

Abstract
The use of semi-occluded vocal tract (SOVT) exercises as habilitative and rehabilitative tools has grown substantially in the past two decades. As the use or these exercises has grown, so too has the number of variations of the phonatory gestures used to create oral semi-occlusions. While much of the research on SOVT exercises to this point has been conducted using straw phonation, there has been little discussion or investigation regarding how other phonatory gestures that are considered to be SOVT compare to one another. The current study sought to measure the intraoral pressure produced by 13 phonatory gestures generally thought of as oral semi-occlusions. Twenty subjects (10 male, 10 female) produced three tokens of each gesture, and intraoral pressure was recorded via a thin, flexible-cannula pressure transducer. Pressures ranged between 0.1 and 1.0 kPa, but varied significantly between gestures and between subjects.
Keywords: Manometry, oral pressures, semi-occlusion, vocal tract
Introduction
Vocal exercises that utilize a semi-occlusion of the vocal tract (SOVT) have seen an increase in use in voice clinics and singing studios over the past several decades. Singing teachers frequently use nasal continuants /m/, /n/, and /ŋ/ to elicit sympathetic vibrations of facial tissues, which the singer can then associate with vocal tract shapes that are advantageous to a more strongly resonant vocal tone (1,2). Additionally, the use of lip trills and ‘raspberries’ to achieve similar ends has become common practice in singing studios of the Western classical music tradition (1,3). Similarly, speech language pathologists have adopted SOVT exercises into their clinical treatment of voice disorders. Indeed, entire therapy protocols such as Lessac Madsen resonant voice therapy (4), vocal function exercises (5), accent method (6), and resonance tubes (7) (later with soft-walled tubes—Lax Vox (8)) have been developed using a variety of SOVT gestures. Even those clinicians who do not utilize these therapies in their entirety still make use of SOVT exercises such as phonating through straws, nasal continuants, or similar phonatory gestures.
Vocal tract semi-occlusions can be formed by oral articulators (lips, tongue, or both) without an assistive device, or with a straw or tube inserted between the lips. Regardless of the nature of the occlusion, SOVT exercises are primarily used for the same general purposes of easing phonatory stresses exerted on the vocal folds and to encourage the development of a voice production that relies more heavily on source-filter interaction than on adductory stress to give the voice acoustic power. Several studies have been conducted to determine precisely what benefits SOVT exercises could be expected to have on vocal production. Tube phonation has been shown theoretically to result in an increased acoustic impedance of the vocal tract (9). In 2006, Titze further described the rationale and theoretical underpinnings for SOVT therapy (10). In this study, computer simulations indicated that semi-occlusions increase the interaction between the sound source and the vocal tract by increasing the mean intraglottal air pressure along with supraglottal pressures. Such an interaction, if in the correct proportions, may create a situation in which the maximum flow declination rate (MFDR) within the glottis is increased (11).
In human subjects studies, SOVT exercises have been found to improve perceived voice quality (12–15) and acoustic output (11, 13), though results relating to the underlying physiology of voice production have been variable. Guzman et al. also observed that SOVT exercises ‘produced a lower [vertical laryngeal position], narrower aryepiglottic opening, and a wider pharynx than resting position’ in 20 subjects with hyperfunctional dysphonia (16), while Laukkanen et al. noted an increase in thyroarytenoid activity relative to cricothryroid activity during and following SOVT exercises (17).
While the theoretical and anecdotal evidence of the usefulness of SOVT exercises in the voice clinic and singing studio is abundant and relatively clear, questions remain regarding which phonatory gestures are considered to be most effective as SOVT exercises. In particular, if the effectiveness of a SOVT gesture to reduce adductory stresses on the vocal folds is related to the supraglottal pressures the gesture produces, can oral occlusions be ranked according to their corresponding intraoral pressure? The current study sought to create such a rank ordering by measuring the intraoral pressure created by 13 semi-occlusions commonly used in SOVT exercises.
Methodology
Subjects
A total of 20 volunteers were recruited to participate in this study, 10 male and 10 female, ranging in age from 20 to 72 years old. Approval for this research was granted by an institutional review board, and each subject was informed of the procedure before consenting to participate in the study. It was anticipated that subjects who had previous singing training may be more skilled at regulating oral pressures. In order to track what effect singing training might have on oral pressures, volunteers were divided into two groups, singers (n = 10; 5 male, 5 female) and non-singers (n = 10; 5 male, 5 female), according to their experience with previous singing training. The threshold for inclusion in the singer group was a history of at least 1 year of singing instruction prior to their participation in the study. Inclusion criteria were healthy adults with normal voices and articulatory facilities necessary to produce all the required phonatory gestures. The exclusion criterion was a history of voice problems that might have been exacerbated by the study protocol. In the end, no subjects were excluded from the entire study. However, three subjects (2 female, 1 male) were unable to produce the raspberry (linguo-labial trill with the tongue extended between closed lips) and five subjects (3 female, 2 male) were unable to produce the tongue trill even after multiple attempts and coaching from the researcher. In these cases, averages were calculated using only data from those participants who could successfully produce the gesture. Table I represents the characteristics of each of the study participants, including a notation if a subject was unable to produce an exercise.
Table I.
Participant characteristics.
| Subject | Gender | Age | Singer (Y/N) | Unable to produce |
|---|---|---|---|---|
| F01 | Female | No response | N | Tongue trill |
| F02 | Female | 41 | Y | |
| F03 | Female | 29 | N | Raspberry, tongue trill |
| F04 | Female | 29 | N | |
| F05 | Female | 32 | N | |
| F06 | Female | 37 | Y | |
| F07 | Female | 21 | Y | |
| F08 | Female | 29 | N | Raspberry, tongue trill |
| F09 | Female | 29 | Y | |
| F10 | Female | 57 | Y | |
| M01 | Male | 23 | Y | |
| M02 | Male | 20 | N | Tongue trill |
| M03 | Male | 26 | N | |
| M04 | Male | 55 | Y | |
| M05 | Male | 42 | N | |
| M06 | Male | 35 | Y | |
| M07 | Male | 30 | Y | |
| M08 | Male | 30 | N | Tongue trill |
| M09 | Male | 71 | Y | |
| M10 | Male | 26 | N | Raspberry |
Equipment
Subjects were fitted with a head-mounted microphone (Countryman Isomax B3) and EGG collar (Kay Elemetrics Model 6103). A Glottal Enterprises PT-25 pressure transducer, connected to an MS-110 analog data and computer interface was used to measure intraoral pressures via an 8-cm length of flexible vinyl tubing (1 mm internal diameter, 3 mm external diameter), which was inserted into the oral cavity and positioned behind the semi-occlusion (Figure 1). An additional microphone was worn by the researcher to record instructions given to the subject. All data input signals were processed through a 16-channel analog-digital data acquisition device capable of DC measurements (ADInstruments Powerlab 16/30). This device was then connected via USB cable to a PC running ADInstruments LabChart7 software, with which all data were recorded in a proprietary format and stored for analysis.
Figure 1.

Pressure transducer with tubing inserted behind occlusion (shown here with small straw as occlusion).
Procedure
Once consent was obtained and subjects were fitted with the instrumentation described above, each subject performed two to three pitch glides and was instructed to stop at a ‘comfortable and repeatable’ pitch. That pitch was noted for each subject and was used for steady phonations throughout the protocol. Subjects were then asked to perform the following tasks with the mouth in an open /a/ vowel shape: 1) three pitch glide ‘sirens’ (gliding from the bottom of their pitch range to the top of their pitch range and returning to the bottom) at a comfortable loudness, 2) three sustained phonations held for 3–5 seconds on the comfortable pitch identified earlier and at a comfortable loudness, 3) one sustained phonation held for 3–5 seconds on the comfortable pitch and as softly as possible, and 4) one sustained phonation held for 3–5 seconds on the comfortable pitch and as loudly as possible (without causing discomfort). During these phonation tasks, the researcher was monitoring the subjects’ performance to ensure proper compliance with the protocol. If necessary, the subjects were given further guidance and tasks were repeated. Once the researcher was reasonably confident in the subjects’ ability to perform the vocal tasks accurately, the entire protocol was repeated for each of the following oral semi-occlusions: a thin stirring straw between the lips (3.5 mm internal diameter, 14.1 cm length; labeled ‘small straw’ in results), a drinking straw between the lips (6 mm internal diameter, 19.5 cm length; labeled ‘large straw’ in results), a long curved straw immersed in water (5 mm internal diameter, 1 cm external diameter, 36 cm length, 7 cm depth in water; labeled ‘straw in water’ in results), an /u/ vowel, voiced fricatives /β:/, /v/, /z/, and /3/, nasal consonants /m/ and /n/, a lip trill, a raspberry (lingo-labial trill), and a tongue trill. Care was taken throughout the recording process to ensure that the pressure transducer tubing was placed behind the semi-occlusion and remained unoccluded by the tongue or cheeks.
Analysis
Following the data collection, LabChart7 was used to extract mean intraoral pressures from the three repeated comfortable pitch/comfortable loudness phonations for each of the 13 occlusion gestures. Upon examination, it frequently appeared that intraoral pressures spiked just after onset of phonation before stabilizing at a somewhat lower level within 0.5 s. Since the aim of this study was to examine the intraoral pressures required to maintain phonation with semi-occlusions of the vocal tract, mean intraoral pressures were recorded from a 3-second section taken from the middle of the token.
Results
The mean intraoral pressures for all subjects are shown in Figure 2, with error bars representing the standard error. As expected, females produced lower pressures overall than males. However, with few exceptions, the average pressures were ranked in the same order for both genders. These results also show a considerable range of pressures being created by the different semi-occlusions. Male mean pressures ranged from 0.08 kPa (0.77 cmH2O) for the /m/ continuant to 1.08 kPa (11.13 cm H2O) for the straw in water. Mean female pressures ranged from 0.06 kPa (0.61 cm H2O) for the /n/ continuant to 0.8 kPa (8.23 cmH2O) for the straw in water. Individual pressures varied to an even greater extent, from 0.03 kPa (0.34 cmH2O) to 1.74 kPa (17.77 cmH2O) in males and from 0.03 kPa (0.35 cmH2O) to 1.15 kPa (11.69 cmH2O) in females. Additionally, as can be seen in Figure 2, relatively large standard errors resulted from the considerable differences in individual performance of each task.
Figure 2.
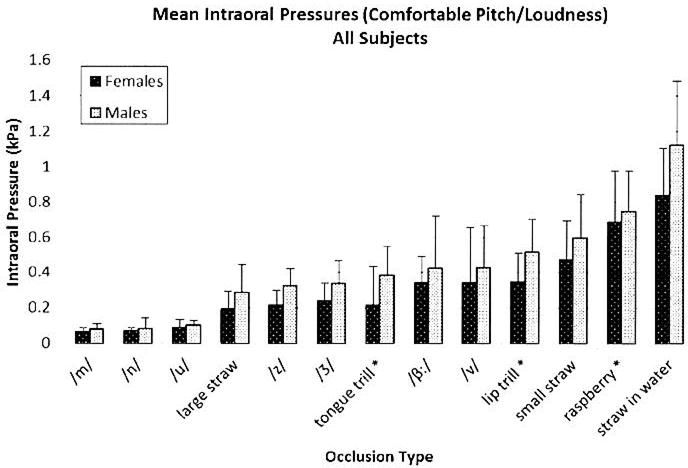
Mean intraoral pressure for all subjects (*indicates subjects had difficulty producing the semi-occlusion).
Figures 3 and 4 represent the male and female mean oral pressures, respectively, comparing singers to non-singers. There does appear to be differences between singers and non-singers; however, the standard errors would indicate that these differences may not have been significant in these subjects.
Figure 3.
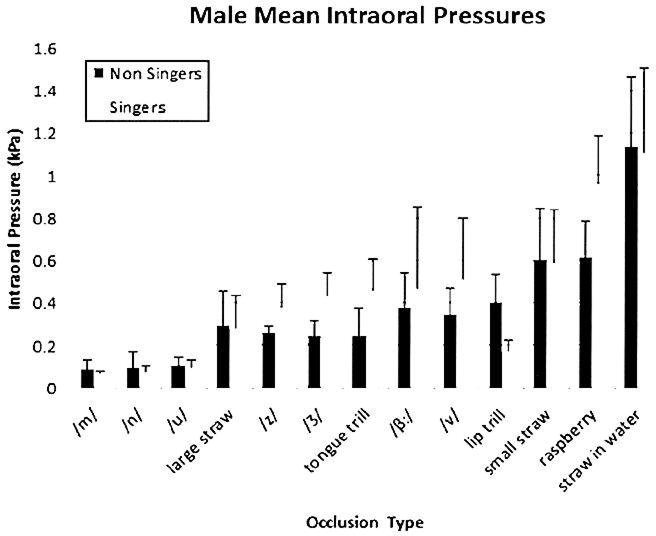
Male mean intraoral pressures, singers versus non-singers.
Figure 4.
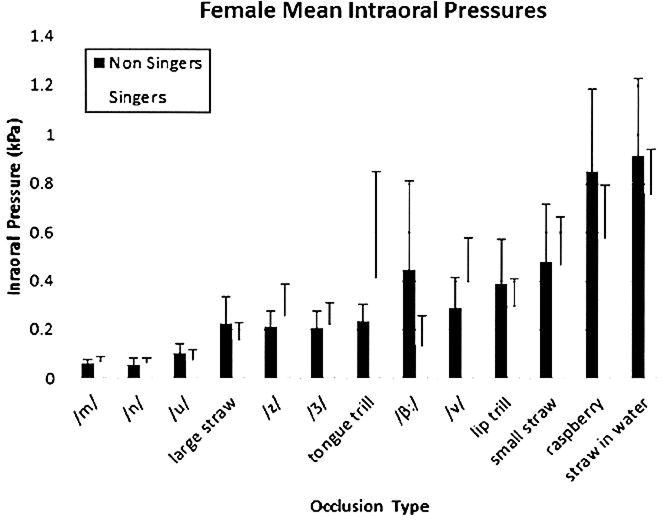
Female mean intraoral pressures, singers versus non-singers.
Discussion
Oral semi-occlusions designed for voice training and therapy produced intraoral pressures within a magnitude range of about 10:1 at comfortable lung pressures (Tables II and III). Nasal consonants (/m/ and /n/) produced only about half of the smallest pressures produced with oral semi-occlusions (e.g. straws, fricatives, and trills). With such a large magnitude range, there may be varied training efficacy within this large inventory of exercises.
Table II.
Female mean pressures and standard errors.
| Females (kPa) | All subjects
|
Non-singers
|
Singers
|
|||
|---|---|---|---|---|---|---|
| Avg | SD | Avg | SD | Avg | SD | |
| /m/ | 0.06882 | 0.018216 | 0.064843 | 0.015945 | 0.072797 | 0.019437 |
| /n/ | 0.062311 | 0.021496 | 0.059363 | 0.023394 | 0.065259 | 0.01896 |
| /u/ | 0.089218 | 0.042842 | 0.101841 | 0.037737 | 0.076595 | 0.043911 |
| Large straw | 0.192907 | 0.096332 | 0.226241 | 0.108673 | 0.159574 | 0.067288 |
| /z/ | 0.236588 | 0.103218 | 0.215216 | 0.060892 | 0.257959 | 0.129177 |
| /Ʒ/ | 0.216041 | 0.078364 | 0.207951 | 0.069365 | 0.224131 | 0.085671 |
| Tongue trill | 0.339722 | 0.317297 | 0.23557 | 0.069448 | 0.416089 | 0.437781 |
| Bilabial fricative | 0.214548 | 0.22327 | 0.44572 | 0.366307 | 0.137626 | 0.123106 |
| /v/ | 0.344737 | 0.164682 | 0.28906 | 0.123946 | 0.400413 | 0.178676 |
| Lip trill | 0.339692 | 0.154148 | 0.389057 | 0.182664 | 0.3002 | 0.112111 |
| Small straw | 0.474503 | 0.216933 | 0.48272 | 0.231978 | 0.466285 | 0.200428 |
| Raspberry | 0.683618 | 0.294121 | 0.851734 | 0.335881 | 0.57748 | 0.215192 |
| Straw in water | 0.839575 | 0.267563 | 0.920262 | 0.310219 | 0.758888 | 0.184182 |
Table III.
Male mean pressures and standard errors.
| Males (kPa) | All subjects
|
Non-singers
|
Singers
|
|||
|---|---|---|---|---|---|---|
| Avg | SD | Avg | SD | Avg | SD | |
| /m/ | 0.079372 | 0.03061 | 0.089436 | 0.040298 | 0.069308 | 0.006887 |
| /n/ | 0.085105 | 0.057577 | 0.09073 | 0.07653 | 0.07948 | 0.026648 |
| /u/ | 0.99855 | 0.028144 | 0.104565 | 0.040726 | 0.096974 | 0.031859 |
| Large straw | 0.286015 | 0.159608 | 0.292158 | 0.1649 | 0.279872 | 0.153888 |
| /z/ | 0.322738 | 0.097256 | 0.2621 | 0.029898 | 0.383375 | 0.103295 |
| /Ʒ/ | 0.337439 | 0.130202 | 0.243622 | 0.071525 | 0.431257 | 0.105763 |
| Tongue trill | 0.380012 | 0.167704 | 0.244698 | 0.130605 | 0.463165 | 0.14519 |
| Bilabial fricative | 0.422454 | 0.298852 | 0.379273 | 0.158474 | 0.465635 | 0.387017 |
| /v/ | 0.429702 | 0.235803 | 0.347575 | 0.122096 | 0.51183 | 0.287765 |
| Lip trill | 0.517554 | 0.18238 | 0.399124 | 0.131042 | 0.1732 | 0.051645 |
| Small straw | 0.596735 | 0.244192 | 0.599753 | 0.242704 | 0.593718 | 0.245633 |
| Raspberry | 0.74522 | 0.230041 | 0.618764 | 0.164493 | 0.964312 | 0.225224 |
| Straw in water | 1.123089 | 0.364047 | 1.139582 | 0.322701 | 1.106596 | 0.400475 |
The likely root cause of the large standard errors in the pressures reported above is differences in lung pressure between subjects. If lung pressure were measured for each of these semi-occlusions, a ratio of intraoral pressure to lung pressure would be a more accurate measure of the ability of these exercises to lower adductory stresses during phonation. Considering the standard errors, it is likely that a single semi-occlusion might well shift in the ranking by one or two positions up or down with the addition of more subjects or more repetitions. It appears unlikely, however, that the ranking would change significantly from this order.
The results also indicate that /m/, /n/, and /u/ produce quite low intraoral/supraglottal pressures. While singing teachers and clinicians may well find benefit from exercises incorporating these semi-occlusions, the current results seem to call into question whether or not those exercises fall into the same category as other SOVT exercises that produce higher intraoral pressures.
It also appears that singing training has some effect on intraoral pressures produced during SOVT phonation. Figures 3 (males) and 4 (females) show significant differences in pressures produced by singers versus non-singers for several of the occlusions. If it is desirable to find exercises that are effective for most individuals, regardless of their history of vocal training, finding exercises that produce pressures consistently across subjects with varied experience levels and training backgrounds is important. The results of this study seem to indicate that straw exercises do just that. Specifically, the 3.5 mm diameter straw between the lips (‘small straw’ in Figures) produced the most consistent pressures across subjects for both males and females. It is likely that straw exercises owe their pressure stability to the fact that they provide a semi-occlusion of fixed diameter and shape. All that the individual must do is ensure that the lips form a tight seal around the straw. This is in contrast to an exercise such as the lip trill or bilabial fricative /β:/, which can be greatly affected by the tightness with which the subject performs the exercise (18).
Why, then, does it appear that the ‘large straw’ failed to provide the same stability among females (Figure 4) that it provided among males (Figure 3)? This may be explained by the difference in dimensions of the glottis and vocal tract between males and females. In order to overcome the effects of vocal training, it appears that the semi-occlusion must provide resistance to the airflow at a level similar to that produced by the glottis itself. The large straw provided sufficient resistance in the males, whose mean glottal openings are larger and thus produce less resistance, but it failed to do so in females, whose mean glottal openings are smaller. Considering this difference between males and females, straws with diameters larger than 3.5 mm in air (i.e. not submerged in water, which would provide more resistance) may not produce the intraoral pressures desired for efficient and effective voice therapy.
Conclusion
This study provides data supporting a preliminary rank-ordering of SOVT exercises according to the intraoral pressures they produce during phonation. There is now evidence that, while many exercises can be considered to fall into the category of SOVT exercises, intraoral pressures vary significantly between them and between individuals, bringing into question their equality in treatment efficacy. In particular, the nasal continuants /m/ and /n/ produce very low intraoral pressures, possibly calling into question their inclusion in the SOVT category of vocal exercises. Phonation through thin tubes or straws that provide resistance comparable to or greater than glottal resistance may be one way to achieve adequate and somewhat controlled intraoral pressures during SOVT exercises.
Moving forward, a more accurate ordering may be created by taking into account the lung pressures that individual subjects are using to produce SOVT exercises. However, barring invasive measurements of lung pressure (e.g. tracheal puncture), the findings of this study provide a new lens through which clinicians may evaluate their own use of these exercises with their patients.
Acknowledgments
This work is partially supported by the National Institutes of Health (NIDCD grant number R01DC012045-01A). We are also happy to acknowledge the University of Utah’s Vice President of Research for continued support of the National Center for Voice and Speech.
Footnotes
Declaration of interest: The authors report no conflicts of interest.
References
- 1.Nix J. Lip trills and raspberries: “High spit factor” alternatives to the nasal continuant consonants. Journal of Singing. 1999;55:15–20. [Google Scholar]
- 2.Gregg J. From song to speech: what humming can do for you. Journal of Singing. 1996;52:37–52. [Google Scholar]
- 3.Titze I. Lip and tongue trills: what do they do for us. Journal of Singing. 1996;52:51–2. [Google Scholar]
- 4.Verdolini-Abbott K. Lessac Madsen resonant voice therapy clinician manual. San Diego, CA: Plural Publishing; 2008. [Google Scholar]
- 5.Stemple J. Vocal function exercises. San Diego, CA: Plural Publishing; 2006. [Google Scholar]
- 6.Kotby MN, Fex B. The accent method: behavior readjustment voice therapy. Logoped PhonatrVocol. 1998;23:39–43. [Google Scholar]
- 7.Simberg S, Laine A. The resonance tube method in voice therapy: description and practical implementations. Logoped Phonatr Vocol. 2007;32:165–70. doi: 10.1080/14015430701207790. [DOI] [PubMed] [Google Scholar]
- 8.Sihvo Deninoglu I. Lax vox voice therapy technique. Proceedings of the 7th Pan European Voice Conference; Groningen, Holland. Aug. 29 – Sep. 1, 2007; 2006. Abstract at: http://www.pevoc.org/pevoc07/index.htm. [Google Scholar]
- 9.Story BH, Laukkanen AM, Titze IR. Acoustic impedance of an artificially lengthened and constricted vocal tract. J Voice. 2000;14:455–69. doi: 10.1016/s0892-1997(00)80003-x. [DOI] [PubMed] [Google Scholar]
- 10.Titze IR. Voice training and therapy with a semi-occluded vocal tract: rationale and scientific underpinnings. J Speech Lang Hear Res. 2006;49:448–59. doi: 10.1044/1092-4388(2006/035). [DOI] [PubMed] [Google Scholar]
- 11.Titze IR. Theory of glottal airflow and source-filter interaction in speaking and singing. Acta Acustica Acustica. 2004;90:641–8. [Google Scholar]
- 12.Sampaio M, Oliveira G, Behlau M. Investigation of the immediate effects of two semi-ocluded vocal tract exercises. Pro Fono. 2008;20:261–6. doi: 10.1590/s0104-56872008000400010. [DOI] [PubMed] [Google Scholar]
- 13.Enflo L, Sundberg J, Romedahl C, McAllister A. Effects on vocal fold collision and phonation threshold pressure of resonance tube phonation with tube end in water. J Speech Lang Hear Res. 2013;56:1530–8. doi: 10.1044/1092-4388(2013/12-0040). [DOI] [PubMed] [Google Scholar]
- 14.Guzman M, Laukkanen AM, Krupa P, Horacek J, Svec JG, Geneid A. Vocal tract and glottal function during and after vocal exercising with resonance tube and straw. J Voice. 2013;27:523.e19–34. doi: 10.1016/j.jvoice.2013.02.007. [DOI] [PubMed] [Google Scholar]
- 15.Schwarz K, Cielo CA. Vocal and laryngeal modifications produced by the sonorous tongue vibration technique. Pro Fono. 2009;21:161–6. doi: 10.1590/s0104-56872009000200013. [DOI] [PubMed] [Google Scholar]
- 16.Guzman M, Castro C, Testart A, Munoz D, Gerhard J. Laryngeal and pharyngeal activity during semioccluded vocal tract postures in subjects diagnosed with hyperfunctional dysphonia. J Voice. 2013;27:709–16. doi: 10.1016/j.jvoice.2013.05.007. [DOI] [PubMed] [Google Scholar]
- 17.Laukkanen AM, Titze IR, Hoffman H, Finnegan E. Effects of a semioccluded vocal tract on laryngeal muscle activity and glottal adduction in a single female subject. Folio Phoniatr Logop. 2008;60:298–311. doi: 10.1159/000170080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Laukkanen A. Voiced bilabial fricative /ß:/ as a vocal exercise. Scandinavian Journal of Logopedics and Phoniatrics. 1992;17:181–9. [Google Scholar]