

Abstract
When performing cementless hip arthroplasty, it is critical to achieve firm primary mechanical stability followed by biological fixation. In order to achieve this, it is essential to fully understand characteristics of implant design. In this review, the authors review fixation principles for a variety of implants used for cementless hip replacement and considerations for making an optimal selection.
Keywords: Hip replacement arthroplasty, Cementless, Implant design
INTRODUCTION
One of the most important factors in driving a successful cementless total hip arthroplasty (THA) is achieving osteointegration between implant and bone. Although multiple factors impacting osteointegration, implant design, appropriate surface treatment, primary mechanical stability, and patient's osteogenesis are the most critical1). In this review, the authors review fixation principles of respective cementless hip replacement implants and considerations for making an optimal selection.
SURFACE TREATMENT OF CEMENTLESS HIP REPLACEMENT IMPLANTS
Osteointegration can be achieved by bone ingrowth and bone ongrowth. Bone ingrowth indicates firm fixation between bone and metal through bone growth into the porous surface of metal implants. Meanwhile, bone ongrowth is fixation between metal and bone via bone growth on the rough surface of an implant. Depending upon the surface treatment, mechanisms of biological fixation differ2).
DESIGN OF ACETABULAR CUP
Acetabular cups can be classified as either cemented or cementless depending on the presence or absence of cement used during fixation. In this chapter, we discuss the design of surface-treated hemispherical press-fit acetabular cups, currently the most widely utilized cementless acetabular cups.
1. Surface-treated Press-fit Fixation Cup
Press-fit fixation is a technique which uses physical force on the substance to be inserted so that maximal press fit can be achieved by surrounding material. For this application, the size of press-fit fixation acetabular cups are generally 1–4 mm bigger than reaming diameter so that viscoelasticity of acetabulum maximizes the binding force of acetabular cups3).
Theoretically, the press-fit method does not require additional fixation such as the use of screws since sufficient primary fixation can be achieved. However, additional screw fixation might be used in the certain cases if press-fit fixation is not satisfactory. Further, inexperienced orthopedic surgeons may judge the gap between acetabular bone and cup through screw holes thus it is recommended to select a cup design with screw holes.
2. Evolution of Cementless Hemispherical Acetabular Cups
Cementless acetabular cups have evolved through three generations based on their development periods and design characteristics4).
1) 1st generation hemispherical acetabular cups
These acetabular cups were an early design developed in the 1980s. Extension of the polyethylene liner was designed to be extruded from the acetabular cup for assembly. However, extruded liners were easily damaged by impingement as liners were somewhat thin and fragile; this results in frequent damage of the locking mechanism and following liner dissociation. Further, congruity was not sufficient, and there often was a gap between liners and the inner surface of acetabular cups in which the back-side of liners was subjected to wear (Fig. 1).
Fig. 1. 1st generation of hemispherical acetabular cup: Harris-Galante I cup (Zimmer, USA).

2) 2nd generation hemispherical acetabular cups
The 2nd generation design was improved from the 1st generation in the 1990s. Extruded liners out of acetabular cups were much thicker and were designed to endure impingement better. In addition, congruity between the liner and the acetabular cup was further improved, significantly reducing the dissociation of liners (Fig. 2).
Fig. 2. 2nd generation of hemispherical acetabular cup: Trilogy cup (Zimmer, USA).

3) 3rd generation hemispherical acetabular cups
This generation was introduced in 2000s. Liners were designed not to be extruded from the acetabular cups to prevent direct collisions and damage of the locking mechanisms. Furthermore, congruity of the liner and acetabular cup was significantly improved whereas ceramic, metal and highly cross-linked polyethylene liners were able to be loaded. This generation makes up the majority of acetabular cups in recent days (Fig. 3).
Fig. 3. Types of 3rd generation of hemispherical press-fix acetabular cups. (A) Metal bead coated Pinnacle cup (DePuy, USA). (B) Plasma spray coated Bencox cup (Corentec, Korea). (C) Tantalum coated Continuum cup (Zimmer, USA).

DESIGN OF FEMORAL STEM
Like the aforementioned factors, femoral stems can be classified as either cemented or cementless, depending upon their fixation methods. We will now discuss design concepts, classification, and characteristics of cementless stems.
1. Basic Elements of Cementless Femoral Stems
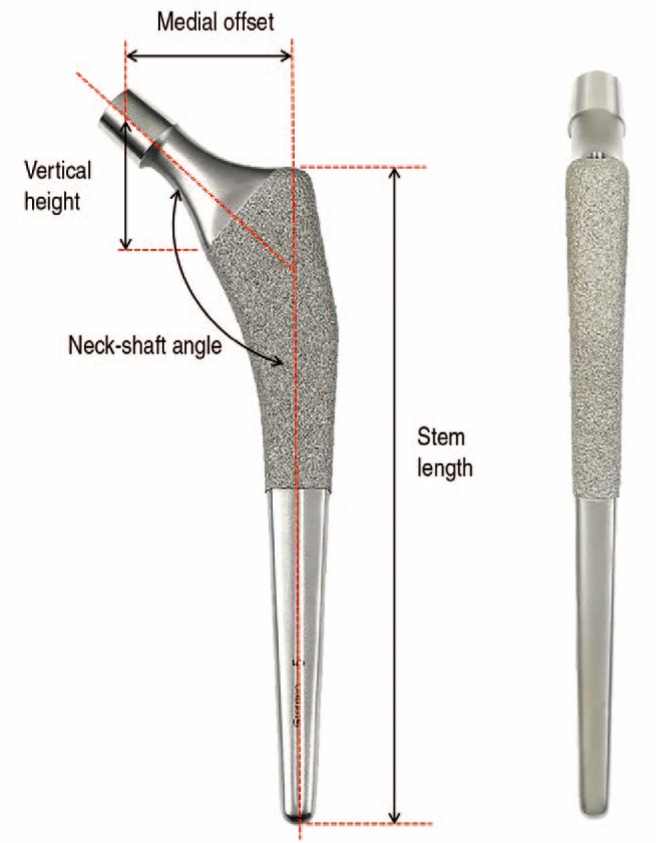
Generally speaking, femoral stems are designed to place the center of rotation at the native hip center. In order for this, vertical height, medial offset, and version of femoral region should be appropriate. The vertical height is often expressed as the height from the proximal margin of lesser trochanter to the center of femoral head. Medial offset is expressed as the distance between a line passing through the vertical axis of femoral stem and the center of femoral head. Last, the version indicates the rotation angle between proximal and distal parts of femurs. Depending on the length of implant neck, the medial offset and vertical height can be adjusted; similarly, the vertical height can be adjusted according to depths of femoral stem into femurs.
In addition, femoral stems represent approximately 125° – 135° of neck-shaft angle which also causes a difference in vertical height and medial offset. Moreover, depending upon their design, femoral stems may have different femoral stem lengths, diameter and width of proximal and distal parts, and the angle narrowing down as approaching to the proximal part (Fig. 4). The measuring systsm of the factors could vary according to respective manufacturer, thus one should not make mistakes by comparing stems as solely relying on numerical values on product brochure.
Fig. 4. Design elements of cementless femoral stems.
2. Classification of Cementless Femoral Stem
Depending on the shape of the cementless stem, the contact site between the implant and femoral cortical bones might differ and can result in differences in primary stability and following biologic fixation. All cementless stem designs aim to achieve best fixation by maximizing primary fixation forces and secondary biological fixation.
When they initially came to market, femoral stems were classified only as either straight or curved; similarly they were divided as either fixing proximally on metaphysis or distally on diaphysis. As additional types of femoral stems were developed and introduced, they were classified and named according to different perspective and classification criteria. In the absence of unified classification systems, it was difficult to make direct comparison and scientific analyses among femoral stems. For instance, Callaghan et al.5) classified femoral stems into 7 different types; modular, extensively coated, hydroxy apatite (HA) coated, proximally ingrown, tapered, press-fit, and custom design. The modular was named per its modularity and extensively coated per the range of surface coating, the HA coating per the surface treatment method, proximally ingrown per surface treatment range and method, and tapered per stem shape, the press-fit per primary fixation method, custom design per manufacture type, respectively.
Similarly there are other classification methods in which femoral stems were divided into 5 categories; fit and fill, modular, distal fitting, proximal tapered wedge, and press-fit tapered wedge. In this classification, the fit and fill was defined by primary fixation method, the modular by modularity, the distal fitting by fixation site, the proximal tapered wedge by the range of surface treatment and shape, the press-fit tapered wedge by fixation method and shape, respectively. As demonstrated here, in order to minimize any potential confusion from classification and nomenclature by different perspective and criterion, further objective and homogenous criteria might be warranted.
3. Classification by the Mont Group
In 2011, the Mont group suggested a classification system for femoral stems with a total of 6 types defined based on the bone contact area and subdivisions of fixation sites (proximal to distal)1). This classification may not be without its limitations but it does provide a general criteria for femoral stem classification thereby making a direct comparison easier.
1) Type 1 stem
This design type might also be called the Single-wedge stem; the design is anteroposteriorly flat and mediolaterally wide with a distally tapering wedge shape. The surface treatment is generally on the proximal 1/3 to 5/8 of the implant and is intended to fix through insertion into the femoral canal between medial and lateral cortical bone of femoral metaphysis. In the lateral view, 3-point fixation is achieved through contact between the proximal posterior cortical bone, anterior cortical bone, and posterior cortical bone. Due to mediolaterally wide shape in the proximal part, it can provide excellent stability against rotation. Outstanding clinical outcomes have been reported, with 99% stem survival rate through more than 20 year follow up, using the type 1 stem6,7) (Fig. 5).
Fig. 5. Type 1 stems. (A) Bencox ID stem (Corentec, Korea). (B) Taperloc stem (Biomet, USA).

2) Type 2 stem
This design is also known as the Double wedge stem. The stem tapers in anteroposterior and mediolateral plane. Similar to the type 1 stems, the stem coating is only applied on the proximal portion. It was designed to fix via contacting the medial and lateral metahyseal cortex and anterior and posterior metaphyseal cortex. Compared to the type 1 stem, it is somewhat thick in anterior-posterior plane and fills most of the femoral metaphysis, hence its name, the metaphyseal-filling design. Approximately 95–100% stem survival rate has been reported through 15–20 year follow up8,9) (Fig. 6).
Fig. 6. Type 2 stems. (A) Summit stem (DePuy, USA). (B) Echo Bi-Metric stem (Biomet, USA).

3) Type 3 stem
This type is also known as the tapered stem as these stems taper distally in both the coronal and sagittal planes. Unlike type 1 and type 2, the contour of the stem is curved smoothly rather than abruptly. And these stems are not only surface-treated proximally but also distally, also distinct from types 1 and 2. Fixation is achieved at the metaphyseal-diaphyseal junction where normal medullary cavity of femurs gets narrow down. Type 3 stems can be further subdivided into three subgroups on the basis of their design characteristics.
(1) Type 3A: Conical design with rounded corners and a tapered shape in both planes. Coating is applied on one-third of the proximal portion and there are either protruding pins or wings that provide rotational stability. Type 3A has shown excellent stem survival rate (99%) over 10 year follow up10) (Fig. 7).
Fig. 7. Type 3A Mallory Head stem (Biomet, USA).

(2) Type 3B: Conical design with a distal taper. Multiple splines are raised throughout the longitudinal axis to provide primary fixation by embedding into the inner cortical bone of femurs. Since its proximal part is a relatively rounded cone, it can provide rotation in wide femoral metaphysis and is thus useful in cases that require some type of adjustment (e.g., anteversion) due to deformity of proximal femurs. Even though these are not widely utilized designs, 1) type 3B stems are mostly fixed in distal parts, and 2) proximal parts are rounded cones and thereby efficient in revision with bone loss and deformity11) (Fig. 8).
Fig. 8. (A) Type 3B Wagner stem (Zimmer, USA). (B, C) Cortical bone is fixed using multiple extruded thin plates thereby provide rotation stability.

(3) Type 3C: Rectangular cross section and thus called rectangular stems. Approaching the distal part, geometries of both anterior-posterior and medio-lateral planes are tapered with a wedge shape. The stems are mostly fixed at femoral metaphyseal-diaphyseal junction and at the proximal part of the diaphysis to obtain three point fixations in the sagittal plane. The stems are grit-blasted across their entire length. Its rectangular cross section provides strong rotational stability with 4 corners embedding into endosteal bone. This type of stems is being widely adopted in European countries and excellent stem survival rate has been reported (96%) through more than 20 year follow up12,13,14,15) (Fig. 9).
Fig. 9. Type 3C stems. (A) Bencox stem (Corentec, Korea). (B) Zweymüeller Alloclassic stem (Zimmer, USA). (C) CLS stem (Zimmer, USA).

4) Type 4 stem
Stems in this type are generally cylindrical and surface-treated throughout the entire length. The distal portion of the stems is designed to be fixed on femoral diaphysis. These stems are inserted into reamed diapysis and their diameters are slightly bigger by approximately 0.5 mm than reamed diameter. This type 4 stem has shown an excellent survival rate of 98% through more than 20 year long-term follow up; however, there is a limitation of stress shielding and thigh pain due to its fixation on distal part16,17) (Fig. 10).
Fig. 10. Type 4 stems. (A) AML stem (DePuy, USA). (B) Versys Beaded Fullcoat stem (Zimmer, USA).
5) Type 5 stem
The stems of type 5 are modular to allow independent preparation and separate components for the metaphysis and diaphysis. Thus, proximal and distal part of femur can be reamed separately, and the optimal size of separate metaphyseal sleeve and diaphyseal stem can be applied respectively.
Therefore, as the design is supposed to fix both metaphysis proximally and diaphysis distally, this type of stem is very useful for complex cases with anatomic abnormalities and rotational malalignments, such as are seen with hip dysplasia. Excellent survival rate of these stems (99%) was reported over 10–11 years of follow-up on average18,19) (Fig. 11).
Fig. 11. Type 5 stems. (A) S-ROM stem (DePuy, USA). (B) Revitan stem (Zimmer, USA). (C) Arcos stem (Biomet, USA).

6) Type 6 stem
The type 6 stems bow posteriorly so that they can be fitted into proximal femoral endosteal geometry and achieve maximal contact. These stems are called anatomical stems. They are conical and narrow proximally in both the anterior-posterior and medio-lateral planes. They maximally fill metaphysis first and the distal part of stem also fills diaphysis to be called the fit and fill design20,21,22). There are limited clinical reports to date and some reports indicate non-satisfactory clinical outcomes thus the design has not very commonly adopted to date (Fig. 12).
Fig. 12. Type 6 stem. The design of this stem type was intended to fit with proximal femurs; femoral stems are curved.

4. Short Femoral Stem
As the design with metaphyseal fixation are recently preferred, a question regarding the need to maintain a long distal part of femoral stems has led to the development of short femoral stem designs. Expected theoretical merits of this short femoral stems are as follows; 1) they are less invasive due to less loss of femoral bone stock, 2) patients experience less pain without stem parts stimulating diaphysis, 3) there is less stress shielding on proximal femurs. Although it has not been fully established with regards to definition of short femoral stems, Feyen and Shimmin23) previously defined it as stems with "total length less than twice tip of greater trochanter to base of lesser trochanter vertical distance".
Short femoral stems are not included in aforementioned classification of the Mont group, and their classification is not completely established yet. In 2014, the Mont group also proposed classifications for short femoral stems based on the loading sites on proximal part of femurs and stem fixation principles23). In this system, the short femoral stems are classified into 4 types depending on the increasing area for loading on the stem. Type 1 are femoral neck only, type 2 are calcar loading, type 3 are calcar loading with lateral flare, and type 4 have shortened tapered conventional stems. Other than this classification, Falez et al.24), classified the short femoral stems into collum, partial collum, trochanter sparing, and trochanter harming based on primary fixation principles, osteotomy level, and bone loss of femoral neck and greater trochanter.
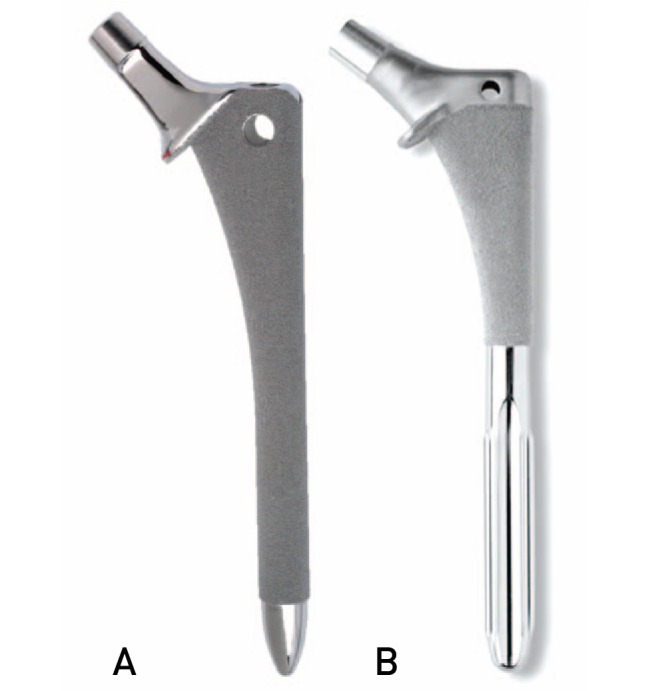
The femoral neck only or collum-type stems showed excellent clinical outcomes in several studies but they are not fully investigated24,25,26) (Fig. 13). Relatively longer types such as shortened tapered conventional stems or trochanter-sparing, trochanter-harming types show approximately 98% survival rates over more than 10-year follow ups, making these stem types as the most widely utilized femoral stem designs recently24,26,27) (Fig. 14). Nonetheless, further long-term follow ups are required since the most studies regarding short femoral stem types are relatively short.
Fig. 13. Short femoral stems. (A) Proxima stem (DePuy, USA). (B) Metha stem (Aesculap, Germany). (C) Clinical case. Due to existing femoral implants from knee revision, Proxima stems were utilized for hip arthroplasty.

Fig. 14. Types of mid-short stems. (A) Bencox M stem (Corentec, Korea). (B) Trilock stem (DePuy, USA). (C) M/L Taper stem (Zimmer, USA). (D) Taperloc Microplasty stem (Biomet, USA).

5. Recent Trends in Stem Designs
Recent trends in femoral stem designs for primary hip arthroplasty in patients without serious anatomical deformities are described as follows.
Recently, the most preferred stem design is proximally coated single wedge stems with wide yet thin proximal portions with no collars. The distal part of the design was shortened by approximately 4–5 cm, compared to conventional stems. The shoulder of the lateral part of a proximal stem is inclined to make a slope to encourage bone preservation which lowers the risk of fracture while stems are inserted. The neck is designed to minimize collision between liners and acetabular cups by making it slightly thinner. The femoral head is comparable for both metal and ceramic materials. Previously, a few attempts were made to achieve better elasticity of stems; 1) distal parts of stems were grooved, 2) thin plates or small bumps were extruded to reduce diameter of stem body, and 3) vertical flutes were made. Recently, for similar reasons, it was attempted to reduce elasticity by making long grooves on both the anterior and posterior sides of distal parts of stems, parallel to the vertical axis. Furthermore, the lateral part of stem tips was partially removed to reduce contacts with lateral cortical bone (Fig. 14). These attempts are all aiming to minimize thigh pain but clear scientific evidence has not been provided fully yet (Fig. 15).
Fig. 15. (A) The Bencox M stem (Corentec, Korea) representing recent stem characteristics. (B) Operative radiographs.

SPECIAL TYPES OF IMPLANT DESIGNS
Bimodular stems (or dual taper modular stems) are designed to assemble neck and body to control leg length, anteversion, and neck shaft angle thus provide benefits for recovery of biomechanical properties in patients with serious and complex deformities. Despite these benefits, application of bimodular stems has caused significantly higher revision rates possibly due to mechanical failures, dissociation of modular components, corrosion, and metal ion release. Most designs with complications have been discontinued and recalled by the manufactures and stems with the same bimodular property showed different clinical outcomes. The suggested causes of poor results of bimodular design such as properties of metals, the Galvanic corrosion due to different metals contacting the modular junction, pitting corrosion by micromotion, and crevice corrosion are believed to contribute to complications to different extents, hence further investigation is needed28,29) (Fig. 16).
Fig. 16. M/L Taper Kinectiv stem with modular neck (Zimmer, USA).

Recently developed dual mobility cup contained one joint plane made by highly cross-linked polyethylene liner with large diameter on metal or ceramic head and the second joint plane made with the liners and large metal surface acetabular cup. The design is similar to acetabular cup of resurfacing arthroplasty (Fig. 17). These two joint planes allow better range of joint movement whereas dislocation risks can be significantly reduced by virtue of large diameter of polyethylene liners. However, there is no long-term follow up study hence clinical effectiveness should be further validated.
Fig. 17. The Dual Mobility system (Biomet, USA) comprising two joint planes with ceramic bone head-highly cross-linked polyethylene liner-metal joint plane acetabular cup.

CONCLUSION
Today, the majority of cementless acetabular cups are hemispherical press-fit. Thus, acetabular cups without extruded liners with improved congruity are being widely introduced and have shown outstanding clinical outcomes. Various designs of cementless femoral stems were developed and utilized in multiple applications. These can be classified and subjected to direct comparisons based on their contact area and contact site between implants and cortical bones. Even though short femoral stems were introduced with several theoretical merits, enough follow-up results have not accumulated, and thus further studies are warranted. A clear understanding of fixation principles per different implant designs would be informative and helpful for selection of optimal implants for respective applications to patients.
Footnotes
CONFLICT OF INTEREST: The authors declare that there is no potential conflict of interest relevant to this article.
References
- 1.Khanuja HS, Vakil JJ, Goddard MS, Mont MA. Cementless femoral fixation in total hip arthroplasty. J Bone Joint Surg Am. 2011;93:500–509. doi: 10.2106/JBJS.J.00774. [DOI] [PubMed] [Google Scholar]
- 2.Yamada H, Yoshihara Y, Henmi O, et al. Cementless total hip replacement: past, present, and future. J Orthop Sci. 2009;14:228–241. doi: 10.1007/s00776-008-1317-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Friedman RJ, Black J, Galante JO, Jacobs JJ, Skinner HB. Current concepts in orthopaedic biomaterials and implant fixation. Instr Course Lect. 1994;43:233–255. [PubMed] [Google Scholar]
- 4.Ries MD. Review of the evolution of the cementless acetabular cup. Orthopedics. 2008;31 [PubMed] [Google Scholar]
- 5.Callaghan JJ, Rosenberg AG, Rubash HE. The adult hip. 2nd ed. New York: Lippincott Williams & Wilkins; 2007. pp. 980–1052. [Google Scholar]
- 6.Burt CF, Garvin KL, Otterberg ET, Jardon OM. A femoral component inserted without cement in total hip arthroplasty. A study of the Tri-Lock component with an average ten-year duration of follow-up. J Bone Joint Surg Am. 1998;80:952–960. doi: 10.2106/00004623-199807000-00003. [DOI] [PubMed] [Google Scholar]
- 7.McLaughlin JR, Lee KR. Total hip arthroplasty with an uncemented tapered femoral component. J Bone Joint Surg Am. 2008;90:1290–1296. doi: 10.2106/JBJS.G.00771. [DOI] [PubMed] [Google Scholar]
- 8.Epinette JA, Manley MT. Uncemented stems in hip replacement--hydroxyapatite or plain porous: does it matter? Based on a prospective study of HA Omnifit stems at 15years minimum followup. Hip Int. 2008;18:69–74. doi: 10.1177/112070000801800201. [DOI] [PubMed] [Google Scholar]
- 9.Lee GY, Srivastava A, D'Lima DD, Pulido PA, Colwell CW., Jr Hydroxyapatite-coated femoral stem survivorship at 10 years. J Arthroplasty. 2005;20(7 Suppl 3):57–62. doi: 10.1016/j.arth.2005.04.022. [DOI] [PubMed] [Google Scholar]
- 10.Park MS, Choi BW, Kim SJ, Park JH. Plasma spray-coated Ti femoral component for cementless total hip arthroplasty. J Arthroplasty. 2003;18:626–630. doi: 10.1016/s0883-5403(03)00203-1. [DOI] [PubMed] [Google Scholar]
- 11.Schuh A, Schraml A, Hohenberger G. Long-term results of the Wagner cone prosthesis. Int Orthop. 2009;33:53–58. doi: 10.1007/s00264-007-0460-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kolb A, Grübl A, Schneckener CD, et al. Cementless total hip arthroplasty with the rectangular titanium Zweymüller stem: a concise follow-up, at a minimum of twenty years, of previous reports. J Bone Joint Surg Am. 2012;94:1681–1684. doi: 10.2106/JBJS.K.01574. [DOI] [PubMed] [Google Scholar]
- 13.Reigstad O, Siewers P, Røkkum M, Espehaug B. Excellent long-term survival of an uncemented press-fit stem and screw cup in young patients: follow-up of 75 hips for 15-18 years. Acta Orthop. 2008;79:194–202. doi: 10.1080/17453670710014978. [DOI] [PubMed] [Google Scholar]
- 14.Suckel A, Geiger F, Kinzl L, Wulker N, Garbrecht M. Long-term results for the uncemented Zweymuller/Alloclassic hip endoprosthesis. A 15-year minimum follow-up of 320 hip operations. J Arthroplasty. 2009;24:846–853. doi: 10.1016/j.arth.2008.03.021. [DOI] [PubMed] [Google Scholar]
- 15.Zweymüller KA, Lintner FK, Semlitsch MF. Biologic fixation of a press-fit titanium hip joint endoprosthesis. Clin Orthop Relat Res. 1988;(235):195–206. [PubMed] [Google Scholar]
- 16.Belmont PJ, Jr, Powers CC, Beykirch SE, Hopper RH, Jr, Engh CA, Jr, Engh CA. Results of the anatomic medullary locking total hip arthroplasty at a minimum of twenty years. A concise follow-up of previous reports. J Bone Joint Surg Am. 2008;90:1524–1530. doi: 10.2106/JBJS.G.01142. [DOI] [PubMed] [Google Scholar]
- 17.Hennessy DW, Callaghan JJ, Liu SS. Second-generation extensively porous-coated THA stems at minimum 10-year followup. Clin Orthop Relat Res. 2009;467:2290–2296. doi: 10.1007/s11999-009-0831-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Biant LC, Bruce WJ, Assini JB, Walker PM, Walsh WR. The anatomically difficult primary total hip replacement: medium- to long-term results using a cementless odular stem. J Bone Joint Surg Br. 2008;90:430–435. doi: 10.1302/0301-620X.90B4.19718. [DOI] [PubMed] [Google Scholar]
- 19.Cameron HU, Keppler L, McTighe T. The role of modularity in primary total hip arthroplasty. J Arthroplasty. 2006;21(4 Suppl 1):89–92. doi: 10.1016/j.arth.2006.02.085. [DOI] [PubMed] [Google Scholar]
- 20.Heekin RD, Callaghan JJ, Hopkinson WJ, Savory CG, Xenos JS. The porous-coated anatomic total hip prosthesis, inserted without cement. Results after five to seven years in a prospective study. J Bone Joint Surg Am. 1993;75:77–91. doi: 10.2106/00004623-199301000-00011. [DOI] [PubMed] [Google Scholar]
- 21.Kim YH. The results of a proximally-coated cementless femoral component in total hip replacement: a five- to 12-year follow-up. J Bone Joint Surg Br. 2008;90:299–305. doi: 10.1302/0301-620X.90B3.20096. [DOI] [PubMed] [Google Scholar]
- 22.Kim YH, Kim JS, Cho SH. Primary total hip arthroplasty with a cementless porous-coated anatomic total hip prosthesis: 10- to 12-year results of prospective and consecutive series. J Arthroplasty. 1999;14:538–548. doi: 10.1016/s0883-5403(99)90074-8. [DOI] [PubMed] [Google Scholar]
- 23.Feyen H, Shimmin AJ. Is the length of the femoral component important in primary total hip replacement? Bone Joint J. 2014;96-B:442–448. doi: 10.1302/0301-620X.96B4.33036. [DOI] [PubMed] [Google Scholar]
- 24.Falez F, Casella F, Papalia M. Current concepts, classification, and results in short stem hip arthroplasty. Orthopedics. 2015;38(3 Suppl):S6–S13. doi: 10.3928/01477447-20150215-50. [DOI] [PubMed] [Google Scholar]
- 25.Kim YH, Park JW, Kim JS, Kang JS. Long-term results and bone remodeling after THA with a short, metaphyseal-fitting anatomic cementless stem. Clin Orthop Relat Res. 2014;472:943–950. doi: 10.1007/s11999-013-3354-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Khanuja HS, Banerjee S, Jain D, Pivec R, Mont MA. Short bone-conserving stems in cementless hip arthroplasty. J Bone Joint Surg Am. 2014;96:1742–1752. doi: 10.2106/JBJS.M.00780. [DOI] [PubMed] [Google Scholar]
- 27.Morrey BF, Adams RA, Kessler M. A conservative femoral replacement for total hip arthroplasty. A prospective study. J Bone Joint Surg Br. 2000;82:952–958. doi: 10.1302/0301-620x.82b7.10420. [DOI] [PubMed] [Google Scholar]
- 28.Krishnan H, Krishnan SP, Blunn G, Skinner JA, Hart AJ. Modular neck femoral stems. Bone Joint J. 2013;95-B:1011–1021. doi: 10.1302/0301-620X.95B8.31525. [DOI] [PubMed] [Google Scholar]
- 29.Fitch DA, Ancarani C, Bordini B. Long-term survivorship and complication rate comparison of a cementless modular stem and cementless fixed neck stems for primary total hip replacement. Int Orthop. 2015;39:1827–1832. doi: 10.1007/s00264-015-2894-4. [DOI] [PubMed] [Google Scholar]