

Abstract
Purpose
We assessed the application of the choroidal vascularity index (CVI) in the follow-up of Vogt-Koyanagi-Harada disease (VKH) patients derived from image binarization of enhanced depth imaging optical coherence tomography (EDI-OCT) images with Fiji software. Our secondary objective was to derive the retinochoroidal vascularity index based on en face fundus fluorescein and indocyanine green angiography (FFA and ICGA).
Methods
In this retrospective cohort study, EDI-OCT scans of 18 eyes of 9 patients with VKH were obtained at baseline within 2 weeks of acute presentation, and again at 6 to 12 months. Images with poor quality were excluded. Choroidal thickness (CT) and CVI were analyzed and compared to 13 eyes of 13 healthy controls. En face FFA and ICGA obtained from 12 eyes of 7 patients were segmented to derive retinochoroidal vascularity index.
Results
There was no statistical difference in age or sex between the study group and controls. Choroidal thickness of patients with VKH was 359.23 ± 57.63 μm at baseline, compared to 274.09 ± 56.98 μm in controls (P = 0.003). Follow-up CT in VKH patients was 282.62 ± 42.51 μm, which was significantly decreased from baseline (P = 0.0001). Choroidal vascularity index in VKH patients was 70.03 ± 1.93% at baseline, compared to 64.63 ± 1.92% in controls (P < 0.001). Choroidal vascularity index was 66.94 ± 1.82% at follow-up, significantly reduced from baseline (P < 0.0001). Fundus fluorescein angiography and ICGA retinochoroidal vascularity indices at baseline were 70.67 ± 2.65% and 66.42 ± 2.16%, respectively.
Conclusions
In this small series of VKH patients, EDI-OCT–derived CVI had a statistically significant reduction over time, similar to CT. We propose that OCT, FFA, and ICGA-derived vascularity indices may be potential novel supportive tools in monitoring disease progression in VKH.
Translational Relevance
Choroidal vascularity index can be used potentially to study and analyze the structural changes in choroid. It can be a useful tool to explain the changes in the CT in different retinochoroidal disorders. Choroidal vascularity index also can be used for longitudinal follow-up in patients with VKH disease and other inflammatory disease involving the choroid.
Keywords: optical coherence tomography, image analysis, choroid, Vogt-Koyanagi-Harada disease
Introduction
Vogt-Koyanagi-Harada (VKH) disease is a systemic autoimmune disorder that affects pigmented tissues.1 It manifests in the eye as bilateral panuveitis with characteristic serous retinal detachments, with or without systemic involvement of the auditory, cutaneous, or central nervous systems. It is thought to be a T-cell–mediated process directed against melanocytes.2 Pathologically, it affects the choroid, and evidence of diffuse choroiditis is one of the criteria for diagnosis of VKH described in the revised diagnostic criteria for VKH disease, manifesting as focal areas of subretinal fluid or with bullous serous retinal detachments.3
The imaging modalities commonly used in the diagnosis and follow-up of VKH are: fundus fluorescein angiography (FFA), indocyanine green angiography (ICGA), and optical coherence tomography (OCT).4 Angiography produces characteristic patterns of fluorescence, while providing an indication of disease activity. The ICGA scans are useful in evaluating choroidal inflammatory disorders.5 However, FFA and ICGA are invasive in nature, with inherent risks of intravenous administration of the dyes.
The advent and advancement of OCT and autofluorescence have allowed more in-depth analyses of the vitreous, retina, and choroid in a noninvasive manner. Optical coherence tomography can provide real time optical cross-sections of the retina, retinal pigment epithelium (RPE), and measure choroidal thickness (CT) as well.6 Further advances in technology with enhanced depth imaging (EDI)–OCT scans provide more insight into qualifiable and quantifiable measurements of choroidal vasculature and other volumetric data in patients with panuveitis.7–17
Numerous studies have been published with CT as the denominator for disease activity in VKH. However, CT may not be a robust tool in clinical research given that many ocular and systemic factors affect the thickness of the choroid.15 We do not know which structures within the choroid constitute increased thickness in patients with VKH and what happens to those structures with disease progression or resolution. Hence, it is imperative to explore and measure novel indices in the choroid and retina, which potentially can be used to monitor disease progression.
We investigated the use of image binarization cross-sectional EDI-OCT as well as enface FFA and ICGA scans and scans using semiautomated software in patients with VKH.
Methods
This was a retrospective cohort study in patients with VKH disease seen at a tertiary referral eye care center in Southern India by a single uveitis specialist (PM) between 2011 and 2013. Inclusion criteria were as follows: EDI-OCT scan obtained within 2 weeks of initial acute presentation, minimum follow-up of 3 months, refractive error not higher than −3.00 diopters (as patients with higher myopia may have a thinner choroid and can be a confounder for CT assessment). Local ethics board approval was obtained to analyze the images using public domain software (available in the public domain at Fiji; http://imagej.nih.gov/ij, version 2.0.0-rc.15/1.49j, date: 2014-10-06).18 The research was conducted in accordance with the tenets set forth in the Declaration of Helsinki.
Age, sex, visual acuity, refractive error, vitreous haze, EDI-OCT scans, FFA, and ICGA scans, medications administered, and follow-up details were recorded on a precoded anonymized data collection sheet (Supplementary Form S1).
Optical coherence tomography images were obtained using the Spectralis OCT device (Spectralis; Heidelberg Engineering; Heidelberg, Germany) and using the EDI protocol first described by Spaide et al.6 The OCT device was positioned in close proximity to the patient's eye to acquire an inverted image, and 11 equally-spaced OCT B-scan sections were obtained in a 20° × 15° horizontal raster pattern. The CT was measured manually using the in-built calipers tool at 3 points (subfoveal, 500 μm temporal and nasal to the fovea). The CT was defined as the vertical distance between the outer surface of the RPE to the choroidal-scleral interface (CSI).
Binarization of EDI-OCT Images
The central scan passing through the foveal/subfoveal region was selected and one image per patient per visit was used for analysis. The protocol proposed by Sonada et al.19 was used for binarization of the entire choroidal area in that scan. Under this protocol, images were analyzed using public domain software Fiji.
After uploading the image on Fiji, the polygon tool was used to select the region of interest (ROI). The upper boundary of the ROI was traced along the choroid-RPE junction and the lower boundary along the CSI (Figs. 1A, 2A). Lower resolution poor quality EDI-OCT scans with inconspicuous CSI were not binarized and those eyes were excluded from the analysis. To binarize the image, it was further converted to 8-bit images to allow the application of auto threshold (Fig. 1B). Brightness was reduced to clearly visualize the choroidal vessels and also to minimize the noise in the EDI-OCT images.
Figure 1.
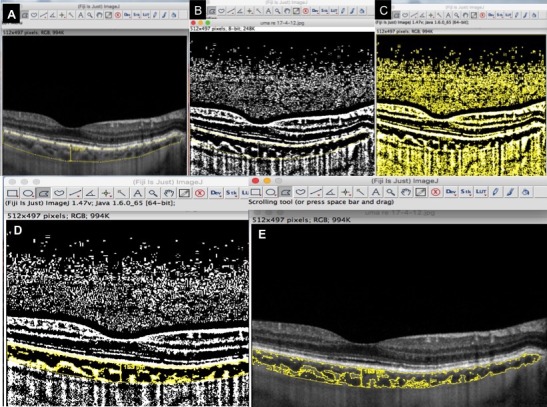
Step-by-step illustrations of image binarization using Image J software and the Niblack image binarization technique. Step-by-step illustrations of image segmentation using the Niblack image binarizaton technique. (A) Manual segmentation of the choroid using the polygon tool on Image J. (B) Conversion to 8 bit image for application of auto local threshold. (C) Niblack autolocal threshold used to get clear segmentation of black and white areas on the choroid. (D) Image after the image binarization was done and when image was reconverted back to RGB image. (E) Superimposed image of binarized segment over the original EDI-OCT scan.
Figure 2.
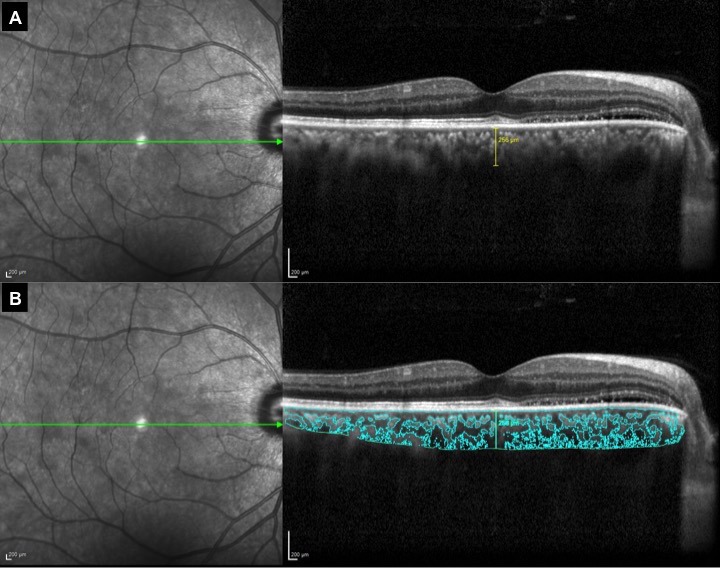
Enhanced depth imaging OCT scans of eyes with VKH before (A) and after (B) binarization using the Niblack auto local thresholding technique on Image J software.
Niblack's auto local threshold tool was applied to give best resolution and demarcation of luminal (vascular) area (LA) and stromal (interstitial) area (SA; Fig. 1C). The image adjusted by auto local threshold was again converted back to an red, green, blue (RGB) image and the luminal area was determined using the color threshold tool (Fig. 1D). Choroidal vascularity index (CVI), defined as the proportion of luminal area to total choroidal area, was computed for all the images at baseline and follow-up. A superimposed image of the binarized segment over the conventional EDI-OCT scan represents the optically segmented choroid and its two components, that is, vascular and stromal area (Figs. 1E, 2B). Figures 2 and 3 illustrate the pre- and postbinarized image of a patient with resolving VKH.
Figure 3.
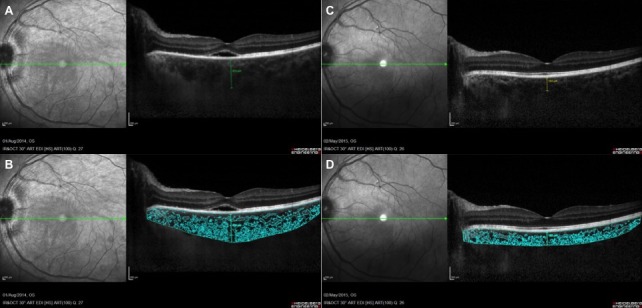
Pre- and postbinarized image for one study patient. (A) Visibly thickened choroid on EDI-OCT scan. (B) Segmented image illustrating the choroidal vasculature and stroma at baseline. (C) Illustrates the EDI-OCT scan at 11-month follow-up. (D) Segmented image at follow-up.
Binarization of FFA and ICGA Images
Mid phase FFA and ICGA scans also were segmented using Niblack auto local threshold technique. Regions of interest using a circle with a radius of 1500 μm centered at the fovea was created for computing retinochoroidal vascularity index on enface FFA scans and CVI on en face ICGA scans. Regions of interest were kept the same for FFA and ICGA scans. The proportion of thresholded area (vascular luminal area) to the total area of ROI provided the vascularity indices for FFA and ICGA scans (Fig. 4).
Figure 4.
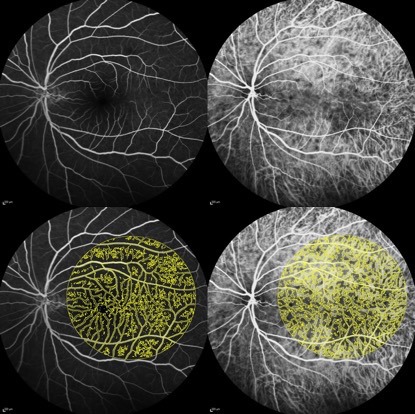
Fundus fluorescein angiography (left) and ICGA (right) enface scans in mid phase with image binarization using Niblack auto local threshold technique on Image J software.
Statistical Analysis
For statistical analysis, eyes with VKH were considered as the study group and eyes from healthy controls were considered as the control group. Qualitative imaging data were analyzed with frequency and descriptive statistics. Quantitative CT measurements at two separate visits 6 months apart were analyzed statistically using the Wilcoxon sign rank test and a P value of <0.05 was considered statistically significant. Using the unpaired t-test and by comparing CT and CVI with the control group, the correlation between the study and control groups was calculated. The ANOVA test was used to compare the variance in means at two different time points, and also to analyze the variance in the means among study eyes and control eyes. Statistical analysis was performed using commercially available software (Intercooled STATA for Windows Version 13; Stata Corp, College Station, TX).
Results
Nine patients (18 eyes) with VKH were included in our study. One image was of poor quality and, hence, excluded. A total of 17 EDI-OCT scans from nine patients were evaluated and compared to EDI-OCT scans from 13 eyes of 13 healthy controls. As the baseline EDI-OCT scans at presentation were nonrecordable due to the severely thickened choroid, we evaluated EDI-OCT scans obtained within 2 weeks of presentation as baseline scans. Only 16 VKH eyes had good quality follow-up EDI-OCT scans at approximately 6 to 12 months, which were segmented to compute CVI. En face FFA and ICGA scans from 12 eyes of seven patients at baseline were binarized. Mean age of the study group was 42 ± 12.96 years (range, 21–55), while mean age of the control group was 32.13 ± 10.37 years (range, 18–60), with no statistically significant difference between both groups (P = 0.171). There were five (55.55%) females in the study group and six (46.15%) in the control group. All patients in the study group received pulse intravenous methylprednisolone followed by oral corticosteroids at 1 mg/kg/day in tapering doses and four (44%) patients had additional immunosuppression. Of the four patients, two had oral methotrexate and two had oral azathioprine, which was started concurrently with oral corticosteroids.
Choroidal Thickness
Choroidal thickness of patients with VKH was 359.23 ± 57.63 μm (229–473 μm) at baseline, which was statistically different from CT in controls (274.09 ± 56.98; range, 209–376 μm; P = 0.003). Follow-up CT in VKH patients was 282.62 ± 42.51 (228–370) μm, which was significantly decreased from baseline (P = 0.0001). Composite box plots are demonstrated in Figures 5A and 5B.
Figure 5.
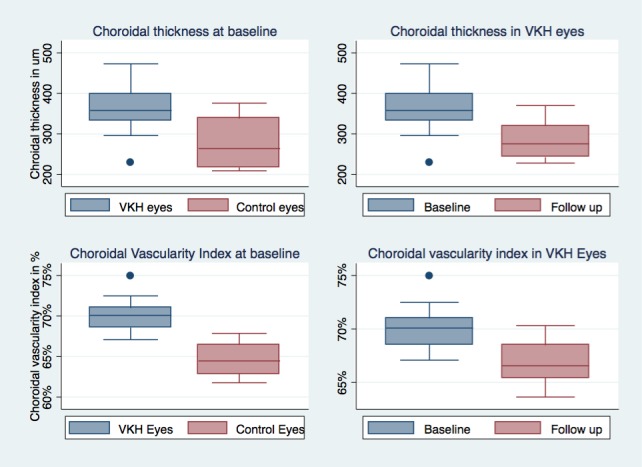
Composite box plots. (A) Comparing CT in VKH eyes compared to controls as baseline. (B) Comparing CT in VKH eyes at baseline and at 3–6 months. (C) Comparing CVI in VKH eyes compared to controls as baseline. (D) Comparing CVI in VKH eyes at baseline and at 3–6 months
Choroidal Vascularity Index
Choroidal vascularity index in VKH patients was 70.03 ± 1.93% (67.08%–74.98%) at baseline, while CVI in the control group was 64.63 ± 1.92% (61.76%–67.85%; P < 0.001; effect size, 5.53). Choroidal vascularity index was 66.94 ± 1.82% (63.63%–70.31%; P < 0.0001; effect size, 3.01) at follow-up. Composite box plots are demonstrated in Figures 5C and 5D. Fundus fluorescein angiography and ICGA–derived retinochoroidal vascularity indices were 70.67 ± 2.65% (64.95%–75.09%) and 66.42 ± 2.16% (61.6%–69.4%), respectively, at baseline. As we did not have any FFA and ICGA images for normal (control) subjects, we could not compare the retinochoroidal vascularity indices between the two groups. Also, no patient had follow-up FFA and ICGA, and, hence, we could not establish the follow-up measurements for retinochoroidal vascularity index in this study cohort.
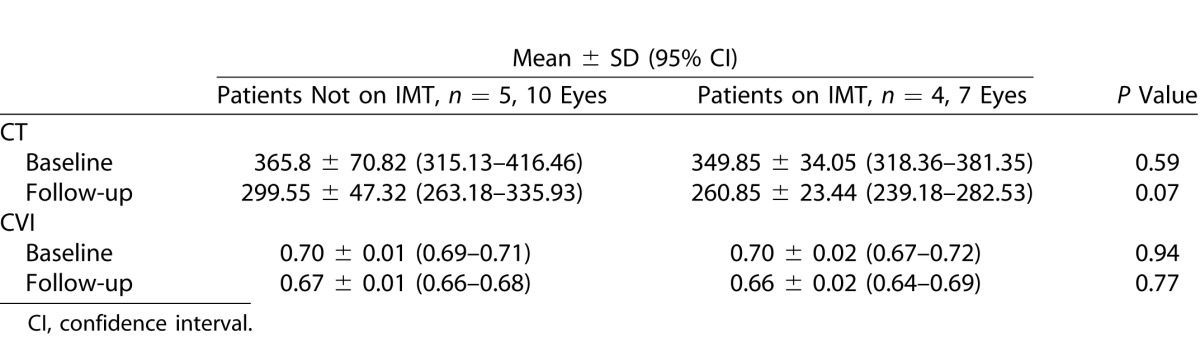
Immunomodulatory Therapy (IMT)
A subgroup analysis was done for four patients (seven eyes) on IMT in comparison with the subjects only on oral corticosteroids. There was no statistically significant difference between the CT and CVI at baseline for the patients on and not on IMT. At follow-up, there again was no statistically significant difference in the patients on IMT for CT and CVI.
Discussion
Segmentation of the choroid in different layers and its vascular components is a significant challenge for all researchers. Automated segmentation software and algorithms have been developed, mainly in the measurement of CT.15,17,20,21 However, further precision and validation is warranted for wider application of this technology in a variety of ocular pathologies.
Our most significant finding was that there were statistically significant changes in CVI in VKH patients at follow-up when compared to baseline. This similarly was found when evaluating the change in CT over the same period. We believe that CVI may be an exciting novel supportive tool in monitoring disease progression in VKH. Other studies have reported correlation of CT with VKH disease progression, with rapid reduction of CT upon initiation of corticosteroids, while increased thickening may indicate recurrence of subclinical disease.22,23 In our study, good quality EDI-OCT scans were difficult to obtain at initial presentation, due to the presence of serous detachments and a grossly thickened choroid. This is similar to other studies, where it was found that the outer border of the choroid might not be evident at initial presentation, but subsequently measureable by 1 week.24
While CT is useful for monitoring initial response to treatment in VKH patients, it may not be a robust tool for the evaluation of residual disease activity at further follow-up over a longer period. Patients with VKH and long-standing disease had thinner choroids when compared to controls, with progressive choroidal thinning related to disease duration.13,25,26 Progression to a sunset glow fundus may indicate underlying subclinical activity that is not detected by follow-up of CT which is progressively reducing over time. Choroidal thickness also is significantly affected by age, sex, and axial length.15 It is likely that because CVI is a ratio, it will be less easily affected by these potential confounding factors. These factors further highlight the importance of the evaluation of other methods to monitor underlying choroidal inflammation and disease activity. In future studies, it may be interesting to evaluate CVI of VKH patients in convalescent disease, and to investigate the correlation of CVI to progressive thinning of the choroid over time.
Evaluation of CVI may enhance our understanding of the pathophysiology of VKH. Typical histopathologic features of VKH include granulomatous panuveitis with preservation of the choriocapillaris, as well as diffuse infiltration of lymphocytes with focal granulomas in the choroidal stroma.27 We found that CVI was significantly higher in VKH eyes at acute presentation, compared to control eyes. This indicates that there is a possible greater vascularity in VKH eyes compared to controls, likely contributing to the increased CT. However, as EDI-OCT is a static image, this does not bear any indication on the velocity of blood flow within the choroid, but rather an increased ratio of the area of vessels compared to the stroma. In fact, choroidal inflammation may result in impaired choroidal blood flow to the macula, which improves with corticosteroid treatment up to several months after treatment.28,29 The higher CVI and, hence, increased vascularity may be an indirect indicator suggestive of stasis of blood flow in the choroid due to the impaired choroidal blood flow. However, at this stage, there are no dynamic measurements using our proposed CVI tool and it merely provides a static two-dimensional measurement of the black and white areas of the choroid.
Further attempts were made to demonstrate this increased vascularity by the segmentation of en face mid phase FFA and ICGA. However, we were not able to compare these values with controls. Indocyanine green angiography is very useful in the evaluation of choroidal inflammation and vascularity in VKH.5,30 It also is able to detect the presence of smouldering subclinical disease which may persist.31 However, due to variable interpretation and its invasive nature, it is less preferred as a tool among clinicians. Indocyanine green angiography also does not allow for cross-sectional analysis of the choroid, with an inability to provide a quantifiable measure of vascularity. In this study, we were able to use a relatively novel way to segment the vasculature of the choroid on a single en face scan and compute the vascularity indices for choroidal vasculature on ICGA and retinochoroidal vasculature on FFA. In this way, we may be able to increase the usefulness of ICGA in providing an objective quantifiable measure to follow-up VKH patients, or in other patients with posterior uveitis.
Our study had several limitations. We have a small sample size, and interrater agreement and intersession agreement of CVI was not performed in this series to validate the results. Nevertheless, the method of binarization we used had good repeatability and reproducibility.19 In this study, we also did not compare this tool with other inflammatory biomarkers, such as vitreous haze.
There also are several difficulties to be encountered when following a patient with CVI. The measurement of CVI sometimes may be difficult, as it requires the acquisition of good quality EDI-OCT scans. Accurate binarization may be challenging in acute inflammatory disease, where there may be media opacity, vitritis, or retinal lesions causing artifacts. In our study, we had to exclude several scans due to poor quality, resulting in an inability to segment the image. Choroidal vascularity index values are not as readily obtained compared to measuring CT, due to the manual binarization process. In the future, the development of automated segmentation software may eliminate this problem. With regards to segmentation of FFA and ICGA, it would be difficult to standardize the phase at which subsequent follow-up images are captured to enable accurate comparison. This may limit the repeatability of this method for the follow-up of patients.
Other studies also have attempted segmentation of the choroid and evaluation of vascularity via various methods.32,33 Branchini et al.33 reported the evaluation of choroidal morphology and thickness of Haller's layer compared to the choriocapillaris in combination with Sattler's layer. In future studies, possible advances in segmentation techniques may enable us to evaluate the various layers of the choroid vasculature separately, and as a result further elucidate the pathophysiology of choroidal involvement in VKH as well as a variety of ocular diseases.
In conclusion, we proposed that EDI-OCT–derived CVI as well as FFA and ICGA-derived vascularity indices may be potential novel supportive tools in monitoring disease progression in VKH. Further large population-based cross-sectional and longitudinal comparative studies in VKH and other ocular diseases are warranted to validate the application of CVI as a robust and reliable biomarker for diseases affecting choroid.
Table 1.
Correlation of CVI and CT in Patients on IMT
Supplementary Material
References
- 1. Sakata VM,, da Silva FT,, Hirata CE,, de Carvalho JF,, Yamamoto JH. Diagnosis and classification of Vogt-Koyanagi-Harada disease. Autoimmun Rev. 2014; 13: 550–555. [DOI] [PubMed] [Google Scholar]
- 2. Greco A,, Fusconi M,, Gallo A,, et al. Vogt-Koyanagi-Harada syndrome. Autoimmun Rev. 2013; 12: 1033–1038. [DOI] [PubMed] [Google Scholar]
- 3. Read RW,, Holland GN,, Rao NA,, et al. Revised diagnostic criteria for Vogt-Koyanagi-Harada disease: report of an international committee on nomenclature. Am J Ophthalmol. 2001; 131: 647–652. [DOI] [PubMed] [Google Scholar]
- 4. Gallagher MJ,, Yilmaz T,, Cervantes-Castaneda RA,, Foster CS. The characteristic features of optical coherence tomography in posterior uveitis. Br J Ophthalmol. 2007; 91: 1680–1685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Agrawal RV,, Biswas J,, Gunasekaran D. Indocyanine green angiography in posterior uveitis. Indian J Ophthalmol. 2013; 61: 148–159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Spaide RF,, Koizumi H,, Pozzoni MC. Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol. 2008; 146: 496–500. [DOI] [PubMed] [Google Scholar]
- 7. Karampelas M,, Sim DA,, Keane PA,, et al. Choroidal assessment in idiopathic panuveitis using optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2013; 251: 2029–2036. [DOI] [PubMed] [Google Scholar]
- 8. Keane PA,, Sadda SR. Imaging chorioretinal vascular disease. Eye. 2010; 24: 422–427. [DOI] [PubMed] [Google Scholar]
- 9. Keane PA,, Allie M,, Turner SJ,, et al. Characterization of birdshot chorioretinopathy using extramacular enhanced depth optical coherence tomography. JAMA Ophthalmol. 2013; 131: 341–350. [DOI] [PubMed] [Google Scholar]
- 10. Zarranz-Ventura J,, Sim DA,, Keane PA,, et al. Characterization of punctate inner choroidopathy using enhanced depth imaging optical coherence tomography. Ophthalmology. 2014; 121: 1790–1797. [DOI] [PubMed] [Google Scholar]
- 11. Mahendradas P,, Madhu S,, Kawali A,, et al. Combined depth imaging of choroid in uveitis. J Ophthalmic Inflamm Infect. 2014; 4: 18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Bittencourt M,, Kherani S,, Ferraz DA,, et al. Variation of choroidal thickness and vessel diameter in patients with posteiro non-infectious uveitis. J Ophthalmic Inflamm Infect. 2014; 4: 14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Nazari H,, Hariri A,, Hu Z,, Ouyang Y,, Sadda S,, Rao NA. Choroidal atrophy and loss of choriocapillaris in convalescent stage of Vogt-Koyanagi-Harada disease: in vivo documentation. J Ophthalmic Inflamm Infect. 2014; 4: 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Staurenghi G,, Sadda S,, Chakravarthy U,, Spaide RF. International Nomenclature for Optical Coherence Tomography P. Proposed lexicon for anatomic landmarks in normal posterior segment spectral-domain optical coherence tomography: the IN*OCT consensus. Ophthalmology. 2014; 121: 1572–1578. [DOI] [PubMed] [Google Scholar]
- 15. Gupta P,, Jing T,, Marziliano P,, et al. Distribution and determinants of choroidal thickness and volume using automated segmentation software in a population-based study. Am J Ophthalmol. 2015; 159: 293–301. [DOI] [PubMed] [Google Scholar]
- 16. Gupta P,, Sidhartha E,, Girard MJ,, Mari JM,, Wong TY,, Cheng CY. A simplified method to measure choroidal thickness using adaptive compensation in enhanced depth imaging optical coherence tomography. PloS One. 2014; 9: e96661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Mahajan NR,, Donapati RC,, Channappayya SS,, Vanjari S,, Richhariya A,, Chhablani J. An automated algorithm for blood vessel count and area measurement in 2-D choroidal scan images. Conf Proc IEEE Eng Med Biol Soc. 2013; 2013: 3355–3358. [DOI] [PubMed] [Google Scholar]
- 18. Schindelin J,, Arganda-Carreras I,, Frise E,, et al. Fiji: an open-source platform for biological-image analysis. Nat Methods. 2012; 9: 676–682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Sonoda S,, Sakamoto T,, Yamashita T,, et al. Choroidal structure in normal eyes and after photodynamic therapy determined by binarization of optical coherence tomographic images. Invest Ophthalmol Vis Sci. 2014; 55: 3893–3899. [DOI] [PubMed] [Google Scholar]
- 20. Beaton L,, Mazzaferri J,, Lalonde F,, Hidalgo-Aguirre M,, Descovich D,, Lesk MR,, Costantino S. Non-invasive measurement of choroidal volume change and ocular rigidity through automated segmentation of high-speed OCT imaging. Biomed Opt Express. 2015; 6: 1694–1706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Zhang L,, Buitendijk GH,, Lee K,, et al. Validity of automated choroidal segmentation in SS-OCT and SD-OCT. Invest Ophthalmol Vis Sci. 2015; 56: 3202–3211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Maruko I,, Iida T,, Sugano Y,, et al. Subfoveal choroidal thickness after treatment of Vogt-Koyanagi-Harada disease. Retina. 2011; 31: 510–517. [DOI] [PubMed] [Google Scholar]
- 23. Nakai K,, Gomi F,, Ikuno Y,, et al. Choroidal observations in Vogt-Koyanagi-Harada disease using high-penetration optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2012; 250: 1089–1095. [DOI] [PubMed] [Google Scholar]
- 24. Nakayama M,, Keino H,, Okada AA,, et al. Enhanced depth imaging optical coherence tomography of the choroid in Vogt-Koyanagi-Harada disease. Retina. 2012; 320: 2061–2069. [DOI] [PubMed] [Google Scholar]
- 25. da Silva FT,, Sakata VM,, Nakashima A,, et al. Enhanced depth imaging optical coherence tomography in long-standing Vogt-Koyanagi-Harada disease. Br J Ophthalmol. 2013; 97: 70–74. [DOI] [PubMed] [Google Scholar]
- 26. Takahashi H,, Takase H,, Ishizuka A,, et al. Choroidal thickness in convalescent Vogt-Koyanagi-Harada disease. Retina. 2014; 34: 775–780. [DOI] [PubMed] [Google Scholar]
- 27. Rao NA. Pathology of Vogt-Koyanagi-Harada disease. Int Ophthalmol. 2007; 27: 81–85. [DOI] [PubMed] [Google Scholar]
- 28. Hirose S,, Saito W,, Yoshida K,, et al. Elevated choroidal blood flow velocity during systemic corticosteroid therapy in Vogt-Koyanagi-Harada disease. Acta Ophthalmol. 2008; 86: 902–907. [DOI] [PubMed] [Google Scholar]
- 29. Hirooka K,, Saito W,, Namba K,, et al. Relationship between choroidal blood flow velocity and choroidal thickness during systemic corticosteroid therapy for Vogt-Koyanagi-Harada disease. Graefes Arch Clin Exp Ophthalmol. 2015; 253: 609–617. [DOI] [PubMed] [Google Scholar]
- 30. Bouchenaki N,, Herbort CP. The contribution of indocyanine green angiography to the appraisal and management of Vogt-Koyanagi-Harada disease. Ophthalmology. 2001; 108: 54–64. [DOI] [PubMed] [Google Scholar]
- 31. Herbort CP,, Mantovani A,, Bouchenaki N. Indocyanine green angiography in Vogt-Koyanagi-Harada disease: angiographic signs and utility in patient follow-up. Int Ophthalmol. 2007; 27: 173–182. [DOI] [PubMed] [Google Scholar]
- 32. Sohrab M,, Wu K,, Fawzi AA. A pilot study of morphometric analysis of choroidal vasculature in vivo using en face optical coherence tomography. PloS One 2012; 7: e48631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Branchini LA,, Adhi M,, Regatieri CV,, et al. Analysis of choroidal morphologic features and vasculature in healthy eyes using spectral-domain optical coherence tomography. Ophthalmology. 2013; 120: 1901–1908. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.