

Abstract
The phenomenon of exercise‐induced hemoptysis is still relatively underrecognised in humans. We report a case of recurrent hemoptysis brought on by vigorous exercise. A 33‐year‐old male presented with several episodes of intermittent fresh small‐volume hemoptysis reproducible on vigorous exercise. There was no other significant medical history other than a past history of testicular tumor, treated with orchidectomy and adjuvant Bleomycin‐based chemotherapy 1 year prior to onset of symptoms. Computed tomography scan showed no major abnormalities other than few small bilateral non‐specific nodules. Computed tomography aortogram and pulmonary angiogram, ventilation/perfusion scan, and echocardiography yielded no significant abnormalities. Infectious, autoimmune disease, coagulopathy, vasculitis, and malignant causes were excluded. Bronchoscopy showed possible endobronchial bleeding. This phenomenon is thought to be due to vulnerability of pulmonary capillaries to stress or mechanical failure during strenuous exercise at high cardiorespiratory workload.
Keywords: Exercise, hemoptysis, pulmonary capillary, pulmonary hemorrhage, pulmonary oedema
Introduction
The phenomenon of exercise‐induced hemoptysis is well known to occur in thoroughbred racehorses, but it is still relatively underrecognised or reported in human subjects 1, 2. However, in humans, still relatively very rare, there are occasional reports of exercise induced pulmonary hemorrhage or exercise‐induced pulmonary oedema in the literature, specially occurring in marathon runners, cyclists and swimmers, and breath‐hold divers 2, 3. A proposed mechanism is due to the alteration in the pulmonary capillary surface and collagen matrix structure in response to high transcapillary pressure during high cardiorespiratory workload 4, 5. We report a case of recurrent frank endobronchial bleeding associated with vigorous exercise (jogging) in a patient previously treated with bleomycin for testicular tumor.
Case Report
A 33‐year‐old Australian male, who worked in the Australian Defence Force, presented to hospital with several episodes of recurrent intermittent fresh small‐volume hemoptysis reproducible on vigorous exercise (jogging) with no associated dyspnoea, constitutional, or other concerning symptoms. Each episode settled spontaneously after about 30 min of ceasing to exercise.
There was a history of stage I testicular mixed germ cell tumor diagnosed earlier, for which he had undergone an orchidectomy and received adjuvant chemotherapy.
There were no other comorbidities or regular medications. There was no history of smoking, alcohol consumption, or illicit substances use. There was no family history of a similar presentation or coagulation abnormality. The patient lived in an urban area and had no pets or infectious contacts.
The hemoptysis started approximately one year after the diagnosis of his cancer. It was always however associated with intense exercise (jogging for about 1.5 km on a usual 5‐km planned running) and resolved spontaneously shortly after 10 to 15 min of rest. Clinical examinations were consistently unremarkable. A computed tomography (CT) of the chest revealed few non‐specific pulmonary nodules measuring 4–6 mm in the lower lobes bilaterally (Fig. 1). A ventilation/perfusion scan was negative for pulmonary emboli. Bronchoscopy showed no endobronchial abnormalities and yielded no positive lavage findings. Importantly, tumor markers remained normal. Respiratory function tests and transthoracic echocardiogram were both normal. Both CT aortogram and pulmonary angiogram were also negative for any vascular malformations. A stress echocardiogram showed normal left atrial pressure at maximum exercise. Autoimmune tests, vasculitis, coagulation abnormality, and serology for infectious causes were also negative. Progress CT scans over the next four months revealed spontaneous resolution of these nodules, except for one remaining 4‐mm right lower lobe nodule.
Figure 1.
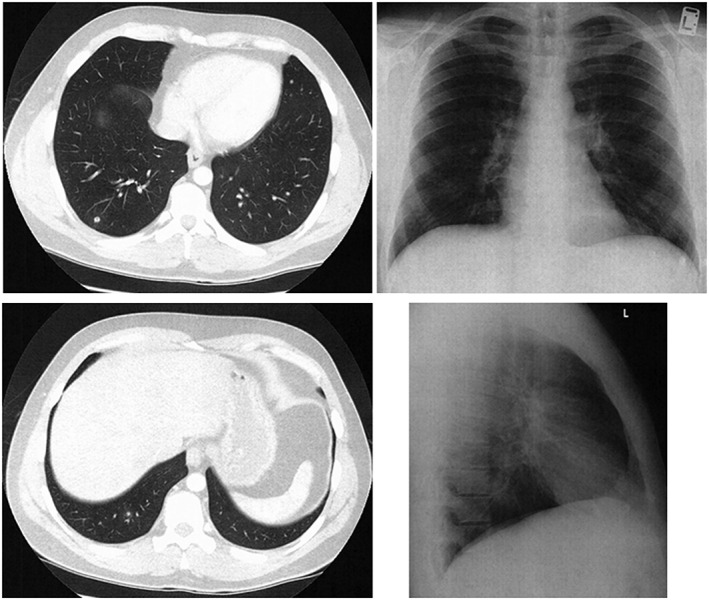
Chest X‐ray demonstrated no significant changes. Computed tomography of the chest revealed non‐specific nodules.
A bronchoscopy was performed within few hours of one of the episodes; this did demonstrate small bleeding spot just distal to the right upper lobe bronchus bifurcation (Fig. 2).
Figure 2.
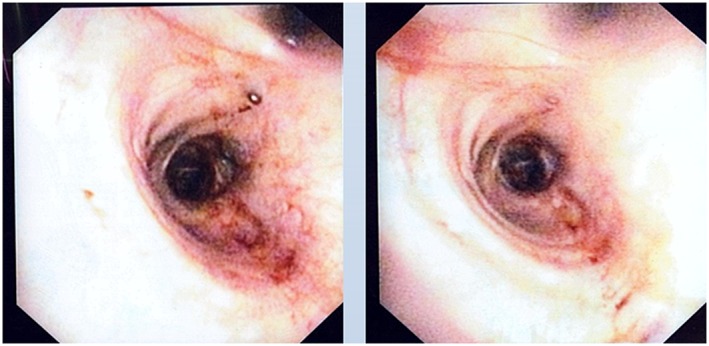
Bronchoscopy revealed an area of possible bleeding.
Because of persistent symptoms, the patient underwent a cardiopulmonary exercise test, performing to 100% predicted heart rate. This again showed no abnormalities and also hemoptysis could not be replicated. A bronchoscopy was performed immediately after the stress test, which showed no endobronchial or post‐nasal bleeding. There was, nonetheless, an area appearing as a small collection of vessels, which was treated with argon plasma coagulation. The patient was advised to monitor and maintain his heart rate under 80% of the predicted maximum during exercise. He remains well and has had no recurrence for the last 12 months (Fig. 3).
Figure 3.
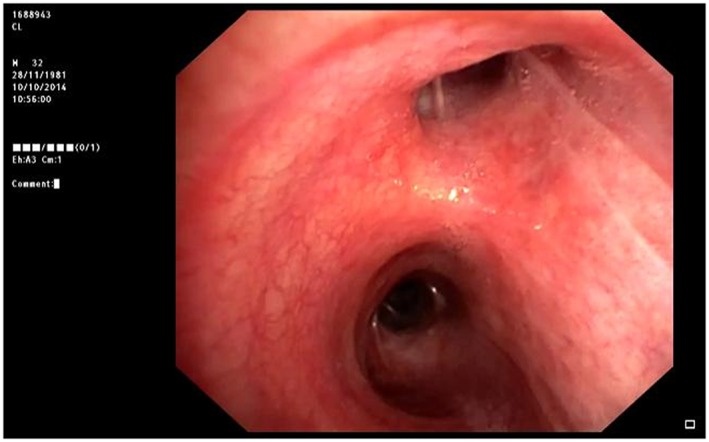
Bronchoscopy pictures immediately after exercise stress test.
Discussion
We described a rare phenomenon in humans that has been well recognised in thoroughbred horses in the past 1. There are now few reports of exercise‐induced pulmonary hemorrhage or exercise‐induced pulmonary oedema as we start to acknowledge the vulnerability of pulmonary capillaries to stress or mechanical failure during strenuous exercise and high cardiorespiratory workload 2, 3. West 4, 5 previously described the pathophysiology underlying this phenomenon. The pulmonary capillary blood–gas barrier, which is extremely thin in humans to allow for efficient gas exchange, and its collagen matrix are overcome by the extreme rise in pulmonary vascular pressure during intense exercise. His two experiments comparing brochoalveolar lavage samples between athletes undergoing intense exercise and sedentary subjects, and between athletes undergoing submaximal exercise and normal volunteers, confirmed higher concentrations of red blood cells, total protein, and leukotriene B4 in subjects with intense exercise. Thus, this suggested that the integrity of the capillary wall can be altered at extreme levels of exercise.
To our puzzle why then this phenomenon is not seen as often with so many athletes around the world. West 5 also proposed that pulmonary capillary remodeling may also occur, similar to the well‐known remodeling in the larger pulmonary vessels in pulmonary hypertension. His past animal experiments suggested increases in gene expression for extracellular matrix proteins and growth factors in the capillary wall. Whether this happens in humans who are repeatedly exposed to high levels of exercise remains a subject for further investigations.
The unique finding in the patient presented here did not have any evidence of alveolar opacities on radiology suggestive of pulmonary oedema as documented in other reports. However, bronchoscopy showed evidence of possible endobronchial bleeding. Moreover, another interesting finding in our patient is the previous Bleomycin therapy. Bleomycin can cause fatal pulmonary toxicity by inducing reactive oxygen radicals, which leads to capillary endothelial injury. It is not clear to our understanding if this contributed to his hemoptysis.
We hope this case will prompt other pulmonologists to share their experience for us to better understand pathophysiology and management strategies.
Disclosure Statements
No conflict of interest declared.
Appropriate written informed consent was obtained for publication of this case report and accompanying images.
Kruavit, A. , Jain, M. , Fielding, D. , and Heraganahally, S. (2016) Exercise‐induced endobronchial hemorrhage: a rare clinical presentation. Respirology Case Reports, 4 (4), e00163. doi: 10.1002/rcr2.163.
References
- 1. West JB, Mathieu‐Costello O, Jones JH, et al. 1993. Stress failure of pulmonary capillaries in racehorses with exercise‐induced pulmonary hemorrhage. J. Appl. Physiol. 75:1097–1109. [DOI] [PubMed] [Google Scholar]
- 2. Kim DS, Lee M, Kwon OJ, et al. 2015. A 45‐year‐old man with recurrent dyspnea and hemoptysis during exercise: exercise‐induced pulmonary hemorrhage/edema. Tuberc Respir Dis. 78:375–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Aversaa M, Lapinskyb SE. 2014. Lung physiology at play: hemoptysis due to underwater hockey. Respir Med Case Rep. 11:16–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. West JB. 2006. Vulnerability of pulmonary capillaries during severe exercise. Br. J. Sports Med. 40:821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. West JB. 2004. Vulnerability of pulmonary capillaries during exercise. Exerc. Sport Sci. Rev. 32:24–30. [DOI] [PubMed] [Google Scholar]