

Abstract
A number of cross-sectional and a few longitudinal studies have shown a developmental relationship between child abuse and adult physical and mental health. Published findings also suggest that social support can lessen the risk of adverse outcomes for some abused children. However, few studies have investigated whether social support mediates or moderates the relationship between child abuse and adult physical and mental health. Structural equation modeling was used to examine data on these topics from a longitudinal study of more than 30 years. While a latent construct of physical and emotional child abuse did not predict adult health outcomes directly, child abuse did predict outcomes indirectly through social support. A test of variable moderation for child abuse and social support was nonsignificant. Results suggest that social support may help explain the association between child abuse and health outcomes at midlife. Implications of the findings for prevention and treatment are discussed.
Keywords: child maltreatment, mental health, physical health, social support, relationships, protective factors
Introduction
Positive developmental experiences in childhood set the foundation for lifelong health and well-being (Braveman, Egerter, Arena, & Aslam, 2014). However, many children encounter adversities that undermine their development and increase their risk for later physical and mental health problems (Finkelhor, Turner, Shattuck, & Hamby, 2013; U.S. Department of Health and Human Services, 2010). Early life adversity includes child maltreatment, which affects nearly 14% of children in the U.S. under the age of 18, according to a national study of households (Finkelhor et al., 2013).
Adults who were abused as children are at higher risk than those not abused for mental health disorders, which includes depression and anxiety (Kendall-Tackett, 2002). They also appear at risk for disabling and sometimes life-threatening physical health conditions, such as heart and lung disease and certain forms of cancer (Anda et al., 1999; Bolger & Patterson, 2001; Dube, Williamson, Thompson, Felitti, & Anda, 2004; Felitti et al., 1998; T. I. Herrenkohl, 2011a; T. I. Herrenkohl, Hong, Klika, Herrenkohl, & Russo, 2013; Leeb, Lewis, & Zolotor, 2011; Repetti, Taylor, & Seeman, 2002; Sachs-Ericsson, Blazer, Plant, & Arnow, 2005). Rates of smoking and drug use, behaviors that contribute to poor health, are also more common among adults who were abused (Anda et al., 1999; T. I. Herrenkohl, 2011a; Kristman-Valente & Wells, 2013). Results of the Adverse Childhood Experiences (ACE) study, a large, retrospective investigation of more than 9,500 middle-aged adults, found that individuals who had been abused and exposed to other forms of adversity before age 18 were at significantly higher risk than were others for self-reported alcoholism, depression, and poor physical health (Felitti et al., 1998). The odds of past-year depression and alcoholism for adults with four or more adversities in childhood, compared to those with no adversities, were 4.6 and 7.4 times greater. The odds of stroke, cancer, and ischemic heart disease were also elevated at about twice the level of those with no reported adversities. Further, Dube et al. (2004) found a link between ACE scores and lifetime risk of multiple sexual partners, sexually transmitted diseases, and suicide attempts.
The ACE study is unique because of its size and comprehensive assessment of adult health, but it is limited by a retrospective design in which adult respondents were asked to recall adversities (e.g., abuse) that occurred many years earlier (Hardt & Rutter, 2004). As noted by Hardt and Rutter (2004), the accuracy of retrospective reports of childhood events can be influenced by any number of factors, including how old an individual was when an adversity was encountered and what has transpired in the individual’s life since the encounter. Later occurring life transitions and other (possibly negative) events, for example, may change how an individual remembers his or her childhood and what remains salient in the memories and recollections that individual has and can share. Prospective longitudinal designs, in which child abuse is assessed proximally to when it occurred, are thought to avoid some of the measurement problems of retrospective studies (Widom & Shepard, 1996). However, there are relatively few prospective studies on child abuse consequences, and even fewer on child abuse and adult health at mid-life (Greenfield, 2010).
In one recently published longitudinal study, Herrenkohl and colleagues (2013) found that a measure of officially recorded child abuse and neglect was associated with adult reports of bodily pain and poorer overall health, as well as symptoms of depression and anxiety. In another study, Batten and colleagues (2004) found that child maltreatment increased the risk of cardiovascular disease in women, and of depression in both women and men. Springer and colleagues (2007) examined the relation between self-reported childhood physical abuse and ill health in a sample of middle-aged men and women. They found that, after controlling for age, sex, and other childhood adversities, physical abuse predicted various medical diagnoses and symptoms, including respiratory problems, fatigue, and pain.
Emerging research on developmental pathways that link child abuse to later health is important for prevention and intervention programs (Greenfield, 2010). One area of research has focused on the damage caused by stress to the internal systems of the body (Shonkoff, Boyce, & McEwen, 2009). In a recent review of the literature, Fagundes and Way (2014) explained that early stress promotes disease by causing systemic inflammation and a weakened immune response. Other scholars have also emphasized the “biological embedding” of adversities in theories of adult health impairments (Shonkoff et al., 2009).
Research on social determinants has focused somewhat less on biology and more on health-risk behaviors as precursors to adult disorders and disease (Leeb et al., 2011). From this perspective, abuse triggers poor coping behaviors in the form of drug and alcohol use, smoking, and risky sexual practices (Widom, Mormonstein, & White, 2006) and these behaviors, in turn, lead to poor health (Springer, 2009). The misuse of drugs and alcohol can increase the risk of accidents from overdose and impaired functioning, which can have even more immediate impacts on physical health than would naturally occur if these harmful behaviors are sustained over many years (Leeb et al., 2011).
In their review of research, Leeb and colleagues (2011) determined that abused children not only appear more susceptible to drug and alcohol abuse and the consequences that follow, they also experience poorer relationships and less social support, which can promote health problems and worsen conditions among those who are ill (Kendall-Tackett, 2002). In this regard, low levels of support increase an individual’s vulnerability to illness by removing protective buffers related to positive coping (Kendall-Tackett, 2002; Murthi & Espelage, 2005). Relationships formed with others can bolster an individual’s determination to overcome an illness and also give rise to better and more informed decision making about health care services (Merrick, Leeb, & Lee, 2013; Zhao, Lynch, & Chen, 2010). As noted in other sources, social support is predominantly a reflection of how well and deeply connected an individual is to family and friends (Murthi & Espelage, 2005), and possibly child welfare and mental health professionals who remain involved with families over an extended periods. For young people, teachers and other adults in schools can also be important sources of social support, particularly when parents are unavailable or conflict weakens bonds between parents and children or among siblings (T. I. Herrenkohl, 2011b).
In one study, Murthi and Espelage (2005) found that social support from family and friends moderated the association between childhood sexual abuse and perceptions of loss extending from abuse, such that those with more support experienced less loss. The significance of this finding is that perceived higher levels of support was associated with less helplessness and fewer feelings of despair—emotions related to depression that can lead in time to poor coping, and eventually to health declines (Kendall-Tackett, 2002). In another study relevant to the topic, Berkman and colleagues (1992) showed that older adults with less social support were at significantly higher risk of dying within a 6-month period following hospitalization for cardiovascular disease than were those with more sources of support. Brummett et al. (2001) found a similar pattern in socially isolated adults with coronary artery disease. Further, in a study of patients selected from cancer registries, Ell and colleagues (1992) found that perceptions of stronger emotional support lessened mortality risk among individuals with certain forms of cancer (e.g., breast cancer). Interestingly, social support appeared less protective for individuals with more aggressive and advanced cancers, suggesting that there may be a limit to how influential social support is at the point one’s health problems have progressed beyond a certain point.
As a theoretical construct, social support describes a configuration of social and relational patterns that are hypothesized to stabilize, lessen stress, and promote positive coping (Batten et al., 2004; Widom, Raphael, & DuMont, 2004). In statistical models, social support variables can be main effect predictors (Ell et al., 1992) or moderators or mediators of risk (Klika & Herrenkohl, 2013). A moderator is a variable that changes the association between a risk factor (e.g., abuse) and an outcome (adult health), whereas a mediator accounts in part or full for the association between a risk factor and an outcome (Masten, 2001).
Notably, in studies of adult health, analyses of social support are mostly descriptive; that is, they typically describe the amount and quality of social support adults receive in relation to their health status but they do not test for moderation, mediation, or predictive relationships (Greenfield, 2010). An exception is a study by Ell and colleagues (1992), which examined social support variables in multivariate models. Springer (2009) also examined several indicators of social support in a structural test of four pathways linking child abuse to adult health. However, data in the study by Ell and colleagues (1992) were drawn from a clinical population in which the outcome (survival versus death from cancer) is more common than in community samples. The study by Springer and colleagues (2007) used retrospective reports of child abuse and examined a relatively narrow constellation of social support indicators.
An important contributor to social support is environmental stability. Caregiver and residence changes, and disruptions in schooling, all common among abused children, can lessen opportunities to form relationships and bond to significant others (E. C. Herrenkohl, Herrenkohl, & Egolf, 2003). In this regard, more transitions are assumed to weaken social support and increase risk for poor functioning, whereas fewer transitions are expected to lessen risk and improve functioning (Klika & Herrenkohl, 2013; Sedlak, 2010). As one example, a study of abused children found that the frequency of residential moves and caregiver changes predicted a significantly higher risk of drug and alcohol use in adolescence (E. C. Herrenkohl et al., 2003).
Essential for Childhood Framework
Attending to the complex interplay between the social environment and individual vulnerabilities caused by child abuse and other adversities, the Centers for Disease Control and Prevention (CDC) developed a research-to-practice framework called Essentials for Childhood. This framework emphasizes the role of social support in the form of safe, stable, and nurturing relationships and environments (SSNRs; CDC, 2014). Although the framework is based on promising research, more studies are needed to establish how social support in the form of SSNRs buffers and helps explain adult health. The objective of the current investigation is therefore to explore whether SSNRs, characterized by warm and nurturing relationships, emotional and instrumental supports, and environmental stability (e.g., fewer caregiver, residence, and school changes), moderate or mediate the effect of physical, emotional, and sexual child abuse on adult physical and mental health.
Methods
Sample
Data are from the Lehigh Longitudinal Study (R. C. Herrenkohl, Herrenkohl, Egolf, & Wu, 1991; T. I. Herrenkohl et al., 2013; T. I. Herrenkohl, Klika, Herrenkohl, Russo, & Dee, 2012), a prospective study of the causes and consequences of child maltreatment, which began in the 1976 – 1977 with a sample of 457 children and their families. Some of the families were selected into the study from child welfare agencies for abuse and neglect caseloads; others were selected from several group settings (Head Start centers and daycare and nursery programs) in the same two-county, mostly suburban area within which those in the child welfare group were living at the time. The first “preschool” wave of the study took place in 1976 – 1977 when children recruited into the study were 18 months to 6 years of age (average: 4 years). A second “school-age” assessment was conducted in 1980 – 1982 when child participants were 8 – 11 years of age (average age: 8 years). A third “adolescent” assessment of all youth participants (91% of the original sample) was conducted in 1990 – 1992. When they were assessed in adolescence, participants were 18 years of age on average. Survey data were most recently collected in 2008 – 2010 from about 80% of the original child (now adult) sample (N = 357). At the last assessment, participants ranged in age from 31 to 41 years (age 36 years on average).
The original child sample was gender balanced: 248 (54%) males and 209 females. The racial and ethnic composition of the original sample was relatively homogeneous but consistent overall with the makeup of the two-county area from which participants were selected. The majority (80.7%) of the participants are White (n = 369); 5.3% (n = 24) Black or African American; 1.3% (n = 6) American Indian and Alaska Native; 0.2% (n = 1) Native Hawaiian or Other Pacific Islander; and 11.2% (n = 51) are of more than one race. Just over 7% (n = 33) are Hispanic or Latino. For a small percentage of the sample (1.3%, n = 6), a participant’s ethnicity remains unknown. Eighty-six percent of the children, now adults in the study, were from two-parent households. The income level of 63% of families in the mid-1970s was below $700 per month and about 60% of the sample would be considered poor according to the income-to-needs ratio and poverty threshold set by the United States Census Bureau in 1976 (http://www.census.gov/hhes/www/poverty/data/threshld/thresh76.html).
The retained adult sample remains gender balanced: 186 (52.1%) males. An analysis of the currently retained and full sample found that, although more of the original child welfare abuse group was lost to attrition (68% retained compared to 79% in the child welfare neglect group and over 80% in the Head Start, daycare, and nursery groups), there were no significant group differences in gender, age, childhood SES, or parent-reported harmful physical or emotional discipline. Due to missing data across variables of the four waves of the study, analyses of the current investigation have an N of 334. In the adult assessment, participants were, on average, 36 years of age (range = 31 – 41). Study procedures were approved by the Human Subjects Division at the University of Washington and the Office of Research and Sponsored Programs at Lehigh University.
Measures
Child abuse
Data on physical and emotional child abuse are from parents’ (mostly mothers’) reports of their own and others’ (fathers and other caregivers) disciplining practices used with children prior to the preschool and school-age waves of the study. In the preschool wave of the study, mothers responded to questions about their own, fathers’, and others’ physical disciplining of children for two time periods: (a) in the last three months and (b) prior to the last three months. Questions asked of mothers about their, fathers’, and others’ emotionally abusive practices in the preschool wave of the study focused only on the 3 months prior to that assessment. Similar questions about physical and emotional disciplining practices were again asked of mothers in the school-age wave of the study for disciplining in the past year.
The assessment of parents’ disciplining at each of the two waves of the study covered a range of practices, some of which were abusive (e.g., shaking a child, slapping a child’s face, hitting a child with a stick or paddle, taking meals away from a child, threatening to leave a child, threatening to send a child away). To differentiate abusive from non-abusive discplining, each practice was assigned a rating of 0 to 5 to reflect its level of severity. Practices with a severity rating of 5 were considered abusive; those with a 4 were considered severely punishing; those with a 3, mildly punishing; those with a 2, mildly rewarding; and those with a 1, highly rewarding. For the current analysis, practices with a rating of 4 or 5 (severely punishing or abusive) were retained and then combined for each participant. Combined scores for physical and emotional abuse are an additive count of the number of abusive or severely punishing disciplining practices a child experienced within a designated (e.g., past year) time period at the hands of all caregivers reported on by the parent respondent at the time of each assessment.
Variable summaries and descriptive statistics for the physical and emotional child abuse variables are provided in Table 1. Scores of 0 on these measures indicate a child was not abused. Scores in the 4- to 5-point range indicate a child was exposed to 1 abusive practice across caregivers; scores in the 8- to 10-point range indicate a child was exposed to two abusive practices; and scores in the 12- to 15-point range indicate a child was exposed to three abusive practices. Scores above 16 indicate a child was exposed to four or more abusive practices across caregivers.
Table 1.
Child Abuse Variables Descriptive Statistics
| Latent variable indicators | Variable description | Score range | Mean (SD) |
|---|---|---|---|
| Preschool physical abuse (last 3 months) | Parent-reported physical abuse for up to three caregivers (mother, father, other). Examples include shaking a child, slapping a child’s face, hitting a child with a stick or paddle. Reports are for the 3 months prior to the preschool assessment. | 0–42.87 | 7.35 (8.33) |
| Preschool physical abuse (prior to the last 3 months) | Parent-reported physical abuse for up to three caregivers (mother, father, other). Reports are for prior to the 3 months before the preschool assessment. | 0–86.48 | 19.14 (18.12) |
| School-age physical abuse (past year) | Parent-reported physical abuse for up to three caregivers (mother, father, other). Reports are for the year prior to the school-age assessment. | 0–57.48 | 10.76 (10.70) |
| Preschool emotional abuse (last 3 months) | Parent-reported emotional abuse for up to three caregivers (mother, father, other). Examples include taking meals away from a child, threatening to leave a child, threatening to send a child away. Reports for the 3 months prior to the preschool assessment. | 0–31.95 | 4.43 (6.66) |
| School-age emotional abuse (past year) | Parent-reported emotional abuse for up to three caregivers (mother, father, other). Reports are for the year prior to the school-age assessment. | 0–37.03 | 7.67 (8.97) |
Sexual abuse was measured separately using youth and adult reports from the two waves of the study. Incidents counted as child sexual abuse occurred before the age of 18 years. In adolescence, a single question was used to ask youth participants whether they had been sexually abused: Were you sexually abused? to which they responded yes or no. Two additional questions that focused on sexual assault and rape were asked of participants. Reports of sexual abuse in the adolescent wave of the study were also recorded in interviewers’ notes and in child welfare case records from the preschool assessment. A total of 103 participants reported or were found to have been sexually abused using these combined sources. To these 103 cases, affirmative responses to questions in the adult survey about childhood sexual abuse were added, bringing the total to 161 cases (38.5% of the full sample and 41% of those for whom data on sexual abuse were available). In the analyses that follow, sexual abuse is modeled apart from physical and emotional abuse because it was found to be weakly correlated with these other variables and because the nature of sexual abuse is itself qualitatively different from other forms of abuse (Greenfield, 2010; Leeb et al., 2011).
Safe, stable, and nurturing relationships (SSNRs)
SSNR social support indicators were modeled as latent variable indicators of a second-order latent construct. These indicator constructs are each composed of several measured (scaled) variables that reflect the care and support of family members and friends (variables 1 and 3); the quality of relationships (variable 2); and the stability of an individual’s living environment during childhood, called “transitions and changes” (variable 4). Information on the scales and descriptive statistics for all SSNR variables in the analysis are provided in Table 2.
Table 2.
SSNR Latent Variable Summaries and Descriptive Statistics
| First-order SSNR latent variables | Measured variable indicators (α for scales) | Variable description | Score range | Mean (SD) |
|---|---|---|---|---|
| 1. Care and support from family | Warmth and care from mother (6 items, α=.924, n=337) | Mother spoke in a warm friendly voice; seemed emotionally cold (reversed); was affectionate; enjoyed talking things over; could make someone feel better when upset; seemed to understand problems/worries. | 1 – 4 | 3.31 (0.73) |
| Warmth and care from father (6 items, α=.921, n=282) | Father spoke in a warm friendly voice; seemed emotionally cold (reversed); was affectionate; enjoyed talking things over; could make someone feel better when upset; seemed to understand problems/worries. | 1 – 4 | 3.07 (0.81) | |
| Warmth and care from sibling (6 items, α=.898, N=329) | Sibling spoke in a warm friendly voice; seemed emotionally cold (reversed); was affectionate; enjoyed talking things over; could make someone feel better when upset; seemed to understand problems/worries. | 1 – 4 | 3.33 (0.78) | |
| Family care (4 items, α=.894, n=357) | Family cares; can rely on them for help; can open up to them if you need to talk about worries. | 1 – 4 | 3.33 (0.73) | |
| 2. Relationship quality and support | Close relationships | Maintaining close relationships has been difficult, frustrating (single item, reversed scored). | 1 – 6 | 3.84 (1.82) |
| Warm relationships | I have not experienced many warm/trusting relationships (single item, reversed scored). | 1 – 6 | 3.92 (1.97) | |
| Supportive friends (4 items, α=.874, n=338) | Friends care, understand the way you feel; can rely on them for help with a serious problem; can open up to them to talk about worries. | 1 – 4 | 3.32 (0.76) | |
| 3. Give and receive support | Provide emotional support | Provide informal/emotional support to spouse or partner, parents, in-laws, (grand)children, other family member or close friends (count of relationships). | 1 – 6 | 3.74 (1.33) |
| Receive emotional support | Receive informal/emotional support from spouse or partner, parents, in-laws, (grand)children, other family member or close friends (count of relationships). | 0 – 6 | 3.35 (1.38) | |
| Provide instrumental support | Provide unpaid assistance to spouse or partner, parents, in-laws, (grand)children, other family member or close friends (count of relationships). | 0 – 6 | 2.96 (1.46) | |
| Receive instrumental support | Receive unpaid assistance from spouse or partner, parents, in-laws, (grand)children, other family member or close friends (count of relationships). | 0 – 6 | 2.37 (1.47) | |
| 4. Transitions and changes | Caretaker changes/stability | Transitions involving family and friends, foster placements, and institutional placements to age 18 (count of occurrences; lower scores reflect fewer changes/more stability). | 1 – 22 | 4.67 (4.01) |
| Residence changes/stability | Total number of residence moves a child experienced up to age 18 (count of occurrences; lower scores reflect fewer changes/more stability). | 1 – 73 | 6.57 (6.22) | |
| School changes/stability | Total number of schools a child attended up to age 18 (count of occurrences; lower scores reflect fewer changes/more stability). | 2 – 20 | 5.45 (2.11) |
Adult physical health and mental health
Physical and mental health data were drawn from the adult survey at age 36 years, which included items from the Short-Form Health Survey (SF-36), a general measure of health and well-being (Ware, Kosinski, & Dewey, 2000; Ware & Sherbourne, 1992).
General health (α = .79) is based on responses to questions about an individual’s proneness to illness, their perception of being healthy, and health expectancies. Examples include: I get sick easier than others; I am as healthy as anybody I know; My health is excellent; and I expect my health to get worse. These were scored on a 5-point scale from mostly true (1) to mostly false (5) (positive items were reversed scored). This variable had a range of 0 to 100 with a mean of 72.23 and standard deviation of 21.55.
Mental health (α = .84) is based on responses to a series of questions about the impacts of emotional problems (such as feeling depressed or anxious) on work and other daily activities. Examples include: Been a very nervous person; Felt so down that nothing could cheer me up; and Felt downhearted and blue. These were scored on a scale from none of the time (6) to all of the time (1). This variable has a range of 8 to 100 with a mean of 75.60 and standard deviation of 19.50. Scale scores for both the physical health and mental health scales are continuous, with higher values reflecting better physical and mental functioning.
Somatic complaints were assessed using the Somatic Symptom Severity Scale of the Patient Health Questionnaire (PHQ-15; Kroenke, Spitzer, & Williams, 2002). Scores reflect how much an individual was bothered over the preceding 4 weeks by problems such as stomach and back pain; pain in arms, legs, or joints; headaches; chest pain; dizziness; feeling tired or having low energy; and trouble sleeping (0 = not bothered at all; 1 = bothered a little; 2 = bothered a lot). The scale alpha for the full adult sample is .85. This variable has a range of 0 to 14 with a mean of 5.12 and standard deviation of 3.45.
Analyses also included a measure of adult health history, which is based on a count of the number of health problems and illnesses (0 = no illness, 1 = illness) reported by participants in the adult wave of the study. These include, but are not limited to, alcohol problems, high blood pressure, ulcers, as well as heart disease, stroke, and cancer. This variable has a range of 0 to 13 with a mean of 3.97 and standard deviation of 2.71.
Covariates
Covariates in the analysis include gender (females = 0, males = 1), childhood socioeconomic status (SES), and child welfare involvement (0 = no child welfare involvement, 1 = child welfare involvement). Child welfare involvement was included to account for the group composition of the sample and to add a measure of officially recorded child maltreatment (see T. I. Herrenkohl et al., 2012; 2013). SES is a standardized index of parents’ occupational status, income, and number of rooms in the house. SES scores for the analysis sample ranged from − 5.43 to 9.18 with a mean of 0.23 and standard deviation of 3.37. Higher scores on the measure correspond to higher SES. The measure of SES used in the analysis is identical to that used in earlier reports on the study sample (T. I. Herrenkohl et al., 2013) and contains families at low, moderate, and higher levels of SES.
Conceptual model
In this study, we explored two primary research questions: (1) Are self-reports of adult physical and mental health problems related to earlier child physical, emotional, and sexual abuse? (2) Is there evidence of social support moderation or mediation in the prediction from child abuse to adult physical and mental health? Constructs and pathways of a conceptual model based on these questions are shown in Figure 1. Directional patterns among the variables are indicated by (−) and (+) in the figure to be consistent with the scoring of each variable. Paths from the SSNR construct to the adult outcomes are also labeled using (−) and (+) to show the hypothesized direction of the paths consistent with variable scoring. Paths from sexual abuse, gender, childhood SES, and child welfare involvement to the adult outcomes also were tested but are not shown in the conceptual model in order to reduce complexity. In addition to tests of the paths illustrated in the figure for mediation, we also conducted tests of variable moderation for child abuse and SSNRs in relation to adult health outcomes. However, results of that test were nonsignificant and this issue of moderation was therefore not examined further (results available on request).
Figure 1.
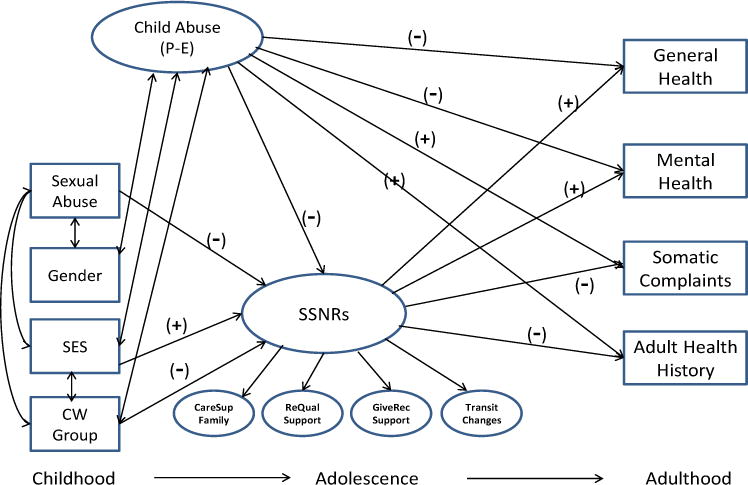
Conceptual model of the relations among measures and latent variables of the tested model.
Note: Directions of the primary paths of the hypothesized model are shown by (−) and (+). Direct paths from sexual abuse and other covariates to the adult outcomes (although tested) are not shown to reduce complexity in the model. P-E = Physical-Emotional; CW = Child Welfare; SSNRs = Safe, Stable, and Nurturing Relationships; CareSup Family = Care and Support from Family; RelQual Support = Relationship Quality and Support; GiveRec Support = Give and Receive Support; Transit Changes = Transitions and Changes.
Structural equation modeling (SEM) analysis was used to investigate the paths of Figure 1. In the analyses, measures of physical and emotional abuse were modeled as indicators of a latent construct. Child sexual abuse was analyzed separately in the model, positioned alongside covariates of childhood socioeconomic status (SES) and gender (male = 1, female = 0). A second-order latent construct of SSNR social support influences was included as a potential mediator of the child abuse latent factor. The SSNR construct consists of four first-order latent variables described in the Measures section and in Table 1, emphasizing the care and support of others, quality of relationships, and transitions up to age 18. Adult outcomes consist of the four outcome measures of adult general health, mental health, somatic complaints, and adult health history. Also estimated, but not shown in Figure 1, are the correlations among the residuals of the outcome variables: general health, mental health, somatic complaints, and adult health history. These correlations were estimated because the physical and mental health outcomes included in the model are known to co-occur but not necessarily conform to a single construct (T. I. Herrenkohl et al., 2013; Leeb et al., 2011).
All analyses were conducted using maximum likelihood estimation in Mplus 7.11 (Muthén & Muthén, 2013). Model fit was based on multiple considerations, including an examination of the Model Chi-Square, the Comparative Fit Index (CFI), the Tucker-Lewis Index (TLI), the Root Mean Square Error of Approximation (RMSEA), and the Standardized Root Mean Square Residual (SRMR). Recommendations for acceptable model fit are for the CFI and TLI to be around .95 or higher, whereas the RMSEA and SRMR should be around .06 or less (Browne & Cudeck, 1993; Hu & Bentler, 1998; MacCallum, Browne, & Sugawara, 1996). There are, however, circumstances in which certain fit statistics fall below their optimal values, while others indicate acceptable model fit (http://davidakenny.net/cm/fit.htm). When this occurs, it is important to evaluate model fit in light of additional considerations, including how the model corresponds to a proposed theory, the statistical significance of the factor loadings, and the pattern of associations among the variables in the analysis (Barrett, 2007; Goffin, 2007). All were considered when evaluating the fit of the model. For the mediation tests involving the child abuse and SSNR variables, bias-corrected bootstrapped 95% confidence intervals were computed to determine the statistical significance of the indirect effects (MacKinnon, Lockwood, & Williams, 2004).
Results
A confirmatory factor analysis (CFA) provided information on the measurement model for each of the two latent constructs as well as the correlations among the measured and latent variables. Fit statistics for the CFA model are as follows: χ2 (283) = 529.213, p < .01; Comparative Fit Index (CFI) = 0.88; Tucker Lewis Index (TLI) = 0.86; Root Mean Square Error of Approximation (RMSEA) = 0.05; and Standardized Root Mean Square Residual (SRMR) = 0.06.
Factor loadings from the CFA for indicators of the estimated latent variables were all statistically significant (p < .05), with standardized coefficients ranging from 0.52 to 0.66 for child physical and emotional abuse and from around 0.40 to 0.85 for the first-order SSNR latent variables. Factor loadings for the second-order SSNR latent construct range from 0.39 to 0.77.
As shown in the correlations of the CFA in Table 3, many variables are correlated and in the expected directions. For example, the child abuse latent construct (physical and emotional abuse) was moderately, inversely correlated with the SSNR construct (r = −0.36, p < .001). Somewhat surprisingly, however, the physical and emotional child abuse latent construct was correlated only with one adult outcome: mental health (r = −0.15, p < .05). Also of interest, sexual abuse was moderately, positively correlated with physical and emotional child abuse at 0.22 (p < .001), and inversely correlated with the SSNR latent construct at −0.48, p < .001. Sexual abuse was also inversely correlated with adult general physical health (r = −0.18, p < .001) and mental health (r = −0.19, p < .001) and positively correlated with somatic symptoms (r = 0.27, p < .001) and adult health history (r = 0.25, p < .001). Additionally, the SSNR construct was significantly (p < .05) correlated with all the adult physical and mental health outcomes. Consistent with the coding of the variables, correlations of the SSNR construct with the general health and mental health variables was positive, indicating that better physical and mental health scores are associated with higher scores on the SSNR indicator variables.
Table 3.
Correlations Among the Variables From the CFA
| Variables | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. |
|---|---|---|---|---|---|---|---|---|---|
| 1. Child abuse (physical and emotional) | .07 | .18** | −.25*** | .12+ | −.36*** | −.05 | −.15* | .10 | .08 |
| 2. Sexual abuse | −.27*** | −.22*** | .22*** | −.48*** | −.18** | −.19*** | .18*** | .25*** | |
| 3. Gender (male) | −.002 | .04 | −.02 | .07 | .07 | −.24*** | −.08 | ||
| 4. SES | −.58*** | .50*** | .23*** | .15** | −.18*** | −.35*** | |||
| 5. Child welfare | −.44*** | −.24*** | −.19*** | .18** | .27*** | ||||
| 6. SSNRs | .49*** | .60*** | −.46*** | −.40*** | |||||
| 7. General health | .47*** | −.57*** | −.46*** | ||||||
| 8. Mental health | −.54*** | −.36*** | |||||||
| 9. Somatic symptoms | .49*** | ||||||||
| 10. Adult health history |
Correlations among other variables in the analysis are also instructive. For example, male gender and sexual abuse were inversely correlated (r = −0.27, p < .001). Childhood socioeconomic status (SES) was inversely correlated with child physical and emotional abuse (r = −0.25, p < .05), sexual abuse (r = −0.22, p < .05), and child welfare involvement (r = −0.58, p < .001).
Results of the structural model test for mediation are provided in Figure 2, which shows only the statistically significant (p < .05) paths among all the paths that were tested. Nonsignificant paths were removed from the diagram to reduce complexity and to show more clearly where effects were observed. Fit statistics for the model shown in Figure 2 are similar to those of the CFA: χ2 (285) = 530.732, p < .01; CFI = 0.87; TLI = 0.85; RMSEA = 0.05; SRMR = 0.06. The child abuse latent construct predicted adult physical and mental health outcomes only indirectly through SSNRs. Except for adult health history (Beta = −.07, p < .101), the total indirect effect of child abuse in relation to adult functioning was statistically significant, operating through SSNRs: general health (Beta = −.14 [−1.19/−0.18], p < .032); mental health (Beta = −.18 [−1.40/−0.25], p < .025); and somatic complaints (Beta = .12 [0.26/1.73], p < .040). Significant indirect effects of the SSNR construct and these same three outcomes were also observed for sexual abuse.
Figure 2.
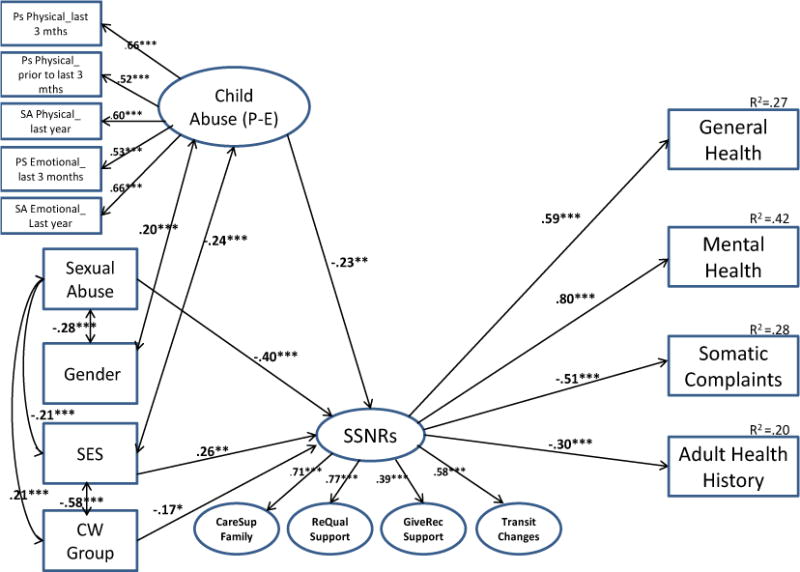
Analysis model results: child abuse, SSNRs, and adult health and mental health.
Note: *p < .05; **p < .01; ***p < .001. Health and mental health outcomes are correlated in the model at .20 – .44***; nonsignificant paths are not shown; paths from gender to somatic complaints (.26***), from SES to adult mental health history (−.20*); and from SES to adult mental health history (−.19**) are significant (p < .05), but not shown to reduce complexity in the model. P-E = Physical-Emotional; CW = Child Welfare; SSNRs = Safe, Stable, and Nurturing Relationships; CareSup Family = Care and Support from Family; RelQual Support = Relationship Quality and Support; GiveRec Support = Give and Receive Support; Transit Changes = Transitions and Changes.
The second-order latent SSNR construct was in all cases significantly related to the adult health and mental health outcomes in the expected direction: general health (Beta = 0.59, p < .001); mental health (Beta = 0.80, p < .001); somatic symptoms (Beta = −0.51, p < .001); and adult health history (Beta = −0.30, p < .001). R-squared values for the outcome variables range from 0.20 for adult health history to 0.42 for mental health, indicating that a sizeable proportion of the variance in each measured variable is explained by predictors in the model.
Discussion
The goal of this study was to investigate the relation between child abuse, social support (SSNRs), and adult physical and mental health. While analyses produced no evidence of social support moderation, findings do support a pattern of mediation consistent with the proposed model. However, correlations between child abuse and adult health were considerably weaker than those that appear in previously published reports on adverse childhood experiences (Anda et al., 1999; Felitti et al., 1998) and sexual and physical abuse (Greenfield, 2010). According to one review of the research literature, studies generally show that sexual, physical, and emotional abuse are predictors of adult health, particularly when the abuse is chronic and severe (Greenfield, 2010). However, the review also points out that most research on these topics is based on retrospective reports from adult child abuse survivors, which can be biased by poor and inaccurate recall of events in years past (Hardt & Rutter, 2004).
Whether the current findings reflect a meaningful departure from published studies, or a discrepancy that stems from the use of prospective data (Greenfield, 2010), is unclear. However, the considerable variability in how child abuse is assessed and analyzed in published studies on health is an issue of concern from the standpoint of trying to compare published findings (Greenfield, 2010). Of course, a primary consideration in the child abuse literature is whether prospective and retrospective measures of abuse are comparable and equally reliable as predictors of later developmental outcomes (Widom & Shepard, 1996). Other considerations include whether data on abuse are from official records or self-reports and whether the frequency and severity of abuse are factored into the measures that are used (Widom et al., 2004). Differences can also arise from measuring adult health differently across studies and from collecting data from non-representative samples.
Another complicating factor is that certain studies combine indicators of child abuse and other adverse experiences (Anda et al., 1999; Dube et al., 2003; Felitti et al., 1998; Middlebrooks & Audage, 2008), making it difficult to determine which risk influence is most strongly related to poor adult health. Indeed, additive models of childhood risk and adversity are conceptually meaningful, but they pertain to research questions that are different from those that focus exclusively on a certain risk factor or developmental process. The additive scaling in certain studies (Anda et al., 1999; Felitti et al., 1998) is informative, but not as well suited to studying the unique effects of child abuse in predictive modeling.
Analyses of social support variables (SSNRs) reported in the current investigation are related to the Essentials for Childhood Framework (Centers for Disease Control and Prevention, n.d.). It is generally proposed that social support will moderate the effect of early adversity on later health (Uchino, 2009). However, it appears that social support also mediates this association (Springer, 2009). Kendall-Tackett (2002) describes this mechanism as a “social pathway” linking abuse to health, which is contrasted to other pathways that include behavioral and biological variables.
Consistent with the social pathway model, it is believed that children who suffer abuse often fail to develop strong, positive relationships, and that the absence of relationships impairs their ability to make good choices about their health, and to seek help when they are in need. A lack of social support for young people may also reflect the absence of positive mentoring from adult role models, which is critical to helping them develop skills and competencies conducive to physical and mental well-being (Kendall-Tackett, 2002; Springer, 2009). Of course, factors other than social support, such as health-risk behaviors of smoking and substance use, as well as those having to do with the biological embedding of stress must also be considered (Shonkoff et al., 2009).
To the extent that social support plays a primary or even a secondary role in the development of adult health problems, implications for prevention and treatment are important to consider. Prevention to enhance social support can include efforts to stabilize the living environments of abused children or to strengthen interpersonal networks that lessen stress and promote positive coping. However, a reality for many abused children is that their living situations are both unstable and unpredictable. If a child is removed from a home due to safety concerns, repeated residence and caregiver changes can cause further harm (Smith, Stormshak, Chamberlain, & Bridges Whaley, 2001). According to a review of the literature on children placed in foster care, rates of disruption in care range from 38% to 57% during the first 12 to 18 months. For victims not placed in foster care, it is still possible that families are in crisis and that parents are mandated into treatment for mental health and substance use problems (E. C. Herrenkohl et al., 2003).
As noted in a report by the CDC (CDC, n.d.), there are a number of established and emerging programs that have been shown to benefit children from abusive home environments. Programs in early childcare, home visitation, and parent-child interaction therapy are good examples. Emerging programs include the Legacy for Children™ parenting intervention program. Legacy is an evidence-based program designed to foster social support, child development knowledge, and positive parenting practices among low-income mothers of young children (Kaminski, Perou, & Visser, 2013). For children who have already experienced abuse, tested interventions like cognitive behavioral therapy and health promotion strategies are potentially viable (Kristman-Valente, Brown, & Herrenkohl, 2013).
In that results underscore the importance of social support, implications for the treatment of adult survivors of child abuse include a goal of helping them develop and expand their networks of support, as well as strengthening interpersonal skills that will draw others closer (Kendall-Tackett, 2002). Because many survivors of abuse have experienced failed relationships, attention may also need to be focused on redressing the emotional hardship and disappointment that those earlier relationships caused. Helping survivors learn cognitive strategies that promote positive coping is also important to help them contend with past loss as well as stressful events in the future (Kendall-Tackett, 2002).
Limitations
Limitations of the study include a reliance on existing data to model SSNR influences, which impacted the range of measures available. Additionally, the temporal ordering of certain variables, including those on social support, cannot be determined because of the nature of the questions asked of participants in the larger study.
Certain indicators of model fit in our CFA and structural model tests are below their optimal values, while others are within the range considered acceptable. As noted earlier, other characteristics of an SEM should be considered when judging the merits of an analysis like the one discussed (Barrett, 2007), such as whether the analysis was guided by theory and whether patterns in the data are consistent with other published findings. The tested model was theoretically guided by the Essentials for Childhood framework, factor loadings were statistically significant, and correlations are generally consistent with those of earlier studies, but weaker for abuse and adult health. Further, findings are based on a sample drawn from a specific area of the Eastern United States, which lacks the diversity characteristic of other regions. The racial and ethnic composition of the sample is, however, consistent with the local context, and the sample itself is socioeconomically diverse and gender balanced. As a result, we accounted for SES and gender in the analysis model, although it may be that other context and cultural factors are also relevant.
Further, the study did not address the impacts of child abuse on youth and adult health habits, including smoking and substance use (Kristman-Valente et al., 2013), which can impact health and lead to health declines. Measures of service utilization and disability are also important but were not considered (Leeb et al., 2011). All limitations duly noted, the prospective design of the study, its use of multiple data sources, and its careful attention to various characteristics of social support make for an important contribution to the research literature. An emphasis on subtypes of child abuse (physical, emotional, sexual) is another noted strength.
Acknowledgments
This research was supported by the Centers for Disease Control and Prevention (200-2011-F-38936) and by grants from the National Institute on Child Health and Human Development and the Office of Behavioral Social Sciences and Research (RO1 HD049767). The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the National Institutes of Health. The funding agencies played no role in the study design; in the collection, analysis, and interpretation of data; in the writing of this article; nor in the decision to submit it for publication.
Contributor Information
Todd I. Herrenkohl, Email: tih@uw.edu.
Hyunzee Jung, Email: hzjung@u.washington.edu.
W. Alex Mason, Email: Walter.Mason@boystown.org.
Eric C. Brown, Email: ricbrown@miami.edu.
Rebecca T. Leeb, Email: rsl4@cdc.gov.
Roy. C. Herrenkohl, Email: rch1@lehigh.edu.
References
- Anda RF, Croft JB, Felitti VJ, Nordenberg D, Giles WH, Williamson DF, Giovano GA. Adverse childhood experiences and smoking during adolescence and adulthood. JAMA. 1999;282:1652–1658. doi: 10.1001/jama.282.17.1652. [DOI] [PubMed] [Google Scholar]
- Barrett P. Structural equation modelling: Adjudging model fit. Personality and Individual Differences. 2007;42:815–824. [Google Scholar]
- Batten SV, Aslan M, Maciejewski PK, Mazure CM. Childhood maltreatment as a risk factor for adult cardiovascular disease and depression. Journal of Clinical Psychiatry. 2004;65:249–254. doi: 10.4088/jcp.v65n0217. [DOI] [PubMed] [Google Scholar]
- Berkman LF, Leo-Summers L, Horwitz RI. Emotional support and survival after myocardial infarction: A prospective, population-based study of the elderly. Annals of Internal Medicine. 1992;117:1003–1009. doi: 10.7326/0003-4819-117-12-1003. [DOI] [PubMed] [Google Scholar]
- Bolger KE, Patterson CJ. Pathways from child maltreatment to internalizing problems: Perceptions of control as mediators and moderators. Development and Psychopathology. 2001;13:913–940. [PubMed] [Google Scholar]
- Braveman P, Egerter S, Arena K, Aslam R. Early childhood experiences shape health and well-being throughout life. Princeton, NJ: Robert Wood Johnson Foundation; 2014. [Google Scholar]
- Browne MW, Cudeck R. Alternate ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation models. Newbury Park, CA: Sage; 1993. pp. 136–162. [Google Scholar]
- Brummett BH, Barefoot JC, Siegler IC, Clapp-Channing NE, Lytle BL, Bosworth HB, Mark DB. Characteristics of socially isolated patients with coronary artery disease who are at elevated risk for mortality. Psychosomatic Medicine. 2001;63:267–272. doi: 10.1097/00006842-200103000-00010. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Essentials for Childhood: Steps to create safe, stable, and nurturing relationships. 2014 Retrieved from http://www.cdc.gov/violenceprevention/pdf/essentials_for_childhood_framework.pdf.
- Centers for Disease Control and Prevention (n.d.) Promoting safe, stable, and nurturing relationships: A strategic direction for child maltreatment prevention. Atlanta, GA: Centers for Disease Control and Prevention, National Center on Injury Prevention and Control; [Google Scholar]
- Dube SR, Felitti VJ, Dong M, Chapman DP, Giles W, Anda RF. Childhood abuse, neglect, and household dysfunction and the risk of illicit drug use: The Adverse Childhood Experiences Study. Pediatrics. 2003;111:564–572. doi: 10.1542/peds.111.3.564. [DOI] [PubMed] [Google Scholar]
- Dube SR, Williamson DF, Thompson T, Felitti VJ, Anda RF. Assessing the reliability of retrospective reports of adverse childhood experiences among adult HMO members attending a primary care clinic. Child Abuse & Neglect. 2004;28:729–737. doi: 10.1016/j.chiabu.2003.08.009. [DOI] [PubMed] [Google Scholar]
- Ell K, Nishimoto R, Mediansky L, Mantell J, Hamovtich M. Social relations, social support and survival among patients with cancer. Journal of Psychosomatic Research. 1992;36:531–541. doi: 10.1016/0022-3999(92)90038-4. [DOI] [PubMed] [Google Scholar]
- Fagundes CP, Way B. Early-life stress and adult inflammation. Current Directions in Psychological Science. 2014;23:277–283. [Google Scholar]
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, Marks JS. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine. 1998;14:245–258. doi: 10.1016/s0749-3797(98)00017-8. [DOI] [PubMed] [Google Scholar]
- Finkelhor D, Turner HA, Shattuck A, Hamby SL. Violence, crime, and abuse exposure in a national sample of children and youth: An update. JAMA Pediatrics. 2013;167:614–621. doi: 10.1001/jamapediatrics.2013.42. [DOI] [PubMed] [Google Scholar]
- Goffin RD. Assessing the adequacy of structural equation models: Golden rules and editorial policies. Personality and Individual Differences. 2007;42:831–839. [Google Scholar]
- Greenfield EA. Child abuse as a life-course social determinant of adult health. Maturitas. 2010;66:51–55. doi: 10.1016/j.maturitas.2010.02.002. [DOI] [PubMed] [Google Scholar]
- Hardt J, Rutter M. Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry. 2004;45:260–273. doi: 10.1111/j.1469-7610.2004.00218.x. [DOI] [PubMed] [Google Scholar]
- Herrenkohl EC, Herrenkohl RC, Egolf BP. The psychosocial consequences of living environment instability on maltreated children. American Journal of Orthopsychiatry. 2003;73:367–380. doi: 10.1037/0002-9432.73.4.367. [DOI] [PubMed] [Google Scholar]
- Herrenkohl RC, Herrenkohl EC, Egolf BP, Wu P. The developmental consequences of child abuse: The Lehigh Longitudinal Study. In: Starr RHJ, Wolfe DA, editors. The effects of child abuse and neglect: Issues and research. New York: The Guilford Press; 1991. pp. 57–81. [Google Scholar]
- Herrenkohl TI. Family violence and co-occurring risk factors for children exposed to violence. In: Herrenkohl TI, Aisenberg E, Williams JH, Jenson JM, editors. Violence in context: Current evidence on risk, protection, and prevention. New York: Oxford University Press; 2011a. pp. 73–91. [Google Scholar]
- Herrenkohl TI. Resilience and protection from violence exposure in children: Implications for prevention and intervention programs with vulnerable populations. In: Herrenkohl TI, Aisenberg E, Williams JH, Jenson JM, editors. Violence in context: Current evidence on risk, protection, and prevention. New York: Oxford University Press; 2011b. pp. 92–108. [Google Scholar]
- Herrenkohl TI, Hong S, Klika JB, Herrenkohl RC, Russo MJ. Developmental impacts of child abuse and neglect related to adult mental health, substance use, and physical health. Journal of Family Violence. 2013;28:191–199. doi: 10.1007/s10896-012-9474-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herrenkohl TI, Klika JB, Herrenkohl RC, Russo MJ, Dee T. A prospective investigation analysis of the relationship between child maltreatment and indicators of adult psychological well-being. Violence and Victims. 2012;27:764–776. doi: 10.1891/0886-6708.27.5.764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu L, Bentler PM. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods. 1998;3:424–453. [Google Scholar]
- Kaminski JW, Perou R, Visser SN. Behavioral and socioemotional outcomes through age 5 years of the Legacy for Children public health approach to improving developmental outcomes among children born into poverty. American Journal of Public Health. 2013;103:1058–1066. doi: 10.2105/AJPH.2012.300996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kendall-Tackett K. The health effects of childhood abuse: Four pathways by which abuse can influence health. Child Abuse & Neglect. 2002;26:715–729. doi: 10.1016/s0145-2134(02)00343-5. [DOI] [PubMed] [Google Scholar]
- Klika JB, Herrenkohl TI. A review of developmental research on resilience in maltreated children. Trauma, Violence, and Abuse. 2013;14:222–234. doi: 10.1177/1524838013487808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kristman-Valente AN, Brown EC, Herrenkohl TI. Child physical and sexual abuse and cigarette smoking behavior in adolescence and adulthood. Journal of Adolescent Health. 2013;53:533–538. doi: 10.1016/j.jadohealth.2013.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kristman-Valente AN, Wells EA. The role of gender in the association between child maltreatment and substance use behavior: A systematic review of longitudinal research from 1995 to 2011. Substance Use and Misuse. 2013;48:645–660. doi: 10.3109/10826084.2013.800115. [DOI] [PubMed] [Google Scholar]
- Kroenke K, Spitzer R, Williams JBW. The PHQ-15: Validity of a new measure for evaluating the severity of somatic symptoms. Psychosomatic Medicine. 2002;64:258–266. doi: 10.1097/00006842-200203000-00008. [DOI] [PubMed] [Google Scholar]
- Leeb RT, Lewis T, Zolotor AJ. A review of physical and mental health consequences of child abuse and neglect and implications for practice. American Journal of Lifestyle Medicine. 2011;5:454–468. [Google Scholar]
- MacCallum RC, Browne MW, Sugawara HM. Power analysis and determination of sample size for covariance structure modeling. Psychological Methods. 1996;1:130–149. [Google Scholar]
- MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research. 2004;39:99–128. doi: 10.1207/s15327906mbr3901_4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masten AS. Ordinary magic: Resilience processes in development. American Psychologist. 2001;56:227–238. doi: 10.1037//0003-066x.56.3.227. [DOI] [PubMed] [Google Scholar]
- Merrick MT, Leeb RT, Lee RD. Examining the role of safe, stable, and nurturing relationships in the intergenerational continuity of child maltreatment—Introduction to the Special Issue. Journal of Adolescent Health. 2013;53:S1–S3. doi: 10.1016/j.jadohealth.2013.06.017. [DOI] [PubMed] [Google Scholar]
- Middlebrooks JS, Audage NC. The effects of childhood stress on health across the lifespan. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; 2008. [Google Scholar]
- Murthi M, Espelage DL. Childhood sexual abuse, social support, and psychological outcomes: A loss framwework. Child Abuse & Neglect. 2005;29:1215–1231. doi: 10.1016/j.chiabu.2005.03.008. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. Los Angeles: Muthen & Muthen; 2013. [Google Scholar]
- Repetti RL, Taylor SE, Seeman TE. Risky families: Family social environments and the mental and physical health of offspring. Psychological Bulletin. 2002;128:330–366. [PubMed] [Google Scholar]
- Sachs-Ericsson N, Blazer D, Plant EA, Arnow B. Childhood sexual and physical abuse and 1-year prevalence of medical problems in the National Comorbidity Survey. Health Psychology. 2005;24:32–40. doi: 10.1037/0278-6133.24.1.32. [DOI] [PubMed] [Google Scholar]
- Sedlak A. Fourth National Incidence Study of Child Abuse and Neglect (NIS-4): Report to Congress. Washington DC: Westat Inc.; 2010. [Google Scholar]
- Shonkoff JP, Boyce WT, McEwen BS. Neuroscience, molecular biology, and the childhood roots of health disparities. JAMA. 2009;301:2252–2260. doi: 10.1001/jama.2009.754. [DOI] [PubMed] [Google Scholar]
- Smith DK, Stormshak E, Chamberlain P, Bridges Whaley R. Placement disruption in treatment foster care. Journal of Emotional and Behavioral Disorders. 2001;9:200–205. [Google Scholar]
- Springer KW. Childhood physical abuse and midlife physical health: Testing a multi-pathway life course model. Social Science and Medicine. 2009;69:138–146. doi: 10.1016/j.socscimed.2009.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Springer KW, Sheridan J, DKuo D, Carnes M. Long-term physical and mental health consequences of childhood physical abuse: Results from a large population-based sample of men and women. Child Abuse & Neglect. 2007;31:517–530. doi: 10.1016/j.chiabu.2007.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services. Child maltreatment 2009. 2010 Retrieved from http://archive.acf.hhs.gov/programs/cb/pubs/cm09/cm09.pdf.
- Uchino BN. Understanding the links between social support and physical health: A life-span perspective with emphasis on the separability of perceived and received support. Perspectives on Psychological Science. 2009;4:236–255. doi: 10.1111/j.1745-6924.2009.01122.x. [DOI] [PubMed] [Google Scholar]
- Ware JE, Kosinski M, Dewey JE. How to score version two of the SF-36 Health Survey. Lincoln, RI: Quality Metric; 2000. [Google Scholar]
- Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Medical Care. 1992;30:473–483. [PubMed] [Google Scholar]
- Widom CS, Mormonstein NR, White HR. Childhood victimization and illicit drug use in middle adulthood. Psychology of Addictive Behaviors. 2006;20:394–403. doi: 10.1037/0893-164X.20.4.394. [DOI] [PubMed] [Google Scholar]
- Widom CS, Raphael KG, DuMont KA. The case for prospective longitudinal studies in child maltreatment research: Commentary on Dube, Williamson, Thompson, Felitti, and Anda (2004) Child Abuse & Neglect. 2004;28:715–722. doi: 10.1016/j.chiabu.2004.03.009. [DOI] [PubMed] [Google Scholar]
- Widom CS, Shepard RL. Accuracy of adult recollections of childhood victimization: Part 1. Childhood physical abuse. Psychological Assessment. 1996;8:412–421. [Google Scholar]
- Zhao X, Lynch JG, Jr, Chen Q. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. Journal of Consumer Research. 2010;37:197–206. [Google Scholar]