

Abstract
Background: As the third leading cause of death, cancers have a special place in the Iranian health system. Several studies have been done in some regions of the country with few years of follow-ups, but this was the first standardized study to investigate the incidence trends of colorectal cancer in Iran in a one-decade period.
Methods: The registered data for colorectal cancer cases in National Cancer Registry System were extracted from the Center for Disease Control & Management of Ministry of Health. The codes from 18 to 21 among cancers were selected for colon and rectum cancers. Incidence rates were directly standardized, using WHO population. The significance of incidence rate trends was tested through Poisson regression.
Results: In this study, 36,650 cases of colorectal cancer were observed for 10 years in Iran, which increased from 813 cases in 2000 to 6,210 cases in 2009. Gender ratio of men to women was 1.39. Significant increasing trends of colorectal cancer were observed during the period of the study. The standardized incidence rate increased from 1.6 per 100,000 persons per year in 2000 to 11.3 in 2009 in males (p<0.001), and it increased from 1.6 per 100,000 persons per year in 2000 to 10.9 in 2009 in females (p<0.001).
Conclusion: Colorectal cancer has an increasing trend in Iran. The rising trend of colorectal cancer as well as other types of cancers is partially due to improvement in cancer registry systems in the early years of registry. Moreover, westernized lifestyle and an increase in environmental risks could explain this rising trend.
Keywords: Incidence Trend, Colorectal, Cancer, Iran
Introduction
Colorectal cancer (CRC) is a major health problem (1,2). According to the global and international statistics, colorectal cancer is the third most common cancer and the third leading cause of cancer death in both genders worldwide (3). In Iran, CRC is the fourth leading cause of death (4) and the third most major cancer after stomach and breast cancer in both genders (5). Colorectal cancer is a fatal and epidemic disease (6). According to special reports, one death occurs due to colorectal cancer in every nine minutes (7). The CRC mortality rate is about two per 100,000 persons per year (8). The CRC incidence rate has been rising over the last 25 years (9). It is between 8-7 per 100,000 persons per year in both genders in Iran (10). This rate is lower than the rate in Western countries (5,11). Data on the prevalence and incidence of cancers in Iran suggest that the incidence rate of colorectal cancer is increasing (12). CRC usually affects people after the age of 55 (13), but recent studies have revealed that 7% of patients diagnosed with CRC are younger than 40 in Iran (14,15),and a half of the Iranian colorectal cancer patients are typically younger than 50 years of age (11). Major differences have been observed in the distribution of colorectal cancer because of the differences in lifestyle and environmental factors (16). Economically transitioning countries and industrialized countries have higher incidence rate (17,18). The incidence rate of colorectal cancer has declined significantly in the United States because of the effective interventions, implementation of earlier screening programs and change in the lifestyle (19). Prognosis of colorectal cancer is helpful if diagnosed early (20), but unfortunately, less than 40% of the cases are diagnosed at local stage (21). Earlier screening is an effective method to reduce the burden of colorectal cancer (22). Generally, screening programs are recommended for average-risk individuals aged 50, but those at high risk should be screened earlier (19). With the increasing trend of this cancer, it is expected to become the major cause of mortality in Asia (23). About 15 million new cases of colorectal cancer and one million new deaths are expected by 2020 (16). Considering the fact that the CRC index varies in different countries and due to the lack of sufficient data on its incidence trends in Iran, this study was designed to investigate the incidence trend of colorectal cancer during 2000-2009 in Iran. The results of this study may help the National Health Planning Center to better control and manage this particular type of cancer.
Methods
This was a cross-sectional population-based study, for which the registered data for colorectal cancer for 2000- 2009 were obtained from the Ministry of Health and Medical Education, and Center for Disease Control (CDC). Data were collected from all pathology centers throughout the country at the end of each year. After receiving the data, CDC controlled the data in terms of proper coding, missing in demographic information, and deleting the repeated cases. Meanwhile, cancers were coded based on International Classification of Diseases ICD-O (24). The C18-C21 codes were extracted for colon and rectum cancers. The results of national census data in 2006 were used to calculate the crude and age-specific incidence. By computing the annual growth rate of 1.01% and based on the population census in 2006, the population of Iran was estimated for the years 2000, 2001, 2002, 2003 2004, and 2005. In addition, WHO standard population was used as the standard population. Using direct method and Stata11 software, age- and gender-standardized incidence rates were computed for various age and gender groups separately. Incidence rates for 2006-2009 were extracted from annual national cancer reports. Poisson regression model was used to assess the significance of the incidence trends. The significance level was set at p<0.05. Then the 2007 version of the Excel software was used to draw the diagrams.
Results
During the 10-year period in Iran, 36,650 cases (19,515 men (53.2%) and 17,135 women (46.8%)) with colorectal cancer were registered; this rate had increased from 813 cases in 2000 to 6,210 cases in 2009. More than half of the cases were reported between 2006 and 2009. The mean±SD average age of all the cases was 57.0±15.04 yrs., which was 55.5±14.5 yrs. and 58.6±15.39 yrs., in women and men, respectively. The age-standardized incidence rate was significantly increased from 1.6 in 2000 to 11.1 cases per 100,000 persons per year in 2009 in Iran (Table 1). This rate increased from 1.6 in 2000 to 11.3 in 2009 cases per 100,000 persons in men, and from 1.6 in 2000 to 10.9 cases per 100,000 persons per year in 2009 in women (Table 1). Similar changes were observed in the incidence rate in both genders, indicating that the age-standardized incidence rate had declined in both genders in 2001, but it increased again noticeably in 2005 and then it experienced a slight fluctuating slope (Fig. 1). Colorectal cancer incidence rate was higher in women than in men until 2005, and after this date, men experienced a higher incidence (Fig. 1). Comparison of the incidence trend in different age groups showed that the incidence rate was the minimum in the younger age groups, but it increased in older age groups (Fig. 2). This increase was more evident after the age of 40 and its maximum was observed in those over 80 years of age, as the age-standardized incidence rate in this group had increased from 13.2 in 2000 to 145.1 per 100,000 persons per year in 2009 (Table 2). The change was minor in younger age groups (younger than 20 yrs.) but it decreased slightly and then increased in the over 50 year old groups (Fig. 3). The incidence rate has increased from the young to the old age groups (Fig. 2).
Table 1. Age Standardized Rate of Colorectal Cancer Incidence in Iran during 2000-2009 (Per100,000 Persons) .
| Year | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | Slope/ P Value | |
| Iran | Male | 1.6 | 1.4 | 3.4 | 5.8 | 6.7 | 8.3 | 9.0 | 9.6 | 12.7 | 11.3 | -2.48/ (<0.001) |
| Female | 1.6 | 1.5 | 3.4 | 6.2 | 7.3 | 9.1 | 8.2 | 8.9 | 9.8 | 10.9 | -2.52/ (< 0.001) | |
| Total | 1.6 | 1.5 | 3.4 | 6 | 7 | 8.7 | 8.6 | 9.2 | 11.3 | 11.1 | -2.50/ (< 0.001) | |
Fig. 1 .
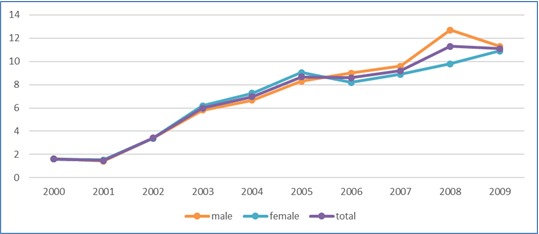
Age Standardized Incidence Rate of Colorectal Cancer in Iran during 2000-2009 by Gender
Fig. 2 .
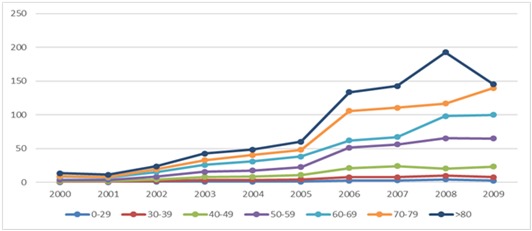
Age Standardized Incidence Rate of Colorectal Cancer in Iran during 2000-2009 by Age Groups
Table 2. Age Standardized Rate of Colorectal Cancer Incidence in Iran during 2000-2009 (Per100,000 Persons) in Different Age Groups in both Genders .
| Age group (yrs) | Gender | Year | ||||||||||
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | Slope/ P Value | ||
| 0-29 | Male | 0.3 | 0.3 | 0.5 | 0.7 | 0.8 | 1.0 | 2.7 | 2.8 | 3.8 | 2 | -4.03(< 0.001) |
| Female | 0.2 | 0.3 | 0.4 | 0.7 | 0.8 | 0.9 | 2.1 | 2.6 | 4.2 | 2.7 | -3.72(< 0.001) | |
| Total | 0.2 | 0.3 | 0.4 | 0.7 | 0.8 | 1.0 | 2.4 | 2.7 | 4.0 | 2.4 | -3.72(< 0.001) | |
| 30-39 | Male | 0.6 | 0.8 | 1.8 | 2.9 | 3.0 | 3.1 | 8.1 | 7.7 | 11.4 | 7.1 | -2.89(< 0.001) |
| Female | 0.6 | 0.8 | 2.1 | 3.1 | 4.0 | 5.2 | 6.7 | 7.1 | 7.9 | 7.8 | -2.91(< 0.001) | |
| Total | 0.6 | 0.8 | 1.9 | 3.0 | 3.5 | 4.1 | 7.4 | 7.4 | 9.6 | 7.5 | -2.93(< 0.001) | |
| 40-49 | Male | 1.8 | 1.5 | 3.5 | 6.1 | 6.9 | 8.7 | 21.2 | 24.6 | 30 | 21.5 | -1.89(< 0.001) |
| Female | 1.7 | 2.1 | 4.6 | 9.3 | 9.8 | 13.2 | 21.1 | 23.4 | 10.2 | 24.6 | -1.94(< 0.001) | |
| Total | 1.7 | 1.8 | 4.0 | 7.7 | 8.3 | 10.9 | 21.2 | 24.0 | 20.1 | 23.0 | -1.92(< 0.001) | |
| 50-59 | Male | 3.2 | 2.7 | 7.4 | 14.2 | 14.9 | 18.5 | 56.6 | 60.1 | 81.7 | 63.7 | -0.87(< 0.001) |
| Female | 4.0 | 3.9 | 9.0 | 16.8 | 19.9 | 26.0 | 46.1 | 51.7 | 48.8 | 66.0 | -1.05(< 0.001) | |
| Total | 3.6 | 3.3 | 8.2 | 15.5 | 17.4 | 22.3 | 51.4 | 55.9 | 65.2 | 64.8 | -1.00(< 0.001) | |
| 60-69 | Male | 8.3 | 7.2 | 16.3 | 25.9 | 31.5 | 39.6 | 55.5 | 61.8 | 78.2 | 104.1 | -0.67(< 0.001) |
| Female | 7.9 | 6.5 | 14.2 | 25.7 | 30.5 | 36.8 | 68.0 | 72.1 | 117.8 | 95.9 | -0.56(< 0.001) | |
| Total | 8.1 | 6.9 | 15.2 | 25.8 | 31.0 | 38.2 | 61.8 | 66.9 | 98.0 | 100.0 | -0.61(< 0.001) | |
| 70-79 | Male | 9.7 | 8.7 | 21.5 | 34.9 | 41.9 | 53.0 | 117.3 | 117.7 | 159.2 | 154.2 | -0.15(< 0.001) |
| Female | 7.9 | 6.7 | 16.2 | 29.7 | 38.6 | 42.1 | 93.9 | 103.2 | 74.2 | 125.6 | -0.44(< 0.001) | |
| Total | 8.9 | 7.8 | 19.0 | 32.5 | 40.4 | 47.9 | 105.6 | 110.4 | 116.7 | 139.9 | -0.28(< 0.001) | |
| 80< | Male | 13.0 | 10.7 | 24.5 | 46.7 | 54.5 | 67.8 | 149.6 | 172.5 | 230.1 | 167.8 | 0.11(< 0.001) |
| Female | 13.3 | 11.8 | 22.5 | 38.2 | 41.7 | 52.0 | 117.5 | 113.2 | 155.2 | 122.4 | -0.19(< 0.001) | |
| Total | 13.2 | 11.2 | 23.5 | 42.6 | 48.4 | 60.2 | 133.5 | 142.6 | 192.7 | 145.1 | -0.02(0.446) | |
Fig. 3 .
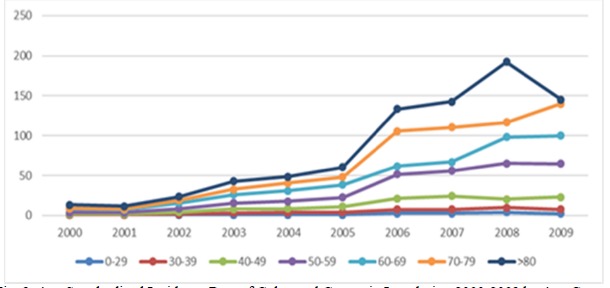
Age Standardized Incidence Rate of Colorectal Cancer in Iran during 2000-2009 by Age Groups
Discussion
The overall results of this study indicated that the incidence trend of colorectal cancer in Iran has been rising and has increased approximately 6.9 times during the past ten years. With respect to the rising trend of colorectal cancer in Iran in a global context, many studies have found that the incidence of colorectal cancer for both genders has increased in Eastern Europe and certain parts of South America as well as in many parts of Asia in the recent years. However, it declined in both genders in the United States, Canada and New Zealand (25). In Asian countries, such as Japan (26), Tunisia (27) Singapore (28) and Saudi Arabia (29) this rising trend has also been reported. In Asia, an increase in the incidence of colorectal cancer has been observed due to the increase in the population or increase in the number of relative risk groups, better diagnosis and aging of the population and the growing population density of the area in the last two decades (30). The most important risk factors for this cancer include change in lifestyle and personal habits, age over 50 and family history (19). Change in personal habits includes tendency to fast food consumption and a diet low in fiber or high in fat, high consumption of meat and meat products and tobacco as well as low consumption of fresh fruit and vegetables (31,32). Of lifestyle-related factors, such causes as sedentary lifestyle and reduced physical activity and increased rates of obesity can be mentioned (33).Increased exposure to such factors could include logical rationales for increasing the trend of colorectal cancer in Iranian society.
The respect to the incidence according to gender, our study found that the incidence rate of colorectal cancer was higher in women than men up to 2005, but there was a higher incidence in men in later years of the study, and the rising trend has had similar changes in both genders. A study in China during 1993-1997 has reported higher incidence in women than in men (34). In addition, a study in Cambodia during 2005-2010 found more incidence of colorectal cancer in women than in men (35). However, most studies conducted in Iran (36,37), Bahrain (38), Canada (39) and the United States (19) represent a lower incidence in women than in men and the reason could be healthier eating habits in women (40). Such a contradiction regarding the results of other countries may be due to the different prevalence of this cancer in the two genders, effects of environmental changes and other risk factors and different exposures in communities.
The results revealed that the incidence rate increased with an increase in age, and this figure was lower in the younger than 20 age groups, but it increased in the older groups; therefore, it can be concluded that this disease becomes dominant after the age of 40 and reaches its maximum in the group above 80 years of age. The trend in the changes was partial in the younger age groups and it was steeper in older age groups. Such a result was consistent with other studies in Canada (39), Singapore (28) and Iran (41). The incidence of colorectal cancer is increasing at older ages in Asia due to overpopulation and increase in the population age (30). The phenomenon of rising the mean age and the population aging may be considered as factors affecting the overall trend rising in the incidence of cancers and colorectal cancer in Iran, as the aging population is a major natural predisposing factor of colorectal cancer (42). As the colorectal cancer incidence rate reaches the peak in the older age groups, it explains a proportion of the increased trend in the incidence of this cancer in Iran. Among the reasons of high incidence in the older age groups, increased exposure to high-risk lifestyle and diet in early life stages can be mentioned (28). As such, a study in Japan suggests that exposure to risk factors at younger ages, increases the incidence risk in the 6th and 7th decades of life (43). It is predicted that by 2030, 70% of malignancies will occur in the age group over 65 (44). Other reasons to be mentioned include a decline in mobility in the older population, and low incidence in the younger age groups due to different effects of westernization on the youths compared to the elderly (45) and lower exposure of the youths to risks from environmental changes (36).
High incidence of colorectal cancer in Iran can be generally attributed to two factors:
True change in the incidence of colorectal cancer, which can be caused by changes in the frequency of exposure to the disease risk factors, most important of which are changes in lifestyle and individual habits (19).
Some reasons for the change in the incidence of the disease can be due to the improved data collection approach associated with cancer registration system. According to the Iranian cancer registration system, coverage of registry had an increasing trend particularly from 2004 to 2005. Similar trends of the incidence during this period was observed in skin (46) andgastric (47,48)cancers, indicating that a part of rising in the incidence is due to changing in cancer registry system and developmental problems. Therefore, the process of cancer registration system (49) should be considered in the interpretation of the results in all cancer researches in Iran.
Conclusion
A percentage of the increase can be due to the result of improved registration and reporting systems on the new cases of cancer. Despite the registration system improvement, our study showed the direction of the processes and predicted the patterns of changes. This study provides a suitable evidence and context for further analyses of cancer registry system.
Acknowledgments
The authors would like to thank Kermanshah University of Medical Sciences for the grant provided for this study.
Cite this article as: Abdifard E, Amini S, Bab S, Masroor N, Khachian A, Heidari M. Incidence trends of colorectal cancer in Iran during 2000-2009: A population-based study. Med J Islam Repub Iran 2016 (5 June). Vol. 30:382.
References
- 1.Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M. et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):359–86. doi: 10.1002/ijc.29210. [DOI] [PubMed] [Google Scholar]
- 2.Wiseman M. The second World Cancer Research Fund/American Institute for Cancer Research expert report Food, nutrition, physical activity, and the prevention of cancer: a global perspective. Proc Nutr Soc. 2008;67(3):253–6. doi: 10.1017/S002966510800712X. [DOI] [PubMed] [Google Scholar]
- 3.Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30. doi: 10.3322/caac.21166. [DOI] [PubMed] [Google Scholar]
- 4.Malekzadeh R, Bishehsari F, Mahdavinia M, Ansari R. Epidemiology and molecular genetics of colorectal cancer in Iran: a review. Arch Iran Med. 2009;12(2):161–9. [PubMed] [Google Scholar]
- 5.Kolahdoozan S, Sadjadi A, Radmard AR, Khademi H. Five common cancers in Iran. Arch Iran Med. 2010;13(2):143–6. [PubMed] [Google Scholar]
- 6. National Report on Cancer Registry, 2005. Tehran: Iranian Ministry of Health and Medical Education – Deputy of Health, Center for Disease Control 2007.
- 7.Benson AB. Epidemiology, disease progression, and economic burden of colorectal cancer. J Manag Care Pharm. 2007;13(6 Suppl C):5–18. doi: 10.18553/jmcp.2007.13.s6-c.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Death in 23 Provinces of Iran. Tehran: Iranian Ministry of Health and Medical Education, Deputy of Health, Center for Network Development and Health promotion and Applied Research Secretariat 2003.
- 9.Azadeh S, Moghimi-Dehkordi B, Fatem SR, Pourhoseingholi MA, Ghiasi S, Zali MR. Colorectal cancer in Iran: an epidemiological study. Asian Pac J Cancer Prev. 2008;9(1):123–6. [PubMed] [Google Scholar]
- 10.Mahdavinia M, Bishehsari F, Ansari R, Norouzbeigi N, Khaleghinejad A, Hormazdi M. et al. Family history of colorectal cancer in Iran. BMC Cancer. 2005;5:112. doi: 10.1186/1471-2407-5-112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Moghimi-Dehkordi B, Safaee A, Zali MR. Prognostic factors in 1,138 Iranian colorectal cancer patients. Int J Colorectal Dis. 2008;23(7):683–8. doi: 10.1007/s00384-008-0463-7. [DOI] [PubMed] [Google Scholar]
- 12.Pahlavan PS, Jensen K. A short impact of epidemiological features of colorectal cancer in Iran. Tumori. 2005;91(4):291–4. doi: 10.1177/030089160509100401. [DOI] [PubMed] [Google Scholar]
- 13.Atkin WS, Edwards R, Kralj-Hans I, Wooldrage K, Hart AR, Northover JM. et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicenter randomized controlled trial. Lancet. 2010;375(9726):1624–33. doi: 10.1016/S0140-6736(10)60551-X. [DOI] [PubMed] [Google Scholar]
- 14.Meyer JE, Narang T, Schnoll-Sussman FH, Pochapin MB, Christos PJ, Sherr DL. Increasing incidence of rectal cancer in patients aged younger than 40 years: an analysis of the surveillance, epidemiology and end results database. Cancer. 2010;116(18):4354–9. doi: 10.1002/cncr.25432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.O'Connell JB, Maggard MA, Liu JH, Etzioni DA, Livingston EH, Ko CY. Rates of colon and rectal cancers are increasing in young adults. Am Surg. 2003;69(10):866–72. [PubMed] [Google Scholar]
- 16.Ganesh B, Talole SD, Dikshit R. A case-control study on diet and colorectal cancer from Mumbai, India. Cancer Epidemiol. 2009;33(3-4):189–93. doi: 10.1016/j.canep.2009.07.009. [DOI] [PubMed] [Google Scholar]
- 17.Cress RD, Morris C, Ellison GL, Goodman MT. Secular changes in colorectal cancer incidence by subsite, stage at diagnosis, and race/ethnicity, 1992-2001. Cancer. 2006;107(5 Suppl):1142–52. doi: 10.1002/cncr.22011. [DOI] [PubMed] [Google Scholar]
- 18.Sonnenberg A, Delco F, Inadomi JM. Cost-effectiveness of colonoscopy in screening for colorectal cancer. Ann Intern Med. 2000;133(8):573–84. doi: 10.7326/0003-4819-133-8-200010170-00007. [DOI] [PubMed] [Google Scholar]
- 19. American Cancer Society. Colorectal cancer, Facts & figures (2013). www.cancer.org/downloads/stt/F861708_finalforweb.pdf.Accessed 7/7/ 2015.
- 20.Ciccolallo L, Capocaccia R, Coleman MP, Berrino F, Coebergh JW, Damhuis RA. et al. Survival differences between European and US patients with colorectal cancer: role of stage at diagnosis and surgery. Gut. 2005;54(2):268–73. doi: 10.1136/gut.2004.044214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kong CK, Roslani AC, Law CW, Law SC, Arumugam K. Impact of socio-economic class on colorectal cancer patient outcomes in Kuala Lumpur and Kuching, Malaysia. Asian Pac J Cancer Prev. 2010;11(4):969–74. [PubMed] [Google Scholar]
- 22.Levin B, Lieberman DA, McFarland B, Smith RA, Brooks D, Andrews KS. et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58(3):130–60. doi: 10.3322/CA.2007.0018. [DOI] [PubMed] [Google Scholar]
- 23.Pignone M, Rich M, Teutsch SM, Berg AO, Lohr KN. Screening for colorectal cancer in adults at average risk: a summary of the evidence for the US Preventive Services Task Force. Ann Intern Med. 2002;137(2):132–41. doi: 10.7326/0003-4819-137-2-200207160-00015. [DOI] [PubMed] [Google Scholar]
- 24. Constance P, Valerie V, Calum M. International Classification of Disease for Oncology. 2nd ed. WHO, Geneva 2000.
- 25.Center MM, Jemal A, Ward E. International trends in colorectal cancer incidence rates. Cancer Epidemiol Biomarkers Prev. 2009;18(6):1688–94. doi: 10.1158/1055-9965.EPI-09-0090. [DOI] [PubMed] [Google Scholar]
- 26.Kuriki K, Tajima K. The increasing incidence of colorectal cancer and the preventive strategy in Japan. Asian Pac J Cancer Prev. 2006;7(3):495–501. [PubMed] [Google Scholar]
- 27.Missaoui N, Jaidaine L, Abdelkader AB, Trabelsi A, Mokni M, Hmissa S. Colorectal cancer in Central Tunisia: increasing incidence trends over a 15-year period. Asian Pac J Cancer Prev. 2011;12(4):1073–6. [PubMed] [Google Scholar]
- 28.De KI, Wong CS, Chia KS, Sim X, Tan CS, Kiemeney LA. et al. Gender differences in the trend of colorectal cancer incidence in Singapore, 1968-2002. Int J Colorectal Dis. 2008;23(5):461–7. doi: 10.1007/s00384-007-0421-9. [DOI] [PubMed] [Google Scholar]
- 29.Mosli MH, Al-Ahwal MS. Colorectal cancer in the Kingdom of Saudi Arabia: need for screening. Asian Pac J Cancer Prev. 2012;13(8):3809–13. doi: 10.7314/apjcp.2012.13.8.3809. [DOI] [PubMed] [Google Scholar]
- 30.Yee YK, Tan VP, Chan P, Hung IF, Pang R, Wong BC. Epidemiology of colorectal cancer in Asia. J Gastroenterol Hepatol. 2009;24(12):1810–6. doi: 10.1111/j.1440-1746.2009.06138.x. [DOI] [PubMed] [Google Scholar]
- 31.Mark-Wahnefried W, Rock CL, Patrick K, Byers T. Lifestyle interventions to reduce cancer risk and improve outcomes. Am Fam Physician. 2008;77(11):1573–8. [PubMed] [Google Scholar]
- 32.Norat T, Bingham S, Ferrari P, Slimani N, Jenab M, Mazuir M. et al. Meat, fish, and colorectal cancer risk: the European Prospective Investigation into cancer and nutrition. J Natl Cancer Inst. 2005;97(12):906–106. doi: 10.1093/jnci/dji164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Anzuini F, Battistella A, Izzotti A. Physical activity and cancer prevention: a review of current evidence and biological mechanisms. J Prev Med Hyg. 2011;52(4):174–80. [PubMed] [Google Scholar]
- 34.Li L, Wang QJ, Zhu WX. The control study on causes of colon cancer with risk factors in Beijing. Chinese Journal of Clinical. 2013;30:556–8. [Google Scholar]
- 35.Hav M, Eav S, Ky V, Cuvelier C, In S, Kong R. et al. Colorectal cancer in young Cambodians. Asian Pac J Cancer Prev. 2011;12(4):1001–5. [PubMed] [Google Scholar]
- 36.Ansari R, Mahdavinia M, Sadjadi A, Nouraie M, Kamangar F, Bishehsari F. et al. Incidence and age distribution of colorectal cancer in Iran: results of a population-based cancer registry. Cancer Lett. 2006;240(1):143–7. doi: 10.1016/j.canlet.2005.09.004. [DOI] [PubMed] [Google Scholar]
- 37.Safaee A, Fatemi SR, Ashtari S, Vahedi M, Moghimi-Dehkordi B, Zali MR. Four years incidence rate of colorectal cancer in Iran: a survey of national cancer registry data - implications for screening. Asian Pac J Cancer Prev. 2012;13(6):2695–8. doi: 10.7314/apjcp.2012.13.6.2695. [DOI] [PubMed] [Google Scholar]
- 38.Alsayyad J, Hamadeh R. Cancer incidence among the Bahraini population: A five-year (1998-2002) experience. Ann Saudi Med. 2007;27(4):251–258. doi: 10.5144/0256-4947.2007.251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Gao RN, Neutel CI, Wai E. Gender differences in colorectal cancer incidence, mortality, hospitalizations and surgical procedures in Canada. J Public Health (Oxf) 2008;30(2):194–201. doi: 10.1093/pubmed/fdn019. [DOI] [PubMed] [Google Scholar]
- 40.Denton M, Prus S, Walters V. Gender differences in health: a Canadian study of the psychosocial, structural and behavioural determinants of health. Soc Sci Med. 2004;58(12):2585–600. doi: 10.1016/j.socscimed.2003.09.008. [DOI] [PubMed] [Google Scholar]
- 41.Abdifard E, Ghaderi S, Hosseini S, Heidari M. Incidence trends of colorectal cancer in the West of Iran during 2000-2005. Asian Pac J Cancer Prev. 2013;14(3):1807–11. doi: 10.7314/apjcp.2013.14.3.1807. [DOI] [PubMed] [Google Scholar]
- 42.Ponz de LM, Marino M, Benatti P, Rossi G, Menigatti M, Pedroni M. et al. Trend of incidence, subsite distribution and staging of colorectal neoplasms in the 15-year experience of a specialized cancer registry. Ann Oncol. 2004;15(6):940–6. doi: 10.1093/annonc/mdh224. [DOI] [PubMed] [Google Scholar]
- 43.Yiu HY, Whittemore AS, Shibata A. Increasing colorectal cancer incidence rates in Japan. Int J Cancer. 2004;109(5):777–81. doi: 10.1002/ijc.20030. [DOI] [PubMed] [Google Scholar]
- 44.Balducci L. Epidemiology of cancer and aging. J Oncol Manag. 2005;14(2):47–50. [PubMed] [Google Scholar]
- 45.Yee YK, Gu Q, Hung I, Tan VP, Chan P, Hsu A. et al. Trend of colorectal cancer in Hong Kong: 1983-2006. J Gastroenterol Hepatol. 2010;25(5):923–7. doi: 10.1111/j.1440-1746.2009.06130.x. [DOI] [PubMed] [Google Scholar]
- 46.Heidari M, Najafi F. Trends of skin cancer incidence in 6 geographical regions of the Islamic Republic of Iran, 2000–2005. East Mediterr Health J. 2013;19(1):59–65. [PubMed] [Google Scholar]
- 47.Haidari M, Nikbakht MR, Pasdar Y, Najafi F. Trend analysis of gastric cancer incidence in Iran and its six geographical areas during 2000-2005. Asian Pac J Cancer Prev. 2012;13(7):3335–41. doi: 10.7314/apjcp.2012.13.7.3335. [DOI] [PubMed] [Google Scholar]
- 48.Rahimi F, Heidari M. Time trend analysis of stomach cancer incidence in the west of Iran. J Health Development. 2012;1(2):100–111. [Google Scholar]
- 49.Grocott P, Richardson A, Ambaum B, Kearney N, Redmond K. Nursing in Colorectal Cancer Initiative: the audit phase Part 2 Content validity of the audit tool and implications of the standards set for clinical practice. Eur J Oncol Nurs. 2001;5(3):165–73. doi: 10.1054/ejon.2001.0140. [DOI] [PubMed] [Google Scholar]