

Abstract
Background
The concept of shared decision making (SDM) has been developing in many countries since the 1990s. The main challenge of SDM, based on the principles of respect for the person’s autonomy, is to improve patients’ participation, should they so wish, in decisions concerning their personal health. To our knowledge, there is only one SDM evaluation tool validated in metropolitan French that does not measure the entire SDM construct. The aim of this review was to identify existing and validated SDM measurement tools to determine which of them could be adapted in French to cover all the dimensions of SDM.
Methods
A systematic literature review was conducted based on articles found in the PubMed and PsycINFO bibliographic databases and published between 2010 and 2014. Studies were included if the main goal of the article was the development and psychometric validation of an SDM measurement tool, not specific to any given disease or situation, in English, French and Spanish. We used the nine essential elements of the Makoul and Clayman’s integrative model to describe the different existing tools.
Results
Nineteen studies were included. Seven new tools had been published since Scholl’s previous review in 2011. We observed a recent spread of the multi-appraiser approach, which combines points of view of patients, healthcare professionals and sometimes external observers. Several models were used for the development of the seven newly identified tools. None of the identified tools assessed the nine elements of the Makoul’s model. Three of these elements, however, were systematically measured in each of the new tools: “defining/explaining the problem”, “patient values/preferences”, and “checking/clarifying understanding”.
Conclusions
We identified several potentially interesting tools for the French context which could cover the whole elements of Makoul’s model. The next step will be the development of a French-language instrument based on these tools.
Electronic supplementary material
The online version of this article (doi:10.1186/s13104-016-2164-6) contains supplementary material, which is available to authorized users.
Keywords: Shared decision making, Patient involvement, Measurement, Questionnaire, Methodology, Systematic review
Background
The concept of shared decision making (SDM) has been developing both in France [1] and in Anglo-Saxon countries [2] since the 1990s. This concept describes the process during which a decision concerning a patient’s health must be made using a decision making model consisting of two key steps in the relationship between a healthcare professional and a patient: information exchange and deliberation, before making a mutually accepted decision [2]. The healthcare professional and patient share medical information, in particular scientific evidence, and the patient receives the support required to express his/her preferences and to consider the various healthcare-related options, in order to reach an informed joint decision [3, 4].
In France, patients’ demand for information and participation in medical decision were introduced in the eighties by AIDS associations, then reinforced by the tainted blood scandal and in the nineties by cancer patients’ associations [5]. These movements are commonly associated with the rise of what has been called in France ‘‘Democracy in healthcare’’, a concept originating from the growing awareness of the civil society [6]. In the French context, while the Patients’ rights healthcare system quality act of 04 March, 2002 introduced the notion of a patient’s right to know and to decide [1], effective patient participation in SDM remains one of the stakes highlighted in 2013 by the HAS (Haute Autorité de Santé, French National Authority for Health) in a guide entitled “Patient and healthcare professionals: deciding together” [2]. Moreover, SDM represents a growing research field and increasing interest for French research teams. Indeed some studies have been conducted in France and papers published both at the national and international level. They were conducted by multidisciplinary research groups, in various domains in particular cancerology [7–13], psychiatry [14, 15], and SDM itself [16]. Furthermore seminars and congresses in the field of SDM are regularly organized in France for example in psychiatry [17, 18] or oncology [19, 20].
The main interest of SDM resides in improving the participation of patients who so wish, though without imposing, in the decisions concerning them, highlighting the fundamental right of each patient to be involved in the decision making process concerning his/her health [21, 22]. Moreover SDM contributes to improving healthcare quality and safety and to reducing inappropriate care, based on the principle of solidarity.
As specified in 2007 by Moumjid and colleagues [23], there is no consensual definition of SDM and a systematic review focusing on the definition of SDM is currently under way, conducted by a Danish team (Prospero no. CRD42015019740). Several models have been developed in the past 30 years, as described by Makoul and Clayman in an overview published in 2006 [24]. These authors defined nine essential elements for SDM which are: defining and explaining the problem, presenting the options, discussing the pros and cons (benefits/risks/cost), discussing the patient’s values and preferences, discussing the patient ability/self-efficacy, considering the physician’s knowledge and recommendations, checking/clarifying understanding, making a decision or explicitly postponing it, and organising the follow-up. In 2013, building in particular on Makoul’s model, Elwyn et al. proposed the “talk model”, that summarised existing models [25]. The “talk model” combines three successive and co-dependent steps in the establishment of a relationship between a healthcare professional and a patient: patient information by the healthcare professional about the nature of the problem and the various possible options, patient questioning concerning his/her preferences in terms of goals and treatments, and finally integration of the informed preferences into the decision making process. Despite its simplicity, this model seems to be less frequently cited than Makoul’s model in the articles of the field of SDM.
Beyond the models, many patient decision support or healthcare professional SDM implementation tools have been developed [26]. Most SDM best practices evaluation tools have been developed in English or German [27]. A survey of existing evaluation tools, now representing a research field in their own right, was conducted through two systematic reviews: one by Légaré et al. [28] and the other by Scholl et al. [27], both being reference teams in this field. very few evaluation tools validated in metropolitan French have been published. The only one found to date in the literature is the Decisional Conflict Scale (DCS) that was translated and validated in 2006 [29]. The DCS contains 16 items, grouped into 5 dimensions and has been validated in many languages. It pertains to decisional conflict and evaluates the uncertainty construct, which is not included in the Makoul’s model. To meet the stakes identified by the HAS for the development of SDM best practices, this is a need to develop standardised evaluation tools.
The objective of this work was to update the systematic review (dating back to 2011) of English, French and Spanish language SDM evaluation tools. The perspective is to develop an SDM evaluation tool (de novo creation or trans-cultural adaptation of an existing tool) validated in French, measuring all the SDM elements identified during a doctor-patient encounter, according to the Makoul’s model.
Methods
The systematic review was registered with PROSPERO (No. CRD42015017101).
Selection criteria
The following inclusion criteria were used:
The full text is available
The article is written in English, French or Spanish
The article was published between January 1, 2010 and December 31, 2014
The main goal of the article was the development and psychometric validation of a measurement tool
The measured construct was SDM
Psychometric validation data are presented
The measurement was performed during a healthcare professional-patient encounter (real or fictitious).
The exclusion criteria were the following:
The tool was not specifically dedicated to SDM
The tool was specific to a given disease or situation and does not appear readily adaptable to other diseases
The study used a tool (whether validated or not) applied to a specific situation, without contributing new psychometric measurements
The study was exclusively qualitative.
Search strategy
The document search strategy was based on the method recommended by the Cochrane Collaboration [30], as described in a guide by the “Institut national d’excellence en santé et en services sociaux du Québec” [31]. It was performed using the PubMed and PsycINFO databases.
For each database, a search query was formalised by combining Medical Subject Heading (MeSH) keywords with the following free text terms: “shared decision making”, “shared medical decision”, “patient participation”, “patient involvement”, questionnaire, “self-report”, “scale”, “tool”, “survey”, “test”, “instrument”, “validation”, “psychometric”, “measure*”, “assess*”. In order to search for the relevant keywords, the search query was based on the strategy used within the two previously identified systematic reviews [27, 28], along with their references.
The search query used in PubMed is described in Appendix.
Study selection
The study selection process consisted of several successive steps. First, the results obtained from the two databases were grouped into a single file. Duplicate records for a single study were eliminated before starting the selection process. An additional table file shows this in more details (see Additional file 1). The study selection form was tested on fifty randomly drawn studies in order to ascertain selection criterion relevance and discrimination.
We then examined the titles in order to exclude any irrelevant article. At this point, the studies were independently selected by the two observers LM and NB. NB examined all selected titles, while LM examined a 20 % random sample. The calculated coefficient of concordance κ1 was of 0.38. Discussions between the two observers helped to clarify the selection strategy when reading titles and to reach an agreement. A second coefficient of concordance κ2 estimated on a 10 % sample was of 0.63. An additional table file shows this in more details (see Additional file 2). During the third phase, the selected abstracts were examined by NB using the same process. Finally, examination of the full articles by NB enabled a decision of whether to include each article in the systematic review to be made. An additional table file shows this in more details (see Additional file 3). All bibliographic references were managed using the Zotero bibliography management application [32].
Data extraction
The two observers, LM and NB, collected the data independently. Initial divergences were discussed among the two observers and a consensus was reached. For each of the selected articles corresponding to new tools, the following data were gathered: tool’s name, first author’s name, publication date, point of view adopted (patient, professional, observer), language of validation, type of healthcare environment (hospital, outpatient), number and types of dimensions evaluated, number and labels of items, response scale, recording type (audio or video) where applicable, description of the physician, patient and observer samples (population size, disease or clinical situation), psychometric properties (validity, reliability), and model if it does exist.
As the name of one of the new tools, developed by Légaré et al. [33] could not be clearly determined, we used the following description proposed by the authors as a name in our study: “Dyadic measure of SDM”.
For each of the selected articles corresponding to tools presenting new psychometrics properties, the following data were gathered: tool’s name, name of the tool’s version, first author’s name, publication date, point of view adopted, study type, number of dimensions, number of items, response scale, and psychometric properties (validity, reliability).
Results analysis strategy
We first studied the characteristics of all included studies. They were classified in three groups: articles already identified in the previous reviews, new psychometric properties of previously identified tools and newly identified tools.
Regarding the latter, we studied their general characteristics, and then focused on the appraiser’s point of view. Finally they were analysed in light of Makoul’s model [24]. We classified each item into one of the nine essential elements described by Makoul and Clayman, in order to determine the extent to which the included tools measured SDM according to this model. Dimension names were not taken into consideration, only the item labels. Each item could match with only one element.
Results
Sample
The study selection steps are documented in the flowchart in Fig. 1.
Fig. 1.
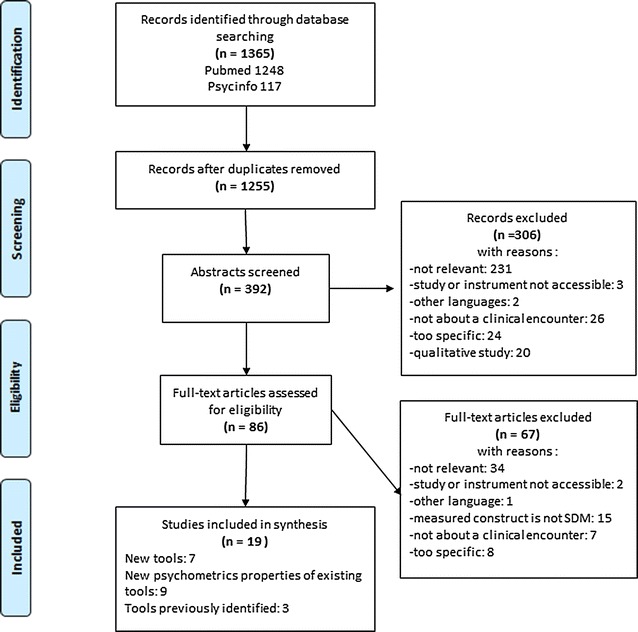
Flowchart of the study
Characteristics of included studies (n = 19)
Overall, nineteen studies were included in this review. Table 1 gives a general description. Amongst the included articles, seven [33–39] described new tools published since the last systematic review conducted by Scholl et al. [27]. Three articles related to tools that had previously been identified by this review [40–42]. Nine studies presented results of new psychometric properties for tools identified [43–51].
Table 1.
General characteristics of the included articles (n = 19)
| Tool’s name | Version | Author, year of publication | Study type |
|---|---|---|---|
| OPTION scale | Revised-scale of OPTION | Kasper, 2012 [43] | Specific psychometric properties (criterion validity) |
| MAPPIN’SDM | Kasper, 2012 [43] | New instrument | |
| SDM’MASS (meeting its concept’s assumptions) | Geiger, 2012 [37] | New instrument | |
| German version of the OPTION scale | Hirsch, 2012 [45] | Transcultural validation in german language | |
| OPTION scale | Nicolai, 2012 [46] | New psychometric properties | |
| Modified-OPTION scale | Keller, 2013 [47] | Specific psychometric properties (criterion validity, ICC, sensitivity analysis) | |
| SDM-Q-9 | SDM-Q-Doc | Schöll, 2012 [34] | New instrument |
| SDM-Q-9 | Kriston, 2010 [42] | Instrument previously identified in Scholl’s review | |
| SDM-Q-9 | De Las Cuevas, 2014 [50] | Transcultural validation in spanish language | |
| Decisional Conflict Scale | DCS | Kawaguchi, 2013 [44] | Transcultural validation in japanese language |
| DCS-LL (low literacy version) | Linder, 2011 [51] | Transcultural validation in low literacy version | |
| IDM (Informed decision making) instrument | Leader, 2012 [36] | New instrument | |
| CICAA-Patient Centered | CICAA-D | Ruiz Moral, 2010 [38] | New instrument |
| Dyadic measure of SDM | Légaré, 2012 [33] | New instrument | |
| CollaboRATE | Barr, 2014 [39] | New instrument | |
| SURE | Ferron Parayre, 2014 [48] | Specific psychometric properties (criterion validity, sensitivity analysis) | |
| I-PICS | Jonsdottir, 2013 [49] | Transcultural validation in icelandic language | |
| SDM scale | Singh, 2010 [40] | Instrument previously identified in Scholl’s review | |
| DAS-O | Brown, 2011 [41] | Instrument previously identified in Scholl’s review |
More than half of the included studies were conducted in Europe [34, 35, 37, 38, 42, 43, 45–47, 49, 50], most of which in Germany. Seven were conducted in North America [33, 36, 39–41, 48, 51] and one in Japan [44]. For most of the studies, the first author was affiliated with a faculty of Medicine, or with a medical organisation (n = 17) [33–43, 45–48, 50, 51]. One of the tools was developed by researchers of a nursing school (n = 1) [49] and one by a team affiliated to a faculty of pharmacy (n = 1) [44].
Concerning the point of view used to evaluate SDM, six studies used the patient’s point of view alone [42, 44, 48–51], eight that of an external observer alone [36, 38–41, 45–47], and one that of a healthcare professional alone [34]. In three studies, the recently published tools focused on the confrontation of points of view by evaluating the patient-professional dyad [33], or the patient-professional-observer triad [35, 37].
Characteristics of tools presenting new psychometric properties (n = 9)
Nine studies presented results of new psychometric properties of already known tools. Table 2 presents the characteristics of these instruments. Amongst them, five articles presented trans-cultural validations, with analysis of the usual psychometric properties. Four of which involved another language (Japanese [44], german [45], Icelandic [49], Spanish [50] and one a specific type of patient (DCS-Low literacy) [51]. Four other articles presented the results of specific analyses of criterion validity [43, 46–48], two of which also presented sensitivity analyses [47, 48].
Table 2.
Characteristics of tools presenting new psychometric properties (n = 9)
| Name of the tool | Name of the tool’s version | First author, year of publication (reference no) | Study type | Point of view | Number of dimensions and items of SDM | Response-scale | Reliability | Validity |
|---|---|---|---|---|---|---|---|---|
| Decisional Conflict Scale | Japanese version of DCS | Kawaguchi, 2013 [44] | Transcultural validation in Japanese language | Patient | 5 dimensions; 16 items Uncertainty (3) Informed (3) Values clarity (3) Support (3) Effective decision (4) |
5-point scale | Cronbach’s alpha = 0.84–0.96 ICC = 0.63–0.93 |
Content validity: Yes Face validity: No Construct validity: Yes Convergent/discriminant validity: Yes |
| OPTION scale | German version of the OPTION scale | Hirsch, 2012 [45] | Transcultural validation in German language | Observer | 1 dimension; 12 items |
5-point scale | Cronbach’s alpha = 0.90 ICC = 0.68–0.82 |
Face validity: No Construct validity: Yes Convergent/discriminant validity: No Criterion validity: Yes |
| PICS | I-PICS | Jonsdottir, 2013 [49] | Transcultural validation in Icelandic language | Patient | 4 dimensions; 20 items Health care professional (HCP)information (6) Patient information (5) Patient participation in decision making (4) HCP facilitation (5) |
5-point Likert scale | Cronbach’s alpha = 0.86 | Face validity: No Construct validity: Yes Convergent/discriminant validity: No Criterion validity: Yes |
| SDM-Q-9 | Spanish version of SDM-Q-9 | De Las Cuevas, 2014 [50] | Transcultural validation in Spanish language | Patient | 1 dimension; 9 items |
6-point scale | Cronbach’s alpha = 0.89 ICC = 0.52–0.82 (item 1: 0.27) |
Face validity: Yes Construct validity: Yes Convergent/discriminant validity: Yes |
| Decisional conflict Scale | DCS-LL (low literacy version of decisional conflict scale) | Linder, 2011 [51] | Transcultural validation in low literacy version | Patient | 4 dimensions; 10 items Uncertainty (2) Informed (3) Values clarity (2) Supported (3) |
3-point scale | Cronbach’s alpha = 0.80 ICC = 0.43–0.87 |
Content validity: No Face validity: No Construct validity: Yes Convergent/discriminant validity: Yes |
| OPTION scale | Revised-scale of OPTION scale | Kasper, 2012 [43] | Specific psychometric properties (criterion validity) | Patient, professional | 1 dimension; 12 items |
5-point scale | Cronbach’s alpha = Yes | Criterion validity: Yes |
| OPTION scale | Modified-OPTION scale | Keller, 2013 [47] | Specific psychometric properties (criterion validity, sensitivity analysis) | Observer | 1 dimension; 12 items |
5-point scale | Cronbach’s alpha = 0.90 ICC = 0.43–0.82 |
Criterion validity: Yes Sensitivity analyses: Yes |
| SURE | SURE | Ferron Parayre, 2014 [48] | Specific psychometric properties (criterion validity, sensitivity analysis) | Patient | 1 dimension; 4 items |
5-point scale | Cronbach’s alpha = 0.70 | Content validity: Yes Face validity: No Construct validity: No Convergent/discriminant validity: No Criterion validity: Yes Sensitivity analyses: Yes |
| OPTION scale | OPTION scale | Nicolai, 2012 [46] | New psychometric properties | Observer | 1 dimension; 12 items |
5-point scale | Cronbach’s alpha = Yes | Criterion validity: Yes Convergent/discriminant validity: unknown |
Amongst these nine studies, four described properties of the OPTION scale [43, 45–47], two those of the decisional conflict scale [44, 51], one those of the PICS [49], one those of the SDM-Q-9 [50] and one those of the SURE tool [48].
Most of these instruments were unidimensional (n = 6) [43, 45–48, 50]. Three tools were multidimensional [44, 49, 51]. The three multidimensional tools comprised 4–5 dimensions. The mean number of items per tool was of 12 (4–20). The response scale used was mainly of the Likert-5 type (n = 7) [43–49]. The other instruments used a 3-point response scale [51], and a 6-point response scale [50].
Concerning reliability, the Cronbach’s alpha coefficient was calculated in all nine studies and the interclass correlation coefficient (ICC) was calculated for five studies [44, 45, 47, 50, 51]. Regarding validity, five of the nine articles presented a construct validity [44, 45, 49–51], one a face validity [50], and three a convergent/discriminating validity [44, 50, 51].
Amongst the nine tools presenting new psychometric properties, one evaluated two points of view simultaneously: that of the patient and healthcare professional (dyad) [43]. Five instruments evaluated SDM according to the patient point of view only [44, 48–51]. Three tools assessed SDM from the external observer’s perspective alone [45–47]. None of the instruments evaluated the healthcare professional’s point of view alone.
Characteristics of newly included tools (n = 7)
General description
Among the seven newly identified tools, two had in fact previously been identified by Scholl et al. work [27], though at the time they were “work in progress”, i.e. with no published psychometric data [33, 34]. As the presence of psychometric data was one of our inclusion criteria, we made the choice to include them in this subgroup. Table 3 presents the characteristics of the seven newly identified instruments: SDM-Q-Doc [34], Mappin’SDM [35], informed decision making instrument [36], SDM’Mass [37], CICAA-Decision [38], Dyadic measure of SDM [33], and collaborate [39].
Table 3.
Characteristics of the newly developed instruments (n=7)
| Name of the tool | First author, year of publication (reference no) | Point of view | Language of validation | Inpatients and/or outpatients | Number of dimensions and items of SDM | Response-scale | Methodology | Sample | Reliability | Validity | Model and items generation process |
|---|---|---|---|---|---|---|---|---|---|---|---|
| SDM-Q-Doc | Scholl I, 2012 [34] | Professional | German | Inpatients and outpatients | 1 dimension; 9 items |
6-point scale | Real consultations | PHYSICIANS: N = 29/General practitioners 51.7 %, orthopaedists 13.8 %, psychiatrists 13.8 %, diabetologists 20.7 % PATIENTS: N = 324/external patients of primary and secondary care with a chronic back pain, type 2 diabetes, or depression | Cronbach’s alpha = 0.88 ICC = 0.35–0.76 |
Content validity: unknown Face validity: Yes Construct validity: Yes Convergent/Discriminant validity: Yes |
Pre-existent tool (SDM-Q, 2006) and theory-driven: Nine practical steps of the SDM process defined by the authors: disclosure that a decision needs to be made, formulation of equality of partners, presentation of treatment options, informing on the benefits and risks of the options, investigation of patient’s understanding and expectations, identification of both parties’ preferences, negotiation, reaching a shared decision, arrangement of follow-up |
| Mappin’SDM | Kasper J, 2012 [35] | Patient, professional, observer | German | Inpatients and outpatients | 15 items | 5-point Likert scale | Real consultations | (video recording) 40 consultations physician-patient videorecorded (Hambourg)/average duration 19.5 min (2.5–51 min)/average duration of decision sequence 15 min (2.5 to 38.8 min)// PHYSICIANS: N = 10/neurologists and internal medicine 40 %, dentists 30 %, general practitioners 30 % PATIENTS: N = 40/55 % of men |
Cronbach’s alpha = 0.91–0.94 ICC = Yes |
Face validity: unknown Construct validity: No Convergent/Discriminant validity: Yes |
Theory-driven (created by the authors): three perspectives, two constructs, three units and seven focus result in a set of three tools, each of them measuring the same fifteen items |
| Informed decision making instrument | Leader A, 2012 [36] | Observer | English | Inpatients and outpatients | 3 dimensions 9 items Patient empowerment (1) Information sharing (4) Active engagement in preference clarification (4) |
2 point-scale | Real consultations audio recorded N = 146 |
PHYSICIANS: N = 22 PATIENTS: N = 146 men candidates screening of prostate cancer |
Cronbach’s alpha = 0.80 ICC = 0.81 |
Construct validity: use of an existing instrument | Theory-driven: Nine elements of Informed Decision Making developed by Dr Braddock [56]: the patient’s role in decision making, the impact of the decision on the patient’s daily life (context of decision), the nature of the decision or clinical issue, alternatives, pros and cons surrounding alternatives, uncertainties regarding alternatives, physician assessment of the patient’s understanding, physician assessment of the patient’s desire for input from trusted others, physician solicitation and exploration of the patient’s preference |
| SDM’Mass (SDM Meeting its concept’s ASSumptions) | Geiger F, 2012 [37] | Patient, professional, observer | German | Inpatients and outpatients | 15 items | 5-point Likert scales | Real consultations video recorded N = 40 |
Average duration 20 min (2.5–51 min; SD = 11)/Average duration of decision sequence 15 min (3 to 39 min; SD = 8)// PHYSICIANS: N = 10/neurologists and internal medicine 40 %, dentists 30 %, general practitioners 30 % PATIENTS: N = 40/55 % of men |
Cronbach’s alpha = 0.94 ICC = 0.74–0.87 |
Face validity: unknown Construct validity: No Convergent/discriminant validity: No |
Theory-driven (created by the authors): Three perspectives, two constructs, three units and seven focus result in a set of three tools, each of them measuring the same fifteen items |
| CICAA-Decision | Ruiz Moral R, 2010 [38] | Observer (on professional ‘s behaviour) | Spanish | Outpatient | 3 dimensions; 17 items Identifying and understanding problems (2) Reach an agreement and help to act (11) Decisions with options (4) |
3-point scale | Real and fictional consultations N = 111 real patients and N = 50 simulated patients |
(Video recording) 161 consultations videorecorded: 61 consultations between “professional” and patient with chronic disease (diabetes et chronic pain) + 100 consultations between last year’s residents and new patients (50) or simulated patients (50)// Then selection of 32 consultations (20 % where item 25 is positive = a bit of participation is detected)/average duration = 11.3 min (SD = 5.6; IC95 = 9.2-13.3) |
Cronbach’s alpha = 0.60–0.51 (1st and 2nd encounter) ICC global = 0.96 |
Content validity: Yes Face validity: Yes Construct validity: Yes Convergent/discriminant validity: No |
Pre-existent tool (CICAA-CP) and literature research (review of pre-existing conceptual frameworks) |
| Dyadic measure of SDM | Légaré F, 2012 [33] | Patient, professional | English and Quebec French (patient and doctors recruited in Ontario and Québec) | Outpatient | 7dimensions; 30 items Information giving (9) Values clarification (3) Doctor recommendations (5) Self-efficacy (3) Feeling uninformed (3) Information verifying (4) Uncertainty (3) |
5-point scale and 10-point scale (different subscales) | Real consultations | PHYSICIANS: N = 272/english language N = 109, french N = 163 PATIENTS: N = 269/english language N = 108, french language N = 161/69 % of women/average age 49 (SD = 18) Complete DYAD: N = 259 (after consultation) |
Cronbach’s alpha = 0.90 ICC = 0.43–0.82 |
Face validity: No Construct validity: Yes Convergent/discriminant validity: No Criterion validity: correlation with OPTION scale: Yes sensitivity analysis (AUC and ROC) Agreement across raters: ICC |
Pre-existent tools and theory-driven (created by the authors): Based on Makoul and Clayman model, creation of a dyadic model that conceptualized the interpersonal and interdependent elements of the relationship between physicians and patients Then identification of instruments tested on both physicians and patients. Finally cross-cultural adaptation of the identified subscales that mapped the essential elements of SDM included in their dyadic model |
| Collaborate | Barr PJ, 2014 [39] | Observer (citizen; has to put in patient’s place) | English | Inappropriate | 3 dimensions; 3 items Explanation of the health issue Elicitation of patient preferences Integration of patient preferences |
2 versions: 5-point scale, and 10-point scale | Fictional consultations N = 6 simulated videos of encounters physician-patient |
OBSERVERS: N = 1341 in study 1/N = 251 in study 2 (1–2 weeks after first answer)/On N = 1341: 46 % of men/47 % of 18-44 years, 33 % of 45-64 years, 20 % of 65 years and more/public in general population acting as the observer. Recruited by the 2010 US Census/representative sample of general population of USA | Cronbach’s alpha: No ICC = 0.76–0.90 |
Convergent/Discriminant validity: Yes Criterion validity: Yes Sensitivity to change: Yes |
Theory-driven (created by the authors): the “talk model” developed by authors in a previous study [25] |
In most cases, the validation language was German (n = 3) [34, 35, 37], followed by English (n = 2) [36, 39] and Spanish (n = 1) [38]. One study presented a tool with a dual French–English version [33]. The first author was always affiliated with a faculty of Medicine or a medical organisation. Patient sample sizes ranged from 40 to 324, with a mean of 163 patients (median = 153.5). The healthcare professionals involved in the studies were explicitly physicians in six of the studies. One study used the terms “professionals” and “residents” [38]. The number of physicians ranged between 10 and 272, with a mean of 67 (median = 22). In four studies, the patient sample consisted of both inpatients and outpatients [34–37] whereas two studies focused on outpatients alone [33, 38].
Most of the newly included tools were multidimensional (n = 4). The four multidimensional tools comprised a median of 3 dimensions (3–7). Only one tool was unidimensional [34]. Two tools described a total of fifteen items, without specifying their grouping into dimensions [35, 37]. The mean number of items per tool was of 14 (3–30). The response scale used was mainly of the Likert-5 type (n = 4) [33, 35, 37, 39] of which two tools used a 5- or 10-point response scale depending on the sub-scales [33] or versions [39]. The other tools used a 2-point [36], 3-point [38], or 6-point [34] response scale.
Regarding reliability, the Cronbach’s alpha coefficient was calculated for six studies [33–38], while the interclass correlation coefficient (ICC) was calculated in all seven studies. As for validity, three of the seven articles reported a construct validity [33, 34, 38], two a face validity [34, 38], and three a convergent/discriminating validity [34, 35, 39]. The criterion validity was presented in two articles [33, 39], and content validity in one article [38].
Evaluated point of view
Amongst the seven newly included tools, two evaluated all three points of view simultaneously (triad) [35, 37], while one evaluated that of the patient and healthcare professional (dyad) [33]. Three instruments evaluated SDM according to the external observer’s point of view only [36, 38, 39]. Amongst them, one study used a sample of patients taken from the general population who were asked to place themselves in the patient’s place, thus assuming a role of external observer [39]. One tool evaluated SDM from the healthcare professional’s perspective alone [34]. None of the instruments explored the patient’s point of view alone.
Amongst the tools evaluating the perspective of an external observer (alone, or jointly with other points of view), the evaluation always involved recordings. Most of these were videos (n = 4) [35, 37–39], while one study used audio recordings [36]. Most of the tools were based on real consultations (n = 5). One tool used only fictitious consultations [39], while another was based on encounters with both real and fictitious patients [38].
Model and comparison to Makoul and Clayman’s integrative model of SDM
The design of six out of seven tools was based on a model:
Four authors had created the model themselves [33, 35, 37, 39].
Two used, in addition to the theory, one or several pre-existent tools [33, 34].
The development of one of the seven tools was not based on a precise model, but rather on a pre-existent tool combined with a literature review [38].
The nine elements defining SDM according to Makoul [24] were inconsistently met in the seven newly identified tools. The distribution is presented in Fig. 2. Three elements were found in all seven tools: “define/explain problem”, “patient values/preferences”, and “check/clarify understanding”. The element “present options” was found in every tool except the collaborate tool.
Fig. 2.
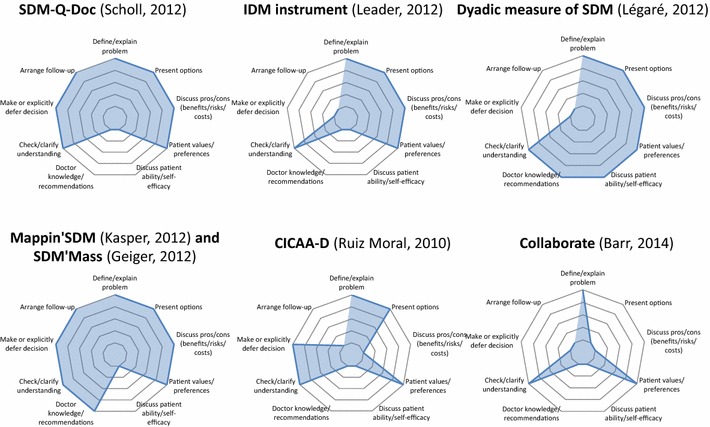
Distribution diagrams of the essential elements of SDM according to Makoul in newly developed tools
Still according on the Makoul’s model, Mappin’SDM [35] and SDM’Mass [37] were the tools that evaluated the greatest number of essential SDM elements: only one “discuss patient ability/self-efficacy” was not explored by these two tools. It is noteworthy that the collaborate tool [39] contained only three of the essential elements described by Makoul and Clayman.
Discussion
This literature review covering the 2010–2014 period identified a total of nineteen publications since the last systematic review by Scholl et al. [27]. Seven articles presented psychometric validations of new tools: SDM-Q-Doc, Mappin’SDM, SDM’Mass, Informed Decision Making Instrument, CICAA-Decision, Dyadic measure of SDM, and Collaborate. Our results partially overlap those of Scholl et al.: indeed, three studies had already been identified in the previous review and nine studies covered new psychometric validations of previously identified tools, including five trans-cultural validations. It shows the growing effort of SDM research in various countries including France. Indeed, the interest paid to the field of SDM is shared internationally both by clinicians and researchers [2], as shown by the multiple languages of the identified evaluation tools.
We have found that there was a recent breakthrough in the field of SDM research with the multiplicity of appraiser points of view. The old approach involving a single appraiser is progressively tending towards a multiple, dyadic [27] or even triadic approach, in accordance to recent recommendations [52]. In the field of clinical practice, SDM evaluation is performed by the healthcare professional or the patient. This approach is helpful to provide an image of the interdependence between the members of this dyad during the decision making process [53, 54]. In the field of research, a third player—the external observer—has emerged, most often using video or audio recordings.
Regarding the different existing models subtending SDM, it is not unequivocal. Several models coexist [24, 25, 52, 55]. The Makoul’s model [24] based on a systematic and broadly acknowledged review in the field of SDM research was published in 2006. We chose this model as a basis for comparison between SDM evaluation tools for three main reasons. First, it is one of the most frequently cited models in the articles of the field. Second, it is based on a systematic review and is therefore a synthesis of other existing models. Third, compared to the “talk model”, also based on a literature review, Makoul’s model describes more elements, and thus provides a broader description of the SDM process. Although some aspects of this process might still be overlooked by Makoul’s model, it seemed to be the most relevant model for standardized comparisons of the seven newly identified tools.
The originality of our work partly lies in these standardized comparisons. They showed notably that none of the newly identified tool covered the whole nine essential elements of Makoul’s model. However, three elements (“define/explain problem”, “patient values/preferences”, and “check/clarify understanding”) were identified in each of the tools, and might therefore constitute necessary—and maybe sufficient—dimensions of the SDM construct. Conversely, the element “discuss patient ability/self-efficacy” was missing in every tool except for the Dyadic measure of SDM [33] and might therefore be more difficult to measure. It is interesting to note that the collaborate tool [39], which contains only three essential elements of Makoul’s model, was specifically designed for a clinical use. For practical reasons, indeed, it might be reasonable to limit the number of elements assessed by clinical tools, as opposed to research tools, which could be more comprehensive.
Five tools were particularly interesting, because of the multiplicity of SDM dimensions and/or points of view that they explored. Mappin’SDM [35] and SDM’Mass [37] cover eight SDM elements according to Makoul’s model and evaluate all three points of view; the Dyadic measure of SDM [33] covers seven dimensions and measures the points of view of both the patient and the healthcare professional; SDM-Q-Doc [34] covers seven dimensions of SDM, and collaborate [39], covers the three dimensions defined by the “talk model” from which it is derived.
There are several limitations in our study that could have prevented relevant studies to be included in our review. For instance, the grey literature was not examined, experts in the SDM field were not contacted and their internet pages and social networks were not consulted. This selection strategy probably resulted in a lack of relevant sources. The authors take into account the fact that it might have led to a selection bias. The articles were obtained by searching solely from the PubMed and PsycINFO databases. However, this latter limitation might not be that important. Indeed, after having tested the search equations on five databases (PubMed, PsycINFO, BDSP, Cairn and Pascal), we decided to use the first two only due to the lack of relevant results in the others. We have also limited our review to articles in French, English and Spanish. Therefore, tools presented in article written in another language would be missing from our review. This language bias in fact occurred in the two previous reviews [27, 28]. Indeed, the inclusion of articles in Spanish allowed us to identify one tool that was missed by these studies [38]. Moreover, while the previous literature reviews focused on several dimensions of the patient-carer relationship, including SDM and communication [27, 28], we deliberately chose to exclude tools that were not exclusively dedicated to SDM, for reasons of clarity. Some interesting tools might have been missed due to this selection process.
Finally, the double independent observers strategy was adopted for a fraction of the titles read only, not for reading the abstracts and full-text articles.
In spite of these limitations, our results are consistent with the already published systematic reviews.
Conclusions
The stakes of SDM are major, whether it be in regard to patient participation improvement, healthcare quality or safety, or inappropriate use of healthcare reduction. Evaluating the quality of SDM between patient and professional for the needs of improvement and training requires the use of subjective measurement tools with good psychometric properties. This review enabled us to identify several interesting tools. The next step of our project will be to develop and validate a French language instrument by operating a trans-cultural adaptation of one or several identified tools, since it could allow both to develop an SDM evaluation tool in French, and to make a cultural comparison in the field.
Authors’ contributions
NB, BL and LM designed the study. NB selected the studies, collected the data, analyzed the results and wrote the manuscript. BL participated in the conception of the methodology and the writing of the manuscript. LM has validated the method, participated in the study selection, data extraction and participated in the writing of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
None.
Competing interests
The authors declare that they have no competing interests.
Availability of data and material
All data generated or analyzed during this study are included in this published article and its supplementary additional files.
Funding
The Nantes University Hospital, France was the single source of funding for the research reported. This funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Abbreviations
- DCS
decisional conflict scale
- HAS
Haute Autorité de Santé
- ICC
interclass correlation coefficient
- SDM
shared decision making
Appendix: search query on PubMed
Filter: publication date from January 1, 2010 to December 31, 2014
((“shared decision making”[Title] OR “shared decision-making”[Title] OR “shared decision making”[TW] OR “shared medical decision”[Title] OR “patient participation”[Title] OR “patient participation”[MH] OR “patient participation”[TW] OR “patient involvement”[Title])) AND (Questionnaire[Title] OR Questionnaires[Title] OR “self report”[Title] OR “self reports”[Title] OR scale[Title] OR scales[Title] OR tool[Title] OR tools[Title] OR measur*[Title] OR assess*[Title] OR survey[Title] OR surveys[Title] OR test[Title] OR tests[Title] OR instrument[Title] OR instruments[Title] OR questionnaires[MH] OR “self report”[MH] OR validation[Title] OR psychometrics[MH] OR Psychometric[Title] OR psychometrics[Title])
Additional files
10.1186/s13104-016-2164-6 List of records identified trough database searching (n=1365) and after removed (n=1255). Description of data: title, author 1 to 5 (first and last name), name of journal, date of publication, abstract, tag 1 to 4, selection’s status (included or duplicate).
10.1186/s13104-016-2164-6 List of records of 20% and 10 % random sample selected by two independent observers and calcul of coefficients of concordance κ1 and κ2. Description of data: Sheet 1: title, selection’s status NB reading 1 20 % titles (excluded/included), selection’s status LM reading 1 20 % titles (excluded/included), comparison between 2 observers, kappa 1. Sheet 2: title, selection’s status NB reading 2 10 % titles (excluded/included), selection’s status LM reading 2 10 % titles (excluded/included), comparison between 2 observers, selection’s status adjustment after discussions (excluded/included), kappa 2.
10.1186/s13104-016-2164-6 List of full-text articles assessed for eligibility (n=86) and full-text articles excluded (n=67). Description of data: title, first author (last name), name of journal, date of publication, abstract, selection’s status (included or excluded), not relevant, study or instrument not accessible, other language, measured construct is not SDM, not about a clinical encounter, too specific.
Contributor Information
Nathalie Bouniols, Phone: +33 (0)2.40.84.69.20, Email: nathalie.bouniols@gmail.com.
Brice Leclère, Email: brice.leclere@chu-nantes.fr.
Leïla Moret, Email: leila.moret@chu-nantes.fr.
References
- 1.Loi n 2002-303 du 4 mars 2002 relative aux droits des malades et à la qualité du système de santé. 2002-303 Mar 4, 2002. http://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000000227015&categorieLien=id. [PubMed]
- 2.Haute Autorité de Santé. Patient et professionnels de santé : décider ensemble. Concept, aides destinées aux patients et impact de la décision médicale partagée. Etat des lieux. 2013.
- 3.Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango) Soc Sci Med. 1997;44:681–692. doi: 10.1016/S0277-9536(96)00221-3. [DOI] [PubMed] [Google Scholar]
- 4.Politi MC, Wolin KY, Légaré F. Implementing clinical practice guidelines about health promotion and disease prevention through shared decision making. J Gen Intern Med. 2013;28:838–844. doi: 10.1007/s11606-012-2321-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Moumjid N, Brémond A, Mignotte H, Faure C, Meunier A, Carrère M-O. Shared decision-making in the physician-patient encounter in France: a general overview. Z Für Ärztl Fortbild Qual. 2007;101:223–228. doi: 10.1016/j.zgesun.2007.02.042. [DOI] [PubMed] [Google Scholar]
- 6.Moumjid N, Durif-Bruckert C, Denois-Régnier V, Roux P, Soum-Pouyalet F. Shared decision making in the physician-patient encounter in France: a general overview in 2011. Z Für Evidenz Fortbild Qual Im Gesundheitswesen. 2011;105:259–262. doi: 10.1016/j.zefq.2011.04.016. [DOI] [PubMed] [Google Scholar]
- 7.Protière C, Moumjid N, Malavolti L, Le corroller-Soriano AG. Les comportements de recherche d’information des patients. Vie Deux Après Diagn. Cancer Une Enq. En 2004 Sur Cond. Vie Mal. Paris: La documentation française; 2008. pp. 137–49. http://www.bdsp.ehesp.fr/Base/379894/.
- 8.Bouhnik A-D, Moumjid N, Protière C. L’implication des patients dans le choix des traitements. Vie Deux Après Diagn. Cancer Une Enq. En 2004 Sur Cond. Vie Mal. Paris: La documentation française; 2008. pp. 123–36. http://www.bdsp.ehesp.fr/Base/379893/.
- 9.Durif-Bruckert C, Roux P, Morelle M, Mignotte H, Faure C, Moumjid-Ferdjaoui N. Shared decision-making in medical encounters regarding breast cancer treatment: the contribution of methodological triangulation: shared decision making and methodological triangulation. Eur J Cancer Care (Engl) 2015;24:461–472. doi: 10.1111/ecc.12214. [DOI] [PubMed] [Google Scholar]
- 10.Vennin P, Taïeb S, Carpentier P. Le patient face aux choix thérapeutiques en cancérologie: vers une décision partagée? Bull Cancer (Paris) 2001;88:391–397. [Google Scholar]
- 11.Brémond A, Carrère M-O, Moumjid N, Nguyen F. La participation des patients à la décision médicale vue par les médecins. Le cas des chirurgiens dans un réseau. In: Carrère C par PC et M-O, editor. Soins En Réseau Prat. Acteurs Régulation En Cancérologie. Editions John Libbey Eurotext; 2007 [cited 2016 Jun 22]. pp. 63–74. https://halshs.archives-ouvertes.fr/halshs-00266853.
- 12.Soumpouyalet F, Regnier V, Querre M, Jacquin JP, Hubert A, Debled M. Influence des facteurs socioculturels dans la prise de décision médicale en cancérologie. Bull Cancer (Paris) 2009;96:733–739. doi: 10.1684/bdc.2009.0882. [DOI] [PubMed] [Google Scholar]
- 13.Moumjid N, Charles C, Morelle M, Gafni A, Brémond A, Farsi F, et al. The statutory duty of physicians to inform patients versus unmet patients’ information needs: the case of breast cancer in France. Health Policy. 2009;91:162–173. doi: 10.1016/j.healthpol.2008.11.010. [DOI] [PubMed] [Google Scholar]
- 14.Pachoud B, Llorca PM, Salmona I, Trabut J-B. La décision médicale partagée en psychiatrie: quelle utilité? Eur Psychiatry. 2015;30:S39. [Google Scholar]
- 15.La Pachoud B. décision médicale partagée et les paradigmes médicaux contemporains: la médecine centrée sur la personne, la médecine fondée sur des preuves, le paradigme du rétablissement. Eur Psychiatry. 2015;S30:S39. [Google Scholar]
- 16.Bouleuc C, Poisson D. La décision médicale partagée. Laennec. 2014;62:4–7. doi: 10.3917/lae.144.0004. [DOI] [Google Scholar]
- 17.Salmona I, Mortier M, Université Paris Diderot. Du pouvoir psychiatrique à la décision partagée. Paris, France; 2014 [cited 2016 Jun 22]. http://www.univ-paris-diderot.fr/sc/site.php?bc=recherche&np=pageActu&ref=6762.
- 18.Salmona I. Décision médicale partagée en psychiatrie: intérêt des méthodologies mixtes et qualitatives. Eur Psychiatry. 2015;30:S40. doi: 10.1016/j.eurpsy.2015.09.113. [DOI] [Google Scholar]
- 19.Bremond A, Carrère M-O, Moumjid N. Décision médicale partagée en oncologie. France: Marseille; 2005. [Google Scholar]
- 20.Moumjid N, Nguyen F, Bremond A, Mignotte H, Faure C, Meunier A, et al. Préférences des patients et prise de décision: état des lieux et retour d’expérience en cancérologie. Rev Dépidémiologie Santé Publique. 2008;56:S231–S238. doi: 10.1016/j.respe.2008.04.008. [DOI] [PubMed] [Google Scholar]
- 21.President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. Making health care decisions, The ethical and legal implications of informed consent in the patient–practitioner relationship. Washington, DC; 1982.
- 22.Edwards A, Elwyn G. Shared decision-making in health care: achieving evidence-based patient choice. Oxford: Oxford University Press; 2009. [Google Scholar]
- 23.Moumjid N, Gafni A, Bremond A, Carrere MO. Shared decision making in the medical encounter: are we all talking about the same thing? Med Decis Mak. 2007 [cited 2015 Apr 14]. http://mdm.sagepub.com/content/early/2007/09/14/0272989X07306779. [DOI] [PubMed]
- 24.Makoul G, Clayman ML. An integrative model of shared decision making in medical encounters. Patient Educ Couns. 2006;60:301–312. doi: 10.1016/j.pec.2005.06.010. [DOI] [PubMed] [Google Scholar]
- 25.Elwyn G, Tsulukidze M, Edwards A, Légaré F, Newcombe R. Using a “talk” model of shared decision making to propose an observation-based measure: observer OPTION 5 Item. Patient Educ Couns. 2013;93:265–271. doi: 10.1016/j.pec.2013.08.005. [DOI] [PubMed] [Google Scholar]
- 26.Stacey D, Bennett CL, Barry MJ, Col NF, Eden KB, Holmes-Rovner M, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD001431.pub3/abstract. [DOI] [PubMed]
- 27.Scholl I, Loon MK, Sepucha K, Elwyn G, Légaré F, Härter M, et al. Measurement of shared decision making—a review of instruments. Z Für Evidenz Fortbild Qual Im Gesundheitswesen. 2011;105:313–324. doi: 10.1016/j.zefq.2011.04.012. [DOI] [PubMed] [Google Scholar]
- 28.Légaré F, Moher D, Elwyn G, LeBlanc A, Gravel K. Instruments to assess the perception of physicians in the decision-making process of specific clinical encounters: a systematic review. BMC Med Inform Decis Mak. 2007;7:30. doi: 10.1186/1472-6947-7-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mancini J, Santin G, Chabal F, Julian-Reynier C. Cross-cultural validation of the decisional conflict scale in a sample of French patients. Qual Life Res. 2006;15:1063–1068. doi: 10.1007/s11136-005-6003-9. [DOI] [PubMed] [Google Scholar]
- 30.Higgins JPT, Green S, Cochrane collaboration, editors. Cochrane handbook for systematic reviews of interventions. Hoboken: Wiley-Blackwell; 2008.
- 31.Institut national d’excellence en santé et en services sociaux (INESSS). Les normes de production des revues systématiques. Guide méthodologique. 2013.
- 32.Zotero. www.zotero.org.
- 33.Légaré F, Turcotte S, Robitaille H, Stewart M, Frosch D, Grimshaw J, et al. Some but not all dyadic measures in shared decision making research have satisfactory psychometric properties. J Clin Epidemiol. 2012;65:1310–1320. doi: 10.1016/j.jclinepi.2012.06.019. [DOI] [PubMed] [Google Scholar]
- 34.Scholl I, Kriston L, Dirmaier J, Buchholz A, Härter M. Development and psychometric properties of the shared decision making questionnaire–physician version (SDM-Q-Doc) Patient Educ Couns. 2012;88:284–290. doi: 10.1016/j.pec.2012.03.005. [DOI] [PubMed] [Google Scholar]
- 35.Kasper J, Hoffmann F, Heesen C, Köpke S, Geiger F. MAPPIN’SDM—the multifocal approach to sharing in shared decision making. PLoS ONE. 2012;7:123. doi: 10.1371/annotation/3e489f03-e7e7-4b41-827e-caa85bb06466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Leader A, Daskalakis C, Braddock CH, Kunkel EJS, Cocroft JR, Bereknyei S, et al. Measuring informed decision making about prostate cancer screening in primary care. Med Decis Mak Int J Soc Med Decis Mak. 2012;32:327–336. doi: 10.1177/0272989X11410064. [DOI] [PubMed] [Google Scholar]
- 37.Geiger F, Kasper J. Of blind men and elephants: suggesting SDM-MASS as a compound measure for shared decision making integrating patient, physician and observer views. Z Für Evidenz Fortbild Qual Im Gesundheitswesen. 2012;106:284–289. doi: 10.1016/j.zefq.2012.03.020. [DOI] [PubMed] [Google Scholar]
- 38.Ruizmoral R, Peraltamunguia L, Pérulatorres LA, Gavilánoral E, Loayssalara JR. Patient involvement in decision making in primary care clinics: development of a measuring tool. Atencion Primaria Soc Esp Med Fam Comunitaria. 2010;42:257–263. doi: 10.1016/j.aprim.2009.09.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Barr PJ, Thompson R, Walsh T, Grande SW, Ozanne EM, Elwyn G. The psychometric properties of CollaboRATE: a fast and frugal patient-reported measure of the shared decision-making process. J Med Internet Res. 2014;16:e2. doi: 10.2196/jmir.3085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Singh S, Butow P, Charles M. Tattersall MHN. Shared decision making in oncology: assessing oncologist behaviour in consultations in which adjuvant therapy is considered after primary surgical treatment. Health Expect Int J Public Particip Health Care. 2010;13:244–257. doi: 10.1111/j.1369-7625.2009.00587.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Brown RF, Butow PN, Juraskova I, Ribi K, Gerber D, Bernhard J, et al. Sharing decisions in breast cancer care: development of the decision analysis system for oncology (DAS-O) to identify shared decision making during treatment consultations. Health Expect Int J Public Particip Health Care. 2011;14:29–37. doi: 10.1111/j.1369-7625.2010.00613.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Kriston L, Scholl I, Hölzel L, Simon D, Loh A, Härter M. The 9-item shared decision making questionnaire (SDM-Q-9). development and psychometric properties in a primary care sample. Patient Educ Couns. 2010;80:94–99. doi: 10.1016/j.pec.2009.09.034. [DOI] [PubMed] [Google Scholar]
- 43.Kasper J, Hoffmann F, Heesen C, Köpke S, Geiger F. Completing the third person’s perspective on patients’ involvement in medical decision-making: approaching the full picture. Z Für Evidenz Fortbild Qual Im Gesundheitswesen. 2012;106:275–283. doi: 10.1016/j.zefq.2012.04.005. [DOI] [PubMed] [Google Scholar]
- 44.Kawaguchi T, Azuma K, Yamaguchi T, Soeda H, Sekine Y, Koinuma M, et al. Development and validation of the Japanese version of the decisional conflict scale to investigate the value of pharmacists’ information: a before and after study. BMC Med Inform Decis Mak. 2013;13:50. doi: 10.1186/1472-6947-13-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Hirsch O, Keller H, Müller-Engelmann M, Gutenbrunner MH, Krones T, Donner-Banzhoff N. Reliability and validity of the German version of the OPTION scale. Health Expect Int J Public Particip Health Care. 2012;15:379–388. doi: 10.1111/j.1369-7625.2011.00689.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Nicolai J, Moshagen M, Eich W, Bieber C. The OPTION scale for the assessment of shared decision making (SDM): methodological issues. Z Für Evidenz Fortbild Qual Im Gesundheitswesen. 2012;106:264–271. doi: 10.1016/j.zefq.2012.03.002. [DOI] [PubMed] [Google Scholar]
- 47.Keller H, Hirsch O, Müller-Engelmann M, Heinzel-Gutenbrunner M, Krones T, Donner-Banzhoff N. Trying to optimise the German version of the OPTION scale regarding the dyadic aspect of shared decision making. Methods Inf Med. 2013;52:514–521. doi: 10.3414/ME13-01-0011. [DOI] [PubMed] [Google Scholar]
- 48.Ferronparayre A, Labrecque M, Rousseau M, Turcotte S, Légaré F. Validation of SURE, a four-item clinical checklist for detecting decisional conflict in patients. Med Decis Mak. 2014;34:54–62. doi: 10.1177/0272989X13491463. [DOI] [PubMed] [Google Scholar]
- 49.Jonsdottir T, Jonsdottir H, Gunnarsdottir S. Validation of the patients’ perceived involvement in care scale among patients with chronic pain. Scand J Caring Sci. 2013;27:740–749. doi: 10.1111/j.1471-6712.2012.01066.x. [DOI] [PubMed] [Google Scholar]
- 50.Lascuevas C, Perestelo-Perez L, Rivero-Santana A, Cebolla-Martí A, Scholl I, Härter M. Validation of the Spanish version of the 9-item shared decision-making questionnaire. Health Expect Int J Public Particip Health Care Health Policy. 2014. [DOI] [PMC free article] [PubMed]
- 51.Linder SK, Swank PR, Vernon SW, Mullen PD, Morgan RO, Volk RJ. Validity of a low literacy version of the decisional conflict scale. Patient Educ Couns. 2011;85:521–524. doi: 10.1016/j.pec.2010.12.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Elwyn G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P, et al. shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27:1361–1367. doi: 10.1007/s11606-012-2077-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Légaré F, Leblanc A, Robitaille H, Turcotte S. The decisional conflict scale: moving from the individual to the dyad level. Z Für Evidenz Fortbild Qual Im Gesundheitswesen. 2012;106:247–252. doi: 10.1016/j.zefq.2012.02.021. [DOI] [PubMed] [Google Scholar]
- 54.Légaré F, Elwyn G, Fishbein M, Frémont P, Frosch D, Gagnon M-P, et al. Translating shared decision-making into health care clinical practices: proof of concepts. Implement Sci. 2008;3:2. doi: 10.1186/1748-5908-3-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Stacey D, Légaré F, Pouliot S, Kryworuchko J, Dunn S. Shared decision making models to inform an interprofessional perspective on decision making: a theory analysis. Patient Educ Couns. 2010;80:164–172. doi: 10.1016/j.pec.2009.10.015. [DOI] [PubMed] [Google Scholar]
- 56.Braddock CH, III, Edwards KA, Hasenberg NM, Laidley TL, Levinson W. informed decision making in outpatient practice: time to get back to basics. JAMA. 1999;282:2313. doi: 10.1001/jama.282.24.2313. [DOI] [PubMed] [Google Scholar]