflux Gastro-oesophagien et de L’endobrachyoesophage (CRITERE). Clinical trial: radiofrequency energy delivery in proton pump inhibitor-dependent gastro-oesophageal reflux disease patients. Aliment Pharmacol Ther. 2008;28(9):1147–1158. doi: 10.1111/j.1365-2036.2008.03790.x. [DOI] [PubMed] [Google Scholar]
- 20.Aziz AMA, El-Khayat HR, Sadek A, et al. A prospective randomized trial of sham, single-dose Stretta, and double-dose Stretta for the treatment of gastroesophageal reflux disease. Surg Endosc. 2010;24(4):818–825. doi: 10.1007/s00464-009-0671-4. [DOI] [PubMed] [Google Scholar]
- 21.Arts J, Bisschops R, Blondeau K, et al. A double-blind sham-controlled study of the effect of radiofrequency energy on symptoms and distensiblity of the gastro-esophageal junction in GERD. Am J Gastroenterol. 2012;107(2):222–230. doi: 10.1038/ajg.2011.395. [DOI] [PubMed] [Google Scholar]
- 22.Perry KA, Banerjee A, Melvin WS. Radiofrequency energy delivery to the lower esophageal sphincter reduces esophageal acid exposure and improves GERD symptoms: a systematic review and meta-analysis. Surg Laparosc Endosc Percutan Tech. 2012;22(4):283–288. doi: 10.1097/SLE.0b013e3182582e92. [DOI] [PubMed] [Google Scholar]
- 23.Witteman BPL, Conchillo JM, Rinsma NF, et al. Randomized controlled trial of transoral incisionless fundoplication vs. proton pump inhibitors for treatment of gastroesophageal reflux disease. Am J Gastroenterol. 2015;110(4):531–542. doi: 10.1038/ajg.2015.28. [DOI] [PubMed] [Google Scholar]
- 24.Håkansson B, Montgomery M, Cadiere GB, et al. Randomised clinical trial: transoral incisionless fundoplication vs. sham intervention to control chronic GERD. Aliment Pharmacol Ther. 2015;42(11-12):1261–1270. doi: 10.1111/apt.13427. [DOI] [PubMed] [Google Scholar]
- 25.Zacherl J, Roy-Shapira A, Bonavina L, et al. Endoscopic anterior fundoplication with the Medigus Ultrasonic Surgical Endostapler (MUSE™) for gastroesophageal reflux disease: 6-month results from a multi-center prospective trial. Surg Endosc. 2015;29(1):220–229. doi: 10.1007/s00464-014-3731-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ganz RA, Peters JH, Horgan S, et al. Esophageal sphincter device for gastro-esophageal reflux disease. N Engl J Med. 2013;368(8):719–727. doi: 10.1056/NEJMoa1205544. [DOI] [PubMed] [Google Scholar]
- 27.Bonavina L, DeMeester T, Fockens P, et al. Laparoscopic sphincter augmentation device eliminates reflux symptoms and normalizes esophageal acid exposure: one- and 2-year results of a feasibility trial. Ann Surg. 2010;252(5):857–862. doi: 10.1097/SLA.0b013e3181fd879b. [DOI] [PubMed] [Google Scholar]
- 28.Ganz RA, Edmundowicz SA, Taiganides PA, et al. Long-term outcomes of patients receiving a magnetic sphincter augmentation device for gastroesophageal reflux. Clin Gastroenterol Hepatol. 2016;14(5):671–677. doi: 10.1016/j.cgh.2015.05.028. [DOI] [PubMed] [Google Scholar]
- 29.US Food and Drug Administration. MAUDE—Manufacturer and User Facility Device Experience. [June 12, 2016]. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/search.cfm
- 30.Ganz RA, Gostout CJ, Grudem J, Swanson W, Berg T, DeMeester TR. Use of a magnetic sphincter for the treatment of GERD: a feasibility study. Gastrointest Endosc. 2008;67(2):287–294. doi: 10.1016/j.gie.2007.07.027. [DOI] [PubMed] [Google Scholar]
- 31.Chiu J, Sofler E. Novel surgical options for gastroesophageal reflux disease. Expert Rev Gastroenterol Hepatol. 2015;9(7):943–951. doi: 10.1586/17474124.2015.1039986. [DOI] [PubMed] [Google Scholar]
- 32.Kappelle WFW, Bredenoord AJ, Conchillo JM, et al. Electrical stimulation therapy of the lower oesophageal sphincter for refractory gastro-oesophageal reflux disease—interim results of an international multicentre trial. Aliment Pharmacol Ther. 2015;42(5):614–625. doi: 10.1111/apt.13306. [DOI] [PubMed] [Google Scholar]
- 33.Rodriguez L, Rodríguez P, Gómez B, et al. Two-year results of intermittent electrical stimulation of the lower esophageal sphincter treatment of gastroesophageal reflux disease. Surgery. 2015;157(3):556–567. doi: 10.1016/j.surg.2014.10.012. [DOI] [PubMed] [Google Scholar]